Can Ultrasound-Guided Femoral Vein Measurements Predict Spinal Anesthesia-Induced Hypotension in Non-Obstetric Surgery? A Prospective Observational Study

Abstract
:1. Introduction
2. Material and Methods
2.1. Ethics and Study Design
2.2. Participants
2.3. Anesthesia-Related Features
2.3.1. Before Spinal Anesthesia
2.3.2. During and after Spinal Anesthesia
2.4. Sonographic Technique and Measurements
2.4.1. Inferior Vena Cava Measurements
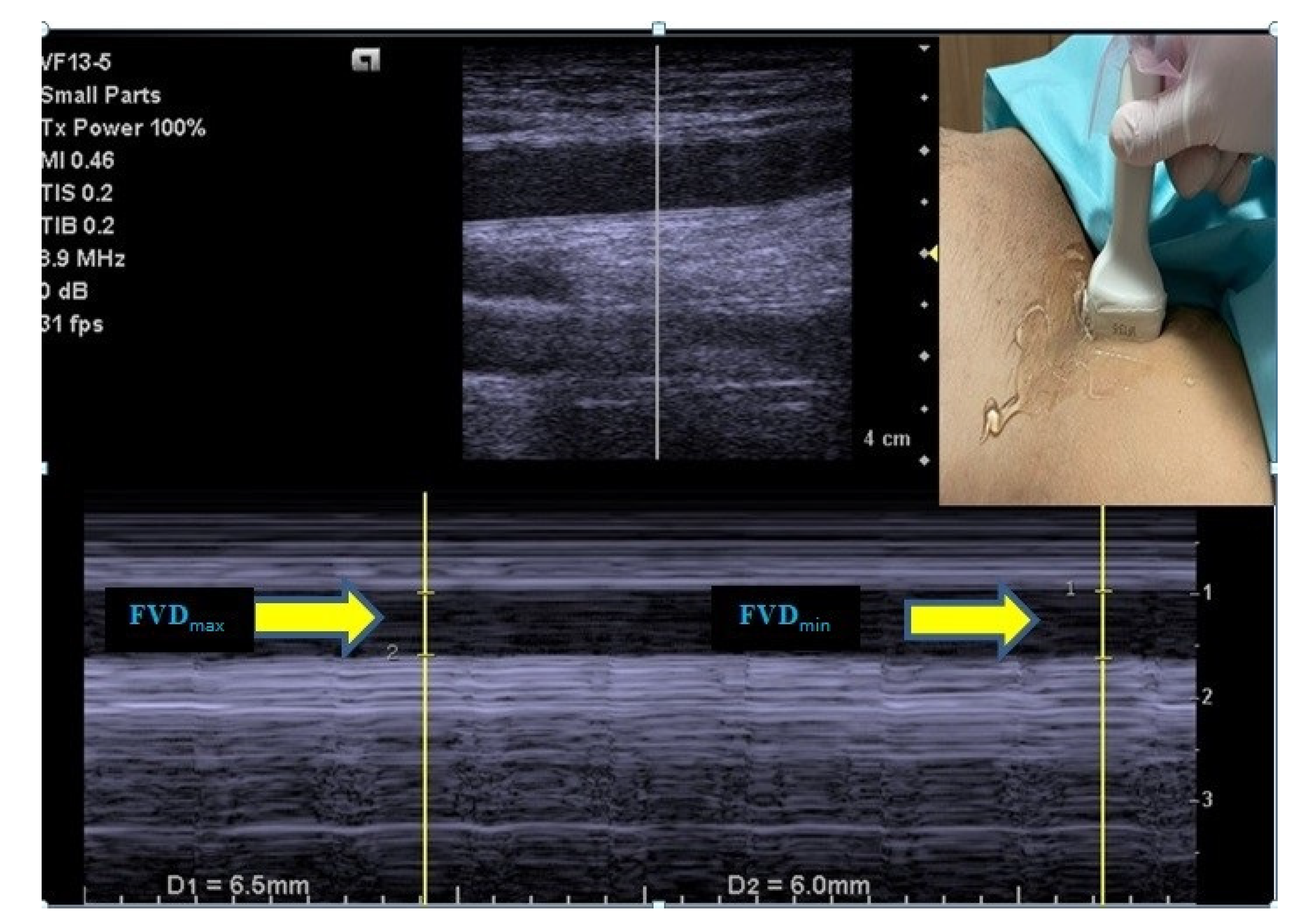
2.4.2. Femoral Vein Measurements
2.5. SAIH Criteria and Treatment
2.6. Outcomes
2.7. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Salama, E.R.; Elkashlan, M. Pre-operative ultrasonographic evaluation of inferior vena cava collapsibility index and caval aorta index as new predictors for hypotension after induction of spinal anaesthesia: A prospective observational study. Eur. J. Anaesthesiol. 2019, 36, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Ceruti, S.; Anselmi, L.; Minotti, B.; Franceschini, D.; Aguirre, J.; Borgeat, A.; Saporito, A. Prevention of arterial hypotension after spinal anaesthesia using vena cava ultrasound to guide fluid management. Br. J. Anaesth. 2018, 120, 101–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lirk, P.; Haller, I.; Wong, C.A. Management of spinal anaesthesia-induced hypotension for caesarean delivery: A European survey. Eur. J. Anaesthesiol. 2012, 29, 452–453. [Google Scholar] [CrossRef] [PubMed]
- Monk, T.G.; Bronsert, M.R.; Henderson, W.G.; Mangione, M.P.; Sum-Ping, S.T.J.; Bentt, D.R.; Nguyen, J.D.; Richman, J.S.; Meguid, R.A.; Hammermeister, K.E. Association between Intraoperative Hypotension and Hypertension and 30-day Postoperative Mortality in Noncardiac Surgery. Anesthesiology 2015, 123, 307–319. [Google Scholar] [CrossRef] [PubMed]
- Berwanger, O.; Le Manach, Y.; Suzumura, E.A.; Biccard, B.; Srinathan, S.K.; Szczeklik, W.; Santo, J.A.E.; Santucci, E.; Cavalcanti, A.B.; Archbold, R.A.; et al. Association between pre-operative statin use and major cardiovascular complications among patients undergoing non-cardiac surgery: The VISION study. Eur. Heart J. 2016, 37, 177–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, S.; Kothari, N.; Goyal, S.; Sharma, A.; Kumar, R.; Kaloria, N.; Bhatia, P. Preoperative assessment of inferior vena cava collapsibility index by ultrasound is not a reliable predictor of post-spinal anesthesia hypotension. Braz. J. Anesthesiol. (Engl. Ed.) 2022. [Google Scholar] [CrossRef]
- Tarkkila, P.; Isola, J. A regression model for identifying patients at high risk of hypotension, bradycardia and nausea during spinal anesthesia. Acta Anaesthesiol. Scand. 1992, 36, 554–558. [Google Scholar] [CrossRef]
