
Effect of Fenugreek on Hyperglycemia: A Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
, 

 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
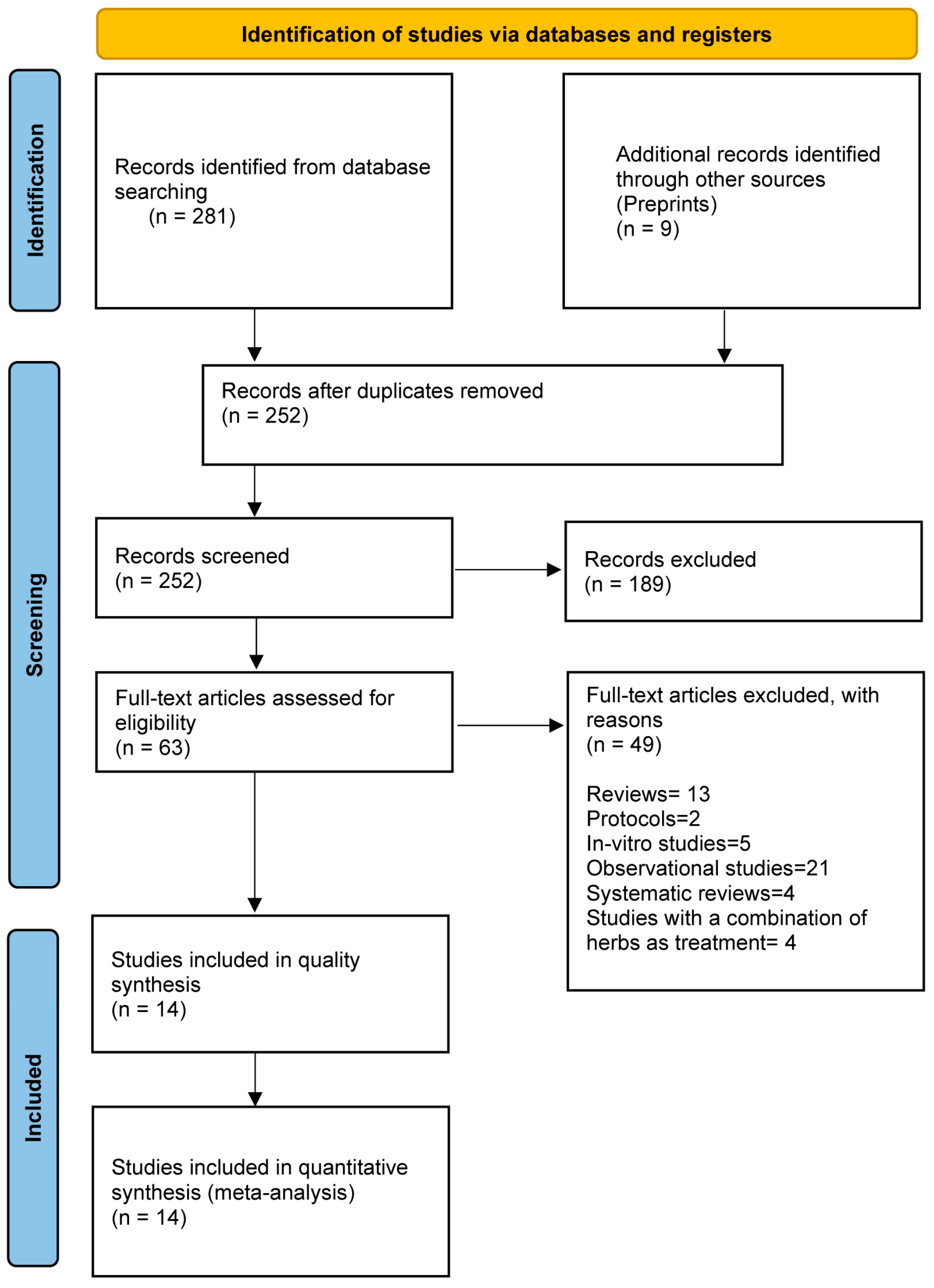
2.3. Study Selection
2.4. Data Extraction and Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Included Studies
3.2. Characteristics of Included Studies
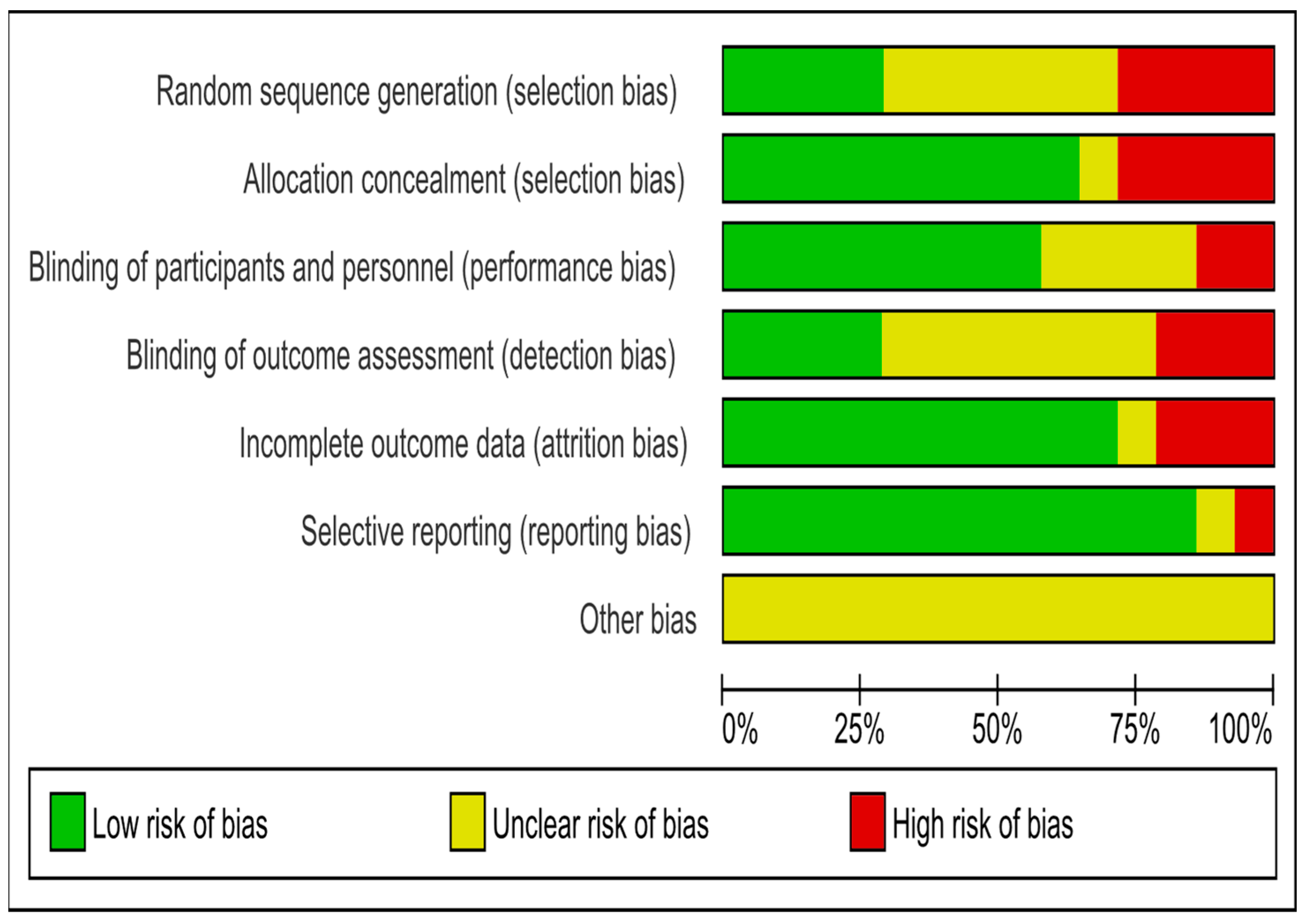
3.3. Risk of Bias
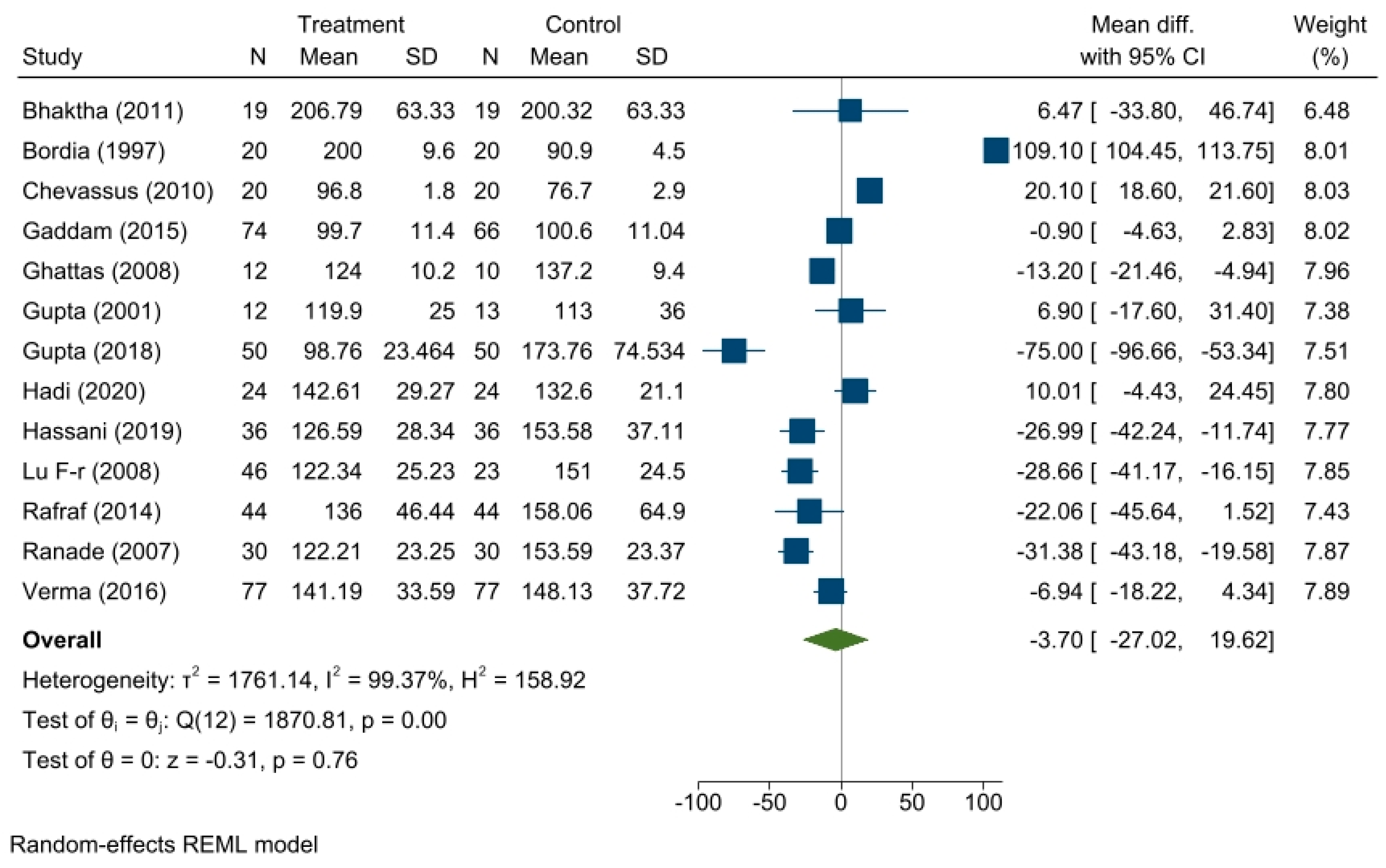
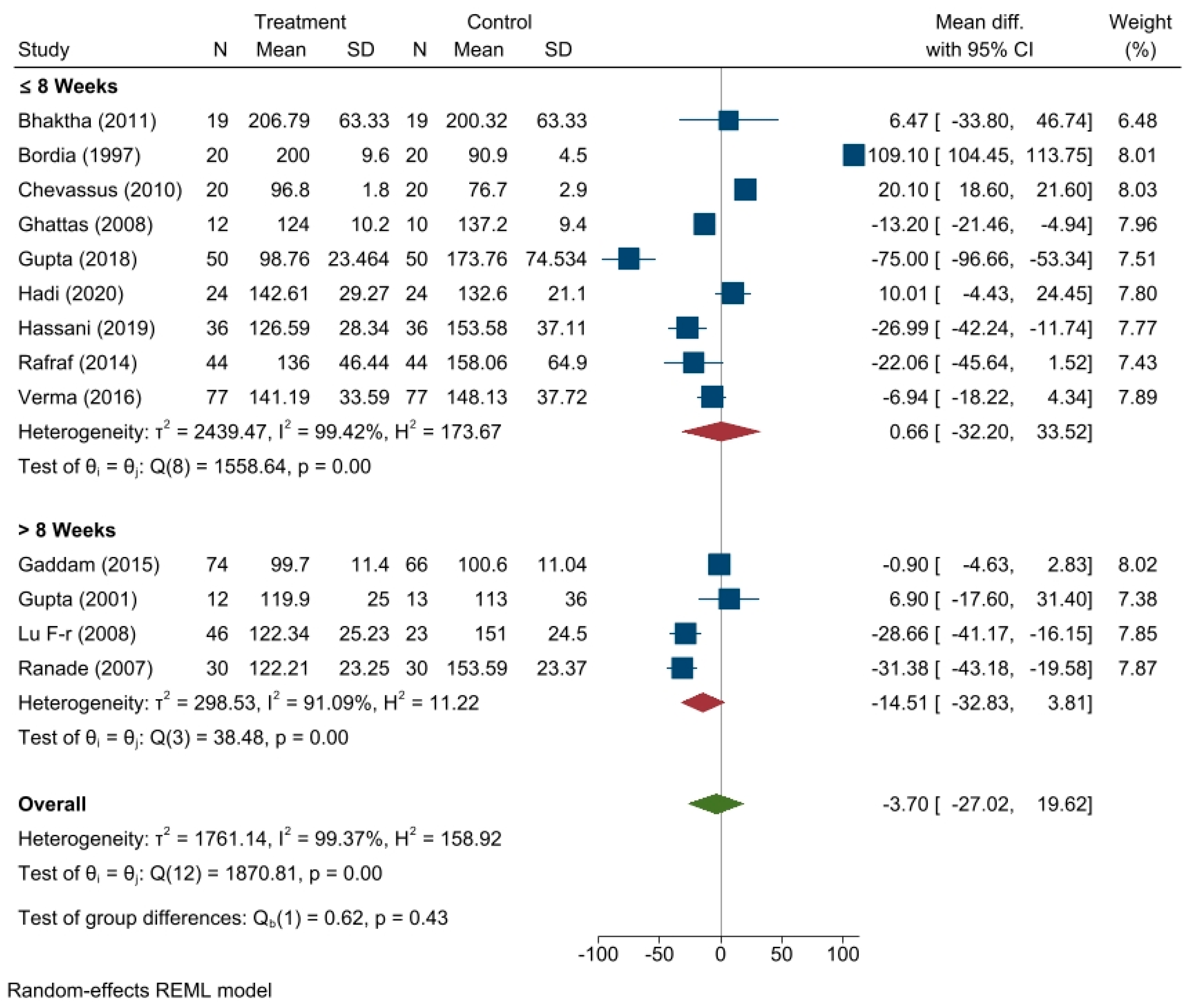
3.4. Effect of Fenugreek on Fasting Blood Glucose Level
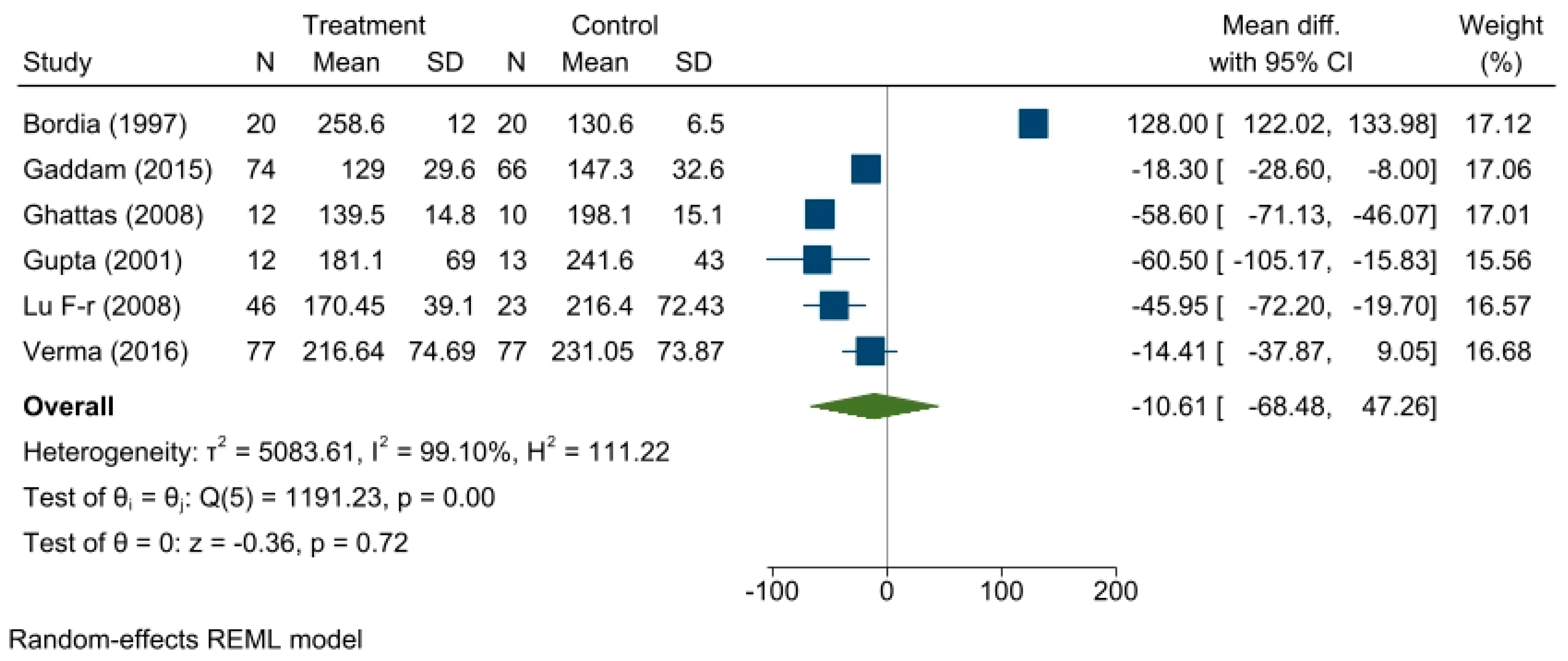
3.5. Effect of Fenugreek on Postprandial Glucose Level
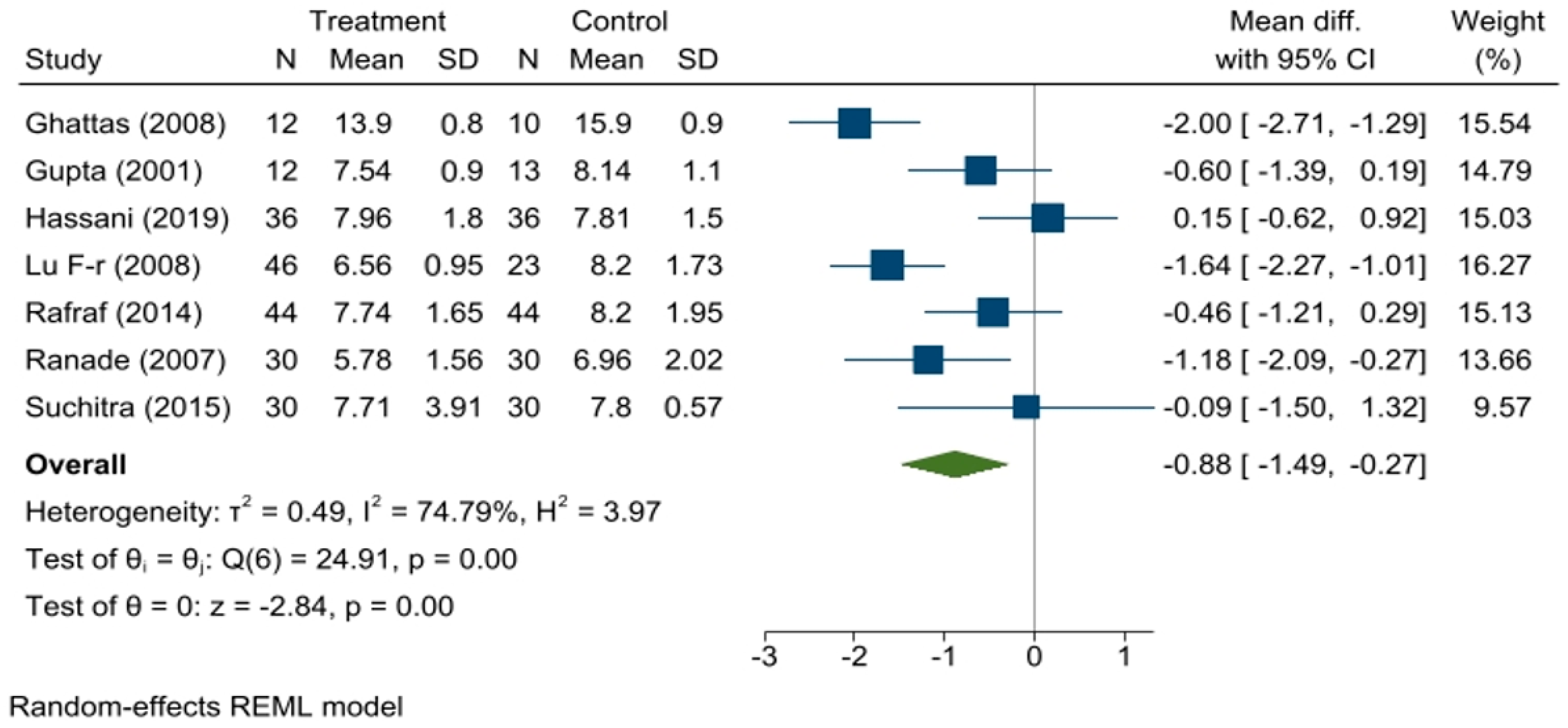
3.6. Effect of Fenugreek on HbA1c
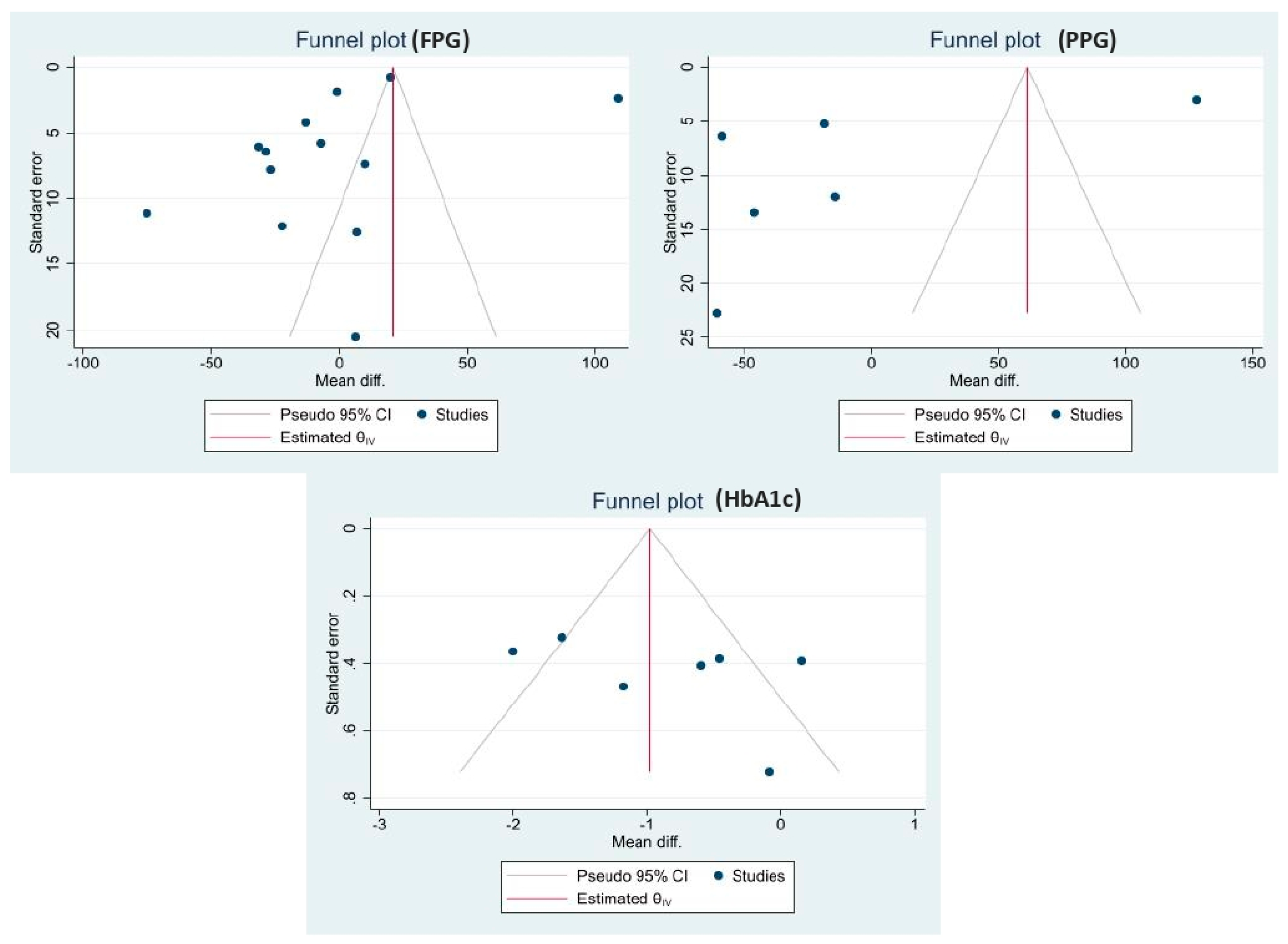
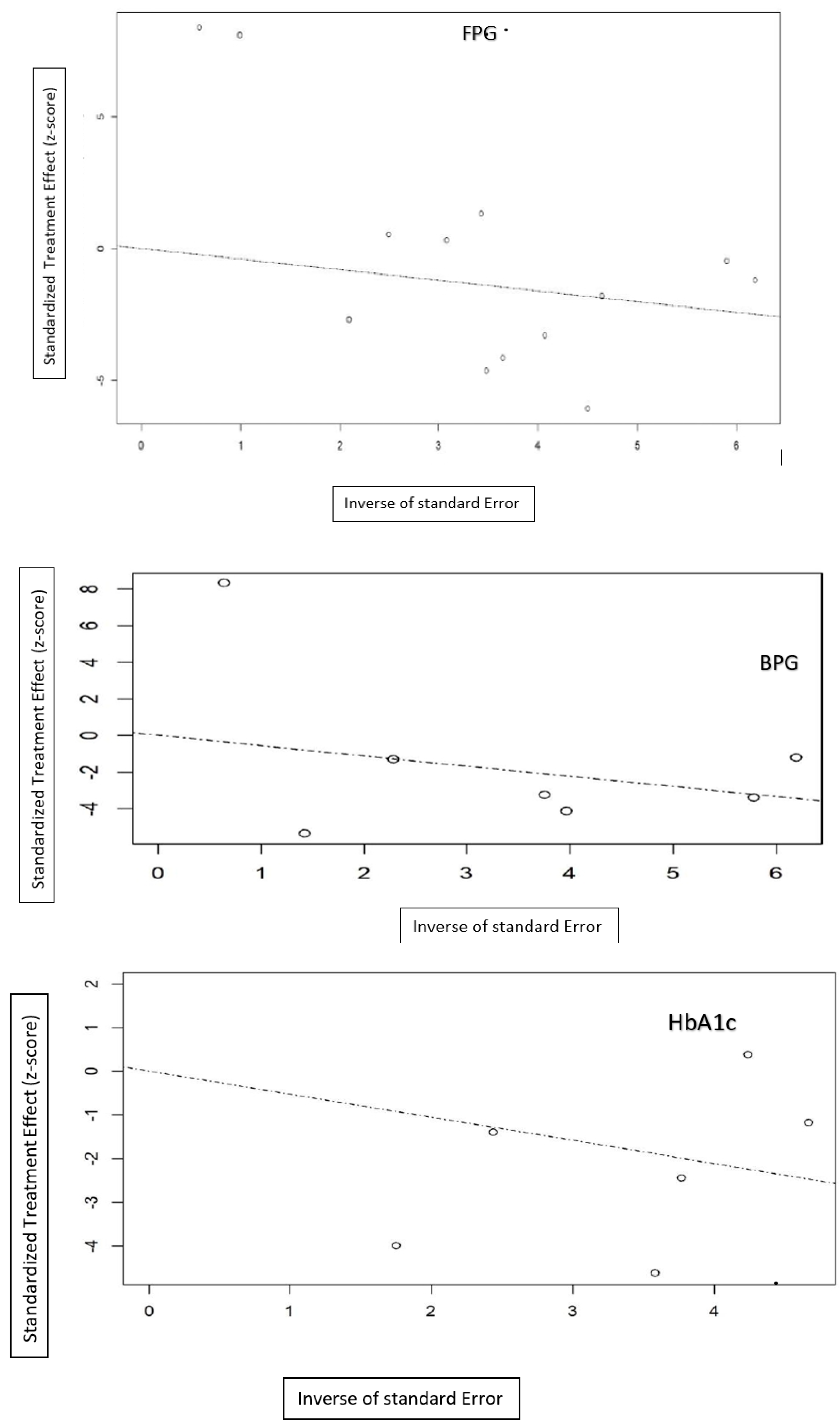
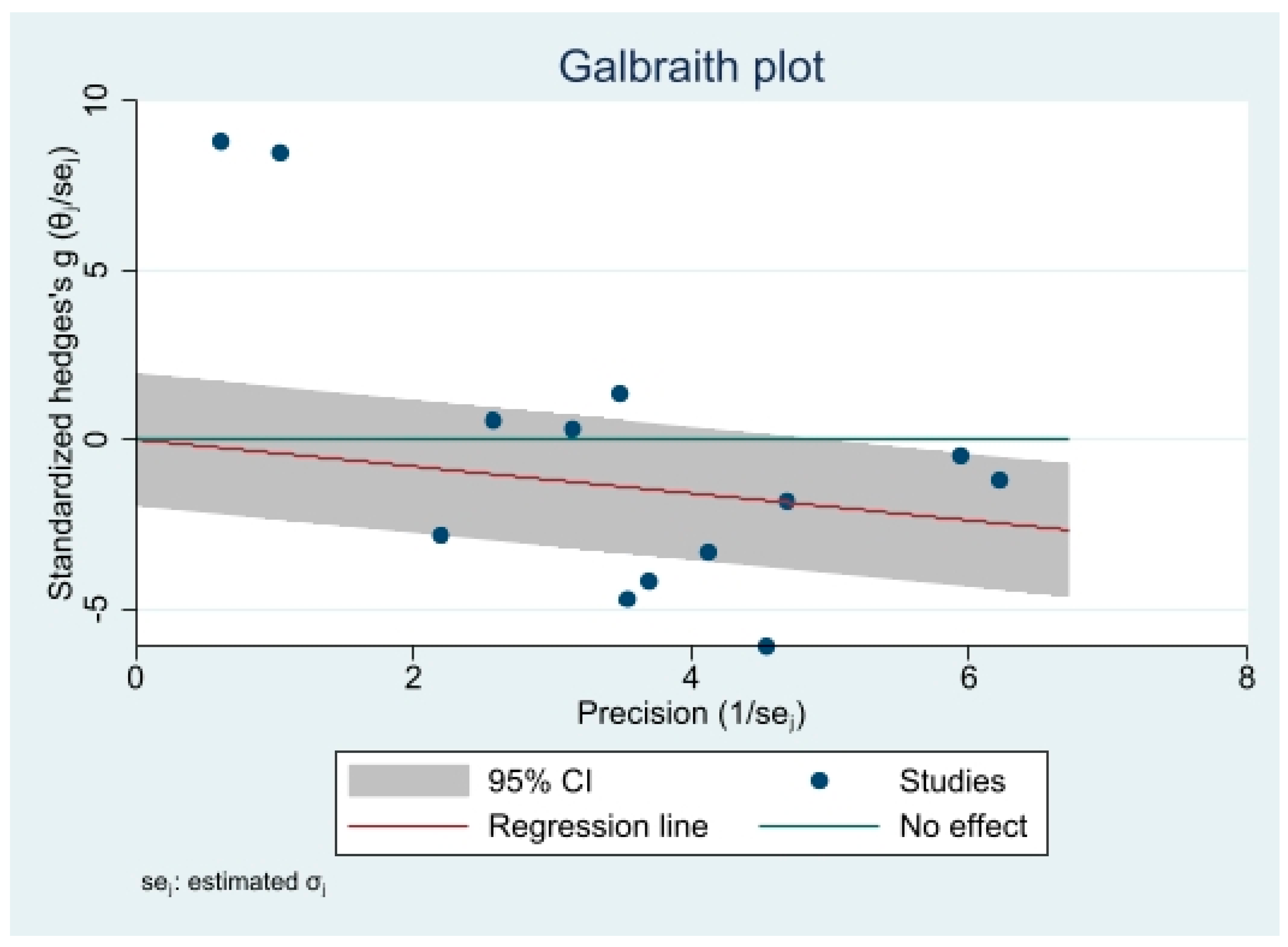
3.7. Publication Bias
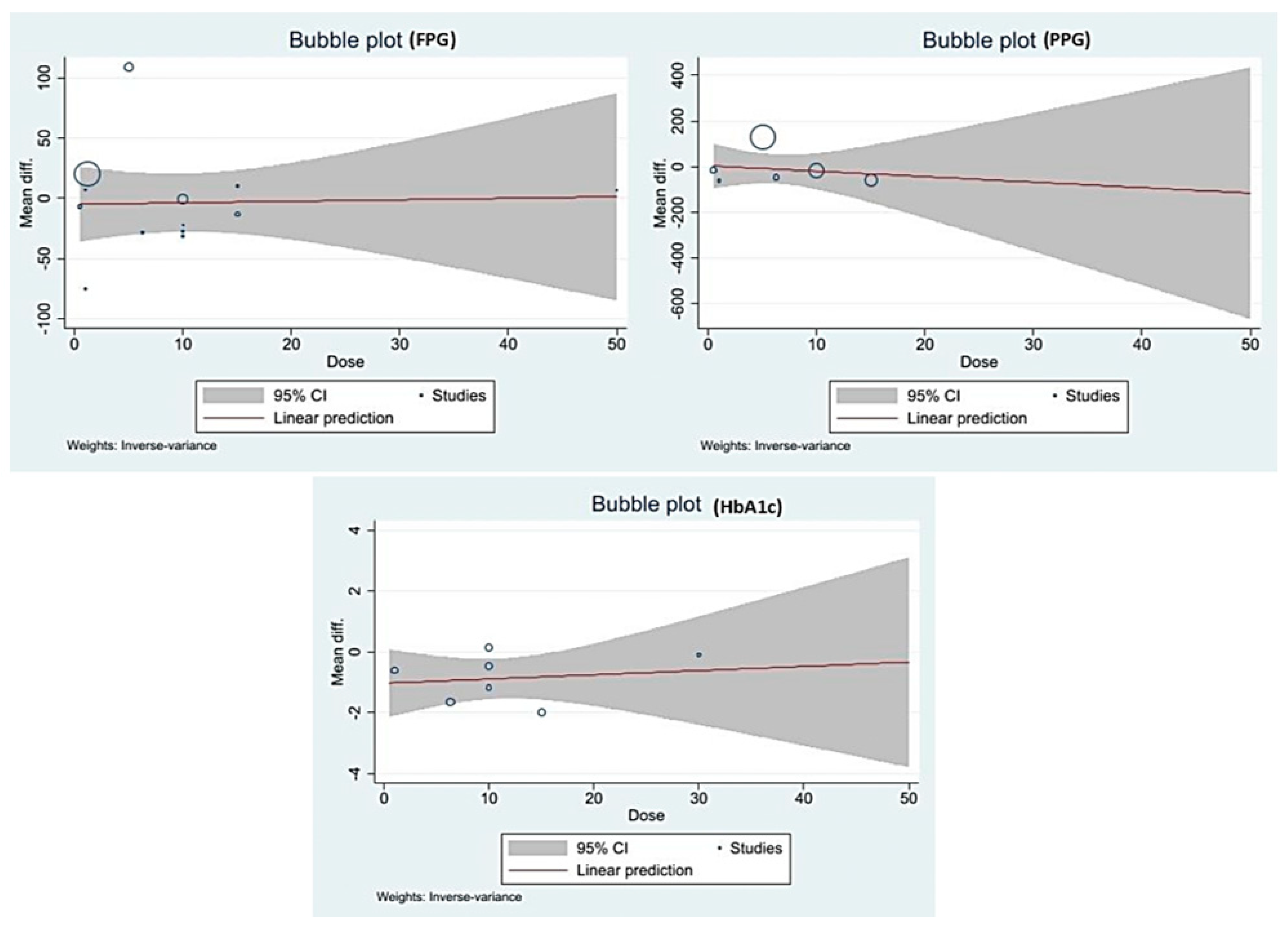
3.8. Meta-Regression
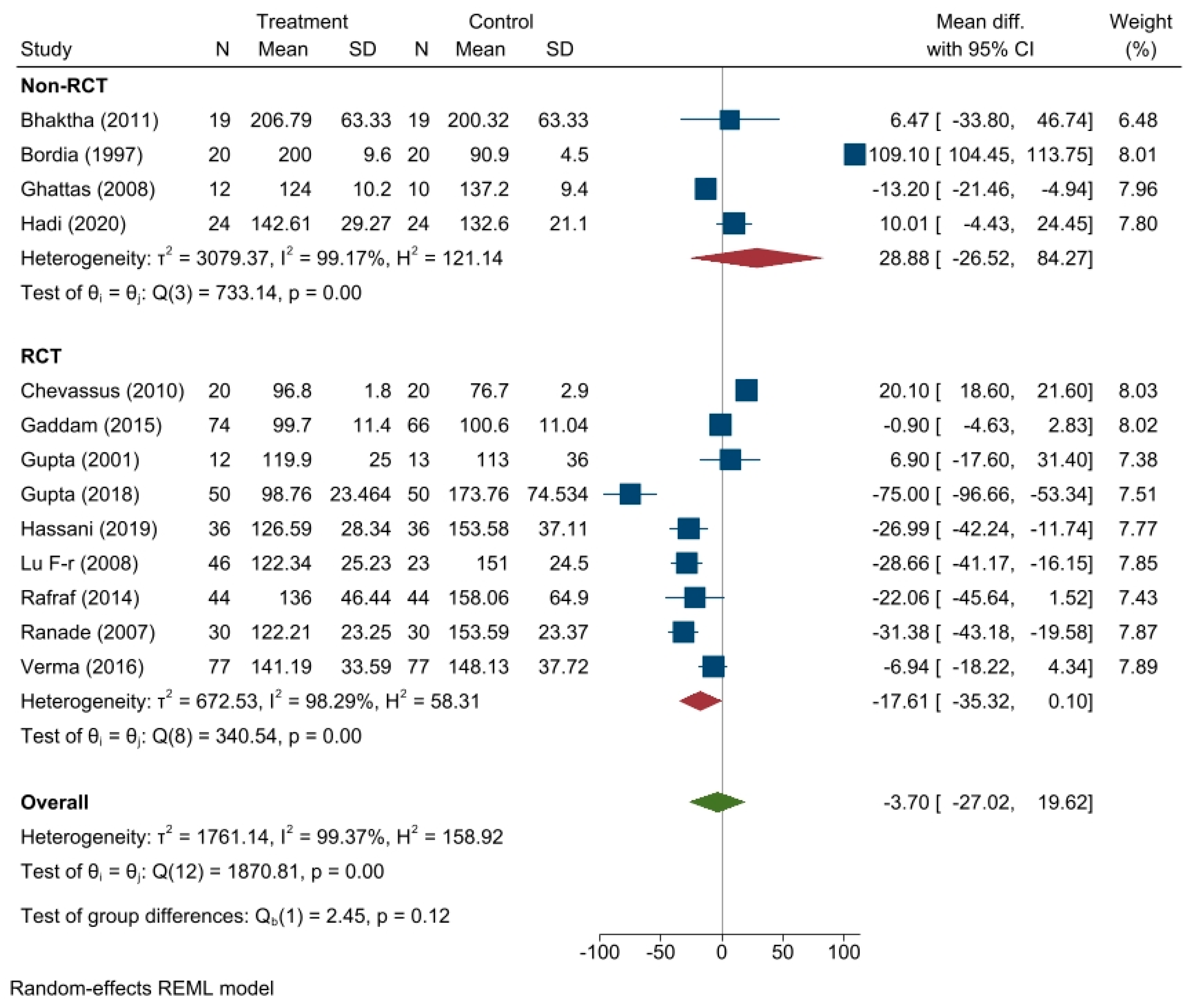
3.9. Subgroup Analsysis
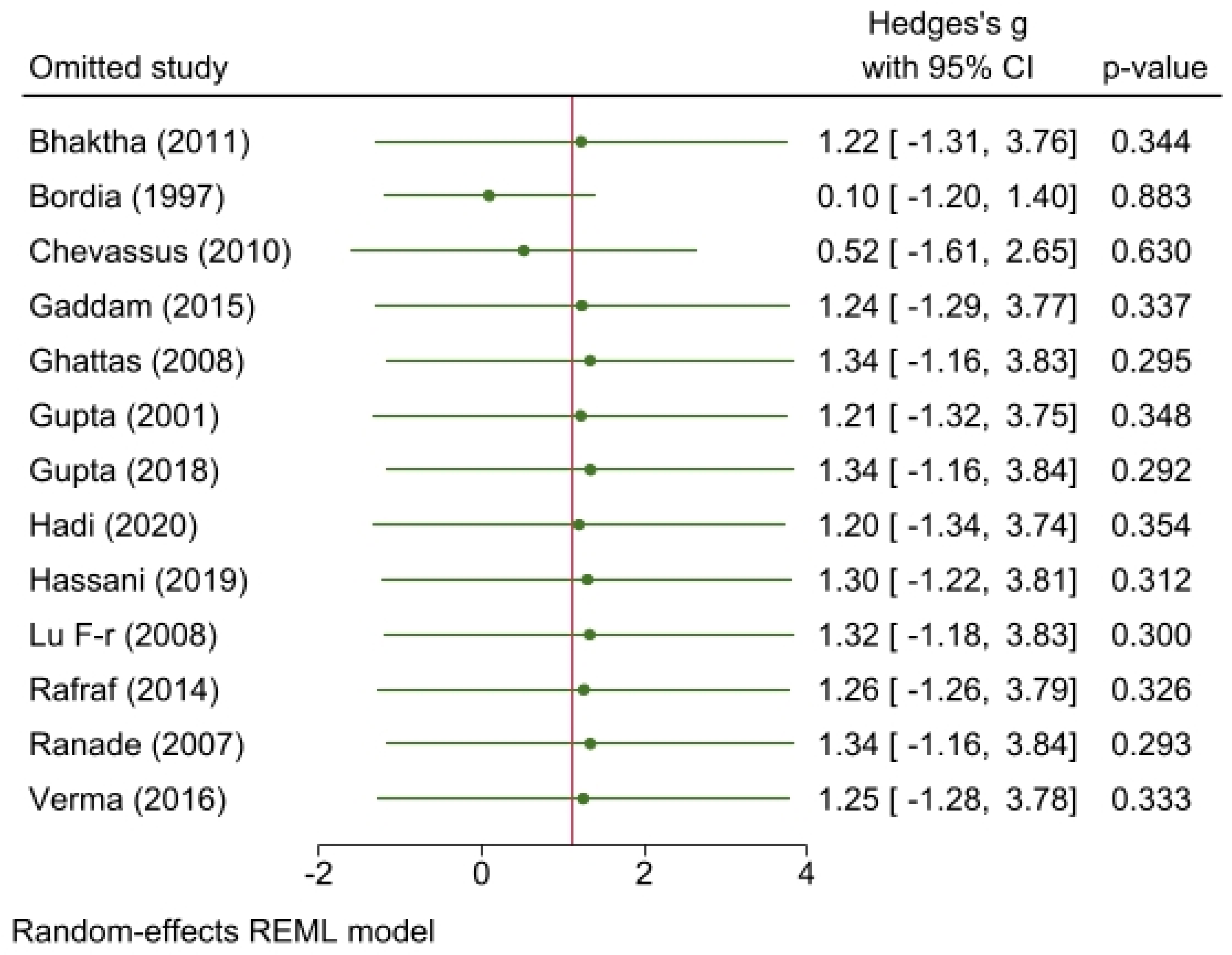
3.10. Sensitivity Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A





References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Misra, A.; Gopalan, H.; Jayawardena, R.; Hills, A.P.; Soares, M.; Reza-Albarrán, A.A.; Ramaiya, K.L. Diabetes in developing countries. J. Diabetes 2019, 11, 522–539. [Google Scholar] [CrossRef]
- Kirtikar, K.R.; Basu, B.D. Indian Medicinal Plants; Sudhindra Nath Basu, M.B., Ed.; Panini Office: Bahadurganj, India, 1932. [Google Scholar]
