
Relationship between Recovery from COVID-19-Induced Smell Loss and General and Oral Health Factors


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Survey Design and Dissemination
2.3. Sample Size and Statistical Power
2.4. Data Gathering and Processing
2.5. Statistical Analyses
3. Results
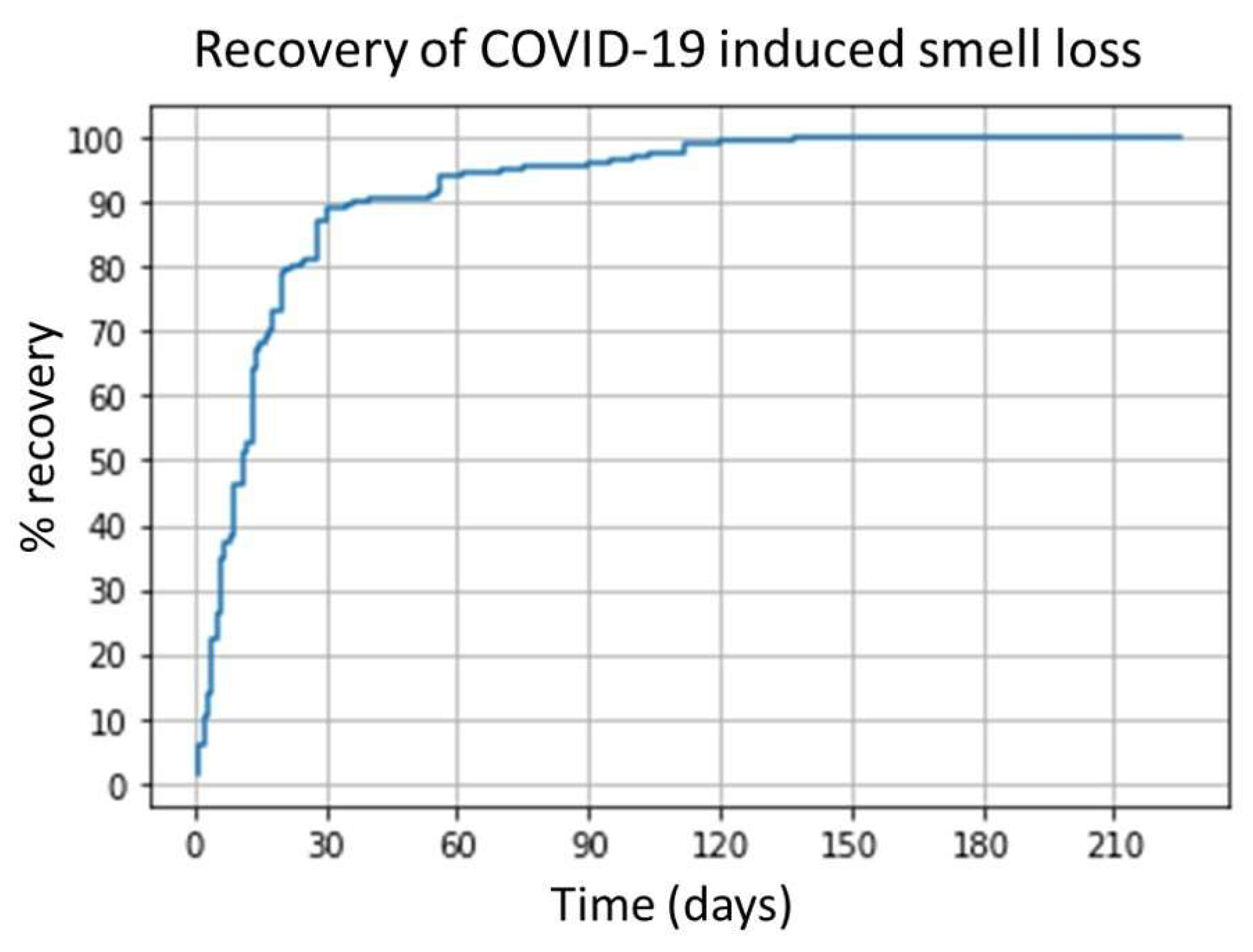
3.1. Resolution of Smell Loss
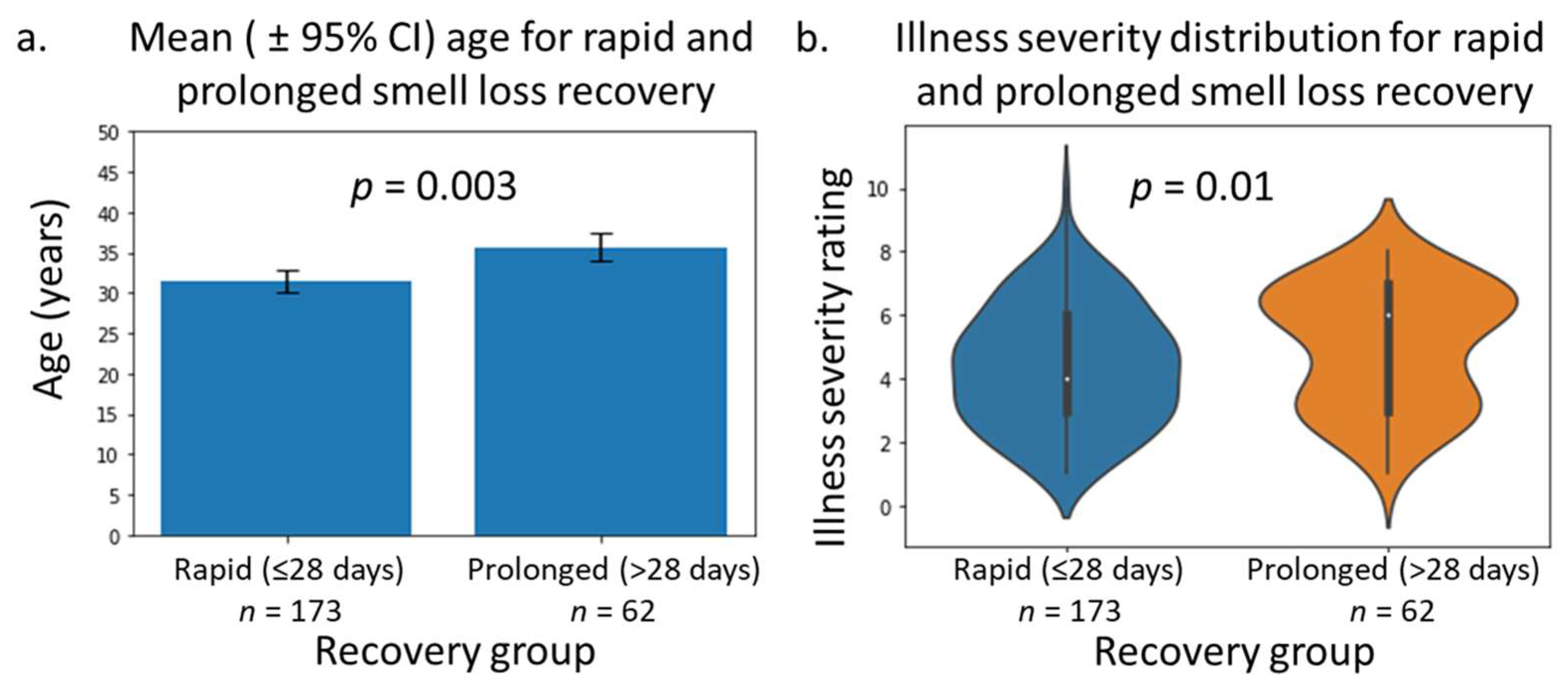
3.2. Differences between Rapid (≤28 Days) and Prolonged (>28 Days) Recovery
4. Discussion
4.1. Pattern of Smell Recovery
4.2. Differences between Rapid and Prolonged Recovery
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lechien, J.R.; Journe, F.; Hans, S.; Chiesa-Estomba, C.M.; Mustin, V.; Beckers, E.; Vaira, L.A.; De Riu, G.; Hopkins, C.; Saussez, S. Severity of anosmia as an early symptom of COVID-19 infection may predict lasting loss of smell. Front. Med. 2020, 7, 582802. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Valdes, A.M.; Freidin, M.B.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Ganesh, S.; Varavsky, T.; Cardoso, M.J.; El-Sayed Moustafa, J.S.; et al. Real-time tracking of self-reported symptoms to predict potential COVID-19. Nat. Med. 2020, 26, 1037–1040. [Google Scholar] [CrossRef] [PubMed]
- Klein, H.; Asseo, K.; Karni, N.; Benjamini, Y.; Nir-Paz, R.; Muszkat, M.; Israel, S.; Niv, M.Y. Onset, duration and unresolved symptoms, including smell and taste changes, in mild COVID-19 infection: A cohort study in Israeli patients. Clin. Microbiol. Infect. 2020, 27, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Keshet, A.; Graham, M.S.; Joshi, A.D.; Shilo, S.; Rossman, H.; Murray, B.; Molteni, E.; Klaser, K.; Canas, L.D. Anosmia, ageusia, and other COVID-19-like symptoms in association with a positive SARS-CoV-2 test, across six national digital surveillance platforms: An observational study. Lancet Digit. Health 2021, 3, e577–e586. [Google Scholar] [CrossRef]
- George, B.; McGee, J.; Giangrasso, E.; Finkelstein, S.; Wu, S.; Glatt, A.E. What Is the Predictive Value of a Single Nasopharyngeal SARS-CoV-2 PCR Swab Test in a Patient With COVID-Like Symptoms and/or Significant COVID-19 Exposure? Open Forum Infect. Dis. 2020, 7, ofaa399. [Google Scholar] [CrossRef]
- Ibekwe, T.S.; Fasunla, A.J.; Orimadegun, A.E. Systematic review and meta-analysis of smell and taste disorders in COVID-19. OTO Open 2020, 4, 2473974X20957975. [Google Scholar] [CrossRef]