- Hartmann, B.; Junger, A.; Klasen, J.; Benson, M.; Jost, A.; Banzhaf, A.; Hempelmann, G. The incidence and risk factors for hypotension after spinal anesthesia induction: An analysis with automated data collection. Anesth. Analg. 2002, 94, 1521–1529. [Google Scholar] [CrossRef]
- Carpenter, R.L.; Caplan, R.A.; Brown, D.L.; Stephenson, C.; Wu, R. Incidence and risk factors for side effects of spinal anesthesia. Anesthesiology 1992, 76, 906–916. [Google Scholar] [CrossRef]
- Kent, A.; Patil, P.; Davila, V.; Bailey, J.K.; Jones, C.; Evans, D.C.; Boulger, C.T.; Adkins, E.; Balakrishnan, J.M.; Valiyaveedan, S.; et al. Sonographic evaluation of intravascular volume status: Can internal jugular or femoral vein collapsibility be used in the absence of IVC visualization? Ann. Thorac. Med. 2015, 10, 44–49. [Google Scholar]
- Jaya, W.; Abshor, U.; Laksono, B.H.; Fatoni, A.Z. Delta Inferior Vena Cava Index Correlated with Mean Arterial Pressure (MAP) in Spinal Anesthesia. J. Anaesth. Pain 2021, 2, 65–69. [Google Scholar] [CrossRef]
- Yu, C.; Gu, J.; Liao, Z.; Feng, S. Prediction of spinal anesthesia-induced hypotension during elective cesarean section: A systematic review of prospective observational studies. Int. J. Obstet. Anesth. 2021, 47, 103175. [Google Scholar] [CrossRef]
- Kent, A.; Bahner, D.P.; Boulger, C.T.; Eiferman, D.S.; Adkins, E.J.; Evans, D.C.; Springer, A.N.; Balakrishnan, J.M.; Valiyaveedan, S.; Galwankar, S.C.; et al. Sonographic evaluation of intravascular volume status in the surgical intensive care unit: A prospective comparison of subclavian vein and inferior vena cava collapsibility index. J. Surg. Res. 2013, 184, 561–566. [Google Scholar] [CrossRef]
- Abdelhamid, B.M.; Ahmed, A.; Ramzy, M.; Rady, A.; Hassan, H. Pre-anaesthetic ultrasonographic assessment of neck vessels as predictors of spinal anaesthesia induced hypotension in the elderly: A prospective observational study. Egypt. J. Anaesth. 2022, 38, 349–356. [Google Scholar] [CrossRef]
- Cho, R.J.; Williams, D.R.; Leatherman, J.W. Measurement of femoral vein diameter by ultrasound to estimate central venous pressure. Ann. Am. Thorac. Soc. 2016, 13, 81–85. [Google Scholar] [CrossRef]
- Nedel, W.L.; Simas, D.M.; Marin, L.G.; Morais, V.D.; Friedman, G. Respiratory variation in femoral vein diameter has moderate accuracy as a marker of fluid responsivity in mechanically ventilated septic shock patients. Ultrasound Med. Biol. 2017, 43, 2713–2717. [Google Scholar] [CrossRef]
