
Post-Operative Complications and Risk Predictors Related to the Avulsion of Lower Impacted Third Molars
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
- Male and female;
- Age ≥ 18 years;
- Non-smoking patients;
- Complete root formation of lower IMTMs based on computed tomography scan (CT scan);
- Followed up to 3-, 7- and 21-day post-intervention.
- Pregnant or breastfeeding;
- Alcohol or drug abuse;
- Upper third molars;
- Presence of suspected neoplastic lesion close to the impacted tooth (based on CT scan);
- Presence of relevant medical history contraindicating surgical therapy;
- Patients who have not undergone periodical follow-up.
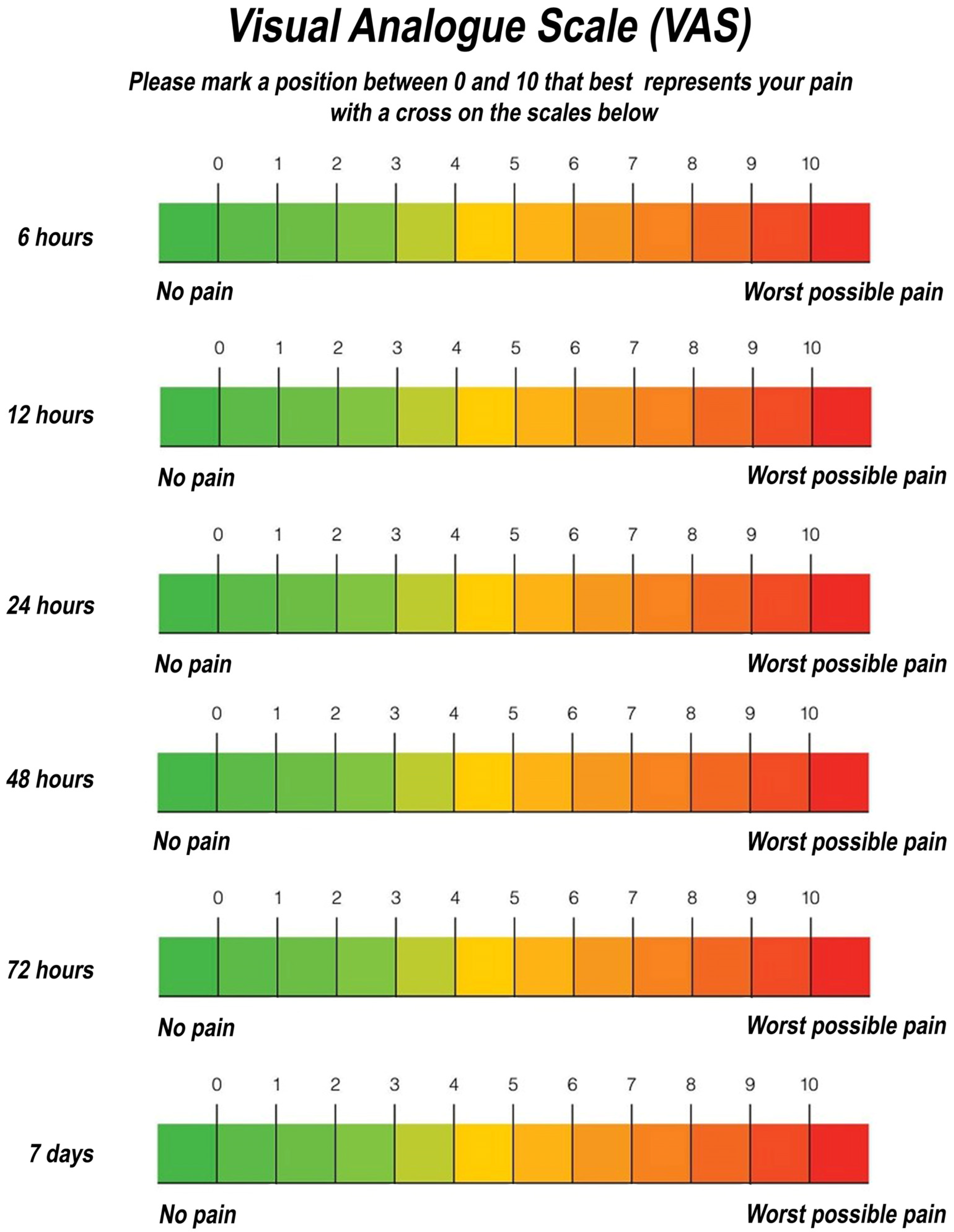
2.2. Outcome Measures
- 0–1: absence of pain;
- 2–4: mild pain;
- 5–7: moderate pain;
- 8–9: severe pain;
- 10: extremely severe pain.
