Abstract
Background and Objectives: This systematic review and meta-analysis of randomized controlled trials was performed to compare the therapeutic effects and safety profiles of silodosin and tamsulosin for medical expulsive therapy (MET) of ureteral stones. Materials and Methods: We searched PubMed, EMBASE, the Cochrane Library, and Web of Science to identify articles published before July 2022 that described randomized controlled trials comparing silodosin and tamsulosin for MET of ureteral stones. Endpoints were stone expulsion rate, stone expulsion time, and total complication rate. Results: In total, 14 studies were included in our analysis. The size of ureteral stones was <1 cm. Compared with tamsulosin, silodosin resulted in a significantly higher stone expulsion rate (p < 0.01, odds ratio (OR) = 2.42, 95% confidence interval (CI) = 1.91 to 3.06, I2 = 0%) and significantly shorter stone expulsion time (p < 0.01, mean difference = −3.04, 95% CI = −4.46 to −1.63, I2 = 89%). The total complication rate did not significantly differ between silodosin and tamsulosin (p = 0.33, OR = 1.15, 95% CI = 0.87 to 1.52, I2 = 7%). Conclusions: Compared with tamsulosin, silodosin resulted in significantly better expulsion of ureteral stones <1 cm. The total complication rate did not significantly differ between silodosin and tamsulosin. Thus, silodosin may be superior to tamsulosin for MET of ureter stones <1 cm.
1. Introduction
The global incidence of urolithiasis, a disease with a high recurrence rate, is increasing [1]. Urolithiasis causes recurrent stone formers to experience a decline in quality of life, and there is an increasing socioeconomic burden associated with the management of urolithiasis [2]. Methods to manage ureteral stones include conservative treatment, pharmacological treatment (e.g., medical expulsive therapy (MET)), shock wave lithotripsy, and surgical treatment. Thus, urologists must select the appropriate treatment for each patient (i.e., non-surgical or surgical).
During the coronavirus disease 2019 (COVID-19) pandemic, there has been a significant change in treatment, such that emergent surgical treatment tended to decrease, whereas non-surgical treatment tended to increase [3].
According to the European Association of Urology (EAU) Guidelines on Urolithiasis, MET is recommended as a treatment option for (distal) ureteral stones >5 mm and can lessen episodes of renal colic [4]. The drugs used for MET include α-blockers, calcium channel inhibitors, and phosphodiesterase-5 inhibitors. α-blockers are regarded as the standard drugs for MET of ureteral stones, and differences in efficacy have been demonstrated among α-blockers [4]. However, whereas the American Urological Association guidelines recommend the use of α-blockers for MET of distal ureteral stones <10 mm, the guidelines do not address differences in efficacy among α-blockers [5]. Here, we performed an updated systematic review and meta-analysis of the efficacies and safety profiles of silodosin and tamsulosin, which are widely regarded as effective α-blockers for MET of ureteral stones, to explore differences in efficacy among α-blockers.
2. Materials and Methods
2.1. Inclusion Criteria
The inclusion criteria were enrollment of patients with ureteral stones; comparison of silodosin and tamsulosin for the treatment of ureteral stones; assessment of outcome measures including stone expulsion rate, stone expulsion time, and complications; and the use of a randomized controlled trial (RCT) design. The exclusion criteria were non-RCT designs; the use of α-blocker combination therapy; studies solely available in abstract, comment, or review format; and publication in languages other than English.
This report conforms to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (Supplement Table S1) [6]. Since systematic reviews and meta-analyses do not need prior approval, neither the institutional review board nor the ethics committee were required to take this study into consideration.
2.2. Search Strategy
A systematic review of the four English-language databases PubMed, EMBASE, the Cochrane Central Register of Controlled Trials (Central), and Web of Science was performed to identify articles published before July 2022 that described comparisons of silodosin versus tamsulosin for MET of ureteral stones. Search strategies included medical subject headings such as “urolithiasis”, “ureterolithiasis”, “ureteral calculi”, “nephrolithiasis”, “medical expulsive therapy”, “tamsulosin”, “silodosin”, and aforementioned terms.