- Agyeman, A.A.; Chin, K.L.; Landersdorfer, C.B.; Liew, D.; Ofori-Asenso, R. Smell and taste dysfunction in patients with COVID-19: A systematic review and meta-analysis. Mayo Clin. Proc. 2020, 8, 1621–1631. [Google Scholar] [CrossRef]
- Gorna, R.; MacDermott, N.; Rayner, C.; O’Hara, M.; Evans, S.; Agyen, L.; Nutland, W.; Rogers, N.; Hastie, C. Long COVID guidelines need to reflect lived experience. Lancet 2021, 397, 455–457. [Google Scholar] [CrossRef]
- Carvalho-Schneider, C.; Laurent, E.; Lemaignen, A.; Beaufils, E.; Bourbao-Tournois, C.; Laribi, S.; Flament, T.; Ferreira-Maldent, N.; Bruyère, F.; Stefic, K. Follow-up of adults with noncritical COVID-19 two months after symptom onset. Clin. Microbio. Infect. 2021, 27, 258–263. [Google Scholar] [CrossRef]
- Eshraghi, A.A.; Mirsaeidi, M.; Davies, C.; Telischi, F.F.; Chaudhari, N.; Mittal, R. Potential mechanisms for COVID-19 induced anosmia and dysgeusia. Front. Physiol. 2020, 11, 1039. [Google Scholar] [CrossRef]
- Sinjari, B.; D’Ardes, D.; Santilli, M.; Rexhepi, I.; D’Addazio, G.; Di Carlo, P.; Chiacchiaretta, P.; Caputi, S.; Cipollone, F. SARS-CoV-2 and Oral Manifestation: An Observational, Human Study. J. Clin. Med. 2020, 9, 3218. [Google Scholar] [CrossRef] [PubMed]
- Gori, A.; Leone, F.; Loffredo, L.; Cinicola, B.L.; Brindisi, G.; De Castro, G.; Spalice, A.; Duse, M.; Zicari, A.M. COVID-19-Related Anosmia: The Olfactory Pathway Hypothesis and Early Intervention. Front. Neurol. 2020, 11, 956. [Google Scholar] [CrossRef] [PubMed]
- Mercante, G.; Ferreli, F.; De Virgilio, A.; Gaino, F.; Di Bari, M.; Colombo, G.; Russo, E.; Costantino, A.; Pirola, F.; Cugini, G. Prevalence of taste and smell dysfunction in coronavirus disease 2019. JAMA Otolaryngol. Head. Neck. 2020, 146, 723–728. [Google Scholar] [CrossRef] [PubMed]
- Shatz, I. Fast, free, and targeted: Reddit as a source for recruiting participants online. Soc. Sci. Comput. Rev. 2017, 35, 537–549. [Google Scholar] [CrossRef]
- Lauc, G.; Sinclair, D. Biomarkers of biological age as predictors of COVID-19 disease severity. Aging 2020, 12, 6490. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, A.; Olsson, P.-E. Sex differences in severity and mortality from COVID-19: Are males more vulnerable? Biol. Sex. Differ. 2020, 11, 53. [Google Scholar] [CrossRef]
- Popkin, B.M.; Du, S.; Green, W.D.; Beck, M.A.; Algaith, T.; Herbst, C.H.; Alsukait, R.F.; Alluhidan, M.; Alazemi, N.; Shekar, M. Individuals with obesity and COVID-19: A global perspective on the epidemiology and biological relationships. Obes. Rev. 2020, 21, e13128. [Google Scholar] [CrossRef]
