
Importance of Retesting for the Final Diagnosis of Post-Stroke Cognitive Impairment


Abstract
:1. Introduction
2. Materials and Methods
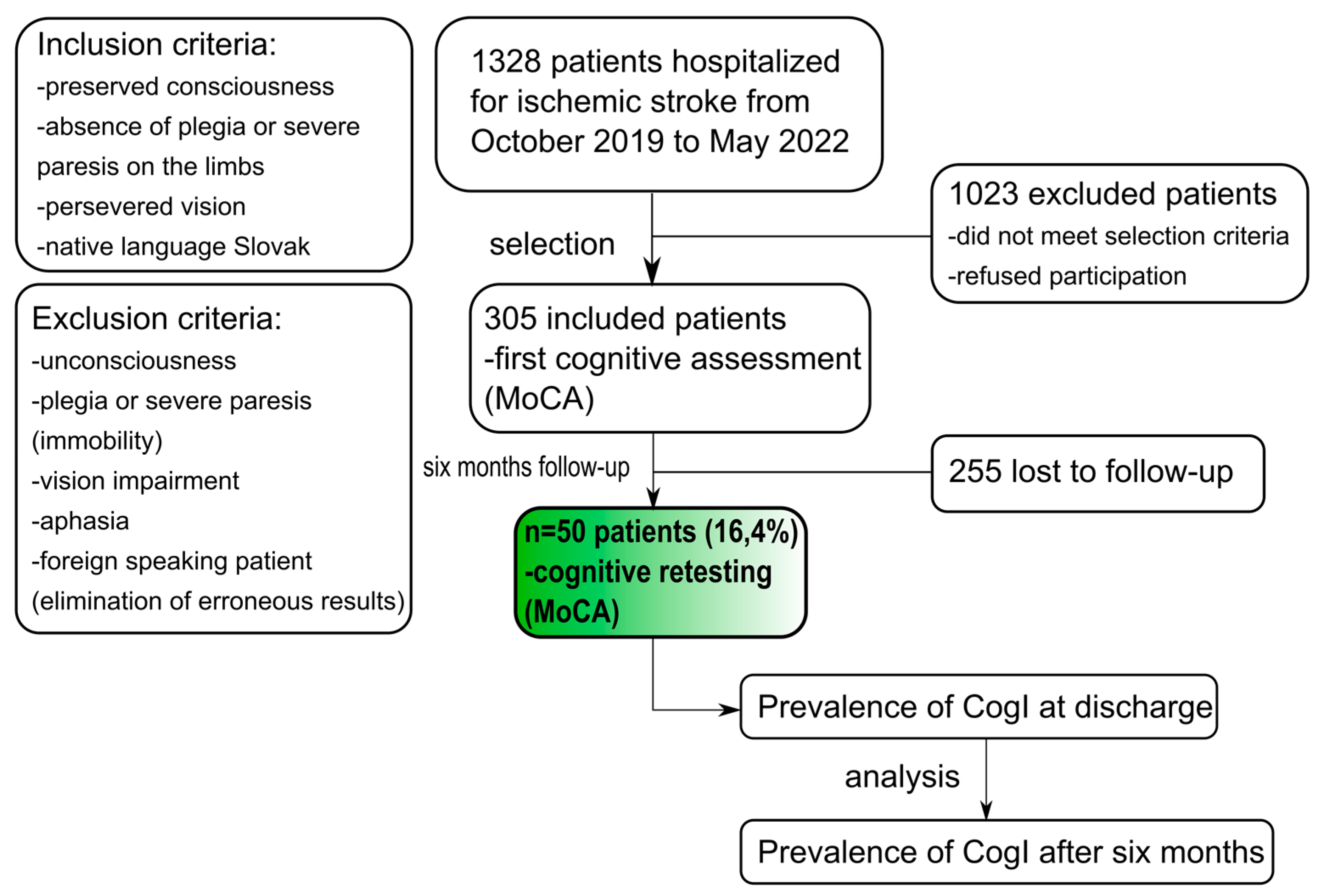
2.1. Study Participants
2.2. Evaluation Tools
2.3. Study Protocol
2.4. Statistical Analysis
3. Results
3.1. Basic Characteristics of Patients with Follow-Up Observation
3.2. CogI in the Follow-Up Cohort
3.3. Risk Factors and CogI
3.4. Imaging Procedures and CogI
4. Discussion
4.1. Prevalence of PSCI
4.2. Risk Factors for CogI at Discharge
4.3. Factors Modifying Cognition in the Post-Stroke Period
4.4. CT/MRI Findings and CogI
4.5. Clinical Implications
4.6. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Dementia Forecasting Collaborators. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: An analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2022, 7, e105–e125. [Google Scholar] [CrossRef] [PubMed]
- Cao, Q.; Tan, C.-C.; Xu, W.; Hu, H.; Cao, X.-P.; Dong, Q.; Tan, L.; Yu, J.-T. The Prevalence of Dementia: A Systematic Review and Meta-Analysis. J. Alzheimer’s Dis. 2020, 73, 1157–1166. [Google Scholar] [CrossRef] [PubMed]
- Weaver, N.A.; Kuijf, H.J.; Aben, H.P.; Abrigo, J.; Bae, H.-J.; Barbay, M.; Best, J.G.; Bordet, R.; Chappell, F.M.; Chen, C.P.L.H.; et al. Strategic infarct locations for post-stroke cognitive impairment: A pooled analysis of individual patient data from 12 acute ischaemic stroke cohorts. Lancet Neurol. 2021, 20, 448–459. [Google Scholar] [CrossRef]
- Zhao, L.; Biesbroek, J.M.; Shi, L.; Liu, W.; Kuijf, H.J.; Chu, W.W.; Chu, W.W.; Abrigo, J.; Lee, R.K.; Leung, T.; et al. Strategic infarct location for post-stroke cognitive impairment: A multivariate lesion-symptom mapping study. J. Cereb. Blood Flow. Metab. 2018, 38, 1299–1311. [Google Scholar] [CrossRef] [PubMed]
- Skrobot, O.A.; O’Brien, J.; Black, S.; Chen, C.; DeCarli, C.; Erkinjuntti, T.; Ford, G.A.; Kalaria, R.N.; Pantoni, L.; Pasquier, F.; et al. The Vascular Impairment of Cognition Classification Consensus Study. Alzheimers Dement 2017, 13, 624–633. [Google Scholar] [CrossRef] [Green Version]