- Trago to nasal border (Tr-Al);
- Trago to anatomic pogonion (TR-Pog);
- Trago to eye’s external corner (Tr-Exo);
- Trago to labial commissure (Tr-Che);
- Anatomic gonion to anatomic pogonion (Go-Pog);
- Anatomic gonion to eye’s external corner (Go-Exo);
- Anatomic gonion to nasal border (Go-Al);
- Anatomic gonion to labial commissure (Go-Che).
2.3. Clinical Procedure
2.4. Data Collection
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eklund, S.A.; Pittman, J.L. Third-molar removal patterns in an insured population. J. Am. Dent. Assoc. 2001, 132, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Ramiro-Verdugo, J.; De Vicente-Corominas, E.; Montiel-Company, J.M.; Gandía-Franco, J.L.; Bellot-Arcís, C. Association between third molar agenesis and craniofacial structure development. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 799–804. [Google Scholar] [CrossRef] [PubMed]
- Brickley, M.; Kay, E.; Shepherd, J.P.; Armstrong, R.A. Decision Analysis for lower-third-molar Surgery. Med. Decis. Mak. 1995, 15, 143–151. [Google Scholar] [CrossRef]
- Costa, M.G.; Pazzini, C.A.; Pantuzo, M.C. Is there justification for prophylactic extraction of third molars? A systemic review. Braz. Oral Res. 2013, 27, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Guerrouani, A.; Zeinoun, T.; Vervaet, C.; Legrand, W. A Four-Year Monocentric Study of the Complications of Third Molars Extractions under General Anesthesia: About 2112 Patients. Int. J. Dent. 2013, 2013, 763837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juodzbalys, G.; Daugela, P. Mandibular Third Molar Impaction: Review of Literature and a Proposal of a Classification. J. Oral Maxillofac. Res. 2013, 4, e1. [Google Scholar] [CrossRef]
- Susarla, S.; Dodson, T.B. Estimating third molar extraction difficulty: A comparison of subjective and objective factors. J. Oral Maxillofac. Surg. 2005, 63, 427–434. [Google Scholar] [CrossRef]
- Bui, C.H.; Seldin, E.B.; Dodson, T.B. Types, frequencies, and risk factors for complications after third molar extraction. J. Oral Maxillofac. Surg. 2003, 61, 1379–1389. [Google Scholar] [CrossRef]
- Blondeau, F.; Daniel, N.G. Extraction of impacted mandibular third molars: Postoperative complications and their risk factors. J. Can. Dent. Assoc. 2007, 73, 325–327. [Google Scholar]
- Xu, G.-Z.; Yang, C.; Fan, X.-D.; Yu, C.-Q.; Cai, X.-Y.; Wang, Y.; He, D. Anatomic relationship between impacted third mandibular molar and the mandibular canal as the risk factor of inferior alveolar nerve injury. Br. J. Oral Maxillofac. Surg. 2013, 51, e215–e219. [Google Scholar] [CrossRef]
