
An Open-Label Trial Study of Quality-of-Life Assessment in Irritable Bowel Syndrome and Their Treatment

Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Diagnosis
2.2. Paraclinical Diagnosis
2.3. Questionnaires
2.4. Statistical Analysis
2.5. Statement
3. Results
3.1. Demographic Description
3.1.1. Clinical Data
- The pain is related to defecation;
- The onset of symptoms is associated with changes in the frequency of stool;
- The onset of symptoms is associated with a change in the shape or appearance of the stool.
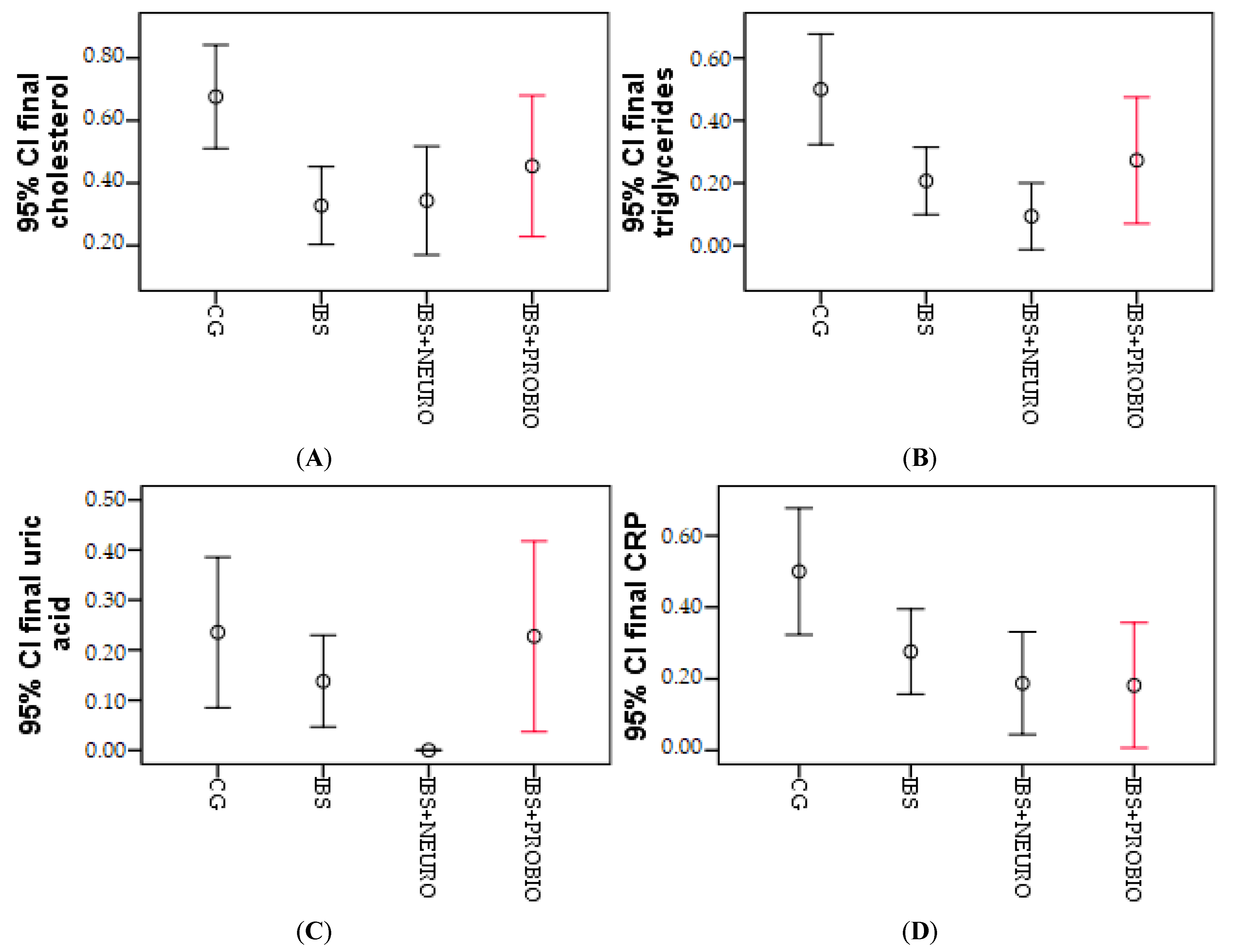
3.1.2. Paraclinical Data
3.1.3. Assessing the Quality of Life
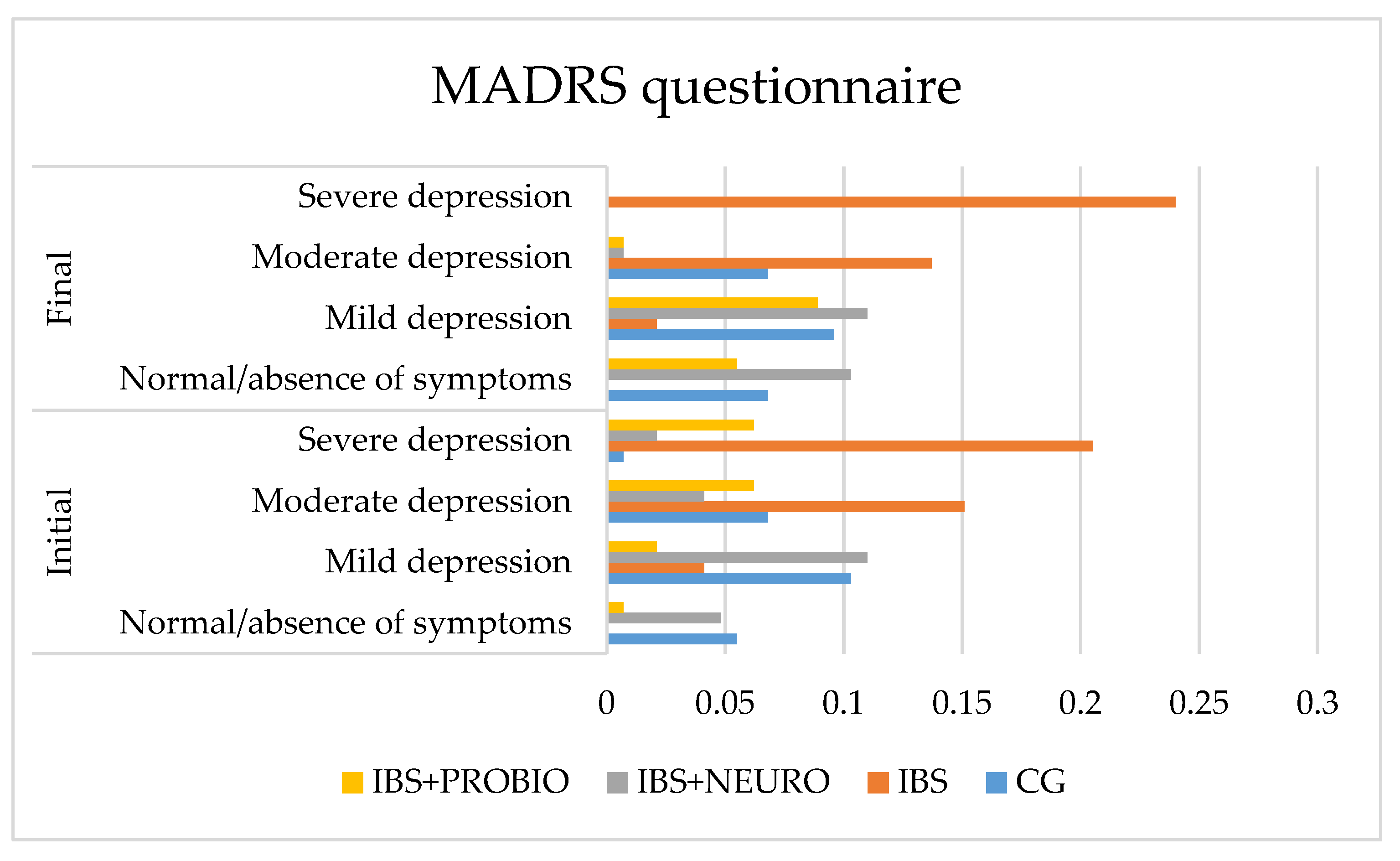
- In CG, the number of asymptomatic patients increased by 0.7%, mild depression decreased by 3.5%, moderate depression did not change, and severe depression decreased by 0.7% of cases. These results are correlated with the increased frequency of PTSD in those with IBS. No significant differences were obtained in this group comparing the final results with the initial values.
- In the IBS group, no change was observed in the number of asymptomatic patients, mild depression decreased by 2.0%, moderate depression decreased by 1.4%, and severe depression increased by 3.5% of cases.
- In the IBS + NEURO group, the number of asymptomatic patients increased by 10.3%, mild depression increased by 6.9%, moderate depression did not change, and severe depression decreased by 8.2% of cases. At the end of the study, a significant decrease in incidence in this group with severe depression measured on the MADRS scale was observed.
- In CG, the number of asymptomatic patients did not change, mild anxiety increased by 0.6%, moderate anxiety did not change, severe anxiety increased by 4.8%, and very severe/severe anxiety decreased by 5.5% of cases. Due to the symptomatic period of less than 3 months, at the end of the research period (6 months), the symptoms have improved and the quality of life improved significantly (p = 0.001).
- In the IBS group, no change was observed in the number of asymptomatic patients, mild anxiety decreased by 8.0%, moderate anxiety decreased by 6.0%, severe anxiety increased by 14%, and very severe/severe anxiety did not change in cases.
- In the IBS + NEURO group, the number of asymptomatic patients increased by 12.0%, mild anxiety increased by 12.0%, moderate anxiety increased by 11.0%, severe anxiety decreased by 6.0%, and very severe/severe anxiety decreased by 7%. At the end, no person in this group was reported with very severe anxiety measured with the HAS scale.