2.3. Study Selection and Data Extraction
To exclude irrelevant studies, the titles and abstracts of articles discovered by the search strategy were separately evaluated by two reviewers (HDJ and DHK). From each study, the articles that were most pertinent were extracted. For included studies, the following information was recorded: author names, year of publication, country, study design, patient characteristics, treatments, and outcome variables (e.g., “stone expulsion rate”, “stone expulsion time”, and “total complication rate”).
2.4. Study Quality Assessment
All RCTs were subjected to risk of bias assessment using the Cochrane risk of bias tool. The qualities of the studies were independently assessed by two reviewers (HDJ and DHK) using the Scottish Intercollegiate Guidelines Network (SIGN) checklist. When two reviewers could not agree on the quality of a study, they discussed with a third reviewer (JYL).
2.5. Statistical Analysis
For dichotomous variables, odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. For continuous variables, weighted mean differences and 95% confidence intervals were calculated. The chi-squared test (with a threshold of p < 0.05) was used to identify statistical heterogeneity, and the I2 statistic was used to quantify heterogeneity [7]. A fixed-effects model was used if the I2 statistic was <50%; otherwise, a random-effects model was used. The Higgins I2 statistic was calculated in the following manner:
where “Q” is the Cochrane heterogeneity statistic, and “df” is the degrees of freedom. Funnel plots and Egger’s test were used to assess the potential for publication bias. Additionally, sensitivity analysis was conducted to identify potential outcome reporting bias. All meta-analyses were conducted using the meta and metasens packages in R software, version 4.1.3 (R Foundation for Statistical Computing, Vienna, Austria; http://www.r-project.org (accessed on 1 September 2022)), as well as Review Manager, version 5.4.1 (RevMan, Copenhagen, Denmark: The Nordic Cochrane Center, The Cochrane Collaboration, 2020). This systematic review was registered in PROSPERO: CRD42022349671.
3. Results
3.1. Eligible Studies
A total of 1912 studies were identified as potentially relevant. Following a full-text review, 14 RCTs and 1552 patients were chosen for inclusion in the meta-analysis (Figure 1).
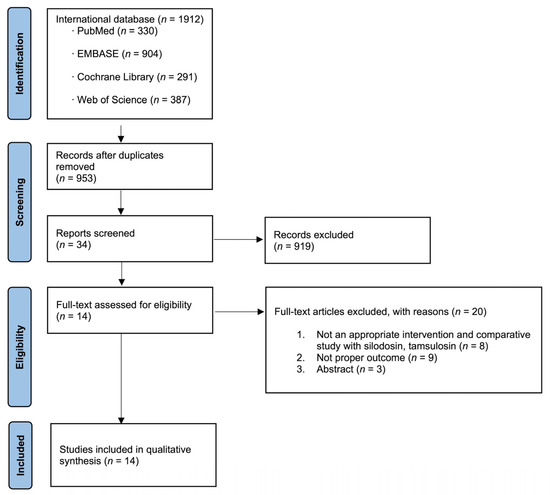
Figure 1.
Study flow chart.
3.2. Characteristic of Included Studies
Table 1 shows the characteristics of the 14 included studies [8,9,10,11,12,13,14,15,16,17,18,19,20,21]. These comparative studies described patients who had received silodosin and tamsulosin for MET of ureteral stones ≤1 cm. There were 11 studies of distal ureteral stones, 1 study of middle or lower ureteral stones, and 2 studies in which the location was not specified. One study comprised an RCT comparing silodosin 4 mg and tamsulosin 0.4 mg [21], while the other studies comprised RCTs comparing silodosin 8 mg and tamsulosin 0.4 mg. All included studies were RCTs published between August 2013 and July 2021.

Table 1.
Characteristics of included studies.
3.3. Quality Assessment
The qualities of the included studies were acceptable, as shown in Table 1. Five studies were rated as 1+ and the remaining nine studies were rated as 1−, according to the SIGN checklist. The risks of bias are shown in Figure 2 and Figure 3; all studies exhibited a reasonable risk of bias.

Figure 2.
Risk of bias graph.
