
Optimal Heart Rate Control Improves Long-Term Prognosis of Decompensated Heart Failure with Reduced Ejection Fraction

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Method
2.1. Data Source
2.2. Study Group and Cohort
2.3. Covariate Measurements
2.4. Outcome Definitions
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics and Baseline Demographics
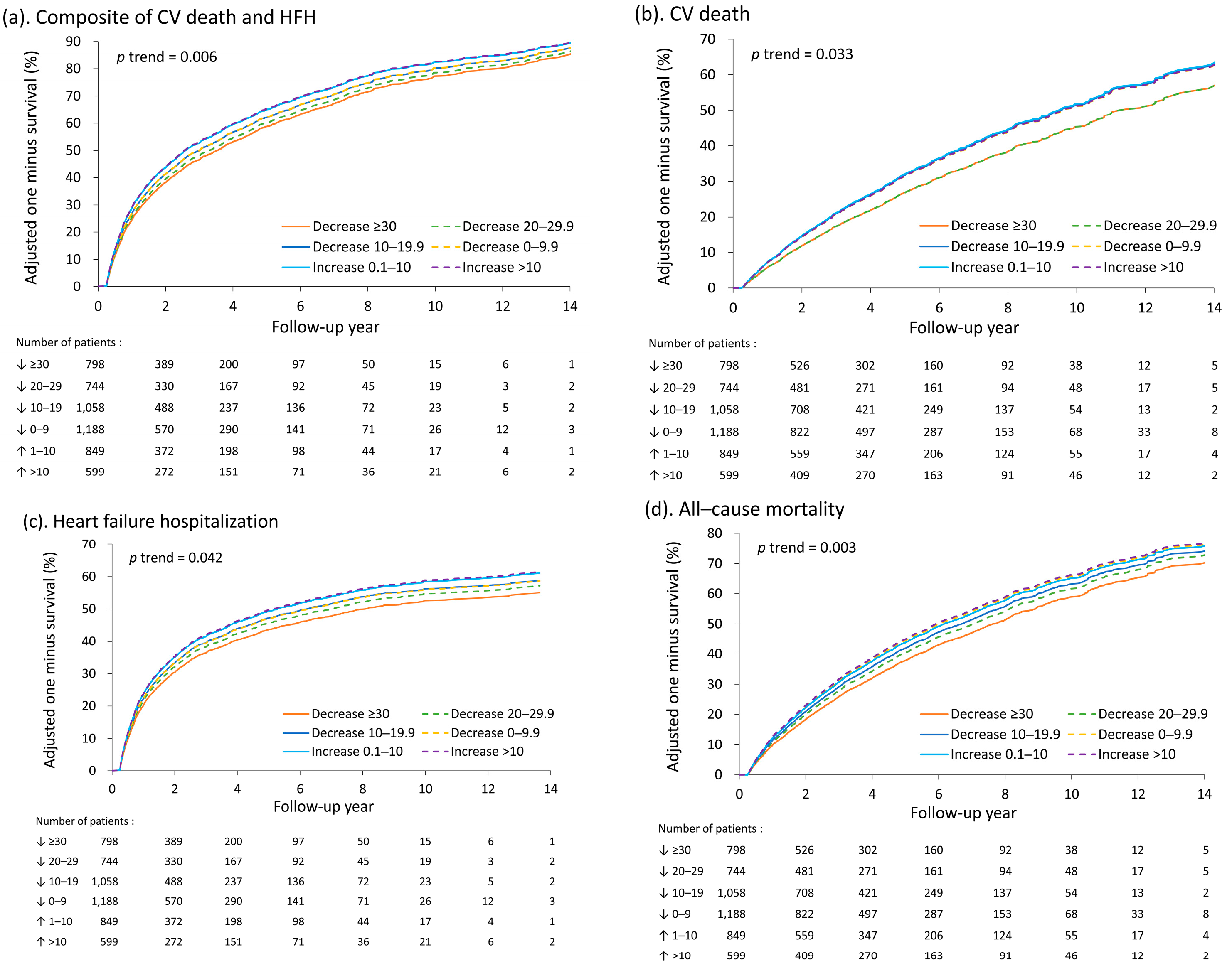
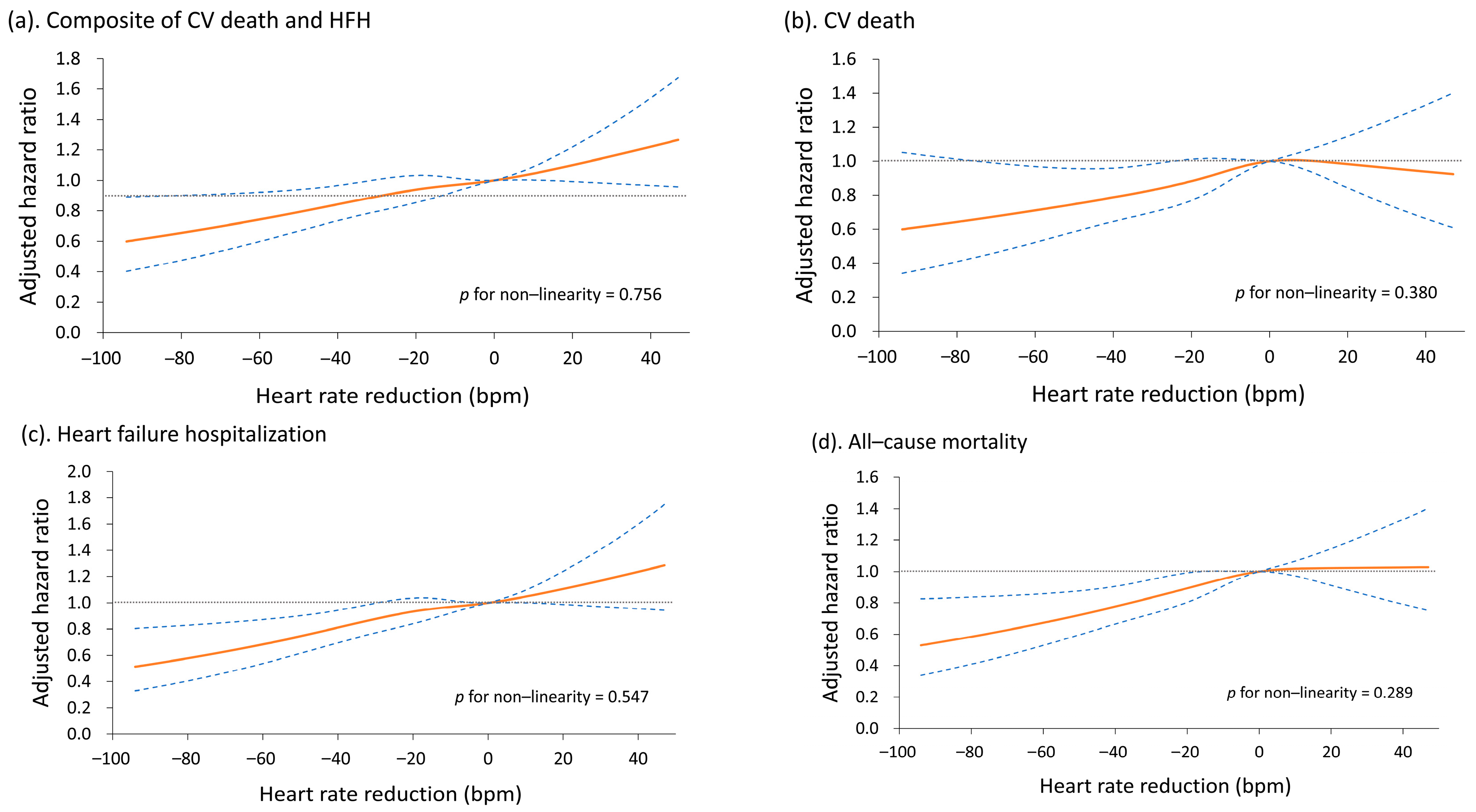
3.2. Changes in Heart Rate by the 3-Month Screening Period and Long-Term Outcomes
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jensen, M.T.; Marott, J.L.; Allin, K.H.; Nordestgaard, B.G.; Jensen, G.B. Resting heart rate is associated with cardiovascular and all-cause mortality after adjusting for inflammatory markers: The copenhagen city heart study. Eur. J. Prev. Cardiol. 2012, 19, 102–108. [Google Scholar] [CrossRef]
- Reil, J.C.; Reil, G.H.; Bohm, M. Heart rate reduction by i(f)-channel inhibition and its potential role in heart failure with reduced and preserved ejection fraction. Trends Cardiovasc. Med. 2009, 19, 152–157. [Google Scholar] [CrossRef]
- Kannel, W.B.; Kannel, C.; Paffenbarger, R.S., Jr.; Cupples, L.A. Heart rate and cardiovascular mortality: The framingham study. Am. Heart J. 1987, 113, 1489–1494. [Google Scholar] [CrossRef]
- Palatini, P.; Julius, S. Elevated heart rate: A major risk factor for cardiovascular disease. Clin. Exp. Hypertens. 2004, 26, 637–644. [Google Scholar] [CrossRef]
- Diaz, A.; Bourassa, M.G.; Guertin, M.C.; Tardif, J.C. Long-term prognostic value of resting heart rate in patients with suspected or proven coronary artery disease. Eur. Heart J. 2005, 26, 967–974. [Google Scholar] [CrossRef]
- Pocock, S.J.; Wang, D.; Pfeffer, M.A.; Yusuf, S.; McMurray, J.J.; Swedberg, K.B.; Ostergren, J.; Michelson, E.L.; Pieper, K.S.; Granger, C.B. Predictors of mortality and morbidity in patients with chronic heart failure. Eur. Heart J. 2006, 27, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.; Borer, J.S.; Camm, A.J.; Danchin, N.; Ferrari, R.; Lopez Sendon, J.L.; Steg, P.G.; Tardif, J.C.; Tavazzi, L.; Tendera, M.; et al. Resting heart rate in cardiovascular disease. J. Am. Coll. Cardiol. 2007, 50, 823–830. [Google Scholar] [CrossRef]
- Ho, J.E.; Bittner, V.; Demicco, D.A.; Breazna, A.; Deedwania, P.C.; Waters, D.D. Usefulness of heart rate at rest as a predictor of mortality, hospitalization for heart failure, myocardial infarction, and stroke in patients with stable coronary heart disease (data from the treating to new targets [tnt] trial). Am. J. Cardiol. 2010, 105, 905–911. [Google Scholar] [CrossRef]