- Mijajlović, M.D.; Pavlović, A.; Brainin, M.; Heiss, W.D.; Quinn, T.J.; Ihle-Hansen, H.B.; Hermann, D.M.; Assayag, E.B.; Richard, E.; Thiel, A.; et al. Post-stroke dementia—A comprehensive review. BMC Med. 2017, 15, 11. [Google Scholar] [CrossRef] [Green Version]
- Quinn, T.J.; Richard, E.; Teuschl, Y.; Gattringer, T.; Hafdi, M.; O’Brien, J.T.; Merriman, N.; Gillebert, C.; Huygelier, H.; Verdelho, A.; et al. European Stroke Organisation and European Academy of Neurology joint guidelines on post-stroke cognitive impairment. Eur. J. Neurol. 2021, 28, 3883–3920. [Google Scholar] [CrossRef]
- George, M.G. Risk Factors for Ischemic Stroke in Younger Adults: A Focused Update. Stroke 2020, 51, 729–735. [Google Scholar] [CrossRef]
- Yahya, T.; Jilani, M.H.; Khan, S.U.; Mszar, R.; Hassan, S.Z.; Blaha, M.J.; Blankstein, R.; Virani, S.S.; Johansen, M.C.; Vahidy, F.; et al. Stroke in young adults: Current trends, opportunities for prevention and pathways forward. Am. J. Prev. Cardiol. 2020, 3, 100085. [Google Scholar] [CrossRef]
- Pendlebury, S.T.; Rothwell, P.M. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: A systematic review and meta-analysis. Lancet Neurol. 2009, 8, 1006–1018. [Google Scholar] [CrossRef]
- Russo, V.; Vio, R.; Proietti, R. Stroke, Dementia, and Atrial Fibrillation: From Pathophysiologic Association to Pharmacological Implications. Medicina 2020, 56, 227. [Google Scholar] [CrossRef] [PubMed]
- Chiti, G.; Pantoni, L. Use of Montreal Cognitive Assessment in patients with stroke. Stroke 2014, 45, 3135–3140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hage, A.V. The NIH stroke scale: A window into neurological status. Nurs. Spectr. 2011, 24, 44–49. [Google Scholar]
- van Swieten, J.C.; Koudstaal, P.J.; Visser, M.C.; Schouten, H.J.; van Gijn, J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef] [Green Version]
- Adams, H.P.; Jr Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E. III Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of ORG 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Aam, S.; Einstad, M.S.; Munthe-Kaas, R.; Lydersen, S.; Ihle-Hansen, H.; Knapskog, A.-B.; Ellekjær, H.; Seljeseth, Y.; Saltvedt, I. Post-stroke Cognitive Impairment—Impact of Follow-Up Time and Stroke Subtype on Severity and Cognitive Profile: The Nor-COAST Study. Front. Neurol. 2020, 11, 699. [Google Scholar] [CrossRef]