- Gong, J.; Fang, K.; Dong, H.; Wang, D.; Hu, M.; Lu, F. Effect of fenugreek on hyperglycemia and hyperlipidemia in diabetes and prediabetes: A meta-analysis. J. Ethnopharmacol. 2016, 194, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.; Wylie-Rosett, J. Review of selected Chinese herbal medicines in the treatment of type 2 diabetes. Diabetes Educ. 2008, 34, 645–654. [Google Scholar] [CrossRef] [PubMed]
- Ranade, M.; Mudgalkar, N. A simple dietary addition of fenugreek seed leads to the reduction in blood glucose levels: A parallel-group, randomized single-blind trial. Ayu 2017, 38, 24. [Google Scholar] [CrossRef] [PubMed]
- Karim, A.; Siroosce, C.; Jabrayel, P. Antidiabetic effects of exercise and fenugreek supplementation in males with NIDDM. Med. Sport 2009, 62, 315–324. [Google Scholar]
- Sharma, R. Effect of fenugreek seeds and leaves on blood glucose and serum insulin responses in human subjects. Nutr. Res. 1986, 6, 1353–1364. [Google Scholar] [CrossRef]
- Kassaian, N.; Azadbakht, L.; Forghani, B.; Amini, M. Effect of fenugreek seeds on blood glucose and lipid profiles in type 2 diabetic patients. Int. J. Vitam. Nutr. Res. 2009, 79, 34–39. [Google Scholar] [CrossRef]
- Madar, Z.; Abel, R.; Samish, S.; Arad, J. Glucose-lowering effect of fenugreek in non-insulin dependent diabetics. Eur. J. Clin. Nutr. 1988, 42, 51–54. [Google Scholar]
- Lu, F.-r.; Shen, L.; Qin, Y.; Gao, L.; Li, H.; Dai, Y. Clinical observation on trigonella foenum-graecum L. total saponins in combination with sulfonylureas in the treatment of type 2 diabetes mellitus. Chin. J. Integr. Med. 2008, 14, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Gupta, R.; Lal, B. Effect of Trigonella foenum-graecum (Fenugreek) seeds on glycaemic control and insulin resistance in type 2 diabetes. J. Assoc. Physicians India 2001, 49, 1057–1061. [Google Scholar]