- Garcia, A.G.; Sampedro, F.G.; Rey, J.G. Pell Gregory classification is unreliable as a predictor of difficulty in extracting impacted lower third molars. Br. J. Oral Maxillofac. Surg. 2000, 38, 585–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diniz-Freitas, M.; Lago-Méndez, L.; Gude-Sampedro, F.; Martín, J.M.S.; Gándara-Rey, J.M.; Garcia-Garcia, A. Pederson scale fails to predict how difficult it will be to extract lower third molars. Br. J. Oral Maxillofac. Surg. 2007, 45, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.-L.; Jiang, E.-S.; Cui, L.-Y.; Li, J.-X. Cone-Beam Computed Tomography Analysis on the Relationship between the Mandibular Third Molar and the Position of the Mandibular Canal in Koreans from the Yanbian Area and the Han People. Int. J. Clin. Pract. 2023, 2023, 9563476. [Google Scholar] [CrossRef] [PubMed]
- Sifuentes-Cervantes, J.S.; Carrillo-Morales, F.; Castro-Núñez, J.; Cunningham, L.L.; Van Sickels, J.E. Third molar surgery: Past, present, and the future. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 132, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, E.; Arduino, P.G.; Schierano, G.; Ferrero, L.; Gallesio, G.; Mozzati, M.; Russo, A.; Scully, C.; Carossa, S. A Split-Mouth Randomized Clinical Trial to Evaluate the Performance of Piezosurgery Compared with Traditional Technique in Lower Wisdom Tooth Removal. J. Oral Maxillofac. Surg. 2014, 72, 1890–1897. [Google Scholar] [CrossRef]
- Alkadi, S.; Stassen, L. Effect of One-Suture and Sutureless Techniques on Postoperative Healing After Third Molar Surgery. J. Oral Maxillofac. Surg. 2019, 77, 703–716. [Google Scholar] [CrossRef]
- Barone, A.; Marconcini, S.; Giacomelli, L.; Rispoli, L.; Calvo, J.L.; Covani, U. A Randomized Clinical Evaluation of Ultrasound Bone Surgery Versus Traditional Rotary Instruments in Lower Third Molar Extraction. J. Oral Maxillofac. Surg. 2010, 68, 330–336. [Google Scholar] [CrossRef]
- López-Cedrún, J.L.; Pijoan, J.I.; Fernández, S.; Santamaria, J.; Hernández, G. Efficacy of Amoxicillin Treatment in Preventing Postoperative Complications in Patients Undergoing Third Molar Surgery: A Prospective, Randomized, Double-Blind Controlled Study. J. Oral Maxillofac. Surg. 2011, 69, e5–e14. [Google Scholar] [CrossRef]
- Monaco, G.; Staffolani, C.; Gatto, M.R.; Checchi, L. Antibiotic therapy in impacted third molar surgery. Eur. J. Oral Sci. 1999, 107, 437–441. [Google Scholar] [CrossRef]
- Poeschl, P.W.; Eckel, D.; Poeschl, E. Postoperative prophylactic antibiotic treatment in third molar surgery—A necessity? J. Oral Maxillofac. Surg. 2004, 62, 3–8. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Di Spirito, F.; Amato, A.; Caggiano, M.; Giudice, R.L.; Martina, S. Attitudes towards Antibiotic Prescription and Antimicrobial Resistance Awareness among Italian Dentists: What Are the Milestones? Healthcare 2022, 10, 1585. [Google Scholar] [CrossRef] [PubMed]
- Cervino, G.; Cicciù, M.; Biondi, A.; Bocchieri, S.; Herford, A.S.; Laino, L.; Fiorillo, L. Antibiotic Prophylaxis on Third Molar Extraction: Systematic Review of Recent Data. Antibiotics 2019, 8, 53. [Google Scholar] [CrossRef] [Green Version]
- Albuquerque, A.; Fonteles, C.; Val, D.D.; Chaves, H.; Bezerra, M.; Pereira, K.; Silva, P.D.B.; de Lima, B.; Soares, E.; Ribeiro, T.; et al. Effect of pre-emptive analgesia on clinical parameters and tissue levels of TNF-α and IL-1β in third molar surgery: A triple-blind, randomized, placebo-controlled study. Int. J. Oral Maxillofac. Surg. 2017, 46, 1615–1625. [Google Scholar] [CrossRef] [Green Version]