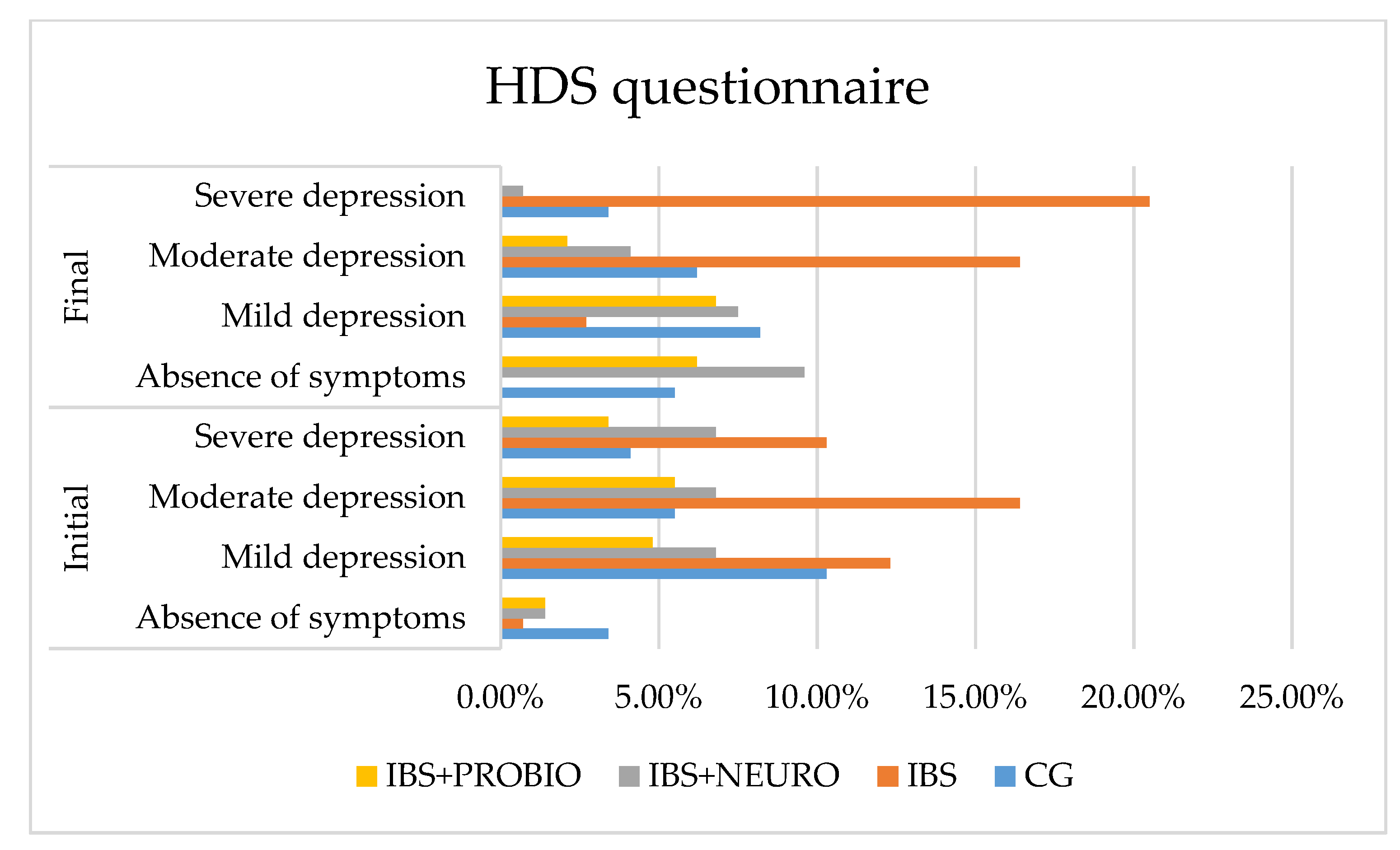
- In CG, the number of asymptomatic patients increased by 2.1%, mild depression decreased by 2.1%, moderate depression increased by 0.7%, and severe depression decreased by 0.7% of cases, but without reaching the lower limit of statistical significance.
- In the IBS group, there was a 0.7% decrease in the number of asymptomatic patients, a 12.6% decrease in mild depression decreased, no change in moderate depression, and a 10.2% increase in severe depression in cases.
- In the IBS + NEURO group, the number of asymptomatic patients increased by 13.1%, mild depression increased by 2.8%, moderate depression decreased by 6.1%, and severe depression decreased by 9.6% of cases, measured with the HDS scale, compared with IBS
- In the IBS + PROBIO group, the number of asymptomatic patients decreased by 2.9%, mild depression increased by 11.1%, moderate depression decreased by 5.2%, and severe depression decreased by 3.2% of cases, measured with the HDS scale, compared with IBS + NEURO.
