
Foreign Body Aspiration in Children—Retrospective Study and Management Novelties


 , , and
, , and
Abstract
:1. Introduction
2. Material and Methods
3. Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ulas, A.B.; Aydin, Y.; Eroglu, A. Foreign body aspirations in children and adults. Am. J. Surg. 2022, 224, 1168–1173. [Google Scholar] [CrossRef] [PubMed]
- Brkic, F.; Umihanic, S.; Altumbabic, H.; Ramas, A.; Salkic, A.; Umihanic, S.; Mujic, M.; Softic, L.; Zulcic, S. Death as a Consequence of Foreign Body Aspiration in Children. Med. Arch. 2018, 72, 220–223. [Google Scholar] [CrossRef] [PubMed]
- Abd-ElGawad, E.A.; Ibrahim, M.A.; Mubarak, Y.S. Tracheobronchial foreign body aspiration in infants & children: Diagnostic utility of multidetector CT with emphasis on virtual bronchoscopy. Egypt. J. Radiol. Nucl. Med. 2014, 45, 1141–1146. [Google Scholar] [CrossRef] [Green Version]
- Engin, M.M.N.; Erdogan, F.; Kucuk, Ö.; Kaya, M. Foreign body aspiration in an 11-month-old child; the importance of anamnesis and respiratory examination. J. Pediatr. Neonatal Care 2020, 10, 156–157. [Google Scholar] [CrossRef]
- Safari, M.; Hashemi Manesh, M.R. Demographic and clinical findings in children undergoing bronchoscopy for foreign body aspiration. Ochsner J. 2016, 16, 120–124. [Google Scholar]
- Sahadan, D.Z.; Zainudin, N.M.; Kassim, A.; Zahari, Z.; Mahadzir, M.; Che Daud, C.Z.; Mohammad, N. Case serires of foreign body aspiration in Paediatric Institute, Hospital Kuala Lumpur. Med. J. Malays. 2011, 66, 484–486. [Google Scholar]
- Holliday, S.; Gurkowski, M.A. Chapter 188—Foreign body aspiration. In Complications in Anesthesia, 2nd ed.; Elsevier Health Sciences: Philadelphia, PA, USA, 2007; pp. 753–755. [Google Scholar]
- Baram, A.; Sherzad, H.; Saeed, S.; Kakamad, F.H.; Hamawandi, A.M.H. Tracheobronchial Foreign Bodies in Children: The Role of Emergency Rigid Bronchoscopy. Glob. Pediatr. Health 2017, 4, 2333794x17743663. [Google Scholar] [CrossRef]
- Dorofaeff, T.; Plumpton, K. 105—Acute respiratory failure in children. In Oh’s Intensive Care Manual, 2nd ed.; Andrew, D., Bersten, N.S., Eds.; Butterworth-Heinemann: Woburn, MA, USA, 2014; pp. 1085–1095. [Google Scholar]