- Hillis, G.S.; Woodward, M.; Rodgers, A.; Chow, C.K.; Li, Q.; Zoungas, S.; Patel, A.; Webster, R.; Batty, G.D.; Ninomiya, T.; et al. Resting heart rate and the risk of death and cardiovascular complications in patients with type 2 diabetes mellitus. Diabetologia 2012, 55, 1283–1290. [Google Scholar] [CrossRef]
- Reil, J.C.; Custodis, F.; Swedberg, K.; Komajda, M.; Borer, J.S.; Ford, I.; Tavazzi, L.; Laufs, U.; Bohm, M. Heart rate reduction in cardiovascular disease and therapy. Clin. Res. Cardiol. 2011, 100, 11–19. [Google Scholar] [CrossRef]
- Lan, W.R.; Lin, S.I.; Liao, F.C.; Chang, H.Y.; Tsai, C.T.; Wu, Y.J.; Liu, P.Y.; Chen, C.H.; Lee, Y.H. Effect of reducing heart rate on outcomes in patients with reduced ejection fraction. Am. J. Cardiol. 2021, 150, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Bohm, M.; Swedberg, K.; Komajda, M.; Borer, J.S.; Ford, I.; Dubost-Brama, A.; Lerebours, G.; Tavazzi, L.; Investigators, S. Heart rate as a risk factor in chronic heart failure (shift): The association between heart rate and outcomes in a randomised placebo-controlled trial. Lancet 2010, 376, 886–894. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 esc guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 aha/acc/hfsa guideline for the management of heart failure: A report of the american college of cardiology/american heart association joint committee on clinical practice guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar]
- Tsai, M.S.; Lin, M.H.; Lee, C.P.; Yang, Y.H.; Chen, W.C.; Chang, G.H.; Tsai, Y.T.; Chen, P.C.; Tsai, Y.H. Chang gung research database: A multi-institutional database consisting of original medical records. Biomed. J. 2017, 40, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Shao, S.C.; Chan, Y.Y.; Kao Yang, Y.H.; Lin, S.J.; Hung, M.J.; Chien, R.N.; Lai, C.C.; Lai, E.C. The chang gung research database-a multi-institutional electronic medical records database for real-world epidemiological studies in taiwan. Pharm. Drug Saf. 2019, 28, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Rickham, P.P. Human experimentation. Code of ethics of the world medical association. Declaration of helsinki. Br. Med. J. 1964, 2, 177. [Google Scholar] [PubMed]
- Hicks, K.A.; Mahaffey, K.W.; Mehran, R.; Nissen, S.E.; Wiviott, S.D.; Dunn, B.; Solomon, S.D.; Marler, J.R.; Teerlink, J.R.; Farb, A.; et al. 2017 cardiovascular and stroke endpoint definitions for clinical trials. Circulation 2018, 137, 961–972. [Google Scholar] [CrossRef] [PubMed]
- Maggioni, A.P.; Dahlstrom, U.; Filippatos, G.; Chioncel, O.; Leiro, M.C.; Drozdz, J.; Fruhwald, F.; Gullestad, L.; Logeart, D.; Metra, M.; et al. Eurobservational research programme: The heart failure pilot survey (esc-hf pilot). Eur. J. Heart Fail. 2010, 12, 1076–1084. [Google Scholar] [CrossRef]