3.1.4. Correlations
3.1.5. Comparison of IBS-NEURO and IBS-PROBIO
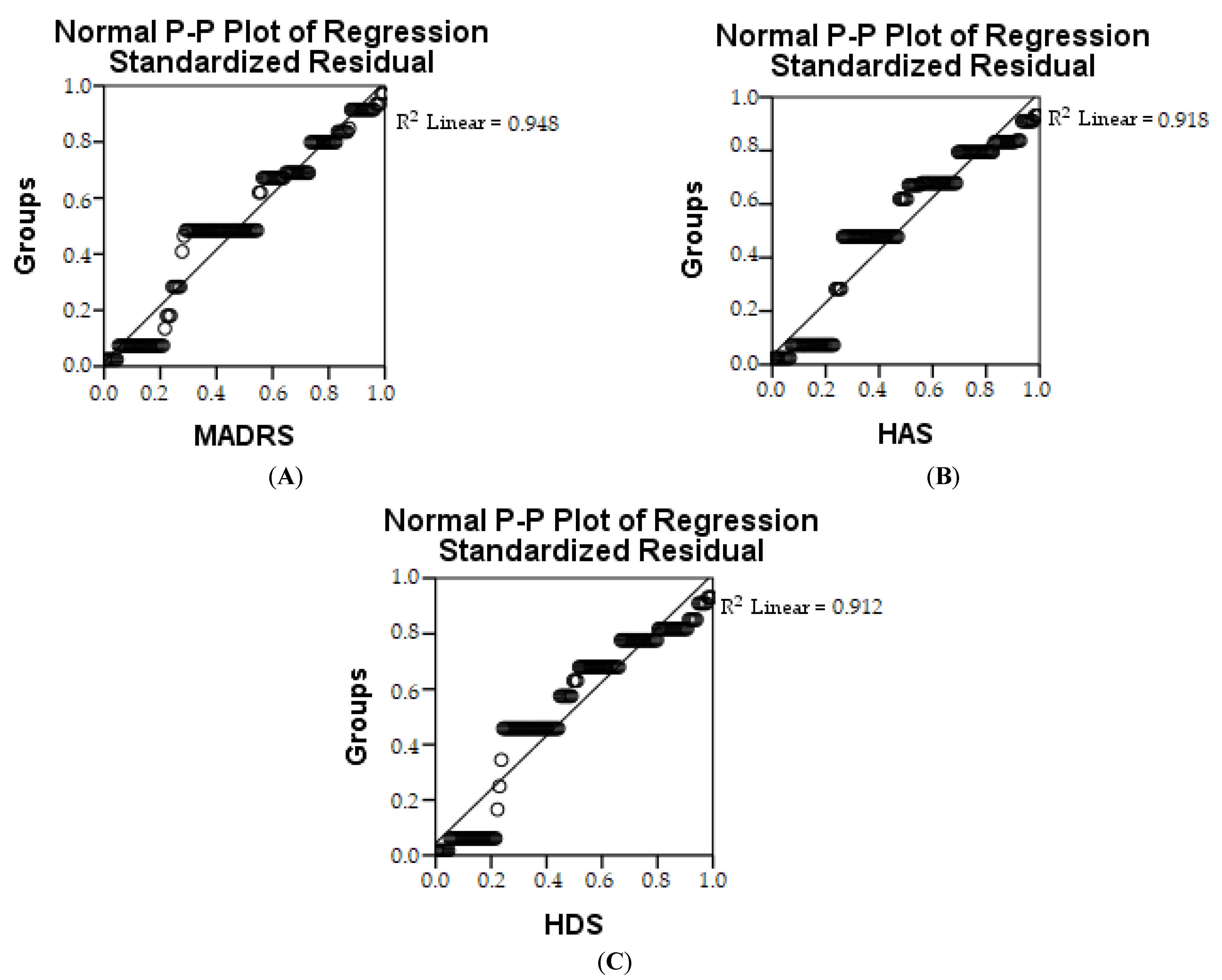
3.1.6. Linear Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saha, L. Irritable bowel syndrome: Pathogenesis, diagnosis, treatment, and evidence-based medicine. World J. Gastroenterol. 2014, 20, 6759–6773. [Google Scholar] [CrossRef] [PubMed]
- Bhattarai, Y.; Pedrogo, D.A.M.; Kashyap, P.C. Irritable bowel syndrome: A gut microbiota-related disorder? Am. J. Physiol.-Gastrointest. Liver Physiol. 2017, 312, G52–G62. [Google Scholar] [CrossRef] [PubMed]
- Ng, Q.X.; Soh, A.Y.S.; Loke, W.; Lim, D.Y.; Yeo, W.-S. The role of inflammation in irritable bowel syndrome (IBS). J. Inflamm. Res. 2018, 11, 345–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez, L.; Nurko, S. 65—Gastrointestinal Motility Procedures. In Pediatric Gastrointestinal and Liver Disease, 4th ed.; Wyllie, R., Hyams, J.S., Eds.; W.B. Saunders: Saint Louis, MO, USA, 2011; pp. 686–698.e683. [Google Scholar]
- Pavel, F.; Vesa, C.; Gheorghe, G.; Diaconu, C.; Stoicescu, M.; Munteanu, M.; Babes, E.; Tit, D.; Toma, M.; Bungau, S. Highlighting the Relevance of Gut Microbiota Manipulation in Inflammatory Bowel Disease. Diagnostics 2021, 11, 1090. [Google Scholar] [CrossRef]
- Sikander, A.; Rana, S.V.; Prasad, K.K. Role of serotonin in gastrointestinal motility and irritable bowel syndrome. Clin. Chim. Acta 2009, 403, 47–55. [Google Scholar] [CrossRef]
- Mawe, G.M.; Hoffman, J.M. Serotonin signalling in the gut—functions, dysfunctions and therapeutic targets. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 473–486. [Google Scholar] [CrossRef] [Green Version]
- Crowell, M.D. Role of serotonin in the pathophysiology of the irritable bowel syndrome. J. Cereb. Blood Flow Metab. 2004, 141, 1285–1293. [Google Scholar] [CrossRef]
- Binienda, A.; Ziolkowska, S.; Hauge, I.H.; Salaga, M. The Role of Immune and Epithelial Stem Cells in Inflammatory Bowel Disease Therapy. Curr. Drug Targets 2020, 21, 1405–1416. [Google Scholar] [CrossRef]
- Soares, R.L.S. Irritable bowel syndrome: A clinical review. World J. Gastroenterol. 2014, 20, 12144–12160. [Google Scholar] [CrossRef]
- Mansueto, P.; D’Alcamo, A.; Seidita, A.; Carroccio, A. Food allergy in irritable bowel syndrome: The case of non-celiac wheat sensitivity. World J. Gastroenterol. 2015, 21, 7089–7109. [Google Scholar] [CrossRef]
- Kopczyńska, M.; Mokros, L.; Pietras, T.; Małecka-Panas, E. Quality of life and depression in patients with irritable bowel syndrome. Gastroenterol. Rev. 2018, 13, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Mykletun, A.; Jacka, F.; Williams, L.; Pasco, J.; Henry, M.; Nicholson, G.C.; Kotowicz, M.A.; Berk, M. Prevalence of mood and anxiety disorder in self reported irritable bowel syndrome (IBS). An epidemiological population based study of women. BMC Gastroenterol. 2010, 10, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabra, N.; Nadkarni, A. Prevalence of depression and anxiety in irritable bowel syndrome: A clinic based study from India. Indian J. Psychiatry 2013, 55, 77–80. [Google Scholar] [CrossRef]
- North, C.S.; Hong, B.A.; Alpers, D.H. Relationship of functional gastrointestinal disorders and psychiatric disorders: Implications for treatment. World J. Gastroenterol. 2007, 13, 2020–2027. [Google Scholar] [CrossRef]