- Morris, I.R. Anesthesia and Airway Management of Laryngoscopy and Bronchoscopy. In Benumof’s Airway Management; Mosby: London, UK, 2007; pp. 859–888. [Google Scholar] [CrossRef]
- Gatto, A.; Capossela, L.; Ferretti, S.; Orlandi, M.; Pansini, V.; Curatola, A.; Chiaretti, A. Foreign Body Ingestion in Children: Epidemiological, Clinical Features and Outcome in a Third Level Emergency Department. Children 2021, 8, 1182. [Google Scholar] [CrossRef]
- Ikenberry, S.O.; Jue, T.L.; Anderson, M.A.; Appalaneni, V.; Banerjee, S.; Ben-Menachem, T.; Decker, G.A.; Fanelli, R.D.; Fisher, L.R.; Fukami, N.; et al. Management of ingested foreign bodies and food impactions. Gastrointest. Endosc. 2011, 73, 1085–1091. [Google Scholar] [CrossRef]
- Eren, Ş.; Balci, A.E.; Dikici, B.; Doblan, M.; Eren, M.N. Foreign body aspiration in children: Experience of 1160 cases. Ann. Trop. Paediatr. 2003, 23, 31–37. [Google Scholar] [CrossRef]
- Berry, F.; Stemland, C. Foreign body aspiration. In Essence of Anesthesia Practice, 3rd ed.; Elsevier Health Sciences: Philadelphia, PA, USA, 2011; p. 156. [Google Scholar]
- Mohammad, M.; Saleem, M.; Mahseeri, M.; Alabdallat, I.; Alomari, A.; Za’atreh, A.; Qudaisat, I.; Shudifat, A.; Nasri Alzoubi, M. Foreign body aspiration in children: A study of children who lived or died following aspiration. Int. J. Pediatr. Otorhinolaryngol. 2017, 98, 29–31. [Google Scholar] [CrossRef]
- Xu, Y.; Feng, R.L.; Jiang, L.; Ren, H.B.; Li, Q. Correlative factors for the location of tracheobronchial foreign bodies in infants and children. J. Thorac. Dis. 2018, 10, 1037–1042. [Google Scholar] [CrossRef] [Green Version]
- Nasir, Z.M.; Subha, S.T. A Five-Year Review on Pediatric Foreign Body Aspiration. Int. Arch. Otorhinolaryngol. 2021, 25, e193. [Google Scholar] [CrossRef]
- Fidkowski, C.W.; Zheng, H.; Firth, P.G. The anesthetic considerations of tracheobronchial foreign bodies in children: A literature review of 12,979 cases. Anesth. Analg. 2010, 111, 1016–1025. [Google Scholar] [CrossRef]
- Ding, G.; Wu, B.; Vinturache, A.; Cai, C.; Lu, M.; Gu, H. Tracheobronchial foreign body aspiration in children: A retrospective single-center cross-sectional study. Medicine 2020, 99, e20480. [Google Scholar] [CrossRef]