- Gazal, G.; Al-Samadani, K.H. Comparison of paracetamol, ibuprofen, and diclofenac potassium for pain relief following dental extractions and deep cavity preparations. Saudi Med. J. 2017, 38, 284–291. [Google Scholar] [CrossRef] [PubMed]
- McGrath, C.; Comfort, M.; Lo, E.; Luo, Y. Changes in life quality following third molar surgery, the immediate postoperative period. Br. Dent. J. 2003, 195, 265–268. [Google Scholar] [CrossRef]
- Phillips, C.; White, R.P., Jr.; Shugars, D.A.; Zhou, X. Risk factors associated with prolonged recovery and delayed healing after third molar surgery. J. Oral Maxillofac. Surg. 2003, 61, 1436–1448. [Google Scholar] [CrossRef]
- Cunningham, S.; Hunt, N.; Feinmann, C. Perceptions of outcome following orthognathic surgery. Br. J. Oral Maxillofac. Surg. 1996, 34, 210–213. [Google Scholar] [CrossRef]
- Costa, F.; Soares, E.; Esses, D.; Silva, P.D.; Bezerra, T.; Scarparo, H.; Ribeiro, T.; Fonteles, C. A split-mouth, randomized, triple-blind, placebo-controlled study to analyze the pre-emptive effect of etoricoxib 120mg on inflammatory events following removal of unerupted mandibular third molars. Int. J. Oral Maxillofac. Surg. 2015, 44, 1166–1174. [Google Scholar] [CrossRef]
- Isola, G.; Matarese, M.; Ramaglia, L.; Cicciù, M. Evaluation of the efficacy of celecoxib and ibuprofen on postoperative pain, swelling, and mouth opening after surgical removal of impacted third molars: A randomized, controlled clinical trial. Int. J. Oral Maxillofac. Surg. 2019, 48, 1348–1354. [Google Scholar] [CrossRef]
- Stone, H.H.; Hooper, C.A.; Kolb, L.D.; Geheber, C.E.; Dawkins, E.J. Antibiotic Prophylaxis in Gastric, Biliary and Colonic Surgery. Ann. Surg. 1976, 184, 443–452. [Google Scholar] [CrossRef]
- Classen, D.C.; Evans, R.S.; Pestotnik, S.L.; Horn, S.D.; Menlove, R.L.; Burke, J.P. The Timing of Prophylactic Administration of Antibiotics and the Risk of Surgical-Wound Infection. N. Engl. J. Med. 1992, 326, 281–286. [Google Scholar] [CrossRef]
- Isola, G.; Matarese, M.; Ramaglia, L.; Iorio-Siciliano, V.; Cordasco, G.; Matarese, G. Efficacy of a drug composed of herbal extracts on postoperative discomfort after surgical removal of impacted mandibular third molar: A randomized, triple-blind, controlled clinical trial. Clin. Oral Investig. 2019, 23, 2443–2453. [Google Scholar] [CrossRef] [PubMed]
- Kruger, E.; Thomson, W.M.; Konthasinghe, P. Third molar outcomes from age 18 to 26: Findings from a population-based New Zealand longitudinal study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2001, 92, 150–155. [Google Scholar] [CrossRef]
- Santos, K.K.; Lages, F.S.; Maciel, C.A.B.; Glória, J.C.R.; Douglas-De-Oliveira, D.W. Prevalence of Mandibular Third Molars According to the Pell & Gregory and Winter Classifications. J. Maxillofac. Oral Surg. 2022, 21, 627–633. [Google Scholar] [CrossRef]