- Tavazzi, L.; Senni, M.; Metra, M.; Gorini, M.; Cacciatore, G.; Chinaglia, A.; Di Lenarda, A.; Mortara, A.; Oliva, F.; Maggioni, A.P.; et al. Multicenter prospective observational study on acute and chronic heart failure: One-year follow-up results of in-hf (italian network on heart failure) outcome registry. Circ. Heart Fail 2013, 6, 473–481. [Google Scholar] [CrossRef]
- O’Connor, C.M.; Mentz, R.J.; Cotter, G.; Metra, M.; Cleland, J.G.; Davison, B.A.; Givertz, M.M.; Mansoor, G.A.; Ponikowski, P.; Teerlink, J.R.; et al. The protect in-hospital risk model: 7-day outcome in patients hospitalized with acute heart failure and renal dysfunction. Eur. J. Heart Fail. 2012, 14, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Bertomeu-Gonzalez, V.; Nunez, J.; Nunez, E.; Cordero, A.; Facila, L.; Ruiz-Granell, R.; Quiles, J.; Sanchis, J.; Bodi, V.; Minana, G.; et al. Heart rate in acute heart failure, lower is not always better. Int. J. Cardiol. 2010, 145, 592–593. [Google Scholar] [CrossRef] [PubMed]
- Greene, S.J.; Vaduganathan, M.; Wilcox, J.E.; Harinstein, M.E.; Maggioni, A.P.; Subacius, H.; Zannad, F.; Konstam, M.A.; Chioncel, O.; Yancy, C.W.; et al. The prognostic significance of heart rate in patients hospitalized for heart failure with reduced ejection fraction in sinus rhythm: Insights from the everest (efficacy of vasopressin antagonism in heart failure: Outcome study with tolvaptan) trial. JACC Heart Fail. 2013, 1, 488–496. [Google Scholar] [CrossRef] [PubMed]
- Traub, O.; Berk, B.C. Laminar shear stress: Mechanisms by which endothelial cells transduce an atheroprotective force. Arterioscler. Thromb. Vasc. Biol. 1998, 18, 677–685. [Google Scholar] [CrossRef]
- Kurgansky, K.E.; Schubert, P.; Parker, R.; Djousse, L.; Riebman, J.B.; Gagnon, D.R.; Joseph, J. Association of pulse rate with outcomes in heart failure with reduced ejection fraction: A retrospective cohort study. BMC Cardiovasc. Disord. 2020, 20, 92. [Google Scholar] [CrossRef]
- Kotecha, D.; Flather, M.D.; Altman, D.G.; Holmes, J.; Rosano, G.; Wikstrand, J.; Packer, M.; Coats, A.J.S.; Manzano, L.; Bohm, M.; et al. Heart rate and rhythm and the benefit of beta-blockers in patients with heart failure. J. Am. Coll. Cardiol. 2017, 69, 2885–2896. [Google Scholar] [CrossRef]
- Metra, M.; Torp-Pedersen, C.; Swedberg, K.; Cleland, J.G.; Di Lenarda, A.; Komajda, M.; Remme, W.J.; Lutiger, B.; Scherhag, A.; Lukas, M.A.; et al. Influence of heart rate, blood pressure, and beta-blocker dose on outcome and the differences in outcome between carvedilol and metoprolol tartrate in patients with chronic heart failure: Results from the comet trial. Eur. Heart J. 2005, 26, 2259–2268. [Google Scholar] [CrossRef]