- Mathern, J.R.; Raatz, S.K.; Thomas, W.; Slavin, J.L. Effect of fenugreek fiber on satiety, blood glucose and insulin response and energy intake in obese subjects. Phytother. Res. 2009, 23, 1543–1548. [Google Scholar] [CrossRef] [PubMed]
- Chevassus, H.; Molinier, N.; Costa, F.; Galtier, F.; Renard, E.; Petit, P. A fenugreek seed extract selectively reduces spontaneous fat consumption in healthy volunteers. Eur. J. Clin. Pharmacol. 2009, 65, 1175–1178. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version; The Cochrnae Collaboration: London, UK; John Wiley & Sons Ltd.: Pondicherry, India, 2011; Volume 5. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Research methods & reporting-preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement-David Moher and colleagues introduce PRISMA, an update of the QUOROM guidelines for reporting systematic reviews and meta-analyses. BMJ 2009, 338, 332. [Google Scholar]
- Higgins, J.; Altman, D.; Sterne, J. Chapter 8: Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.1. 0 [Updated March 2011]; The Cochrane Collaboration: London, UK, 2011; pp. 187–214. [Google Scholar]
- Riley, R.; Higgins, J.; Deeks, J. Interpretation of random effects meta-analyses. BMJ 2011, 342, d549. [Google Scholar] [CrossRef] [PubMed]
- Verma, N.; Usman, K.; Patel, N.; Jain, A.; Dhakre, S.; Swaroop, A.; Bagchi, M.; Kumar, P.; Preuss, H.G.; Bagchi, D. A multicenter clinical study to determine the efficacy of a novel fenugreek seed (Trigonella foenum-graecum) extract (Fenfuro™) in patients with type 2 diabetes. Food Nutr. Res. 2016, 60, 32382. [Google Scholar] [CrossRef]