- Field, N.; Cohen, T.; Struelens, M.J.; Palm, D.; Cookson, B.; Glynn, J.R.; Gallo, V.; Ramsay, M.; Sonnenberg, P.; MacCannell, D.; et al. Strengthening the Reporting of Molecular Epidemiology for Infectious Diseases (STROME-ID): An extension of the STROBE statement. Lancet Infect. Dis. 2014, 14, 341–352. [Google Scholar] [CrossRef]
- Dehghani, N.; Ludemann, P. Aspirated foreign bodies in children: BC Children’s Hospital emergency room protocol. BCMJ BC Med. J. 2008, 50, 252–256. [Google Scholar]
- Tang, L.F.; Xu, Y.C.; Wang, Y.S.; Wang, C.F.; Zhu, G.H.; Bao, X.E.; Lu, M.P.; Chen, L.X.; Chen, Z.M. Airway foreign body removal by flexible bronchoscopy: Experience with 1027 children during 2000–2008. World J. Pediatr. 2009, 5, 191–195. [Google Scholar] [CrossRef]
- Gvetadze, P.; Chkhaidze, I.; Baldas, S.; Comoretto, R.; Gregori, D.; Berchialla, P.; Rodriguez, H.; Zaupa, P.; Spitzer, P.; Demetriades, C.; et al. Injuries due to foreign body aspirations in Georgia: A prevention perspective. Int. J. Pediatr. Otorhinolaryngol. 2016, 83, 84–87. [Google Scholar] [CrossRef]
- Tomaske, M.; Gerber, A.C.; Stocker, S.; Weiss, M. Tracheobronchial foreign body aspiration in children-diagnostic value of symptoms and signs. Swiss Med. Wkly. 2006, 136, 533–538. [Google Scholar]
- Kalyanappagol, V.T.; Kulkarni, N.H.; Bidri, L.H. Management of tracheobronchial foreign body aspirations in paediatric age group-a 10 year retrospective analysis. Indian J. Anaesth. 2007, 51, 20–23. [Google Scholar]
- Nyeki, A.R.N.; Miloundja, J.; Dalil, A.B.; Lawson, J.M.M.; Nzenze, S.; Sougou, E.; Nziengui, A.; N’zouba, L. Les corps étrangers laryngo-trachéo-bronchiques: Expérience de l’hôpital d’instruction des armées Omar Bongo Ondimba (HIAOBO) de Libreville. Pan Afr. Med. J. 2015, 20, 298. [Google Scholar] [CrossRef] [PubMed]
- Haller, L.; Barazzone-Argiroffo, C.; Vidal, I.; Corbelli, R.; Anooshiravani-Dumont, M.; Mornand, A. Safely decreasing rigid bronschoscopies for foreign-body aspiration in children: An algorithm for the emergency department. Eur. J. Pediatr. Surg. 2018, 28, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Fasseeh, N.A.; Elagamy, O.A.; Gaafar, A.H.; Reyad, H.M.; Abougabal, M.S.; Heiba, D.A.; Kantar, A. A new scoring system and clinical algorithm for the management of suspected foreign body aspiration in children: A retrospective cohort study. Ital. J. Pediatr. 2021, 47, 194. [Google Scholar] [CrossRef]