- Enck, P.; Aziz, Q.; Barbara, G.; Farmer, A.D.; Fukudo, S.; Mayer, E.A.; Niesler, B.; Quigley, E.M.M.; Rajilic-Stojanovic, M.; Schemann, M.; et al. Irritable bowel syndrome. Nat. Rev. Dis. Prim. 2016, 2, 16014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, Q.X.; Soh, A.Y.S.; Loke, W.; Venkatanarayanan, N.; Lim, D.Y.; Yeo, W.-S. Systematic review with meta-analysis: The association between post-traumatic stress disorder and irritable bowel syndrome. J. Gastroenterol. Hepatol. 2019, 34, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Corb Aron, R.A.; Abid, A.; Vesa, C.M.; Nechifor, A.C.; Behl, T.; Ghitea, T.C.; Munteanu, M.A.; Fratila, O.; Andronie-Cioara, F.L.; Toma, M.M. Recognizing the benefits of pre-/probiotics in metabolic syndrome and type 2 diabetes mellitus considering the influence of akkermansia muciniphila as a key gut bacterium. Microorganisms 2021, 9, 618. [Google Scholar] [CrossRef]
- Khan, I.; Ullah, N.; Zha, L.; Bai, Y.; Khan, A.; Zhao, T.; Che, T.; Zhang, C. Alteration of Gut Microbiota in Inflammatory Bowel Disease (IBD): Cause or Consequence? IBD Treatment Targeting the Gut Microbiome. Pathogens 2019, 8, 126. [Google Scholar] [CrossRef] [Green Version]
- Ilias, T.; Bungau, S.; Tit, D.M.; Maghiar, D.; Hocopan, C.; Brata, R.; Bratu, O.G.; Negrut, N.; Diaconu, C.; Fratila, O. Psychosocial profile of the patients with inflammatory bowel disease. Exp. Ther. Med. 2020, 20, 2493–2500. [Google Scholar] [CrossRef]
- Amiri, P.; Hosseini, S.A.; Ghaffari, S.; Tutunchi, H.; Ghaffari, S.; Mosharkesh, E.; Asghari, S.; Roshanravan, N. Role of Butyrate, a Gut Microbiota Derived Metabolite, in Cardiovascular Diseases: A comprehensive narrative review. Front. Pharmacol. 2022, 12, 837509. [Google Scholar] [CrossRef]
- Arora, A.; Behl, T.; Sehgal, A.; Singh, S.; Sharma, N.; Bhatia, S.; Sobarzo-Sanchez, E.; Bungau, S. Unravelling the involvement of gut microbiota in type 2 diabetes mellitus. Life Sci. 2021, 273, 119311. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Qu, H.; Guo, M.; Zhang, Y.; Cui, Y.; Yang, Q.; Bai, R.; Shi, D. ANRIL and atherosclerosis. J. Clin. Pharm. Ther. 2020, 45, 240–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, B.; Wei, J.; Ju, P.; Chen, J. Effects of regulating intestinal microbiota on anxiety symptoms: A systematic review. Gen. Psychiatry 2019, 32, e100056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahabi, L.; Naliboff, B.D.; Shapiro, D. Self-regulation evaluation of therapeutic yoga and walking for patients with irritable bowel syndrome: A pilot study. Psychol. Health Med. 2015, 21, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Barandouzi, Z.A.; Lee, J.; Maas, K.; Starkweather, A.R.; Cong, X.S. Altered Gut Microbiota in Irritable Bowel Syndrome and Its Association with Food Components. J. Pers. Med. 2021, 11, 35. [Google Scholar] [CrossRef] [PubMed]
- Barandouzi, Z.A.; Lee, J.; del Carmen Rosas, M.; Chen, J.; Henderson, W.A.; Starkweather, A.R.; Cong, X.S. Associations of neurotransmitters and the gut microbiome with emotional distress in mixed type of irritable bowel syndrome. Sci. Rep. 2022, 12, 1648. [Google Scholar] [CrossRef] [PubMed]
- Sharon, G.; Sampson, T.; Geschwind, D.H.; Mazmanian, S.K. The Central Nervous System and the Gut Microbiome. Cell 2016, 167, 915–932. [Google Scholar] [CrossRef] [Green Version]
- Strandwitz, P. Neurotransmitter modulation by the gut microbiota. Brain Res. 2018, 1693, 128–133. [Google Scholar] [CrossRef]
- Ford, A.C.; Sperber, A.D.; Corsetti, M.; Camilleri, M. Irritable bowel syndrome. Lancet 2020, 396, 1675–1688. [Google Scholar] [CrossRef]
- Moayyedi, P.; Mearin, F.; Azpiroz, F.; Andresen, V.; Barbara, G.; Corsetti, M.; Emmanuel, A.; Hungin, A.P.S.; Layer, P.; Stanghellini, V.; et al. Irritable bowel syndrome diagnosis and management: A simplified algorithm for clinical practice. United Eur. Gastroenterol. J. 2017, 5, 773–788. [Google Scholar] [CrossRef] [Green Version]
- Altobelli, E.; Del Negro, V.; Angeletti, P.M.; Latella, G. Low-FODMAP Diet Improves Irritable Bowel Syndrome Symptoms: A Meta-Analysis. Nutrients 2017, 9, 940. [Google Scholar] [CrossRef] [PubMed]