- Zabetakis, I.; Lordan, R.; Norton, C.; Tsoupras, A. COVID-19: The inflammation link and the role of nutrition in potential mitigation. Nutrients 2020, 12, 1466. [Google Scholar] [CrossRef]
- Xu, Y.; Baylink, D.J.; Chen, C.-S.; Reeves, M.E.; Xiao, J.; Lacy, C.; Lau, E.; Cao, H. The importance of vitamin d metabolism as a potential prophylactic, immunoregulatory and neuroprotective treatment for COVID-19. J. Transl. Med. 2020, 18, 322. [Google Scholar] [CrossRef]
- Saengow, U.; Assanangkornchai, S.; Casswell, S. Alcohol: A probable risk factor of COVID-19 severity. Addiction 2020, 116, 204–205. [Google Scholar] [CrossRef]
- Patanavanich, R.; Glantz, S.A. Smoking is associated with COVID-19 progression: A meta-analysis. Nicotine Tob. Res. 2020, 22, 1653–1656. [Google Scholar] [CrossRef] [PubMed]
- Vennemann, M.M.; Hummel, T.; Berger, K. The association between smoking and smell and taste impairment in the general population. J. Neurol. 2008, 255, 1121–1126. [Google Scholar] [CrossRef] [PubMed]
- Neyraud, E.; Morzel, M. Biological films adhering to the oral soft tissues: Structure, composition, and potential impact on taste perception. J. Texture Stud. 2019, 50, 19–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, M.; Canon, F.; Feron, G.; Neiers, F.; Gamero, A. Impact of oral microbiota on flavor perception: From food processing to in-mouth metabolization. Foods 2021, 10, 2006. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, L.E.; Robertson, D.; Nile, C.J.; Cross, L.J.; Riggio, M.; Sherriff, A.; Bradshaw, D.; Lambert, M.; Malcolm, J.; Buijs, M.J. The oral microbiome of denture wearers is influenced by levels of natural dentition. PLoS ONE 2015, 10, e0137717. [Google Scholar] [CrossRef]
- Koskinen, K.; Reichert, J.L.; Hoier, S.; Schachenreiter, J.; Duller, S.; Moissl-Eichinger, C.; Schöpf, V. The nasal microbiome mirrors and potentially shapes olfactory function. Sci. Rep. 2018, 8, 1296. [Google Scholar] [CrossRef] [Green Version]
- Feehan, A.K.; Rose, R.; Nolan, D.J.; Spitz, A.M.; Graubics, K.; Colwell, R.R.; Garcia-Diaz, J.; Lamers, S.L. Nasopharyngeal Microbiome Community Composition and Structure Is Associated with Severity of COVID-19 Disease and Breathing Treatment. Appl. Microbiol. 2021, 1, 177–188. [Google Scholar] [CrossRef]
- Atukorallaya, D.S.; Ratnayake, R.K. Oral Mucosa, Saliva, and COVID-19 Infection in Oral Health Care. Front. Med. 2021, 8, 340. [Google Scholar] [CrossRef]