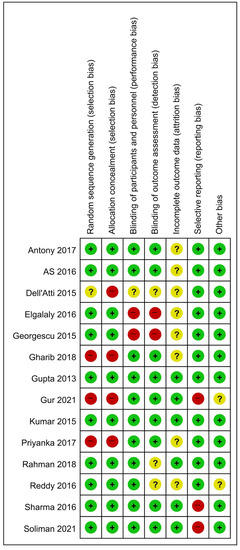
Figure 3.
Risk of bias summary.
3.4. Publication Bias and Heterogeneity Assessment
Funnel plots of the meta-analyses are shown in Figure 4. Little publication bias was identified in Figure 4A,C, whereas some publication bias was identified in Figure 4B. However, Egger’s test showed no evidence of publication bias (Figure 4A, p = 0.40; Figure 4B, p = 0.22; Figure 4C, p = 0.40). Forest plots of the meta-analyses are shown in Figure 5. Little heterogeneities were observed in terms of the stone expulsion rate and total complication rate (Figure 5A, I2 = 0%; Figure 5C, I2 = 7%). Thus, fixed-effects models were used to compare the stone expulsion rate and total complication rate between silodosin and tamsulosin. High heterogeneity was observed in terms of stone expulsion time (Figure 5B, I2 = 89%). After the selection of the effect models, some heterogeneity was also observed in the radial plot of stone expulsion time (Figure 4D). Therefore, a random-effects model was used to compare stone expulsion time between silodosin and tamsulosin. Additionally, to investigate the degree of heterogeneity, a sensitivity analysis of outcome reporting bias was performed. This meta-analysis exhibited robust heterogeneity because the findings concerning stone expulsion time were not affected until at least five studies were excluded (Figure 6).
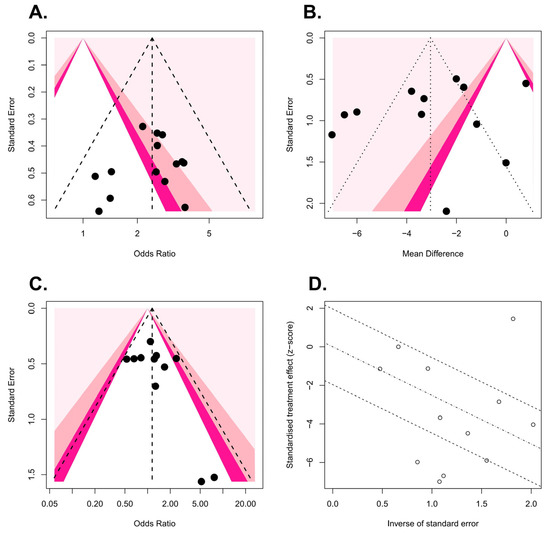
Figure 4.
Funnel plots: (A) stone expulsion rate, (B) stone expulsion time, and (C) total complication rate. Radial plot: (D) stone expulsion time.
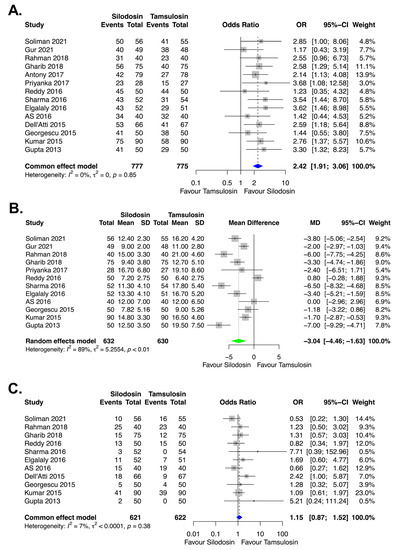
Figure 5.
Forest plots: (A) stone expulsion rate, (B) stone expulsion time, and (C) total complication rate. CI, confidence interval; MD, mean difference; OR, odds ratio; SD, standard deviation.
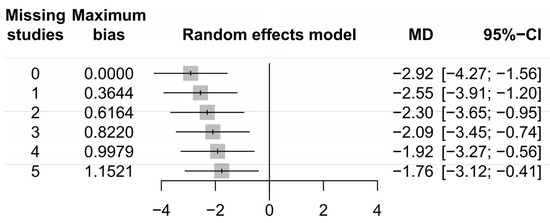
Figure 6.
Sensitivity analysis for outcome reporting bias: stone expulsion time. CI, confidence interval; MD, mean difference.