- Jacquin, A.; Binquet, C.; Rouaud, O.; Graule-Petot, A.; Daubail, B.; Osseby, G.-V.; Bonithon-Kopp, C.; Giroud, M.; Béjot, Y. Post-Stroke Cognitive Impairment: High Prevalence and Determining Factors in a Cohort of Mild Stroke. J. Alzheimer’s Dis. 2014, 40, 1029–1038. [Google Scholar] [CrossRef]
- Douiri, A.; Rudd, A.G.; Wolfe, C.D. Prevalence of poststroke cognitive impairment: South London Stroke Register 1995–2010. Stroke 2013, 44, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Yu, K.-H.; Cho, S.-J.; Oh, M.S.; Jung, S.; Lee, J.-H.; Shin, J.-H.; Koh, I.-S.; Cha, J.-K.; Park, J.-M.; Bae, H.-J.; et al. Cognitive Impairment Evaluated With Vascular Cognitive Impairment Harmonization Standards in a Multicenter Prospective Stroke Cohort in Korea. Stroke 2013, 44, 786–788. [Google Scholar] [CrossRef]
- Gutiérrez Pérez, C.; Sävborg, M.; Påhlman, U.; Cederfeldt, M.; Knopp, E.; Nordlund, A.; Tarkowski, E. High frequency of cognitive dysfunction before stroke among older people. Int. J. Geriatr. Psychiatry 2011, 26, 622–629. [Google Scholar] [CrossRef]
- Rasquin, S.M.C.; Verhey, F.R.J.; Van Oostenbrugge, R.J.; Lousberg, R.; Lodder, J. Demographic and CT scan features related to cognitive impairment in the first year after stroke. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1562–1567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calabrese, P.; Sitek, E.J.; Korczyn, A.D.; Dong, Y.; Manso-Calderón, R.; Sierra-Beltrán, M.; Skrzypkowska, A.; Stefanova, E. The assessment of cognitive and behavioural disturbances in vascular cognitive impairment (VCI)—Recommendations of an expert working group. Neurol. Neurochir. Polska 2021, 55, 333–345. [Google Scholar] [CrossRef] [PubMed]