- Islam, M.R. Sample size and its role in Central Limit Theorem (CLT). J. Computat. Appl. Math. 2018, 4, 1–7. [Google Scholar]
- Lee, Y.; Min, P.; Lee, S.; Kim, S.-W. Prevalence and duration of acute loss of smell or taste in COVID-19 patients. J. Korean Med. Sci. 2020, 35, e174. [Google Scholar] [CrossRef]
- Song, J.; Deng, Y.K.; Wang, H.; Wang, Z.C.; Liao, B.; Ma, J.; He, C.; Pan, L.; Liu, Y.; Alobid, I.; et al. Self-reported taste and smell disorders in patients with COVID-19: Distinct features in China. Curr. Med. Sci. 2021, 41, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.K.C.; Gendeh, H.S.; Thong, H.K.; Lum, S.G.; Gendeh, B.S.; Saim, A.; Salina, H. A review of smell and taste dysfunction in COVID-19 patients. Med. J. Malaysia 2020, 75, 574–581. [Google Scholar] [PubMed]
- Dell’Era, V.; Farri, F.; Garzaro, G.; Gatto, M.; Aluffi Valletti, P.; Garzaro, M. Smell and taste disorders during COVID-19 outbreak: Cross-sectional study on 355 patients. Head Neck 2020, 42, 1591–1596. [Google Scholar] [CrossRef] [PubMed]
- Printza, A.; Katotomichelakis, M.; Valsamidis, K.; Metallidis, S.; Panagopoulos, P.; Panopoulou, M.; Petrakis, V.; Constantinidis, J. Smell and Taste Loss Recovery Time in COVID-19 Patients and Disease Severity. J. Clin. Med. 2021, 10, 966. [Google Scholar] [CrossRef] [PubMed]
- Coelho, D.H.; Reiter, E.R.; Budd, S.G.; Shin, Y.; Kons, Z.A.; Costanzo, R.M. Predictors of smell recovery in a nationwide prospective cohort of patients with COVID-19. Am. J. Otolaryngol. 2022, 43, 103239. [Google Scholar] [CrossRef]
- Schwab, J.; Jensen, C.D.; Fjaeldstad, A.W. Sustained Chemosensory Dysfunction during the COVID-19 Pandemic. ORL 2021, 83, 209–218. [Google Scholar] [CrossRef]
- Chary, E.; Carsuzaa, F.; Trijolet, J.-P.; Capitaine, A.-L.; Roncato-Saberan, M.; Fouet, K.; Cazenave-Roblot, F.; Catroux, M.; Allix-Beguec, C.; Dufour, X. Prevalence and recovery from olfactory and gustatory dysfunctions in Covid-19 infection: A prospective multicenter study. Am. J. Rhinol. Allergy 2020, 34, 686–693. [Google Scholar] [CrossRef]
- Chapurin, N.; Totten, D.J.; Chaballout, B.; Brennan, J.; Dennis, S.; Lubner, R.; Chowdhury, N.I.; Turner, J.H.; Trone, T.; Chandra, R.K. Differential olfactory outcomes in COVID-19: A large healthcare system population study. Int. Forum Allergy Rhinol. 2022, 12, 108–111. [Google Scholar] [CrossRef]
- Marouf, N.; Cai, W.; Said, K.N.; Daas, H.; Diab, H.; Chinta, V.R.; Hssain, A.A.; Nicolau, B.; Sanz, M.; Tamimi, F. Association between periodontitis and severity of COVID-19 infection: A case–control study. J. Clin Periodontol. 2021, 48, 483–491. [Google Scholar] [CrossRef]