- Hadi, A.; Arab, A.; Hajianfar, H.; Talaei, B.; Miraghajani, M.; Babajafari, S.; Marx, W.; Tavakoly, R. The effect of fenugreek seed supplementation on serum irisin levels, blood pressure, and liver and kidney function in patients with type 2 diabetes mellitus: A parallel randomized clinical trial. Complement. Ther. Med. 2020, 49, 102315. [Google Scholar] [CrossRef]
- Bhaktha, G.; Nayak, S.; Shantaram, M. Management of newly diagnosed Type 2 Diabetes by Trigonella Foenum-Graecum. Int. J. Ayurveda Res. 2011, 2, 1231–1234. [Google Scholar]
- Gupta, R.; Grover, A.; Goel, A.; Tiwari, K. Clinical Study to Determine Efficacy of Trigonella Foenum-Graecum Extract in Patients with Type 2 Diabetes. Diabetes Complicat. 2018, 2, 1–5. [Google Scholar]
- Gupta, A.; Gupta, R.; Lal, B. Effect of Trigonella foenum-graecum (fenugreek) seeds on glycaemic control and insulin resistance in type 2 diabetes mellitus: A double blind placebo controlled study. Altern. Med. Rev. 2002, 7, 255–256. [Google Scholar]
- Bordia, A.; Verma, S.; Srivastava, K. Effect of ginger (Zingiber officinale Rosc.) and fenugreek (Trigonella foenumgraecum L.) on blood lipids, blood sugar and platelet aggregation in patients with coronary artery disease. Prostaglandins Leukot. Essent. Fat. Acids 1997, 56, 379–384. [Google Scholar] [CrossRef]
- Rafraf, M.; Malekiyan, M.; Asghari-Jafarabadi, M.; Aliasgarzadeh, A. Effect of fenugreek seeds on serum metabolic factors and adiponectin levels in type 2 diabetic patients. Int. J. Vitam. Nutr. Res. 2014, 84, 196–205. [Google Scholar] [CrossRef]