- Lo, J.W.; Crawford, J.D.; Desmond, D.W.; Godefroy, O.; Jokinen, H.; Mahinrad, S.; Bae, H.-J.; Lim, P.-S.; Köhler, P.; Douven, E.; et al. Profile of and risk factors for poststroke cognitive impairment in diverse ethnoregional groups. Neurology 2019, 93, e2257–e2271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AlTurki, A.; Maj, J.B.; Marafi, M.; Donato, F.; Vescovo, G.; Russo, V.; Proietti, R. The Role of Cardiovascular and Metabolic Comorbidities in the Link between Atrial Fibrillation and Cognitive Impairment: An Appraisal of Current Scientific Evidence. Medicina 2019, 55, 767. [Google Scholar] [CrossRef] [Green Version]
- Gallinoro, E.; D’Elia, S.; Prozzo, D.; Lioncino, M.; Natale, F.; Golino, P.; Cimmino, G. Cognitive Function and Atrial Fibrillation: From the Strength of Relationship to the Dark Side of Prevention. Is There a Contribution from Sinus Rhythm Restoration and Maintenance? Medicina 2019, 55, 587. [Google Scholar] [CrossRef] [Green Version]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Cumming, T.B.; Marshall, R.S.; Lazar, R.M. Stroke, Cognitive Deficits, and Rehabilitation: Still an Incomplete Picture. Int. J. Stroke 2012, 8, 38–45. [Google Scholar] [CrossRef]
- Cuartero, M.I.; García-Culebras, A.; Torres-López, C.; Medina, V.; Fraga, E.; Vázquez-Reyes, S.; Jareño-Flores, T.; García-Segura, J.M.; Lizasoain, I.; Moro, M. Post-stroke Neurogenesis: Friend or Foe? Front. Cell Dev. Biol. 2021, 9, 657846. [Google Scholar] [CrossRef]
- Slotnick, S.D. The hippocampus and long-term memory. Cogn. Neurosci. 2022, 13, 113–114. [Google Scholar] [CrossRef]
- Cascella, M.; Al Khalili, Y. Short Term Memory Impairment. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Thiebaut de Schotten, M.; Foulon, C.; Nachev, P. Brain disconnections link structural connectivity with function and behaviour. Nat. Commun. 2020, 11, 5094. [Google Scholar] [CrossRef]
- Desowska, A.; Turner, D.L. Dynamics of brain connectivity after stroke. Rev. Neurosci. 2019, 30, 605–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blaschke, S.J.; Hensel, L.; Minassian, A.; Vlachakis, S.; Tscherpel, C.; Vay, S.U.; Rabenstein, M.; Schroeter, M.; Fink, G.R.; Hoehn, M.; et al. Translating Functional Connectivity After Stroke: Functional Magnetic Resonance Imaging Detects Comparable Network Changes in Mice and Humans. Stroke 2021, 52, 2948–2960. [Google Scholar] [CrossRef] [PubMed]