- Gupta, S.; Mohindra, R.; Singla, M.; Khera, S.; Sahni, V.; Kanta, P.; Soni, R.K.; Kumar, A.; Gauba, K.; Goyal, K.; et al. The clinical association between Periodontitis and COVID-19. Clin. Oral Investig. 2021, 126, 1361–1374. [Google Scholar] [CrossRef]
- Kamel, A.H.M.; Basuoni, A.; Salem, Z.A.; AbuBakr, N. The impact of oral health status on COVID-19 severity, recovery period and C-reactive protein values. Br. Dent. J. 2021, 24, 1–7. [Google Scholar] [CrossRef]
- Cazzolla, A.P.; Lovero, R.; Lo Muzio, L.; Testa, N.F.; Schirinzi, A.; Palmieri, G.; Pozzessere, P.; Procacci, V.; Di Comite, M.; Ciavarella, D. Taste and smell disorders in COVID-19 patients: Role of interleukin-6. ACS Chem. Neurosci. 2020, 11, 2774–2781. [Google Scholar] [CrossRef] [PubMed]
- Worthington, H.V.; MacDonald, L.; Pericic, T.P.; Sambunjak, D.; Johnson, T.M.; Imai, P.; Clarkson, J.E. Home use of interdental cleaning devices, in addition to toothbrushing, for preventing and controlling periodontal diseases and dental caries. Cochrane Database Syst. Rev. 2019, 4, 1–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graves, R.C.; Disney, J.A.; Stamm, J.W. Comparative effectiveness of flossing and brushing in reducing interproximal bleeding. J. Periodontol. 1989, 60, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Pitones-Rubio, V.; Chávez-Cortez, E.G.; Hurtado-Camarena, A.; González-Rascón, A.; Serafín-Higuera, N. Is periodontal disease a risk factor for severe COVID-19 illness? Med. Hypotheses 2020, 144, 109969. [Google Scholar] [CrossRef]
- Shoemark, D.K.; Allen, S.J. The microbiome and disease: Reviewing the links between the oral microbiome, aging, and Alzheimer’s disease. J. Alzheimer’s Dis. 2015, 43, 725–738. [Google Scholar] [CrossRef] [Green Version]
- D’Ercole, S.; D’Addazio, G.; Di Lodovico, S.; Traini, T.; Di Giulio, M.; Sinjari, B. Porphyromonas Gingivalis Load is Balanced by 0.20% Chlorhexidine Gel. A Randomized, Double-Blind, Controlled, Microbiological and Immunohistochemical Human Study. J. Clin. Med. 2020, 9, 284. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, G.; Thimmappa, L.; Upadhya, N.; Carnelio, S. Could mouth rinses be an adjuvant in the treatment of SARS-CoV-2 patients? An appraisal with a systematic review. Int. J. Dent. Hyg. 2021, 20, 136–144. [Google Scholar] [CrossRef]
- Helms, J.A.; Della-Fera, M.A.; Mott, A.E.; Frank, M.E. Effects of chlorhexidine on human taste perception. Arch. Oral Biol. 1995, 40, 913–920. [Google Scholar] [CrossRef]