- McAlister, F.A.; Wiebe, N.; Ezekowitz, J.A.; Leung, A.A.; Armstrong, P.W. Meta-analysis: Beta-blocker dose, heart rate reduction, and death in patients with heart failure. Ann. Intern. Med. 2009, 150, 784–794. [Google Scholar] [CrossRef]
- Bohm, M.; Borer, J.; Ford, I.; Gonzalez-Juanatey, J.R.; Komajda, M.; Lopez-Sendon, J.; Reil, J.C.; Swedberg, K.; Tavazzi, L. Heart rate at baseline influences the effect of ivabradine on cardiovascular outcomes in chronic heart failure: Analysis from the shift study. Clin. Res. Cardiol. 2013, 102, 11–22. [Google Scholar] [CrossRef]
- Wang, C.C.; Chang, H.Y.; Yin, W.H.; Wu, Y.W.; Chu, P.H.; Wu, C.C.; Hsu, C.H.; Wen, M.S.; Voon, W.C.; Lin, W.S.; et al. Tsoc-hfref registry: A registry of hospitalized patients with decompensated systolic heart failure: Description of population and management. Acta Cardiol. Sin. 2016, 32, 400–411. [Google Scholar]
- Hamill, V.; Ford, I.; Fox, K.; Bohm, M.; Borer, J.S.; Ferrari, R.; Komajda, M.; Steg, P.G.; Tavazzi, L.; Tendera, M.; et al. Repeated heart rate measurement and cardiovascular outcomes in left ventricular systolic dysfunction. Am. J. Med. 2015, 128, 1102–1108.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Variable | n | Decrease ≥30 (n = 798) | Decrease 20–29 (n = 744) | Decrease 10–19 (n = 1058) | Decrease <10 (n = 1188) | Increase 1–10 (n = 849) | Increase >10 (n = 599) | p Trend |
|---|---|---|---|---|---|---|---|---|
| Age, year | 5236 | 62.9 ± 16.7 | 63.6 ± 15.7 | 63.5 ± 15.2 | 63.2 ± 14.9 | 63.1 ± 15.1 | 61.0 ± 15.4 | 0.020 |
| Male | 5236 | 553 (69.3) | 521 (70.0) | 720 (68.1) | 804 (67.7) | 594 (70.0) | 442 (73.8) | 0.215 |
| Smoking | 5236 | 315 (39.5) | 269 (36.2) | 381 (36.0) | 428 (36.0) | 310 (36.5) | 238 (39.7) | 0.919 |
| BMI, kg/m2 | 4920 | 24.9 ± 5.1 | 24.8 ± 4.6 | 25.0 ± 4.8 | 25.1 ± 4.7 | 25.1 ± 5.1 | 25.2 ± 5.1 | 0.092 |
| Baseline vital sign | ||||||||
| SBP, mmHg | 5236 | 134.9 ± 28.2 | 134.9 ± 27.2 | 134.6 ± 27.0 | 132.9 ± 24.8 | 129.3 ± 24.6 | 129.0 ± 23.2 | <0.001 |
| DBP, mmHg | 5235 | 84.0 ± 20.1 | 81.7 ± 17.6 | 80.7 ± 18.4 | 78.7 ± 16.0 | 76.9 ± 16.0 | 77.9 ± 15.4 | <0.001 |
| Heart rate, beat/minute | 5236 | 113.9 ± 18.0 | 98.3 ± 11.2 | 92.3 ± 12.1 | 87.0 ± 10.9 | 84.3 ± 10.2 | 81.6 ± 9.2 | <0.001 |
| HF admission in the previous year | 5236 | 93 (11.7) | 112 (15.1) | 159 (15.0) | 196 (16.5) | 148 (17.4) | 123 (20.5) | <0.001 |
| No. of HF admission in the previous 3 years | 5236 | <0.001 | ||||||