- Chevassus, H.; Gaillard, J.B.; Farret, A.; Costa, F.; Gabillaud, I.; Mas, E.; Dupuy, A.M.; Michel, F.; Cantié, C.; Renard, E.; et al. A fenugreek seed extract selectively reduces spontaneous fat intake in overweight subjects. Eur. J. Clin. Pharmacol. 2010, 66, 449–455. [Google Scholar] [CrossRef]
- Suchitra, M.; Parthasarathy, S. Effect of administration of fenugreek seeds on HbA1C levels in uncontrolled diabetes mellitus-a randomized controlled trial. Int. J. Pharm. Tech. Res. 2015, 8, 180–182. [Google Scholar]
- Gaddam, A.; Galla, C.; Thummisetti, S.; Marikanty, R.K.; Palanisamy, U.D.; Rao, P.V. Role of Fenugreek in the prevention of type 2 diabetes mellitus in prediabetes. J. Diabetes Metab. Disord. 2015, 14, 74. [Google Scholar] [CrossRef]
- Ghattas, L.A.; Hanna, L.M.; Tapozada, S.T.; El-Shebini, S.M. Some complementary hypoglycemic supplements from grains and legumes for the management of type 2 diabetes mellitus. J. Med. Sci. 2008, 8, 102–103. [Google Scholar]
- Hassani, S.S.; Arezodar, F.F.; Esmaeili, S.S.; Gholami-Fesharaki, M. Effect of fenugreek use on fasting blood glucose, glycosylated hemoglobin, body mass index, waist circumference, blood pressure and quality of life in patients with type 2 diabetes mellitus: A randomized, double-blinded, placebo-controlled clinical trials. Galen Med. J. 2019, 8, e1432. [Google Scholar] [CrossRef] [PubMed]
- Neelakantan, N.; Narayanan, M.; de Souza, R.J.; van Dam, R.M. Effect of fenugreek (Trigonella foenum-graecum L.) intake on glycemia: A meta-analysis of clinical trials. Nutr. J. 2014, 13, 7. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.; Prasad, S.K.; Kumar, R.; Hemalatha, S. An overview on antidiabetic medicinal plants having insulin mimetic property. Asian Pac. J. Trop. Biomed. 2012, 2, 320–330. [Google Scholar] [CrossRef] [PubMed]