- Hannum, M.E.; Ramirez, V.A.; Lipson, S.J.; Herriman, R.D.; Toskala, A.K.; Lin, C.; Joseph, P.V.; Reed, D.R. Objective Sensory Testing Methods Reveal a Higher Prevalence of Olfactory Loss in COVID-19–Positive Patients Compared to Subjective Methods: A Systematic Review and Meta-Analysis. Chem. Senses 2020, 45, 865–874. [Google Scholar] [CrossRef]
- Printza, A.; Constantinidis, J. The role of self-reported smell and taste disorders in suspected COVID-19. Eur. Arch. Oto-Rhino-L. 2020, 277, 2625–2630. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, C.; Surda, P.; Vaira, L.A.; Lechien, J.R.; Safarian, M.; Saussez, S.; Kumar, N. Six month follow-up of self-reported loss of smell during the COVID-19 pandemic. Rhinology 2021, 59, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Borsetto, D.; Hopkins, C.; Philips, V.; Obholzer, R.; Tirelli, G.; Polesel, J.; Boscolo-Rizzo, P. Self-reported alteration of sense of smell or taste in patients with COVID-19: A systematic review and meta-analysis on 3563 patients. Rhinology 2020, 58, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Harrison, E.M.; Docherty, A.B.; Barr, B.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A. Ethnicity and outcomes from COVID-19: The ISARIC CCP-UK prospective observational cohort study of hospitalised patients. Prepr. Lancet 2020, 1–41. [Google Scholar] [CrossRef]
- Pan, D.; Sze, S.; Minhas, J.S.; Bangash, M.N.; Pareek, N.; Divall, P.; Williams, C.M.; Oggioni, M.R.; Squire, I.B.; Nellums, L.B. The impact of ethnicity on clinical outcomes in COVID-19: A systematic review. EClinicalMedicine 2020, 23, 100404. [Google Scholar] [CrossRef]
- Hendricks, B.; Paul, R.; Smith, C.; Wen, S.; Kimble, W.; Amjad, A.; Atkins, A.; Hodder, S. Coronavirus testing disparities associated with community level deprivation, racial inequalities, and food insecurity in West Virginia. Ann. Epidemiol. 2021, 59, 44–49. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Test | Short Smell Loss (≤28 Days) Mean ± 95% CI | Long Smell Loss (>28 Days) Mean ± 95% CI | Test Statistic | p-Value | ||
|---|---|---|---|---|---|---|---|
| Age | t-test | 31.53 (30.17–32.88) | 36.0 (33.0–39.0) | −3.04 | 0.003 ** | ||
| BMI | t-test | 26.81 (25.95–27.69) | 25.92 (24.64–27.20) | 1.077 | 0.28 | ||
| Fruit/vegetable intake | t-test | 2.91 (2.66–3.16) | 3.07 (2.62–3.52) | −0.608 | 0.54 | ||
| Illness severity | Mann–Whitney | 4.39 (4.11–4.66) | 5.01 (4.58–5.55) | −2.42 | 0.016 * | ||