| 0 | 687 (86.1) | 613 (82.4) | 866 (81.9) | 933 (78.5) | 659 (77.6) | 444 (74.1) | ||
| 1 | 89 (11.2) | 106 (14.2) | 156 (14.7) | 200 (16.8) | 144 (17.0) | 122 (20.4) | ||
| ≥2 | 22 (2.8) | 25 (3.4) | 36 (3.4) | 55 (4.6) | 46 (5.4) | 33 (5.5) | ||
| Comorbidity | ||||||||
| Coronary artery disease | 5236 | 414 (51.9) | 408 (54.8) | 621 (58.7) | 727 (61.2) | 482 (56.8) | 348 (58.1) | 0.005 |
| Myocardial infarction | 5236 | 62 (7.8) | 82 (11.0) | 118 (11.2) | 166 (14.0) | 109 (12.8) | 71 (11.9) | 0.001 |
| Hypertension | 5236 | 506 (63.4) | 499 (67.1) | 732 (69.2) | 817 (68.8) | 584 (68.8) | 393 (65.6) | 0.170 |
| Dyslipidemia | 5236 | 299 (37.5) | 310 (41.7) | 443 (41.9) | 539 (45.4) | 385 (45.3) | 239 (39.9) | 0.024 |
| Diabetes mellitus | 5236 | 318 (39.8) | 360 (48.4) | 529 (50.0) | 590 (49.7) | 430 (50.6) | 298 (49.7) | <0.001 |
| Chronic kidney disease | 5236 | 313 (39.2) | 316 (42.5) | 416 (39.3) | 495 (41.7) | 313 (36.9) | 227 (37.9) | 0.202 |
| Dialysis | 5236 | 48 (6.0) | 76 (10.2) | 109 (10.3) | 118 (9.9) | 88 (10.4) | 61 (10.2) | 0.015 |
| Stroke | 5236 | 52 (6.5) | 62 (8.3) | 79 (7.5) | 103 (8.7) | 62 (7.3) | 46 (7.7) | 0.547 |
| Chronic obstructive Pulmonary disease | 5236 | 139 (17.4) | 142 (19.1) | 160 (15.1) | 205 (17.3) | 167 (19.7) | 108 (18.0) | 0.475 |
| Peripheral arterial disease | 5236 | 55 (6.9) | 63 (8.5) | 103 (9.7) | 101 (8.5) | 87 (10.2) | 68 (11.4) | 0.005 |
| Liver cirrhosis | 5236 | 24 (3.0) | 19 (2.6) | 32 (3.0) | 29 (2.4) | 38 (4.5) | 26 (4.3) | 0.041 |
| Laboratory data | ||||||||
| BNP, pg/mL | 2884 | 1230 (599, 2239) | 1168 (565, 2290) | 1240 (612, 2449) | 1100 (514, 2190) | 1155 (509, 2580) | 1166 (500, 2239) | 0.382 |
| BUN, mg/dL | 5014 | 29.6 ± 20.9 | 31.2 ± 21.9 | 30.8 ± 22.8 | 31.0 ± 23.5 | 30.2 ± 21.7 | 30.1 ± 22.9 | 0.943 |
| Creatinine, mg/dL | 5219 | 2.0 ± 2.1 | 2.2 ± 2.4 | 2.2 ± 2.5 | 2.2 ± 2.7 | 2.2 ± 2.5 | 2.2 ± 2.6 | 0.364 |
| eGFR, mL/min/1.73 m2 | 5219 | 58.0 ± 32.7 | 57.9 ± 35.1 | 59.3 ± 34.9 | 60.7 ± 36.4 | 61.8 ± 36.4 | 63.3 ± 36.4 | <0.001 |
| Sodium (Na), mEq/L | 5197 | 137.8 ± 4.6 | 137.6 ± 4.5 | 137.9 ± 4.4 | 137.9 ± 4.3 | 138.1 ± 4.0 | 138.4 ± 3.9 | 0.001 |
| Potassium (K), mEq/L | 5204 | 3.9 ± 0.7 | 4.0 ± 0.7 | 4.0 ± 0.6 | 4.0 ± 0.6 | 4.0 ± 0.6 | 4.0 ± 0.6 | 0.045 |
| Uric acid, mg/dL | 3275 | 8.0 ± 2.8 | 7.8 ± 2.5 | 7.7 ± 2.4 | 7.5 ± 2.5 | 7.7 ± 2.5 | 7.7 ± 2.8 | 0.028 |
| AST, U/L | 4014 | 34 (24, 62) | 31 (22, 49) | 29 (22, 45) | 30 (22, 46) | 28 (21, 42) | 29 (21, 44) | <0.001 |
| ALT, U/L | 4833 | 27 (17, 54) | 25 (16, 45) | 24 (15, 42) | 25 (16, 44) | 24 (16, 40) | 22 (14, 38) | <0.001 |
| LDL-C, mg/dL | 4131 | 82.9 ± 47.8 | 83.8 ± 48.1 | 85.7 ± 49.7 | 86.6 ± 50.1 | 86.0 ± 49.2 | 88.1 ± 48.8 | 0.056 |