- Baldassarre, A.; Ramsey, L.; Siegel, J.S.; Shulman, G.L.; Corbetta, M. Brain connectivity and neurological disorders after stroke. Curr. Opin. Neurol. 2016, 29, 706–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dillen, Y.; Kemps, H.; Gervois, P.; Wolfs, E.; Bronckaers, A. Adult Neurogenesis in the Subventricular Zone and Its Regulation After Ischemic Stroke: Implications for Therapeutic Approaches. Transl. Stroke Res. 2019, 11, 60–79. [Google Scholar] [CrossRef] [PubMed]
- Alia, C.; Spalletti, C.; Lai, S.; Panarese, A.; Lamola, G.; Bertolucci, F.; Vallone, F.; Di Garbo, A.; Chisari, C.; Micera, S.; et al. Neuroplastic Changes Following Brain Ischemia and their Contribution to Stroke Recovery: Novel Approaches in Neurorehabilitation. Front. Cell. Neurosci. 2017, 11, 76. [Google Scholar] [CrossRef] [Green Version]
- Esmael, A.; Elsherief, M.; Eltoukhy, K. Prevalence of cognitive impairment in acute ischaemic stroke and use of Alberta Stroke Programme Early CT Score (ASPECTS) for early prediction of post-stroke cognitive impairment. Neurol. i Neurochir. Polska 2021, 55, 179–185. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | |
|---|---|
| Age | 63.6 years (SD ± 10.9 years) |
| Gender | 35 men |
| Low education level (<13 years) | 41 (82%) |
| Risk Factors | Prevalence: Number of Patients (%) |
| Arterial hypertension | 42 (84) |
| Dyslipidaemia | 30 (60) |
| Nicotinism | 23 (46) |
| Atrial fibrillation | 7 (14) |
| Diabetes mellitus | 6 (12) |
| Hypothyroidism | 5 (10) |
| Stroke | 5 (10) |
| Stroke Severity | Mean (SD) |
| NIHSS at discharge | 2 (SD ± 1.8) |
| mRS at discharge | 1 (SD ± 1.2) |
| Affected Circulation | Number of Patients (%) |
| Anterior circulation | 35 (70) |
| Posterior circulation | 13 (26) |
| Both | 2 (4) |
| Stroke Aethiology | Number of Patients (%) |
| LVD | 14 (28) |
| SVD | 11 (22) |
| CE | 8 (16) |
| Undetermined | 16 (32) |
| Other | 1 (2) |
| Therapy | Number of Patients (%) |
| IVT | 3 (6) |
| TE | 4(8) |
| IVT + TE | 5 (10) |
| APT | 39 (78) |