- Smith, W. The relative risk of neurosensory deficit following removal of mandibular third molar teeth: The influence of radiography and surgical technique. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Gidron, Y.; McGrath, P.J.; Goodday, R. The physical and psychosocial predictors of Adolescents’ recovery from oral surgery. J. Behav. Med. 1995, 18, 385–399. [Google Scholar] [CrossRef] [PubMed]
- Lago-Méndez, L.; Diniz-Freitas, M.; Senra-Rivera, C.; Gude-Sampedro, F.; Rey, J.M.G.; García-García, A. Relationships Between Surgical Difficulty and Postoperative Pain in Lower Third Molar Extractions. J. Oral Maxillofac. Surg. 2007, 65, 979–983. [Google Scholar] [CrossRef]
- Alvira-Gonzalez, J.; Figueiredo, R.; Valmaseda-Castellon, E.; Quesada-Gomez, C.; Escoda, C.G. Predictive factors of difficulty in lower third molar extraction: A prospective cohort study. Med. Oral Patol. Oral Y Cir. Bucal 2017, 22, e108–e114. [Google Scholar] [CrossRef] [Green Version]
- Sharif, K.; Watad, A.; Bragazzi, N.L.; Lichtbroun, M.; Amital, H.; Shoenfeld, Y. Physical activity and autoimmune diseases: Get moving and manage the disease. Autoimmun. Rev. 2018, 17, 53–72. [Google Scholar] [CrossRef]
- Peterson, L.J.; Miyawaki, T.; Maeda, S.; Shimada, M. Elevation of plasma interleukin-6 level in patients undergoing oral and maxillofacial surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 1996, 81, 15–20. [Google Scholar] [CrossRef]
- Yuasa, H.; Sugiura, M. Clinical postoperative findings after removal of impacted mandibular third molars: Prediction of postoperative facial swelling and pain based on preoperative variables. Br. J. Oral Maxillofac. Surg. 2004, 42, 209–214. [Google Scholar] [CrossRef] [PubMed]
- De Menezes, S.; Cury, P. Efficacy of nimesulide versus meloxicam in the control of pain, swelling and trismus following extraction of impacted lower third molar. Int. J. Oral Maxillofac. Surg. 2010, 39, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Barbalho, J.; Vasconcellos, R.; de Morais, H.; Santos, L.; Almeida, R.D.A.; Rêbelo, H.; Lucena, E.; de Araújo, S. Effects of co-administered dexamethasone and nimesulide on pain, swelling, and trismus following third molar surgery: A randomized, triple-blind, controlled clinical trial. Int. J. Oral Maxillofac. Surg. 2017, 46, 236–242. [Google Scholar] [CrossRef]
- Bartuli, F.N.; Luciani, F.; Caddeo, F. Piezosurgery vs High Speed Rotary Handpiece: A comparison between the two techniques in the impacted third molar surgery. Oral Implantol. 2013, 6, 5–10. [Google Scholar] [CrossRef] [Green Version]
- Kaposvári, I.; Körmöczi, K.; Csurgay, K.; Horváth, F.; Ashourioun, A.H.; Buglyó, A.; Turai, A.R.; Joób-Fancsaly, Á. Delayed-onset infections after lower third molar surgery: A Hungarian case-control study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 132, 641–647. [Google Scholar] [CrossRef]