- Gauttam, V.K.; Kalia, A.N. Development of polyherbal antidiabetic formulation encapsulated in the phospholipids vesicle system. J. Adv. Pharm. Technol. Res. 2013, 4, 108. [Google Scholar]
- Bera, T.K.; Ali, K.M.; Jana, K.; Ghosh, A.; Ghosh, D. Protective effect of aqueous extract of seed of Psoralea corylifolia (Somraji) and seed of Trigonella foenum-graecum L. (Methi) in streptozotocin-induced diabetic rat: A comparative evaluation. Pharmacogn. Res. 2013, 5, 277. [Google Scholar]
- Heshmat-Ghahdarijani, K.; Mashayekhiasl, N.; Amerizadeh, A.; Teimouri Jervekani, Z.; Sadeghi, M. Effect of fenugreek consumption on serum lipid profile: A systematic review and meta-analysis. Phytother. Res. 2020, 34, 2230–2245. [Google Scholar] [CrossRef] [PubMed]
- Askarpour, M.; Alami, F.; Campbell, M.S.; Venkatakrishnan, K.; Hadi, A.; Ghaedi, E. Effect of fenugreek supplementation on blood lipids and body weight: A systematic review and meta-analysis of randomized controlled trials. J. Ethnopharmacol. 2020, 253, 112538. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Country, Year | Design | Age | Population | Subjects (n) | Medications | FENUGREEK FORM | Daily Dose | Treatment Duration | Control Group | Outcomes of Interest |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Verma N [19] | India, 2016 | Parallel | 25–60 | T2DM < 5 years | 154 | Metformin | FENFURO capsule | 0.5 g | 4 weeks | Placebo | FBG, PPG |