- Yao, S.-F.; Zhao, Y.-H.; Zheng, J.; Qian, J.-Y.; Zhang, C.; Xu, Z.; Xu, T. The transverse diameter of right common femoral vein by ultrasound in the supine position for predicting post-spinal hypotension during cesarean delivery. BMC Anesthesiol. 2021, 21, 1–9. [Google Scholar] [CrossRef]
- Doyle, D.J.; Goyal, A.; Bansal, P.; Garmon, E.H. American Society of Anesthesiologists Classification. In Statpearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- McNeil-Masuka, J.; Boyer, T.J. Insensible Fluid Loss. 2019. Available online: https://www.ncbi.nlm.nih.gov/books/NBK544219/ (accessed on 15 October 2022).
- DeMers, D.; Wachs, D. Physiology, Mean Arterial Pressure. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography: Endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar]
- Ni, T.-T.; Zhou, Z.-F.; He, B.; Zhou, Q.-H. Inferior Vena Cava Collapsibility Index Can Predict Hypotension and Guide Fluid Management After Spinal Anesthesia. Front. Surg. 2022, 9, 831539. [Google Scholar] [CrossRef]
- Abd Elraziq, B.A.; Ali, S.F.; Abotaleb, U.I.; Alqassas, M.H. Norepinephrine versus Ephedrine in Prevention of Hypotension after Spinal Anesthesia. Al-Azhar Int. Med. J. 2020, 1, 37–42. [Google Scholar] [CrossRef]
- Favre, M.; Ceruti, S.; Biggiogero, M.; Musiari, M.; Glotta, A.; Gimigliano, I.; Aguirre, J.; Borgeat, A.; Saporito, A. Fluid administration guided by inferior vena cava ultrasound before spinal anaesthesia may reduce post procedural hypotension rate. medRxiv 2021. [Google Scholar] [CrossRef]
- Chowdhury, S.R.; Baidya, D.K.; Maitra, S.; Singh, A.K.; Rewari, V.; Anand, R.K. Assessment of role of inferior vena cava collapsibility index and variations in carotid artery peak systolic velocity in prediction of post-spinal anaesthesia hypotension in spontaneously breathing patients: An observational study. Indian J. Anaesth. 2022, 66, 100. [Google Scholar] [PubMed]
- Zidan, D.; Baess, A. Comparison between femoral vein diameter and inferior vena cava diameter by ultrasound in estimation of central venous pressure in mechanically ventilated patients. Res. Opin. Anesth. Intensive Care 2020, 7, 100. [Google Scholar] [CrossRef]
- Kim, D.-W.; Chung, S.; Kang, W.-S.; Kim, J. Diagnostic Accuracy of Ultrasonographic Respiratory Variation in the Inferior Vena Cava, Subclavian Vein, Internal Jugular Vein, and Femoral Vein Diameter to Predict Fluid Responsiveness: A Systematic Review and Meta-Analysis. Diagnostics 2021, 12, 49. [Google Scholar] [CrossRef] [PubMed]
- Ayyanagouda, B.; Ajay, B.; Joshi, C.; Hulakund, S.; Ganeshnavar, A.; Archana, E. Role of ultrasonographic inferior venacaval assessment in averting spinal anaesthesia-induced hypotension for hernia and hydrocele surgeries—A prospective randomised controlled study. Indian J. Anaesth. 2020, 64, 849. [Google Scholar]