| Total cholesterol, mg/dL | 4275 | 167.7 ± 44.5 | 168.6 ± 46.8 | 167.8 ± 45.6 | 170.3 ± 45.3 | 166.6 ± 45.9 | 167.8 ± 44.9 | 0.859 |
| Hemoglobin, g/dL | 5228 | 12.7 ± 2.6 | 12.5 ± 2.6 | 12.5 ± 2.5 | 12.4 ± 2.5 | 12.4 ± 2.5 | 12.6 ± 2.4 | 0.613 |
| Total bilirubin, mg/dL | 3315 | 1.1 ± 0.9 | 1.0 ± 0.8 | 0.9 ± 0.7 | 0.9 ± 0.7 | 0.9 ± 0.7 | 0.9 ± 0.6 | <0.001 |
| Albumin, mg/dL | 3734 | 3.5 ± 0.6 | 3.5 ± 0.6 | 3.5 ± 0.6 | 3.5 ± 0.6 | 3.5 ± 0.6 | 3.5 ± 0.5 | 0.023 |
| Platelet, count × 103 | 5225 | 233.2 ± 86.1 | 224.3 ± 84.3 | 227.6 ± 82.4 | 218.2 ± 75.1 | 217.5 ± 82.8 | 220.9 ± 76.5 | <0.001 |
| WBC, count × 103 | 5228 | 10.8 ± 4.7 | 9.3 ± 3.8 | 9.2 ± 3.8 | 8.6 ± 3.5 | 8.5 ± 3.5 | 8.5 ± 3.2 | <0.001 |
| Echocardiography result | ||||||||
| LVEF, % | 5236 | 29.1 ± 7.7 | 29.8 ± 7.5 | 30.2 ± 7.3 | 30.5 ± 7.0 | 30.5 ± 6.9 | 30.6 ± 7.0 | <0.001 |
| LVEDD, mm | 5233 | 58.7 ± 9.1 | 59.1 ± 8.6 | 59.4 ± 8.9 | 59.0 ± 8.6 | 59.5 ± 8.4 | 59.6 ± 8.4 | 0.047 |
| LVESD, mm | 5231 | 49.8 ± 9.4 | 49.8 ± 8.8 | 49.9 ± 9.8 | 49.6 ± 8.7 | 49.9 ± 8.8 | 50.2 ± 8.6 | 0.530 |
| LA diameter, mm | 5194 | 42.5 ± 8.2 | 42.5 ± 7.4 | 42.8 ± 7.7 | 42.4 ± 7.7 | 42.3 ± 7.6 | 42.5 ± 7.9 | 0.719 |
| MR severity | 5236 | 0.133 | ||||||
| Severe | 47 (5.9) | 44 (5.9) | 92 (8.7) | 92 (7.7) | 81 (9.5) | 49 (8.2) | ||
| Moderate | 214 (26.8) | 201 (27.0) | 266 (25.1) | 307 (25.8) | 221 (26.0) | 146 (24.4) | ||
| Mild | 440 (55.1) | 411 (55.2) | 590 (55.8) | 660 (55.6) | 457 (53.8) | 348 (58.1) | ||
| Trivial/None | 89 (11.2) | 79 (10.6) | 96 (9.1) | 122 (10.3) | 82 (9.7) | 51 (8.5) | ||
| Follow up duration, month | 5236 | 46.4 ± 36.4 | 47.4 ± 38.4 | 48.4 ± 36.8 | 49.8 ± 38.2 | 49.7 ± 39.1 | 52.6 ± 40.3 | 0.001 |
| Variable | n | Decrease ≥30 (n = 798) | Decrease 20–29 (n = 744) | Decrease 10–19 (n = 1058) | Decrease <10 (n = 1188) | Increase 1–10 (n = 849) | Increase >10 (n = 599) | p Trend |
|---|---|---|---|---|---|---|---|---|
| Medication for heart failure during the index admission | ||||||||
| ARNI | 5236 | 18 (2.3) | 19 (2.6) | 27 (2.6) | 23 (1.9) | 27 (3.2) | 13 (2.2) | 0.811 |
| ACEI/ARB | 5236 | 719 (90.1) | 651 (87.5) | 916 (86.6) | 995 (83.8) | 714 (84.1) | 525 (87.6) | 0.004 |
| Beta-blocker | 5236 | 693 (86.8) | 648 (87.1) | 879 (83.1) | 953 (80.2) | 637 (75.0) | 468 (78.1) | <0.001 |
| Ivabradine | 5236 | 146 (18.3) | 71 (9.5) | 86 (8.1) | 59 (5.0) | 36 (4.2) | 25 (4.2) | <0.001 |
| MRAs | 5236 | 386 (48.4) | 317 (42.6) | 462 (43.7) | 459 (38.6) | 308 (36.3) | 207 (34.6) | <0.001 |
| Loop diuretics | 5236 | 725 (90.9) | 648 (87.1) | 895 (84.6) | 965 (81.2) | 685 (80.7) | 488 (81.5) | <0.001 |