| Hadi A [20] | Iran, 2020 | Parallel | 30–65 | T2DM | 48 | Anti-diabetic drugs | Powder | 15 g | 8 weeks | No placebo | FBG |
| Bhaktha G [21] | India, 2011 | Parallel | 30–45 | New diagnosed T2DM | 38 | N/A | Powder | 50 g | 8 weeks | No placebo | FBG |
| Gupta R [22] | India, 2018 | Parallel | 28–65 | T2DM | 100 | Anti-diabetic drugs | FENFURO capsule | 1 g | 12 weeks | No placebo | FPG, HbA1c |
| Lu F-r [11] | China, 2008 | Parallel | 54.26 | T2DM poorly controlled | 69 | Sulphonyl urea | Capsule | 6.3 g | 12 weeks | Chinese yam as placebo | FBG, PPG, HbA1c |
| Gupta A [23] | India, 2001 | Parallel | 51 | NIDDM | 25 | Sulphonyl urea/biguanide | Capsule extract | 1 g | 8 weeks | Placebo is given | FPG, PPG, HbA1c |
| A. Bordia [24] | India, 1997 | Parallel | N/A | T2DM | 40 | N/A | Capsule | 5 g | 4 weeks | Placebo is given | FBG, PPG, |
| Rafraf M [25] | Iran, 2014 | Parallel | 40.535 | T2DM | 44 | Metformin/ Glibemclamide | Powder | 10 g | 8 weeks | Placebo is given | FBG, HbA1c |
| Chevassus H [26] | France, 2010 | Parallel | 38.0 | Healthy overweight | 39 | N/A | Coated tablet | 1176 mg | 6 weeks | Placebo is given | FBG |
| Suchitra M [27] | India, 2015 | Parallel | 50.2 | T2DM | 60 | Oral hypoglycemic agent | Fenugreek seeds | 30 g | 8 weeks | No placebo | HbA1c |
| Gaddam A [28] | India, 2015 | Parallel | 30–70 | Pre-diabetic | 79 | N/A | Powder | 10 g | 3 years | No placebo | FBG, PPG |
| Ghattas LA [29] | Egypt, 2008 | Parallel | 43–64 | T2DM | 22 | N/A | Powder | 15 g | 1 week | No placebo | HbA1c, FBG, PPG |
| Ranade M [6] | India, 2007 | Parallel | 46.22–48 | T2DM | 60 | Anti-diabetic medication | Fenugreek seed, water soaked | 10 g | 6 months | No placebo | FBG, HbA1c |