- Ghitea, T.C.; Vlad, S.; Birle, D.; Tit, D.M.; Lazar, L.; Nistor-Cseppento, C.; Behl, T.; Bungau, S. The Influence of Diet Therapeutic Intervention on the Sarcopenic Index of Patients with Metabolic Syndrome. Acta Endocrinol. 2020, 16, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Marsh, A.; Eslick, E.M.; Eslick, G.D. Does a diet low in FODMAPs reduce symptoms associated with functional gastrointestinal disorders? A comprehensive systematic review and meta-analysis. Eur. J. Nutr. 2015, 55, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Ireton-Jones, C. The low FODMAP diet: Fundamental therapy in the management of irritable bowel syndrome. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 414–419. [Google Scholar] [CrossRef]
- Franquesa, M.; Pujol-Busquets, G.; García-Fernández, E.; Rico, L.; Shamirian-Pulido, L.; Aguilar-Martínez, A.; Medina, F.-X.; Serra-Majem, L.; Bach-Faig, A. Mediterranean Diet and Cardiodiabesity: A Systematic Review through Evidence-Based Answers to Key Clinical Questions. Nutrients 2019, 11, 655. [Google Scholar] [CrossRef] [Green Version]
- Chong, R.I.H.; Yaow, C.Y.L.; Loh, C.Y.L.; Teoh, S.E.; Masuda, Y.; Ng, W.K.; Lim, Y.L.; Ng, Q.X. Vitamin D supplementation for irritable bowel syndrome: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2022. [Google Scholar] [CrossRef]
- van Lanen, A.-S.; de Bree, A.; Greyling, A. Efficacy of a low-FODMAP diet in adult irritable bowel syndrome: A systematic review and meta-analysis. Eur. J. Nutr. 2021, 60, 3505–3522. [Google Scholar] [CrossRef]
- Harvie, R.M.; Chisholm, A.W.; Bisanz, J.E.; Burton, J.P.; Herbison, P.; Schultz, K.; Schultz, M. Long-term irritable bowel syndrome symptom control with reintroduction of selected FODMAPs. World J. Gastroenterol. 2017, 23, 4632–4643. [Google Scholar] [CrossRef]
- Wang, J.; Yang, P.; Zhang, L.; Hou, X. A Low-FODMAP Diet Improves the Global Symptoms and Bowel Habits of Adult IBS Patients: A Systematic Review and Meta-Analysis. Front. Nutr. 2021, 8, 683191. [Google Scholar] [CrossRef]
- Behl, T.; Bungau, S.; Kumar, K.; Zengin, G.; Khan, F.; Kumar, A.; Kaur, R.; Venkatachalam, T.; Tit, D.M.; Vesa, C.M.; et al. Pleotropic Effects of Polyphenols in Cardiovascular System. Biomed. Pharmacother. 2020, 130, 110714. [Google Scholar] [CrossRef]
- Oprea, O.B.; Apostol, L.; Bungau, S.; Cioca, G.; Samuel, A.D.; Badea, M.; Gaceu, L. Researches on the chemical composition and the rheological properties of wheat and grape epicarp flour mixes. Rev. Chim. 2018, 69, 70–75. [Google Scholar] [CrossRef]
- Adriani, A.; Ribaldone, D.G.; Astegiano, M.; Durazzo, M.; Saracco, G.M.; Pellicano, R. Irritable bowel syndrome: The clinical approach. Panminerva Medica 2018, 60, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Jee, S.R. Irritable Bowel Syndrome. Korean J. Gastroenterol. 2019, 73, 84–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mudyanadzo, T.A.; Hauzaree, C.; Yerokhina, O.; Architha, N.N.; Ashqar, H.M. Irritable Bowel Syndrome and Depression: A Shared Pathogenesis. Cureus 2018, 10, e3178. [Google Scholar] [CrossRef] [Green Version]
- Simpson, C.A.; Mu, A.; Haslam, N.; Schwartz, O.; Simmons, J.G. Feeling down? A systematic review of the gut microbiota in anxiety/depression and irritable bowel syndrome. J. Affect. Disord. 2020, 266, 429–446. [Google Scholar] [CrossRef]
- Canakis, A.; Haroon, M.; Weber, H.C. Irritable bowel syndrome and gut microbiota. Curr. Opin. Endocrinol. Diabetes Obes. 2020, 27, 28–35. [Google Scholar] [CrossRef]
- Araceli, M.-G.; Cristina, D.-P.; Francisco, T.J. Gut microbiota and type 2 diabetes mellitus. Endocrinol. Y Nutr. Organo Soc. Esp. Endocrinol. Nutr. 2016, 63, 560–568. [Google Scholar] [CrossRef]