| Smell-loss severity | Mann–Whitney | 8.47 (8.12–8.83) | 8.58 (7.93–9.24) | −0.77 | 0.44 | ||
| Congestion | Mann–Whitney | 3.08 (2.64–3.53) | 2.72 (1.92–3.52) | −0.10 | 0.32 | ||
| Sex | Fisher’s exact | M | 64 (65) | M | 24 (23) | NA | 0.88 |
| F | 109 (108) | F | 38 (39) | ||||
| Vitamin D | Fisher’s exact | No | 149 (151) | No | 56 (54) | NA | 0.27 |
| Yes | 24 (22) | Yes | 6 (8) | ||||
| Antidepressant | Fisher’s exact | No | 155 (155) | No | 56 (56) | NA | 0.54 |
| Yes | 18 (18) | Yes | 6 (6) | ||||
| Flossing | Fisher’s exact | No | 44 (52) | No | 27 (19) | NA | 0.01 ** |
| Yes | 129 (121) | Yes | 35 (43) | ||||
| Missing teeth | Fisher’s exact | No | 145 (145) | No | 53 (53) | NA | 0.83 |
| Yes | 23 (23) | Yes | 9 (9) | ||||
| Appliances | Fisher’s exact | No | 138 (140) | No | 52 (50) | NA | 0.57 |
| Yes | 35 (33) | Yes | 10 (12) | ||||
| Brushing freq. | Pearson’s Chi2 | Daily | 40 (34) | Daily | 32 (38) | 3.88 | 0.14 |
| 2 × day | 66 (69) | >2 × day | 80 (77) | ||||
| >2 × day | 5 (8) | >2 × day | 11 (8) | ||||
| Smoking | Pearson’s Chi2 | Never | 136 (135) | Never | 47 (48) | 0.21 | 0.90 |
| Former | 12 (12) | Former | 5 (5) | ||||
| Current | 25 (26) | Current | 10 (9) | ||||
| Alcohol freq. | Pearson’s Chi2 | Never | 32 (37) | Never | 18 (13) | 4.61 | 0.20 |
| Monthly | 43 (38) | Monthly | 9 (14) | ||||
| Weekly | 63 (63) | Weekly | 23 (23) | ||||
| Daily | 35 (35) | Daily | 12 (12) | ||||
| No. fillings | Pearson’s Chi2 | None | 49 (50) | None | 19 (18) | 1.99 | 0.57 |
| <5 | 74 (71) | <5 | 23 (26) | ||||
| 5–10 | 36 (39) | 5–10 | 17 (14) | ||||
| >10 | 14 (13) | >10 | 3 (5) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Catton, G.; Gardner, A. Relationship between Recovery from COVID-19-Induced Smell Loss and General and Oral Health Factors. Medicina 2022, 58, 283. https://doi.org/10.3390/medicina58020283
Catton G, Gardner A. Relationship between Recovery from COVID-19-Induced Smell Loss and General and Oral Health Factors. Medicina. 2022; 58(2):283. https://doi.org/10.3390/medicina58020283
Chicago/Turabian StyleCatton, Georgia, and Alexander Gardner. 2022. "Relationship between Recovery from COVID-19-Induced Smell Loss and General and Oral Health Factors" Medicina 58, no. 2: 283. https://doi.org/10.3390/medicina58020283
APA StyleCatton, G., & Gardner, A. (2022). Relationship between Recovery from COVID-19-Induced Smell Loss and General and Oral Health Factors. Medicina, 58(2), 283. https://doi.org/10.3390/medicina58020283