- Rahpeyma, A.; Khajehahmadi, S.; Ilkhani, S. Wound Dehiscence after Wisdom Tooth Removal in Mandibular Mesioangular Class IB Impactions: Triangular Transposition Flap versus Envelope Flap. J. Dent. Res. Dent. Clin. Dent. Prospect. 2015, 9, 175–180. [Google Scholar] [CrossRef]
- Nogami, S.; Yamauchi, K.; Shiiba, S.; Kataoka, Y.; Hirayama, B.; Takahashi, T. Evaluation of the Treatment Modalities for Neurosensory Disturbances of the Inferior Alveolar Nerve Following Retromolar Bone Harvesting for Bone Augmentation. Pain Med. 2015, 16, 501–512. [Google Scholar] [CrossRef] [Green Version]
- Grossi, G.B.; Maiorana, C.; Garramone, R.A.; Borgonovo, A.; Creminelli, L.; Santoro, F. Assessing Postoperative Discomfort After Third Molar Surgery: A Prospective Study. J. Oral Maxillofac. Surg. 2007, 65, 901–917. [Google Scholar] [CrossRef]
- Sarikov, R.; Juodzbalys, G. Inferior Alveolar Nerve Injury after Mandibular Third Molar Extraction: A Literature Review. J. Oral Maxillofac. Res. 2014, 5, e1. [Google Scholar] [CrossRef]
- Lo Giudice, R.; Puleio, F.; Rizzo, D.; Alibrandi, A.; Lo Giudice, G.; Centofanti, A.; Fiorillo, L.; Di Mauro, D.; Nicita, F. Comparative Investigation of Cutting Devices on Bone Blocks: An SEM Morphological Analysis. Appl. Sci. 2019, 9, 351. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
 | Class | |
| Class I | There is enough space between the ramus and the distal surface of the second molar for the accommodation of the mesiodistal size of the crown of the third molar | |
| Class II | The space between the ramus and the distal surface of the second molar is less than the mesiodistal size of the crown of the third molar | |
| Class III | All or most of the third molar is located within the ramus | |
| Position | ||
| Position A | The highest point of the tooth is on level or above the occlusal plane of the second molar | |
| Position B | The highest point of the tooth is below the occlusal plane but above the cervical line of the second molar | |
| Position C | The highest point of the tooth is below the cervical line of the second molar | |
| Patients (N = 25) | % | ||
|---|---|---|---|
| Gender | Female = 21 Male = 4 | 84% 16% | |
| Mean age | 25 ± 3 years | ||
| Systemic disease | Healthy (ASA Index ≤ 2) = 22 Multiple sclerosis (MS) = 2 Fibromyalgia (FMS) = 1 | 88% 8% 4% | |
| Reason of surgery | Dysodontiasis Severe tooth decay Orthodontics Periodontal | =15 =3 =4 =3 | 60% 12% 16% 12% |
| Inclusion type | Partially impacted Totally impacted | =15 =10 | 60% 40% |
| Surgical site | Third molar dx (4.8) Third molar sin (3.8) | =14 = 11 | 56% 44% |
| Patients (N = 25) | % | ||
|---|---|---|---|
| Classification (Pell and Gregory) | BII AII BIII CII | =9 =7 =5 =4 | 36% 28% 20% 16% |
| Angulation | Vertical Mesio-inclined Horizontal | =10 =7 =8 | 40% 28% 32% |
| Root anatomy | Fused roots Separated roots Buttoned roots | =13 =11 =1 | 52% 44% 4% |
| IAN relationship | Proximity > 2 mm Proximity ≤ 2 mm Continuity | =14 =8 =3 | 56% 32% 12% |
| Pericoronaritis | Yes No | =15 =10 | 60% 40% |