3.5. Stone Expulsion Rate
The stone expulsion rate was compared between silodosin and tamsulosin in 14 studies [8,9,10,11,12,13,14,15,16,17,18,19,20,21]. The maximum follow-up periods were 2 weeks in one study [11], 3 weeks in one study [13], and 4 weeks in all other studies [8,9,10,12,14,15,16,17,18,19,20,21]. Compared with tamsulosin, silodosin resulted in a significantly higher stone expulsion rate (p < 0.01, OR = 2.42, 95% CI = 1.91 to 3.06, I2 = 0%) (Figure 5A).
3.6. Stone Expulsion Time
The stone expulsion time (in days) was compared between silodosin and tamsulosin in 12 studies [8,9,10,12,14,15,16,17,18,19,20,21]. Compared with tamsulosin, silodosin resulted in a significantly shorter stone expulsion time (p < 0.01, mean difference (MD) = −3.04, 95% CI = −4.46 to −1.63, I2 = 89%) (Figure 5B).
3.7. Total Complication Rate
The total complication rate was compared between silodosin and tamsulosin in 11 studies [9,10,12,13,14,15,16,17,19,20,21]. The following complications were analyzed: orthotopic hypotension, headache, dizziness, nasal congestion, nausea, backache, retrograde ejaculation, and diarrhea. The total complication rate did not significantly differ between silodosin and tamsulosin (p = 0.33, OR = 1.15, 95% CI = 0.87 to 1.52, I2 = 7%) (Figure 5C).
4. Discussion
The COVID-19 pandemic continues to impact public health worldwide [22]. Pandemic-related shortages of hospital beds and healthcare workers have made it challenging to treat patients with common diseases [23]. Outbreaks of COVID-19 have led to hospital staffing difficulties and increased use of hospital resources for the treatment of affected patients [24]. During the Omicron variant surge, for example, the 7-day moving average of hospitals with critical staffing shortages reached nearly 22%, whereas the 7-day moving average of COVID-19 inpatient beds peaked 1–2 weeks later at approximately 21% [25].
Thus, the EAU Guidelines Office Rapid Reaction Group suggested adaptations of the EAU guidelines for use in the COVID-19 era [26]. According to these recommendations, MET and minimal interventional treatment should be used when possible to avoid surgical intervention during outbreaks of COVID-19.
Current guidelines for MET mainly recommend the use of α-blockers, rather than other drugs [4,5]. Calcium channel inhibitors (e.g., nifedipine) demonstrated efficacy in terms of stone expulsion and renal colic alleviation [27,28], but these effects were weaker than the effects of tamsulosin for distal ureteral stones [29]. Combination MET using phosphodiesterase-5 inhibitors or corticosteroids with α-blockers is not recommended because the available data were collected from studies that involved small numbers of patients [4,30].
For the first time, Borghi et al. [31] conducted an RCT of MET for ureteral stones ≤15 mm; they compared nifedipine 40 mg plus methylprednisolone 16 mg daily (group 1), with methylprednisolone 16 mg plus placebo daily (group 2). The success rate was higher in group 1 (87%, 34/39) than in group 2 (65%, 13/24). Parsons et al. [32] conducted the first meta-analysis regarding the clinical effectiveness of α-blockers for treatment of distal ureteral stones; the rate of spontaneous stone passage was 44% greater in patients receiving α-blockers (10 studies, tamsulosin 0.4 mg; 2 studies, terazosin 5 mg; 1 study, doxazosin 4 mg) than in patients who did not receive such treatment.
In a Cochrane review to compare the effectiveness of α-blockers with placebo for treatment of ureteral stones ≤10 mm, α-blockers alleviated renal colic (MD = −0.66, 95% CI: −0.91 to −0.42; p < 0.001; I2 = 80%) and facilitated ureteral stone expulsion (risk ratio = 1.45, 95% CI: 1.36 to 0.55; p < 0.001; I2 = 76%). Subgroup analysis according to α-blocker type (tamsulosin, alfuzosin, terazosin, naftopidil, or silodosin) showed no significant difference (χ2 = 1.44, I2 = 46.1%, p = 0.13) [27].