- Ghitea, T.C. Correlation of Periodontal Bacteria with Chronic Inflammation Present in Patients with Metabolic Syndrome. Biomedicines 2021, 9, 1709. [Google Scholar] [CrossRef]
- Nibali, L.; Tatarakis, N.; Needleman, I.; Tu, Y.-K.; D’Aiuto, F.; Rizzo, M.; Donos, N. Association Between Metabolic Syndrome and Periodontitis: A Systematic Review and Meta-analysis. J. Clin. Endocrinol. Metab. 2013, 98, 913–920. [Google Scholar] [CrossRef] [Green Version]
- Ghitea, T.C.; Aleya, L.; Tit, D.M.; Behl, T.; Stoicescu, M.; Sava, C.; Iovan, C.; El-Kharoubi, A.; Uivarosan, D.; Pallag, A.; et al. Influence of diet and sport on the risk of sleep apnea in patients with metabolic syndrome associated with hypothyroidism—A 4-year survey. Environ. Sci. Pollut. Res. 2021, 29, 23158–23168. [Google Scholar] [CrossRef]
- Ghitea, T.C.; Bungau, S.; Tit, D.M.; Purza, L.; Otrisal, P.; Aleya, L.; Cioca, G.; Pantis, C.; Lazar, L. The Effects of Oregano Oil on Fungal Infections Associated with Metabolic Syndrome. Rev. Chim. 2020, 71, 335–341. [Google Scholar] [CrossRef]
- Romijn, A.R.; Rucklidge, J.J.; Kuijer, R.G.; Frampton, C. A double-blind, randomized, placebo-controlled trial of Lactobacillus helveticus and Bifidobacterium longum for the symptoms of depression. Aust. New Zealand J. Psychiatry 2017, 51, 810–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paduano, D.; Cingolani, A.; Tanda, E.; Usai, P. Effect of Three Diets (Low-FODMAP, Gluten-free and Balanced) on Irritable Bowel Syndrome Symptoms and Health-Related Quality of Life. Nutrients 2019, 11, 1566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bian, L.-Q.; Lu, F.; Li, Z.-H.; Ll, B.-S.; Gao, R.; Wang, F.-Y.; Zhang, Y.-Q.; Tang, X.-D. Analysis of Response of IBS-SSS, AR, and IBS-QOL in IBS Clinical Effect Evaluation. Chin. J. Integr. Tradit. West. Med. 2016, 36, 1191–1196. [Google Scholar]
- Majeed, M.; Nagabhushanam, K.; Arumugam, S.; Majeed, S.; Ali, F. Bacillus coagulans MTCC 5856 for the management of major depression with irritable bowel syndrome: A randomised, double-blind, placebo controlled, multi-centre, pilot clinical study. Food Nutr. Res. 2018, 62. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Description | Groups | Total | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| CG | IBS | IBS + NEURO | IBS + PROBIO | ||||||||
| Count | % | Count | % | Count | % | Count | % | Count | % | ||
| Gender | Male | 18 | 12.3 | 24 | 16.4 | 22 | 15.1% | 12 | 8.2% | 76 | 52.1 |
| Female | 16 | 11.0 | 34 | 23.3 | 10 | 6.8% | 10 | 6.8% | 70 | 47.9 | |
| Area | Urban | 27 | 18.5 | 47 | 32.2 | 23 | 15.8% | 20 | 13.7% | 117 | 80.1 |
| Rural | 7 | 4.8 | 11 | 7.5 | 9 | 6.2% | 2 | 1.4% | 29 | 19.9 | |
| Parameters | Groups | Total | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| CG | IBS | IBS + NEURO | IBS + PROBIO | ||||||||
| Count | % | Count | % | Count | % | Count | % | Count | % | ||
| Pain | Absent | 0 | 0.0 | 0 | 0.0 | 0 | 0.0% | 0 | 0.0% | 0 | 0.0 |
| Present | 34 | 23.3 | 58 | 39.7 | 32 | 21.9% | 22 | 15.1% | 146 | 100.0 | |
| Pain related to the defecation | Absent | 3 | 2.1 | 5 | 3.4 | 7 | 4.8% | 3 | 2.1% | 18 | 12.3 |
| Present | 31 | 21.2 | 53 | 36.3 | 25 | 17.1% | 19 | 13.0% | 128 | 87.7 | |
| Presence duration of symptoms | Less than 3 months | 34 | 23.3 | 0 | 0.0 | 0 | 0.0% | 0 | 0.0% | 34 | 23.3 |
| Between 3 and 6 months | 0 | 0.0 | 26 | 17.8 | 16 | 11.0% | 7 | 4.8% | 49 | 33.6 | |
| More than 6 months | 0 | 0.0 | 32 | 21.9 | 16 | 11.0% | 15 | 10.3% | 63 | 43.2 | |
| Stool consistency | Constipation | 1 | 0.7 | 9 | 6.2 | 4 | 2.7% | 4 | 2.7% | 18 | 12.3 |
| Mixed | 22 | 15.1 | 15 | 10.3 | 9 | 6.2% | 6 | 4.1% | 52 | 35.6 | |
| Over 3 stools a day | 11 | 7.5 | 34 | 23.3 | 19 | 13.0% | 12 | 8.2% | 76 | 52.1 | |