- Rance, A.; Mittaine, M.; Michelet, M.; Martin Blondel, A.; Labouret, G. Delayed diagnosis of foreign body aspiration in children. Arch. Pediatr. 2022, 29, 424–428. [Google Scholar] [CrossRef]
- Divarci, E.; Toker, B.; Dokumcu, Z.; Musayev, A.; Ozcan, C.; Erdener, A. The multivariate analysis of indications of rigid bronchoscopy in suspected foreign body aspiration. Int. J. Pediatr. Otorhinolaryngol. 2017, 100, 232–237. [Google Scholar] [CrossRef]
- Buonsenso, D.; Chiaretti, A.; Curatola, A.; Morello, R.; Giacalone, M.; Parri, N. Pediatrician performed point-of-care ultrasound for the detection of ingested foreign bodies: Case series and review of the literature. J. Ultrasound 2021, 24, 107–114. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | Frequency | Percentage |
|---|---|---|
| Total number of patients | 232 | |
| Sex | ||
| Male:Female ratio | 1.77 | |
| Age | ||
| <1 year old | 17 | 7.32% |
| 1–3 years old | 182 | 78.45% |
| 4–16 years old | 33 | 14.22% |
| Place of origin | ||
| Rural area | 162 | 69.82% |
| Urban area | 70 | 30.17% |
| No. of cases based of the nature of the foreign body | ||
| Organic + inorganic bodies | 10 | 4.31% |
| Organic (vegetable) bodies (alone and combined) | 202 | |
| Seeds | 111 | 55% |
| Hazelnut | 47 | 23% |
| Walnut kernel | 26 | 13% |
| Corn kernel | 10 | 5% |
| Beans | 8 | 4% |
| Inorganic bodies | 20 | |
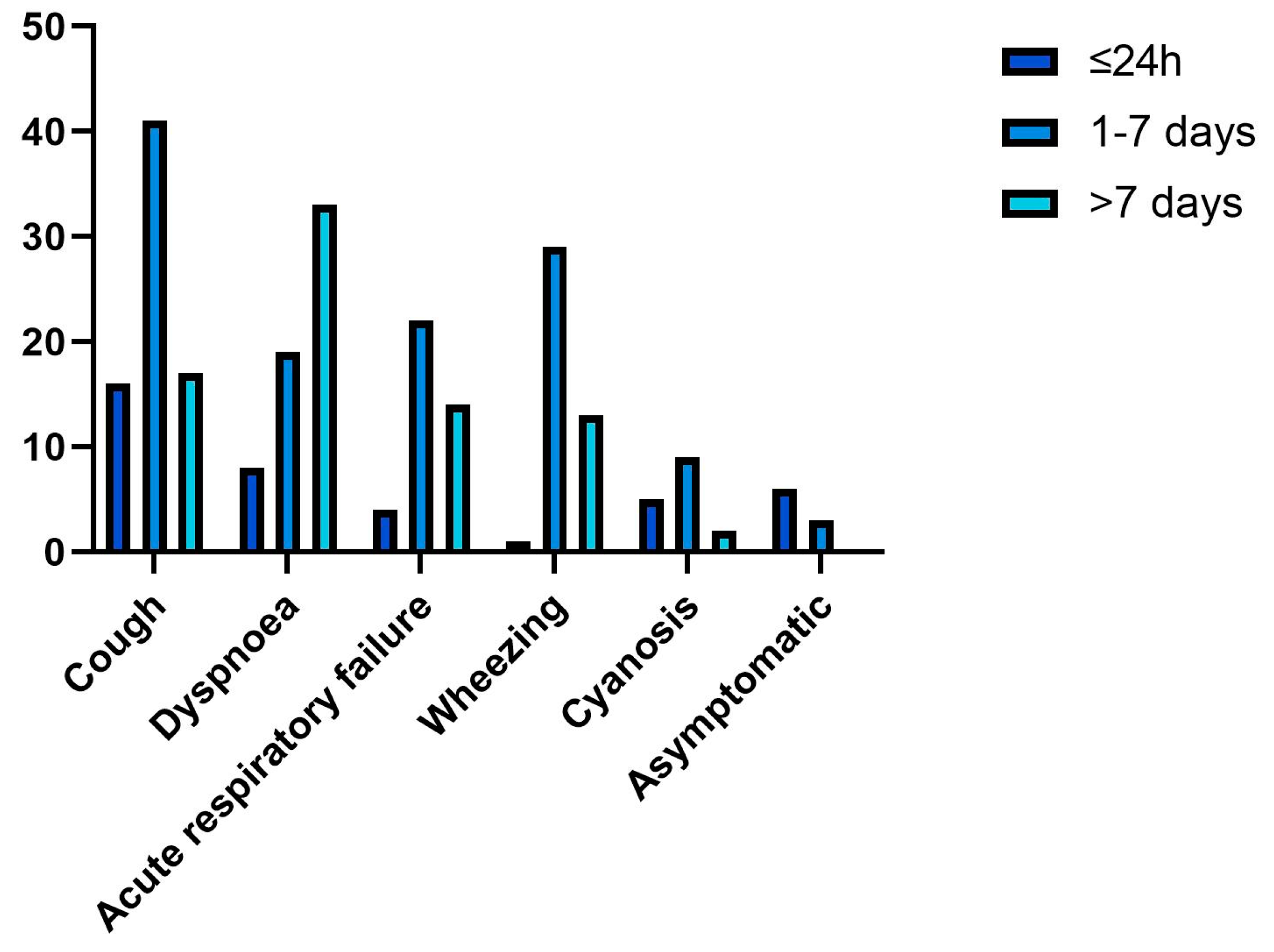
| Time of admission | ||
| Within the first 24 h | 49 | 21% |
| After the first 24 h | 143 | 61.63% |
| After 7 days | 40 | 16.94% |
| Main clinical manifestation | ||
| Sudden onset of cough | 77 | 33.05% |
| Dyspnea | 49 | 21.09% |
| Acute respiratory failure | 44 | 19% |
| Wheezing | 35 | 14.87% |
| Cyanosis | 21 | 9.09% |
| Initial clinical examination | ||
| Decreased lung sounds | 78 | 33.62% |
| Bronchial obstruction and coarse vesicular murmur | 55 | 23.7% |