To determine the effects of specific classes of α-blockers, Yilmaz et al. [33] conducted an RCT comparing tamsulosin, terazosin, and doxazosin for MET of distal ureteral stones. Their study showed that stone expulsion rates were comparable among all three drugs.
α-blockers function through the following mechanism. The most widespread subtypes of a1-adrenoceptors in the distal ureter are α1a- and α1d-adrenoceptors. These α1-adrenoceptors are stimulated, which increases frequency and the force of ureteral contractions. However, inhibition of these receptors reduces basal ureteral tone, as well as peristaltic frequency and amplitude; these changes reduce intraluminal pressure while enhancing the rate of urine transport, thereby increasing the likelihood of stone passage [34].
Itoh et al. [35] reported that, in the human ureter, the expression of α1d-adrenoceptors was greater than the expression of α1a-adrenoceptors. Additionally, Tomiyama et al. [36] investigated α1-adrenoceptor subtypes in the hamster ureter according to gene and protein expression patterns, as well as contractile function. They found that α1d-adrenoceptors were more prevalent than α1a-adrenoceptors, but ureteral smooth muscle contraction was mainly mediated by α1a-adrenoceptors. Subsequently, Sasaki et al. [37] reported that α1a-adrenoceptors were the main receptors involved in phenylephrine-induced contraction in the human ureter, suggesting that α1a-adrenoceptors have a central role in contraction in the human ureter.
Thus, Itoh et al. [38] conducted the first prospective RCT of silodosin for MET of ureteral stones <10 mm. Compared with patients instructed to consume 2 L of water daily, patients who received silodosin 8 mg daily exhibited a shorter mean stone expulsion time and higher stone expulsion rate. Since that RCT of silodosin, meta-analyses have shown that silodosin is more potent than tamsulosin for MET of ureteral stones [39,40]. In a meta-analysis with five RCTs, Liu et al. [40] found that silodosin significantly increased the expulsion rate of distal ureteral stones, compared with tamsulosin, but there was no significant difference between treatments in terms of stone expulsion time or retrograde ejaculation rate. Hsu et al. [39] conducted a meta-analysis with 13 RCTs (including 2 RCTs solely available in abstract format) and 3 observational studies. They found that, compared with tamsulosin, silodosin resulted in a higher stone expulsion rate and shorter expulsion time; however, silodosin also led to a higher incidence of retrograde ejaculation.
Here, we conducted an updated systematic review and meta-analysis of 14 RCTs to compare the efficacies and safety profiles of silodosin and tamsulosin for MET of ureteral stones ≤1 cm. We found that, compared with tamsulosin, silodosin resulted in a higher stone expulsion rate and shorter stone expulsion time. Moreover, we found no difference in the total complication rate between silodosin and tamsulosin.
Experimental studies have demonstrated that α1a-adrenoceptors are the main receptors involved in contraction in the human ureter. Furthermore, the results of previous meta-analyses and our meta-analysis suggest that silodosin is superior to tamsulosin for MET of ureteral stones.
This updated systematic review and meta-analysis had some limitations. First, one of the analyzed studies comprised an RCT conducted with silodosin 4 mg [21], whereas other studies were RCTs conducted with silodosin 8 mg. Despite the lower dose of silodosin, the study involving silodosin 4 mg showed that the stone expulsion rate was higher and the stone expulsion time was shorter with silodosin than with tamsulosin. Silodosin 4 mg also performed better than tamsulosin in terms of the total complication rate, which might have influenced the meta-analysis finding of no significant difference in the total complication rate. Second, we could not conduct subgroup analysis according to ureteral stone location because 11 studies focused on distal ureteral stones, 1 study focused on middle or lower ureteral stones, and 2 studies focused on an unspecified location. Third, we could not conduct subgroup analysis by dividing ureteral stones according to size (e.g., ≤5 mm and 5–10 mm). Although five studies had inclusion criteria of ureteral stone size 5–10 mm, the remaining nine studies had inclusion criteria of ureteral stone size <10 mm and did not separately evaluate ureteral stones ≤5 mm.