| Hassani SS [30] | Iran, 2019 | Parallel | 51.27 | T2DM | 72 | N/A | Powder | 10 g | 8 weeks | Wheat flour placebo | FBG, HbA1c |
| Variables | β (95%CI) | p-Value | |
|---|---|---|---|
| Unadjusted | Adjusted | ||
| Treatment Dose (mg) | 0.125 (−1.938, 2.190) | −1.424 (−3.665, 0.817) | 0.213 |
| Treatment Duration (Weeks) | −0.030 (−0.686, 0.625) | 0.181 (−0.410, 0.772) | 0.548 |
| Study design (RCT) | −47.680 (−92.620, −2.740) | −80.814 (−141.917, −19.712) | 0.010 |
| Total Sample | −0.030 (−0.733, 0.672) | 0.273 (−0.411, 0.959) | 0.433 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shabil, M.; Bushi, G.; Bodige, P.K.; Maradi, P.S.; Patra, B.P.; Padhi, B.K.; Khubchandani, J. Effect of Fenugreek on Hyperglycemia: A Systematic Review and Meta-Analysis. Medicina 2023, 59, 248. https://doi.org/10.3390/medicina59020248
Shabil M, Bushi G, Bodige PK, Maradi PS, Patra BP, Padhi BK, Khubchandani J. Effect of Fenugreek on Hyperglycemia: A Systematic Review and Meta-Analysis. Medicina. 2023; 59(2):248. https://doi.org/10.3390/medicina59020248
Chicago/Turabian StyleShabil, Muhammed, Ganesh Bushi, Pavan Kalyan Bodige, Pavan Sagar Maradi, Bibhu Prasad Patra, Bijaya K. Padhi, and Jagdish Khubchandani. 2023. "Effect of Fenugreek on Hyperglycemia: A Systematic Review and Meta-Analysis" Medicina 59, no. 2: 248. https://doi.org/10.3390/medicina59020248
APA StyleShabil, M., Bushi, G., Bodige, P. K., Maradi, P. S., Patra, B. P., Padhi, B. K., & Khubchandani, J. (2023). Effect of Fenugreek on Hyperglycemia: A Systematic Review and Meta-Analysis. Medicina, 59(2), 248. https://doi.org/10.3390/medicina59020248