| Bronchial rales | 116 | 50% |
| Aspiration pneumonia and pulmonary obstruction | 32 | 13.79% |
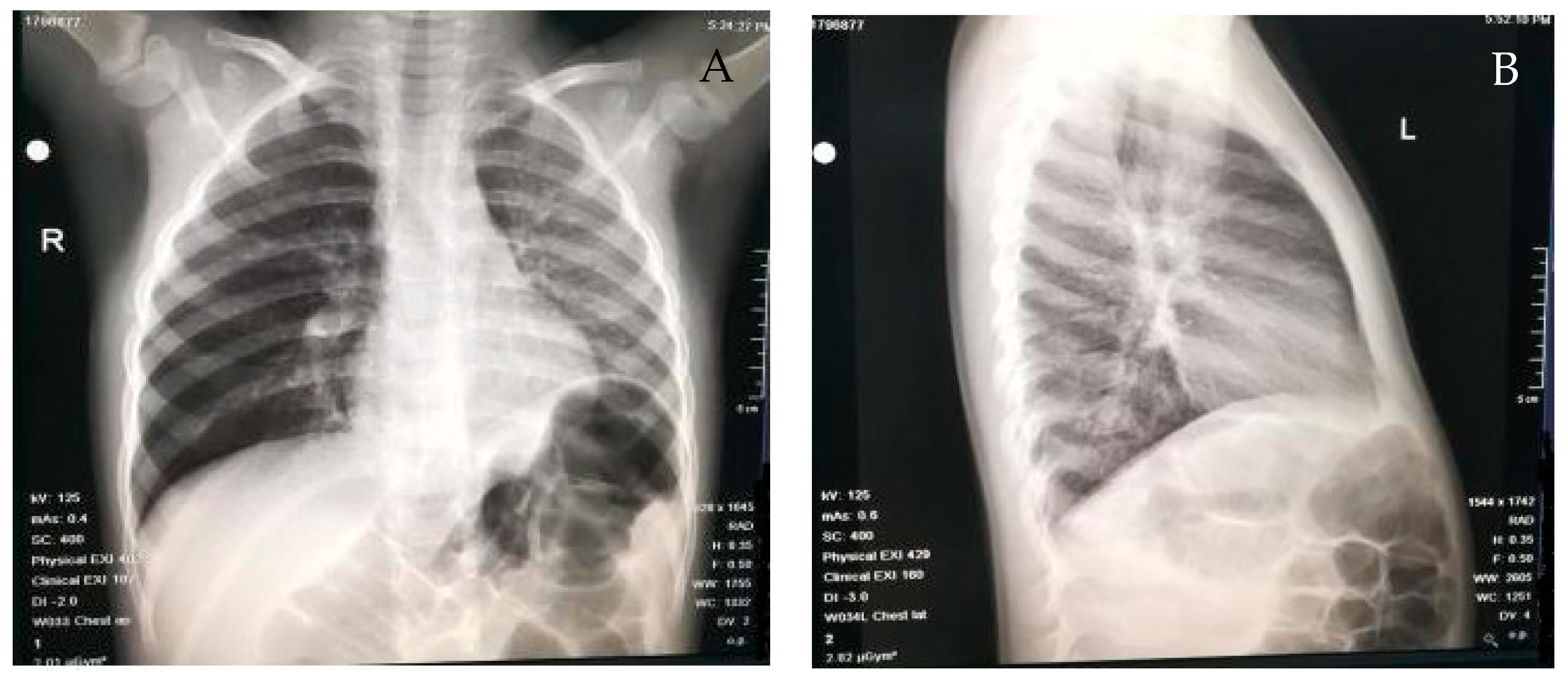
| Chest radiography results | ||
| Pulmonary atelectasis | 62 | 26.85% |
| Pulmonary emphysema | 41 | 17.76% |
| Direct visualization of the foreign body | 8 | 3.44% |
| Location of the foreign body | ||
| Right bronchial tree | 124 | 51.23% |
| Left primitive bronchus | 81 | 33.45% |
| Trachea | 17 | 7.02% |
| Tracheal bifurcation | 13 | 5.37% |
| Upper airways (nostrils and glottis) | 7 | 3% |
| Complications | ||
| Aspiration pneumonia | 123 | 53.01% |
| Acute tracheobronchitis | 13 | 5.6% |
| Laryngitis | 3 | 1.29% |
| Lung abscess | 2 | 0.86% |
| Assisted ventilation | 5 | 2.15% |
| Temporary tracheostomy | 1 | 0.43% |
| Antibiotic therapy | 204 | 88% |
| Period of hospitalization | ||
| <5 days | 107 | 46% |
| >5 days | 125 | 54% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mîndru, D.E.; Păduraru, G.; Rusu, C.D.; Țarcă, E.; Azoicăi, A.N.; Roșu, S.T.; Curpăn, A.-Ș.; Ciomaga Jitaru, I.M.; Pădureț, I.A.; Luca, A.C. Foreign Body Aspiration in Children—Retrospective Study and Management Novelties. Medicina 2023, 59, 1113. https://doi.org/10.3390/medicina59061113
Mîndru DE, Păduraru G, Rusu CD, Țarcă E, Azoicăi AN, Roșu ST, Curpăn A-Ș, Ciomaga Jitaru IM, Pădureț IA, Luca AC. Foreign Body Aspiration in Children—Retrospective Study and Management Novelties. Medicina. 2023; 59(6):1113. https://doi.org/10.3390/medicina59061113
Chicago/Turabian StyleMîndru, Dana Elena, Gabriela Păduraru, Carmen Daniela Rusu, Elena Țarcă, Alice Nicoleta Azoicăi, Solange Tamara Roșu, Alexandrina-Ștefania Curpăn, Irina Mihaela Ciomaga Jitaru, Ioana Alexandra Pădureț, and Alina Costina Luca. 2023. "Foreign Body Aspiration in Children—Retrospective Study and Management Novelties" Medicina 59, no. 6: 1113. https://doi.org/10.3390/medicina59061113
APA StyleMîndru, D. E., Păduraru, G., Rusu, C. D., Țarcă, E., Azoicăi, A. N., Roșu, S. T., Curpăn, A.-Ș., Ciomaga Jitaru, I. M., Pădureț, I. A., & Luca, A. C. (2023). Foreign Body Aspiration in Children—Retrospective Study and Management Novelties. Medicina, 59(6), 1113. https://doi.org/10.3390/medicina59061113