5. Conclusions
This updated systematic review and meta-analysis of RCTs showed that, compared with tamsulosin, silodosin performed significantly better in the expulsion of ureteral stones <1 cm. The total complication rate did not differ between silodosin and tamsulosin. Thus, silodosin may be preferable to tamsulosin for MET of ureteral stones <1 cm.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/1648-9144/58/12/1794/s1, Table S1: PRISMA Checklist.
Author Contributions
Conceptualization, J.Y.L. and K.S.C.; methodology, J.Y.L. and K.S.C.; software, H.D.J. and D.Y.J.; validation, J.Y.L. and D.H.K.; formal analysis, J.Y.J. and H.D.J.; investigation, Y.J.M. and H.D.J.; resources, J.Y.L. and K.S.C.; data curation, D.H.K. and H.D.J.; writing—original draft preparation, H.D.J.; writing—review and editing, J.Y.L.; visualization, D.Y.C. and S.C.; supervision, K.S.C.; project administration, J.Y.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was exempt from requiring the approval of an ethics committee or institutional review board because of systematic review and meta-analysis.
Informed Consent Statement
Patient consent was waived because this paper is a systematic review and meta-analysis.
Data Availability Statement
The data presented in this study are available in the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jung, H.D.; Seo, I.Y.; Lee, J.Y. Large database study of urinary stone composition in south korea: Korean society of endourology and robotics (kser) research series. Investig. Clin. Urol. 2021, 62, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.Y.; Jung, H.D.; Kwon, S.H.; Lee, E.K.; Lee, J.Y.; Lee, S.H. Does early retrograde intrarenal surgery improve the cost-effectiveness of renal stone management? Yonsei Med. J. 2020, 61, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Tefik, T.; Guven, S.; Villa, L.; Gokce, M.I.; Kallidonis, P.; Petkova, K.; Kiremit, M.C.; Sonmez, M.G.; de Lorenzis, E.; Eryildirim, B.; et al. Urolithiasis practice patterns following the COVID-19 pandemic: Overview from the eulis collaborative research working group. Eur. Urol. 2020, 78, e21–e24. [Google Scholar] [CrossRef] [PubMed]
- Türk, C.; Skolarikos, A.; Neisius, A.; Petrik, A.; Seitz, C.; Thomas, K. EAU guidelines on urolithiasis, EAU guidelines. In Proceedings of the EAU Annual Congress Amsterdam 2020, Amsterdam, The Netherlands, 20–24 March 2020. [Google Scholar]
- Assimos, D.; Krambeck, A.; Miller, N.L.; Monga, M.; Murad, M.H.; Nelson, C.P.; Pace, K.T.; Pais, V.M., Jr.; Pearle, M.S.; Preminger, G.M.; et al. Surgical management of stones: American urological association/endourological society guideline, part ii. J. Urol. 2016, 196, 1161–1169. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Priyanka, P.; Jadhav, R.R. Comparison between tamsulosin and silodosin in lower ureteric stone—A randomised controlled study. J. Evol. Med. Dent. Sci. 2017, 6, 6766–6769. [Google Scholar] [CrossRef]
- Reddy, S.; Prathvi, P.; Kulshreshtha, M.; Singh, P. A prospective study comparing tamsulosin and silodosin in medical expulsive therapy for lower ureteric stones. J. Evol. Med. Dent. Sci. 2016, 5, 4108–4111. [Google Scholar] [CrossRef]
- Sharma, G.; Khadav, B.; Sandhasukhi, T.C.; Gupta, M.; Gupta, H.L. Comparative analysis of silodosin and tamsulosin in distal ureteric calculus treatment. J. Evid. Based Med. Healthc 2016, 3, 4647–4649. [Google Scholar] [CrossRef] [PubMed]
- Antony, D. Comparative efficacy of silodosin vs tamsulosin for ureteric calculus: A single centre double blind randomised controlled trial. J. Med. Sci. Clin. Res. 2017, 5, 31928–31932. [Google Scholar] [CrossRef]