| Digoxin | 5236 | 145 (18.2) | 100 (13.4) | 147 (13.9) | 177 (14.9) | 121 (14.3) | 94 (15.7) | 0.325 |
| Other medication during the index admission | ||||||||
| DHP-CCB | 5236 | 302 (37.8) | 293 (39.4) | 437 (41.3) | 433 (36.4) | 283 (33.3) | 211 (35.2) | 0.010 |
| Amiodarone | 5236 | 70 (8.8) | 42 (5.6) | 64 (6.0) | 66 (5.6) | 38 (4.5) | 26 (4.3) | <0.001 |
| Oral hypoglycemic agents | 5236 | 266 (33.3) | 307 (41.3) | 432 (40.8) | 489 (41.2) | 343 (40.4) | 237 (39.6) | 0.032 |
| Insulin | 5236 | 266 (33.3) | 238 (32.0) | 352 (33.3) | 346 (29.1) | 240 (28.3) | 186 (31.1) | 0.029 |
| Statin | 5236 | 363 (45.5) | 356 (47.8) | 518 (49.0) | 595 (50.1) | 371 (43.7) | 274 (45.7) | 0.579 |
| Aspirin | 5236 | 538 (67.4) | 523 (70.3) | 760 (71.8) | 873 (73.5) | 596 (70.2) | 418 (69.8) | 0.239 |
| P2Y12 | 5236 | 423 (53.0) | 400 (53.8) | 586 (55.4) | 623 (52.4) | 434 (51.1) | 303 (50.6) | 0.133 |
| In-hospital event | ||||||||
| Hospital days | 5236 | 15.1 ± 11.6 | 14.2 ± 12.2 | 13.8 ± 14.5 | 11.8 ± 10.4 | 12.1 ± 15.4 | 11.9 ± 10.9 | <0.001 |
| ICU days | 5236 | 3.0 ± 4.6 | 2.0 ± 3.8 | 2.0 ± 4.1 | 1.4 ± 3.4 | 1.1 ± 2.9 | 1.2 ± 3.0 | <0.001 |
| Shock | 5236 | 185 (23.2) | 111 (14.9) | 169 (16.0) | 153 (12.9) | 102 (12.0) | 91 (15.2) | <0.001 |
| Intubation | 5236 | 34 (4.3) | 22 (3.0) | 38 (3.6) | 24 (2.0) | 10 (1.2) | 10 (1.7) | <0.001 |
| Acute coronary syndrome | 5236 | 217 (27.2) | 166 (22.3) | 232 (21.9) | 229 (19.3) | 140 (16.5) | 102 (17.0) | <0.001 |
| PCI | 5236 | 133 (16.7) | 142 (19.1) | 184 (17.4) | 196 (16.5) | 148 (17.4) | 92 (15.4) | 0.343 |
| Medication for heart failure within 3 months after discharge | ||||||||
| Beta-blocker | 5236 | 609 (76.3) | 559 (75.1) | 706 (66.7) | 748 (63.0) | 515 (60.7) | 340 (56.8) | <0.001 |
| Ivabradine | 5236 | 113 (14.2) | 58 (7.8) | 61 (5.8) | 51 (4.3) | 33 (3.9) | 23 (3.8) | <0.001 |
| Digoxin | 5236 | 109 (13.7) | 70 (9.4) | 105 (9.9) | 121 (10.2) | 82 (9.7) | 78 (13.0) | 0.535 |
| ACEi/ARB | 5236 | 604 (75.7) | 539 (72.4) | 715 (67.6) | 790 (66.5) | 564 (66.4) | 411 (68.6) | <0.001 |
| ARNI | 5236 | 16 (2.0) | 14 (1.9) | 24 (2.3) | 16 (1.3) | 23 (2.7) | 11 (1.8) | 0.876 |
| MRAs | 5236 | 321 (40.2) | 260 (34.9) | 366 (34.6) | 363 (30.6) | 234 (27.6) | 163 (27.2) | <0.001 |
| Loop diuretics | 5236 | 554 (69.4) | 520 (69.9) | 687 (64.9) | 756 (63.6) | 523 (61.6) | 366 (61.1) | <0.001 |
| Outcome | Decrease ≥30 (n = 798) | Decrease 20–29 (n = 744) | Decrease 10–19 (n = 1058) | Decrease <10 (n = 1188) | Increase 1–10 (n = 849) | Increase >10 (n = 599) | p Trend |
|---|---|---|---|---|---|---|---|
| Composite of heart failure hospitalization and cardiovascular death | |||||||