| Cognitive Domain | Prevalence of CogI at Discharge [n (%); Mean MoCA Score (SD)] | Prevalence of CogI after Six Months [n (%); Mean MoCA Score (SD)] | t-Test p-Value |
|---|---|---|---|
| Executive functions | 21 (43%); 0.43 (0.5) | 19 (38%); 0.37 (0.5) | 0.371 |
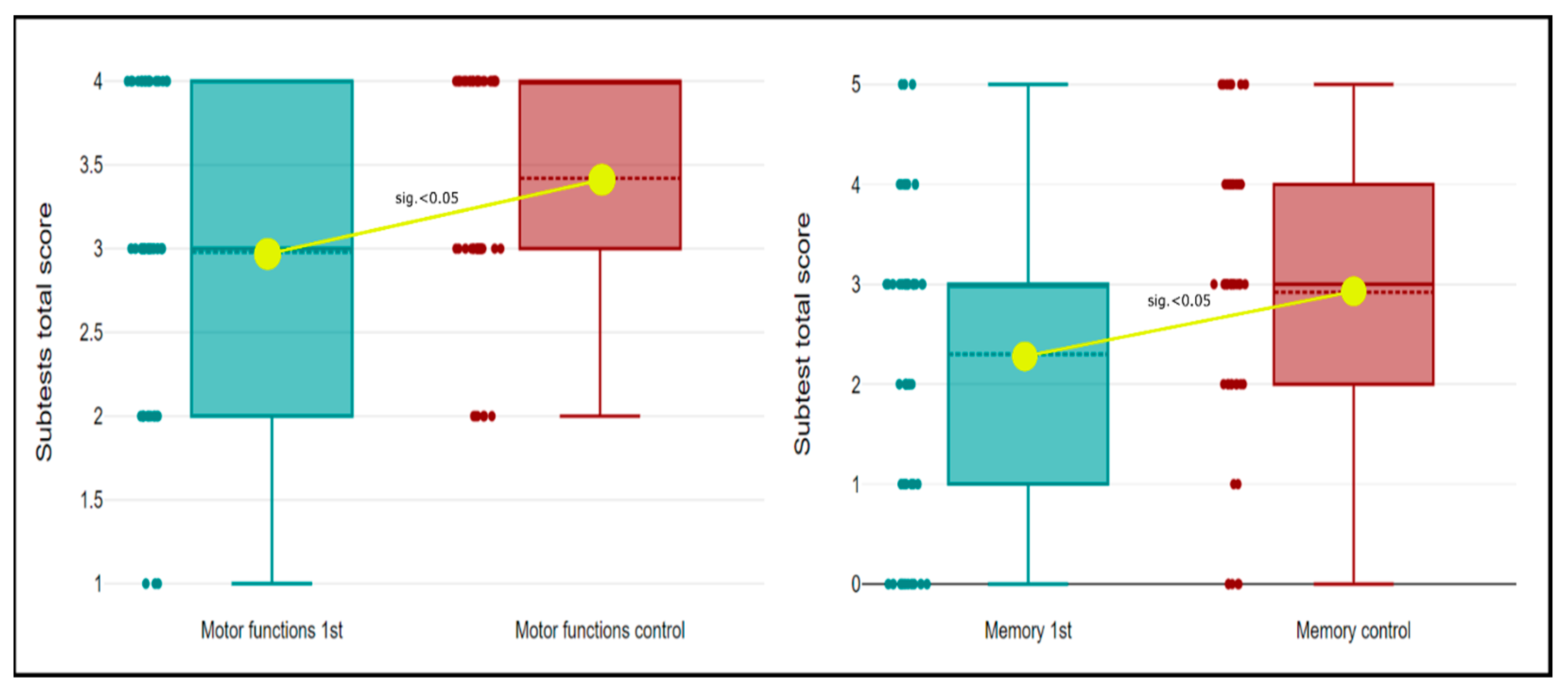
| Motor and constructional functions | 34 (68%); 3.0 (0.9) | 24 (48%); 3.4 (0.7) | 0.000 * |
| Language & speech | 35 (70%); 4.6 (1.3) | 37 (74%); 4.7 (1.1) | 0.542 |
| Attention | 24 (48%); 5.04 (1.2) | 23 (46%); 5.31 (0.9) | 0.065 |
| Abstract thinking | 19 (38%); 1.56 (0.6) | 16 (32%); 1.6 (0.6) | 0.687 |
| Memory | 39 (78%); 2.3 (1.54) | 33 (66%); 2.9 (1.43) | 0.004 * |
| Presence of CogI at Discharge vs. Risk Factors | |||
|---|---|---|---|
| Factors | OR, 95% CI | Pearsons r | p-Value |
| Education (<13 years) | 9.7 (2.0–48.5) | 0.434 | 0.002 * |
| Age | 0.317 | 0.025 * | |
| AH | 15 (2.5–90.2) | 0.488 | 0.001 * |
| AF | 0.9 (0.2–5.1) | −0.024 | 0.867 |
| DLP | 1.4 (0.4–5.1) | 0.074 | 0.599 |
| DM | 1.1 (1.0–1.4) | 0.219 | 0.122 |
| stroke | 1.2 (1.0–1.3) | 0.198 | 0.162 |
| smoking | 1 (0.23–3.53) | −0.002 | 0.990 |
| hypothyroidism | 0.5 (0.1–3.3) | −0.106 | 0.452 |
| Presence of CogI at Discharge vs. Aetiology of Stroke | |||
| Aetiology | OR, 95% CI | Pearsons r | p-Value |
| LAA | 1.4 (0.3–6.1) | 0.065 | 0.646 |
| lacunar | 0.9 (0.2–4.2) | −0.015 | 0.913 |
| CE | 0.5 (0.1–2.6) | −0.114 | 0.418 |
| UE | 1.1 (0.2–4.8) | 0.013 | 0.928 |
| Presence of CogI at Discharge vs. Treatment | |||
| Treatment | OR, 95% CI | Pearsons r | p-Value |
| IVT/TE | 0.6 (0.2–2.6) | −0.020 | 0.893 |
| Progression of CogI (Decline in MoCA Score after 6 Months) vs. Risk Factors | |||
| Risk Factors | OR, 95% CI | Pearsons r | p-Value |
| education | 2.9 (0.6–15.0) | 0.187 | 0.186 |
| AH | 0.6 (0.1–3.6) | −0.08 | 0.574 |
| AF | 0.7 (0.1–6.9) | −0.039 | 0.783 |
| DLP | 0.5 (0.1–2.0) | −0.149 | 0.293 |
| DM | 0.8 (0.7–0.9) | −0.173 | 0.221 |
| smoking | 3.0 (0.6–12.9) | 0.194 | 0.170 |
| stroke | 0.8 (0.7–0.9) | −0.156 | 0.269 |
| CT/MRI Findings of Acute Ischaemic Lesions | |||
|---|---|---|---|
| Anatomical Region | Number of Patients | % | |
| Frontal lobe | 12 | 24 | |
| Temporal lobe | 14 | 28 | |