- AS, A.; Pillai, S.R.; Mary, A.; Aravindakshan, R. Efficacy of tamsulosin and silodosin as medical expulsive therapy in the management of distal ureteral stones: A randomized controlled study. Int. Surg. J. 2016, 3, 4. [Google Scholar] [CrossRef]
- Dell’Atti, L. Silodosin versus tamsulosin as medical expulsive therapy for distal ureteral stones: A prospective randomized study. Urologia 2015, 82, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Elgalaly, H.; Sakr, A.; Fawzi, A.; Salem, E.A.; Desoky, E.; Shahin, A.; Kamel, M. Silodosin vs tamsulosin in the management of distal ureteric stones: A prospective randomised study. Arab J. Urol. 2016, 14, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Georgescu, D.; Ionita Radu, F.; Multescu, R.; Dragutescu, M.; Geavlete, B.; Geavlete, P.; Negrei, C.; Mischianu, D.; Georgescu, M.; Ginghina, O. The role of alpha 1-blockers in the medical expulsive therapy for ureteral calculi—A prospective controlled randomized study comparing tamsulosin and silodosint. Farmacia 2015, 63, 184–188. [Google Scholar]
- Gharib, T.; Mohey, A.; Fathi, A.; Alhefnawy, M.; Alazaby, H.; Eldakhakhny, A. Comparative study between silodosin and tamsulosin in expectant therapy of distal ureteral stones. Urol. Int. 2018, 101, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Lodh, B.; Singh, A.K.; Somarendra, K.; Meitei, K.S.; Singh, S.R. Comparing the efficacy of tamsulosin and silodosin in the medical expulsion therapy for ureteral calculi. J. Clin. Diagn. Res. 2013, 7, 1672–1674. [Google Scholar] [CrossRef]
- Gur, M.; Ulu, M.B.; Caliskan, S.T.; Ozturk, K.; Akdeniz, E. Dexketoprofen vs. Tamsulosin vs. Silodosin vs. Tadalafil as medical expulsive therapy for distal ureteral stones in men. J. Coll. Physicians Surg. Pak. 2021, 31, 947–952. [Google Scholar]
- Kumar, S.; Jayant, K.; Agrawal, M.M.; Singh, S.K.; Agrawal, S.; Parmar, K.M. Role of tamsulosin, tadalafil, and silodosin as the medical expulsive therapy in lower ureteric stone: A randomized trial (a pilot study). Urology 2015, 85, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.J.; Faridi, M.S.; Mibang, N.; Singh, R.S. Comparing tamsulosin, silodosin versus silodosin plus tadalafil as medical expulsive therapy for lower ureteric stones: A randomised trial. Arab J. Urol. 2018, 16, 245–249. [Google Scholar] [CrossRef]
- Soliman, M.G.; El-Gamal, O.; El-Gamal, S.; Abdel Raheem, A.; Abou-Ramadan, A.; El-Abd, A. Silodosin versus tamsulosin as medical expulsive therapy for children with lower-third ureteric stones: Prospective randomized placebo-controlled study. Urol. Int. 2021, 105, 568–573. [Google Scholar] [CrossRef]
- Zoumpourlis, V.; Goulielmaki, M.; Rizos, E.; Baliou, S.; Spandidos, D.A. [comment] the COVID-19 pandemic as a scientific and social challenge in the 21st century. Mol. Med. Rep. 2020, 22, 3035–3048. [Google Scholar] [CrossRef] [PubMed]
- Shin, W.Y.; Kim, C.; Lee, S.Y.; Lee, W.; Kim, J.H. Role of primary care and challenges for public-private cooperation during the coronavirus disease 2019 pandemic: An expert delphi study in south korea. Yonsei Med. J. 2021, 62, 660–669. [Google Scholar] [CrossRef]
- Kim, J.; Gewertz, B. Teleurology and digital health app in COVID-19 pandemic. Investig. Clin. Urol. 2020, 61, 333–334. [Google Scholar] [CrossRef]
- Impact of the COVID-19 Pandemic on the Hospital and Outpatient Clinician Workforce: Challenges and Policy Responses (issue brief no. Hp-2022-13); Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services: Washington, DC, USA, 2022.