| Changes in the appearance of the stool | No | 8 | 5.5 | 9 | 6.2 | 6 | 4.1% | 4 | 2.7% | 27 | 18.5 |
| Yes | 26 | 17.8 | 49 | 33.6 | 26 | 17.8% | 18 | 12.3% | 119 | 81.5 | |
| Variable | Groups | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| CG | IBS | IBS + NEURO | IBS + PROBIO | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Cholesterol initial | 0.68 | 0.47 | 0.72 | 0.45 | 0.44 | 0.50 | 0.68 | 0.48 | 0.64 | 0.48 |
| Cholesterol final | 0.68 | 0.47 | 0.33 | 0.47 | 0.34 | 0.48 | 0.45 | 0.51 | 0.43 | 0.50 |
| Triglycerides initial | 0.41 | 0.50 | 0.64 | 0.48 | 0.41 | 0.50 | 0.59 | 0.50 | 0.53 | 0.50 |
| Triglycerides final | 0.50 | 0.51 | 0.21 | 0.41 | 0.09 | 0.30 | 0.27 | 0.46 | 0.26 | 0.44 |
| Uric acid initial | 0.24 | 0.43 | 0.50 | 0.50 | 0.13 | 0.34 | 0.59 | 0.50 | 0.37 | 0.48 |
| Uric acid final | 0.24 | 0.43 | 0.14 | 0.35 | 0.00 | 0.00 | 0.23 | 0.43 | 0.14 | 0.35 |
| CRP initial | 0.50 | 0.51 | 0.50 | 0.50 | 0.25 | 0.44 | 0.55 | 0.51 | 0.45 | 0.50 |
| CRP final | 0.50 | 0.51 | 0.28 | 0.45 | 0.19 | 0.40 | 0.18 | 0.39 | 0.29 | 0.46 |
| Variable | Mean | SD | Lower | Upper | T | Sig. | r/Z | Sig. | |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Cholesterol initial—cholesterol final | 0.21233 | 0.55347 | 0.12180 | 0.30286 | 4.635 | 0.001 | 0.359 | 0.001 |
| 2 | Triglycerides initial—triglycerides final | 0.26712 | 0.50229 | 0.18496 | 0.34928 | 6.426 | 0.436 | ||
| 3 | Uric acid initial—uric acid final | 0.22603 | 0.41970 | 0.15738 | 0.29468 | 6.507 | 5.745 | ||
| 4 | CRP initial—CRP final | 0.15753 | 0.36556 | 0.09774 | 0.21733 | 5.207 | 0.711 | ||
| Variables | n | Mean | Std. Deviation | p | |
|---|---|---|---|---|---|
| Cholesterol | IBS + NEURO | 32 | 0.3438 | 0.48256 | 1.000 |
| IBS + PROBIO | 22 | 0.4545 | 0.50965 | ||
| Triglycerides | IBS + NEURO | 32 | 0.0938 | 0.29614 | 0.759 |
| IBS + PROBIO | 22 | 0.2727 | 0.45584 | ||
| Uric acid | IBS + NEURO | 32 | 0.0000 | 0.00000 | 0.112 |
| IBS + PROBIO | 22 | 0.2273 | 0.42893 | ||
| CRP | IBS + NEURO | 32 | 0.1875 | 0.39656 | 1.000 |
| IBS + PROBIO | 22 | 0.1818 | 0.39477 | ||
| MADRS | IBS + NEURO | 32 | 0.5625 | 0.56440 | 1.000 |
| IBS + PROBIO | 22 | 0.6818 | 0.56790 | ||
| HAS | IBS + NEURO | 32 | 1.0625 | 0.80071 | 1.000 |
| IBS + PROBIO | 22 | 1.0909 | 0.86790 | ||
| HDS | IBS + NEURO | 32 | 0.8125 | 0.85901 | 1.000 |
| IBS + PROBIO | 22 | 0.7273 | 0.70250 | ||
| Parametri | Correlate | R2 (%) | r | β1 | β2 | t | F |
|---|---|---|---|---|---|---|---|
| MADRS | Groups | 94.80 | 0.432 ** | −0.379 ** | −0.432 ** | 5.749 ** | 33.050 ** |
| HAS | 91.80 | 0.419 ** | −0.372 ** | −0.418 ** | 5.519 ** | 30.454 ** | |
| HDS | 91.20 | 0.471 ** | −0.398 ** | −0.471 ** | 6.406 ** | 41.043 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alexandru, B.A.; Rat, L.A.; Moldovan, A.F.; Mihancea, P.; Mariș, L. An Open-Label Trial Study of Quality-of-Life Assessment in Irritable Bowel Syndrome and Their Treatment. Medicina 2022, 58, 763. https://doi.org/10.3390/medicina58060763
Alexandru BA, Rat LA, Moldovan AF, Mihancea P, Mariș L. An Open-Label Trial Study of Quality-of-Life Assessment in Irritable Bowel Syndrome and Their Treatment. Medicina. 2022; 58(6):763. https://doi.org/10.3390/medicina58060763
Chicago/Turabian StyleAlexandru, Bogdana Ariana, Lavinia Alina Rat, Andrada Florina Moldovan, Petru Mihancea, and Lavinia Mariș. 2022. "An Open-Label Trial Study of Quality-of-Life Assessment in Irritable Bowel Syndrome and Their Treatment" Medicina 58, no. 6: 763. https://doi.org/10.3390/medicina58060763
APA StyleAlexandru, B. A., Rat, L. A., Moldovan, A. F., Mihancea, P., & Mariș, L. (2022). An Open-Label Trial Study of Quality-of-Life Assessment in Irritable Bowel Syndrome and Their Treatment. Medicina, 58(6), 763. https://doi.org/10.3390/medicina58060763