- Gui, J.; Guo, J.; Nong, F.; Jiang, D.; Xu, A.-D.; Yang, F.; Chen, Q.; Lin, Y. Impact of individual characteristics on sonographic IVC diameter and the IVC diameter/aorta diameter index. Am. J. Emerg. Med. 2015, 33, 1602–1605. [Google Scholar] [CrossRef]
- Masugata, H.; Senda, S.; Okuyama, H.; Murao, K.; Inukai, M.; Hosomi, N.; Iwado, Y.; Noma, T.; Kohno, M.; Himoto, T.; et al. Age-related decrease in inferior vena cava diameter measured with echocardiography. Tohoku J. Exp. Med. 2010, 222, 141–147. [Google Scholar] [CrossRef] [Green Version]
- Zhang, N.; He, L.; Ni, J.-X. Level of sensory block after spinal anesthesia as a predictor of hypotension in parturient. Medicine 2017, 96, e7184. [Google Scholar] [CrossRef]
- Buggy, D.; Higgins, P.; Moran, C.; O’Brien, D.; O’Donovan, F.; McCarroll, M. Prevention of spinal anesthesia-induced hypotension in the elderly: Comparison between preanesthetic administration of crystalloids, colloids, and no prehydration. Anesth. Analg. 1997, 84, 106–110. [Google Scholar] [CrossRef]


{kind=link}
| Hypotension | ||||
|---|---|---|---|---|
| All Patients | No (n = 83) | Yes (n = 12) | p | |
| Age | 51 (19–71) | 48 (21–71) | 58 (19–70) | 0.081 |
| Sex | ||||
| Male | 62 (65.3%) | 53 (63.9%) | 9 (75.0%) | 0.533 |
| Female | 33 (34.7%) | 30 (36.1%) | 3 (25.0%) | |
| Body mass index (kg/m2) | 26.0 (16.5–39.0) | 26.1 (16.5–35.0) | 25.4 (19.0–39.0) | 0.494 |
| ASA classification | ||||
| 1 | 51 (53.7%) | 50 (60.2%) | 1 (8.3%) | 0.002 |
| 2 | 44 (46.3%) | 33 (39.8%) | 11 (91.7%) | |
| Department of surgery | ||||
| Urology | 19 (20.0%) | 16 (19.3%) | 3 (25.0%) | 0.240 |
| Orthopedics | 38 (40.0%) | 36 (43.4%) | 2 (16.7%) | |
| Cardiovascular | 13 (13.7%) | 10 (12.0%) | 3 (25.0%) | |
| General | 25 (26.3%) | 21 (25.3%) | 4 (33.3%) | |
| Inferior vena cava | ||||
| Maximum diameter (cm) | 2.45 (1.30–3.20) | 2.56 (1.30–3.20) | 2.05 (1.89–2.87) | 0.728 |
| Minimum diameter (cm) | 2.01 (0.70–2.90) | 2.04 (0.70–2.90) | 1.96 (1.34–2.30) | 0.556 |
| Collapsibility index (%) | 18.52 (1.99–58.58) | 18.29 (4.49–58.58) | 20.00 (1.99–31.98) | 0.556 |
| Femoral vein | ||||
| Maximum diameter (cm) | 0.93 (0.57–1.40) | 0.93 (0.59–1.40) | 0.95 (0.57–1.19) | 0.982 |
| Minimum diameter (cm) | 0.78 (0.39–1.03) | 0.78 (0.42–1.03) | 0.83 (0.39–1.02) | 0.766 |
| Collapsibility index (%) | 15.52 (1.32–40.71) | 16.05 (1.32–40.71) | 10.99 (4.41–34.45) | 0.370 |
| Systolic blood pressure (mmHg) | |
| Baseline | 146 (107–178) a |
| 0th minute | 142 (110–171) a |