- Ribal, M.J.; Cornford, P.; Briganti, A.; Knoll, T.; Gravas, S.; Babjuk, M.; Harding, C.; Breda, A.; Bex, A.; Rassweiler, J.J.; et al. European association of urology guidelines office rapid reaction group: An organisation-wide collaborative effort to adapt the european association of urology guidelines recommendations to the coronavirus disease 2019 era. Eur. Urol. 2020, 78, 21–28. [Google Scholar] [CrossRef]
- Campschroer, T.; Zhu, X.; Vernooij, R.W.M.; Lock, T. A-blockers as medical expulsive therapy for ureteric stones: A cochrane systematic review. BJU Int. 2018, 122, 932–945. [Google Scholar] [CrossRef] [PubMed]
- Seitz, C.; Liatsikos, E.; Porpiglia, F.; Tiselius, H.G.; Zwergel, U. Medical therapy to facilitate the passage of stones: What is the evidence? Eur. Urol. 2009, 56, 455–471. [Google Scholar] [CrossRef]
- Wang, H.; Man, L.B.; Huang, G.L.; Li, G.Z.; Wang, J.W. Comparative efficacy of tamsulosin versus nifedipine for distal ureteral calculi: A meta-analysis. Drug. Des. Devel. 2016, 10, 1257–1265. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Yang, Y.; Wang, X.; Tang, Y.; Han, P.; Wang, J. Tadalafil facilitates the distal ureteral stone expulsion: A meta-analysis. J. Endourol. 2017, 31, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Borghi, L.; Meschi, T.; Amato, F.; Novarini, A.; Giannini, A.; Quarantelli, C.; Mineo, F. Nifedipine and methylprednisolone in facilitating ureteral stone passage: A randomized, double-blind, placebo-controlled study. J. Urol. 1994, 152, 1095–1098. [Google Scholar] [CrossRef]
- Parsons, J.K.; Hergan, L.A.; Sakamoto, K.; Lakin, C. Efficacy of alpha-blockers for the treatment of ureteral stones. J. Urol. 2007, 177, 983–987, discussion 987. [Google Scholar] [CrossRef]
- Yilmaz, E.; Batislam, E.; Basar, M.M.; Tuglu, D.; Ferhat, M.; Basar, H. The comparison and efficacy of 3 different alpha1-adrenergic blockers for distal ureteral stones. J. Urol. 2005, 173, 2010–2012. [Google Scholar] [CrossRef] [PubMed]
- Griwan, M.S.; Singh, S.K.; Paul, H.; Pawar, D.S.; Verma, M. The efficacy of tamsulosin in lower ureteral calculi. Urol. Ann. 2010, 2, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Itoh, Y.; Kojima, Y.; Yasui, T.; Tozawa, K.; Sasaki, S.; Kohri, K. Examination of alpha 1 adrenoceptor subtypes in the human ureter. Int. J. Urol. 2007, 14, 749–753. [Google Scholar] [CrossRef]
- Tomiyama, Y.; Kobayashi, K.; Tadachi, M.; Kobayashi, S.; Inada, Y.; Kobayashi, M.; Yamazaki, Y. Expressions and mechanical functions of alpha1-adrenoceptor subtypes in hamster ureter. Eur. J. Pharm. 2007, 573, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Tomiyama, Y.; Kobayashi, S.; Kojima, Y.; Kubota, Y.; Kohri, K. Characterization of α1-adrenoceptor subtypes mediating contraction in human isolated ureters. Urology 2011, 77, 762.e13–762.e17. [Google Scholar] [CrossRef] [PubMed]
- Itoh, Y.; Okada, A.; Yasui, T.; Hamamoto, S.; Hirose, M.; Kojima, Y.; Tozawa, K.; Sasaki, S.; Kohri, K. Efficacy of selective α1a adrenoceptor antagonist silodosin in the medical expulsive therapy for ureteral stones. Int. J. Urol. 2011, 18, 672–674. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.P.; Hsu, C.W.; Bai, C.H.; Cheng, S.W.; Chen, K.C.; Chen, C. Silodosin versus tamsulosin for medical expulsive treatment of ureteral stones: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0203035. [Google Scholar] [CrossRef]
- Liu, X.J.; Wen, J.G.; Wan, Y.D.; Hu, B.W.; Wang, Q.W.; Wang, Y. Role of silodosin as medical expulsive therapy in ureteral calculi: A meta-analysis of randomized controlled trials. Urolithiasis 2018, 46, 211–218. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).