| Average duration of oral surgery | 35 ± 5 min | ||
| Patients (N = 25) | ||||||
|---|---|---|---|---|---|---|
| VAS Score | 6 h | 12 h | 24 h | 48 h | 72 h | 7 Days |
| 0–1 | 4 (16%) | 4 (16%) | 4 (16%) | 4 (16%) | 19 (76%) | 25 (100%) |
| 2–4 | 11 (44%) | 12 (48%) | 17 (68%) | 17 (68%) | 6 (24%) | 0 (0%) |
| 5–7 | 8 (32%) | 8 (32%) | 4 (16%) | 4 (16%) | 0 (0%) | 0 (0%) |
| 8–9 | 2 (8%) | 1 (4%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| 10 | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Patients (N = 25) | |||
|---|---|---|---|
| Follow Up | Trismus | Average Interincisal Distance Difference (from Baseline) | |
| 3-day | Yes No | =5 (20%) =20 (80%) | 7 mm ± 3 |
| 7-day | Yes No | =4 (16%) =21 (84%) | 3 mm ± 3 |
| 21-day | Yes No | =0 (0%) =25 (100%) | 0 mm ± 3 |
| Patients (N = 25) | |||
|---|---|---|---|
| Follow Up | Edema | Facial Measurements | Average Facial and Gnathological Measurements Differences (from Baseline) |
| 3-day | Yes = 16 (64%) No = 9 (36%) |
|
|
|
| ||
|
| ||
|
| ||
|
| ||
|
| ||
|
| ||
|
| ||
| 7-day | Yes = 3 (12%) No = 22 (88%) |
|
|
|
| ||
|
| ||
|
| ||
|
| ||
|
| ||
|
| ||
|
| ||
| 21-day | Yes = 0 (0%) No = 25 (100%) | / | / |
| Follow up | Complication | Patients (N = 25) | % |
|---|---|---|---|
| 3-day | Alveolitis | Yes = 3 No = 22 | 12% 88% |
| Dehiscence | Yes = 0 No = 25 | 0% 100% | |
| Nevralgic injury | Yes = 1 No = 24 | 4% 96% | |
| Suppuration | Yes = 0 No = 25 | 0% 100% | |
| 7-day | Alveolitis | Yes = 1 No = 24 | 4% 96% |
| Dehiscence | Yes = 0 No = 25 | 0% 100% | |
| Nevralgic injury | Yes = 1 No = 24 | 4% 96% | |
| Suppuration | Yes = 0 No = 25 | 0% 100% | |
| 21-day | Alveolitis | Yes = 0 No = 25 | 0% 100% |
| Dehiscence | Yes = 0 No = 25 | 0% 100% | |
| Nevralgic injury | Yes = 1 No = 24 | 4% 96% | |
| Suppuration | Yes = 0 No = 25 | 0% 100% | |
| Model Summary | ||||||
| Model | R | R-square | Adapted R-square | Std. error of the estimate | ||
| 1 | 0.828 a | 0.685 | 0.496 | 0.605 | ||
| ANOVA | ||||||
| 1 | Sum of squares | df | Mean Square | F | Sign. | |
| Regression | 11.946 | 9 | 1.327 | 3.624 | 0.14 a | |
| Residual | 5.494 | 15 | 0.366 | |||
| Total | 17.440 | 24 | ||||
| Coefficients | ||||||
| 1 | Non-standardized coefficients | Standardized coefficients | ||||
| B | Standard Error | Beta | t | Sign. | ||
| (Constant) | 3.384 | 2.127 | 0.133 | |||
| Pell and Gregory classification | 0.255 | 0.299 | 0.243 | 0.854 | 0.406 | |
| IAN relationship | 0.392 | 0.280 | 0.327 | 1.401 | 0.182 | |
| Duration of oral surgery | 1.279 | 0.384 | 0.808 | 3.329 | 0.005 | |
| Systemic disease | 0.405 | 0.428 | 0.284 | 0.946 | 0.359 | |
| Edema at 3-day | 0.037 | 0.309 | ||||
| Edema at 7-day | 0.089 | 0.489 | ||||
| Trismus at 3-day | 0.550 | 0.385 | 0.319 | 1.428 | 0.174 | |
| Trismus at 7-day | 0.689 | 0.855 | ||||
| Angulation | 0.107 | 0.204 | 0.108 | 0.525 | 0.607 | |
| Model Summary | ||||||
| Model | R | R-square | Adapted R-square | Std. error of the estimate | ||