| Parietal lobe | 13 | 26 | |
| Occipital lobe | 9 | 18 | |
| Insula | 8 | 16 | |
| Basal ganglia | 11 | 22 | |
| Internal capsule | 5 | 10 | |
| External capsule | 6 | 12 | |
| Thalamus | 4 | 8 | |
| Brainstem | 6 | 12 | |
| Cerebellum | 7 | 14 | |
| Number of Affected Regions | Number of Patients | % | |
| 1 | 18 | 36 | |
| 2 | 15 | 30 | |
| 3 | 5 | 10 | |
| 4 | 4 | 8 | |
| 5 | 2 | 4 | |
| 6 | 1 | 2 | |
| Relationship between Presence of CogI at Discharge and Localisation of Ischaemic Lesion | |||
| Symptomatic Circulation & Hemisphere | OR | Pearson r | p-Value |
| Anterior | 1 | 0.01 | 0.944 |
| Posterior | 1 | 0.040 | 0.775 |
| Right | 2 | −0.319 | 0.154 |
| Left | 4 | 0.276 | 0.072 |
| Both | 0.6 | 0.624 | 1289 |
| Affected Regions | OR | Pearson r | p-Value |
| Frontal lobe | 1.2 | 0.094 | 0.506 |
| Parietal lobe | 1.3 | 0.168 | 0.234 |
| Temporal lobe | 1.2 | 0.138 | 0.329 |
| Occipital lobe | 1.1 | 0.078 | 0.580 |
| Insula | 1.6 | 0.239 | 0.091 |
| Basal ganglia | 1.5 | 0.236 | 0.096 |
| Internal capsule | 1 | 0.046 | 0.747 |
| External capsule | 2.4 | 0.342 | 0.165 |
| Thalamus | 1 | 0.007 | 0.962 |
| Cerebellum | 1 | 0.024 | 0.867 |
| Brainstem | 0.91 | 0.079 | 0.578 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koren, D.; Slavkovska, M.; Vitkova, M.; Gdovinova, Z. Importance of Retesting for the Final Diagnosis of Post-Stroke Cognitive Impairment. Medicina 2023, 59, 637. https://doi.org/10.3390/medicina59030637
Koren D, Slavkovska M, Vitkova M, Gdovinova Z. Importance of Retesting for the Final Diagnosis of Post-Stroke Cognitive Impairment. Medicina. 2023; 59(3):637. https://doi.org/10.3390/medicina59030637
Chicago/Turabian StyleKoren, Dominik, Miriam Slavkovska, Marianna Vitkova, and Zuzana Gdovinova. 2023. "Importance of Retesting for the Final Diagnosis of Post-Stroke Cognitive Impairment" Medicina 59, no. 3: 637. https://doi.org/10.3390/medicina59030637
APA StyleKoren, D., Slavkovska, M., Vitkova, M., & Gdovinova, Z. (2023). Importance of Retesting for the Final Diagnosis of Post-Stroke Cognitive Impairment. Medicina, 59(3), 637. https://doi.org/10.3390/medicina59030637