| 1st minute | 131 (95–164) b |
| 5th minute | 124 (90–168) c |
| 10th minute | 118 (73–157) d |
| 15th minute | 118 (77–160) d |
| p | <0.001 |
| Diastolic blood pressure (mmHg) | |
| Baseline | 82 (58–104) a |
| 0th minute | 75 (54–103) a |
| 1st minute | 70 (48–99) b |
| 5th minute | 67 (45–96) bc |
| 10th minute | 63 (42–92) d |
| 15th minute | 64 (51–98) cd |
| p | <0.001 |
| Mean blood pressure (mmHg) | |
| Baseline | 103 (61–129) a |
| 0th minute | 101 (66–127) a |
| 1st minute | 94 (61–121) b |
| 5th minute | 89 (63–116) b |
| 10th minute | 81 (61–114) c |
| 15th minute | 82 (61–117) c |
| p | <0.001 |
| Heart rate (beats/min) | |
| Baseline | 76 (58–118) a |
| 0th minute | 76 (51–117) a |
| 1st minute | 78 (55–114) a |
| 5th minute | 76 (53–113) ab |
| 10th minute | 76 (46–108) b |
| 15th minute | 73 (51–107) b |
| p | <0.001 |
| Hypotension criteria met | |
| Decrease in systolic blood pressure, ≥30% | 12 (12.6%) |
| Systolic blood pressure, <90 | 5 (5.3%) |
| Mean blood pressure, <60 | 0 (0.0%) |
| β Coefficient | Standard Error | p | Exp(β) | 95.0% CI for Exp(β) | ||
|---|---|---|---|---|---|---|
| Age | 0.051 | 0.032 | 0.114 | 1.052 | 0.988 | 1.121 |
| Sex, Female | −0.839 | 0.808 | 0.299 | 0.432 | 0.089 | 2.105 |
| Body mass index | −0.028 | 0.099 | 0.779 | 0.973 | 0.801 | 1.181 |
| ASA classification, 2 | 2.707 | 1.102 | 0.014 | 14.982 | 1.727 | 129.930 |
| Department, Orthopedics | −1.500 | 0.946 | 0.113 | 0.223 | 0.035 | 1.426 |
| Inferior vena cava collapsibility index | −0.049 | 0.042 | 0.235 | 0.952 | 0.877 | 1.033 |
| Femoral vein collapsibility index | −0.004 | 0.037 | 0.925 | 0.996 | 0.926 | 1.072 |
| Constant | −4.092 | 3.270 | 0.211 | 0.017 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yılmaz, A.; Demir, U.; Taşkın, Ö.; Soylu, V.G.; Doğanay, Z. Can Ultrasound-Guided Femoral Vein Measurements Predict Spinal Anesthesia-Induced Hypotension in Non-Obstetric Surgery? A Prospective Observational Study. Medicina 2022, 58, 1615. https://doi.org/10.3390/medicina58111615
Yılmaz A, Demir U, Taşkın Ö, Soylu VG, Doğanay Z. Can Ultrasound-Guided Femoral Vein Measurements Predict Spinal Anesthesia-Induced Hypotension in Non-Obstetric Surgery? A Prospective Observational Study. Medicina. 2022; 58(11):1615. https://doi.org/10.3390/medicina58111615
Chicago/Turabian StyleYılmaz, Ayşe, Ufuk Demir, Öztürk Taşkın, Veysel Garani Soylu, and Zahide Doğanay. 2022. "Can Ultrasound-Guided Femoral Vein Measurements Predict Spinal Anesthesia-Induced Hypotension in Non-Obstetric Surgery? A Prospective Observational Study" Medicina 58, no. 11: 1615. https://doi.org/10.3390/medicina58111615