| 1 | 0.839a | 0.703 | 0.526 | 0.537 | ||
| ANOVA | ||||||
| 1 | Sum of squares | df | Mean Square | F | Sign. | |
| Regression | 10.242 | 9 | 1.138 | 3.954 | 0.009 a | |
| Residual | 4.138 | 15 | 0.288 | |||
| Total | 14.560 | 24 | ||||
| Coefficients | ||||||
| 1 | Non-standardized coefficients | Standardized coefficients | ||||
| B | Standard Error | Beta | t | Sign. | ||
| (Constant) | 3.971 | 1.886 | 0.052 | |||
| Pell and Gregory classification | 0.119 | 0.265 | 0.124 | 0.448 | 0.660 | |
| IAN relationship | 0.234 | 0.248 | 0.214 | 0.944 | 0.360 | |
| Duration of oral surgery | 1.209 | 0.341 | 0.836 | 3.351 | 0.003 | |
| Systemic disease | 0.380 | 1.858 | 0.083 | |||
| Edema at 3-day | 0.032 | 0.600 | ||||
| Edema at 7-day | 0.034 | 0.079 | 0.115 | 0.429 | 0.674 | |
| Trismus at 3-day | 0.458 | 0.342 | 0.290 | 1.340 | 0.200 | |
| Trismus at 7-day | 0.582 | 0.611 | 0.305 | 0.952 | 0.356 | |
| Angulation | 0.117 | 0.181 | 0.129 | 0.646 | 0.528 | |
| Classification Table a,b | |||||||||
| Observed | Predicted | ||||||||
| Complications | Percentage correct | ||||||||
| No (0) | Yes (1) | ||||||||
| Step 0 | Complications | No (0) | 21 | 0 | 100.0 | ||||
| Yes (1) | 4 | 0 | 0.0 | ||||||
| Overall percentage | 84.0 | ||||||||
| Variables in the Equation | |||||||||
| Step 0 | B | S.E. | Wald | df | Sign. | Exp (B) | |||
| Constant | 0.546 | 9.239 | 1 | 0.002 | 0.190 | ||||
| Variables not in the Equation a | |||||||||
| Step 0 | Score | df | Sign. | ||||||
| Variables | Angulation | 0.043 | 1 | 0.836 | |||||
| Pell and Gregory classification | 6.361 | 1 | 0.12 | ||||||
| IAN relationship | 1.895 | 1 | 1.169 | ||||||
| Duration of oral surgery | 8.622 | 1 | 0.003 | ||||||
| Systemic disease | 14.187 | 1 | 0.000 | ||||||
| VAS at 6-h | 9.505 | 1 | 0.002 | ||||||
| VAS at 12-h | 4.723 | 1 | 0.030 | ||||||
| VAS at 24-h | 3.720 | 1 | 0.054 | ||||||
| VAS at 48-h | 3.720 | 1 | 0.054 | ||||||
| VAS at 72-h | 1.765 | 1 | 0.184 | ||||||
| Trismus at 3-day | 6.857 | 1 | 0.009 | ||||||
| Trismus at 7-day | 9.003 | 1 | 0.003 | ||||||
| Edema at 3-day | 11.049 | 1 | 0.001 | ||||||
| Edema at 7-day | 6.512 | 1 | 0.011 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blasi, A.; Cuozzo, A.; Marcacci, R.; Isola, G.; Iorio-Siciliano, V.; Ramaglia, L. Post-Operative Complications and Risk Predictors Related to the Avulsion of Lower Impacted Third Molars. Medicina 2023, 59, 534. https://doi.org/10.3390/medicina59030534
Blasi A, Cuozzo A, Marcacci R, Isola G, Iorio-Siciliano V, Ramaglia L. Post-Operative Complications and Risk Predictors Related to the Avulsion of Lower Impacted Third Molars. Medicina. 2023; 59(3):534. https://doi.org/10.3390/medicina59030534
Chicago/Turabian StyleBlasi, Andrea, Alessandro Cuozzo, Renata Marcacci, Gaetano Isola, Vincenzo Iorio-Siciliano, and Luca Ramaglia. 2023. "Post-Operative Complications and Risk Predictors Related to the Avulsion of Lower Impacted Third Molars" Medicina 59, no. 3: 534. https://doi.org/10.3390/medicina59030534