| Model 1 | Ref | 1.08 (0.94–1.24) | 1.15 (1.01–1.30) * | 1.15 (1.02–1.30) * | 1.25 (1.10–1.42)* | 1.24 (1.07–1.42) * | <0.001 |
| Model 2 | Ref | 1.05 (0.91–1.22) | 1.12 (0.97–1.30) | 1.14 (0.97–1.32) | 1.23 (1.04–1.45)* | 1.25 (1.05–1.50) * | 0.003 |
| Model 3 | Ref | 1.05 (0.91–1.22) | 1.12 (0.96–1.29) | 1.13 (0.97–1.31) | 1.22 (1.03–1.44)* | 1.24 (1.03–1.48) * | 0.006 |
| Cardiovascular death | |||||||
| Model 1 | Ref | 1.03 (0.84–1.26) | 1.19 (0.99–1.42) | 1.09 (0.92–1.31) | 1.12 (0.93–1.36) | 1.07 (0.87–1.32) | 0.404 |
| Model 2 | Ref | 1.01 (0.81–1.26) | 1.30 (1.05–1.61) * | 1.29 (1.03–1.62) * | 1.31 (1.03–1.67) * | 1.33 (1.02–1.73) * | 0.012 |
| Model 3 | Ref | 1.01 (0.81–1.25) | 1.27 (1.02–1.57) * | 1.25 (0.998–1.57) | 1.27 (0.998–1.63) | 1.27 (0.97–1.66) | 0.033 |
| Heart failure hospitalization | |||||||
| Model 1 | Ref | 1.08 (0.93–1.26) | 1.16 (1.01–1.33) * | 1.19 (1.04–1.36) * | 1.27 (1.10–1.47) * | 1.26 (1.08–1.47) * | <0.001 |
| Model 2 | Ref | 1.07 (0.90–1.26) | 1.12 (0.95–1.32) | 1.13 (0.95–1.34) | 1.20 (1.002–1.45) * | 1.23 (1.003–1.50) * | 0.027 |
| Model 3 | Ref | 1.07 (0.91–1.27) | 1.12 (0.95–1.32) | 1.12 (0.94–1.33) | 1.20 (0.99–1.44) | 1.22 (0.99–1.49) | 0.042 |
| All-cause mortality | |||||||
| Model 1 | Ref | 1.15 (0.98–1.33) | 1.11 (0.96–1.27) | 1.13 (0.98–1.30) | 1.12 (0.97–1.30) | 1.14 (0.97–1.33) | 0.197 |
| Model 2 | Ref | 1.12 (0.95–1.32) | 1.19 (1.01–1.41)* | 1.33 (1.11–1.58) * | 1.29 (1.07–1.56) * | 1.38 (1.12–1.69) * | 0.001 |
| Model 3 | Ref | 1.11 (0.94–1.31) | 1.17 (0.99–1.39) | 1.30 (1.09–1.55) * | 1.26 (1.05–1.53) * | 1.34 (1.09–1.64) * | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, M.-L.; Lin, S.-I.; Kao, Y.-C.; Lin, H.-C.; Lin, M.-S.; Peng, J.-R.; Wang, C.-Y.; Wu, V.C.-C.; Cheng, C.-W.; Lee, Y.-H.; et al. Optimal Heart Rate Control Improves Long-Term Prognosis of Decompensated Heart Failure with Reduced Ejection Fraction. Medicina 2023, 59, 348. https://doi.org/10.3390/medicina59020348
Tsai M-L, Lin S-I, Kao Y-C, Lin H-C, Lin M-S, Peng J-R, Wang C-Y, Wu VC-C, Cheng C-W, Lee Y-H, et al. Optimal Heart Rate Control Improves Long-Term Prognosis of Decompensated Heart Failure with Reduced Ejection Fraction. Medicina. 2023; 59(2):348. https://doi.org/10.3390/medicina59020348
Chicago/Turabian StyleTsai, Ming-Lung, Shu-I Lin, Yu-Cheng Kao, Hsuan-Ching Lin, Ming-Shyan Lin, Jian-Rong Peng, Chao-Yung Wang, Victor Chien-Chia Wu, Chi-Wen Cheng, Ying-Hsiang Lee, and et al. 2023. "Optimal Heart Rate Control Improves Long-Term Prognosis of Decompensated Heart Failure with Reduced Ejection Fraction" Medicina 59, no. 2: 348. https://doi.org/10.3390/medicina59020348