
A Review of Treatment Methods Focusing on Human Induced Pluripotent Stem Cell-Derived Neural Stem/Progenitor Cell Transplantation for Chronic Spinal Cord Injury


 , ,
, ,  and
and
Abstract
:1. Introduction
2. Time-Dependent Changes in the Microenvironment of the Injured Spinal Cord
3. Neural Stem/Progenitor Cell Transplantation for Spinal Cord Injury
3.1. Optimal Time for Transplantation
3.2. Transplantation in the Subacute Phase
3.3. Transplantation in the Chronic Phase
4. Rehabilitation Therapy for Spinal cord Injury in Preclinical Studies
5. Drug Intervention for Scars in Chronic Spinal Cord Injury
6. Combined Therapy for Chronic Spinal Cord Injury
6.1. Combination of Cell Transplantation and Rehabilitation
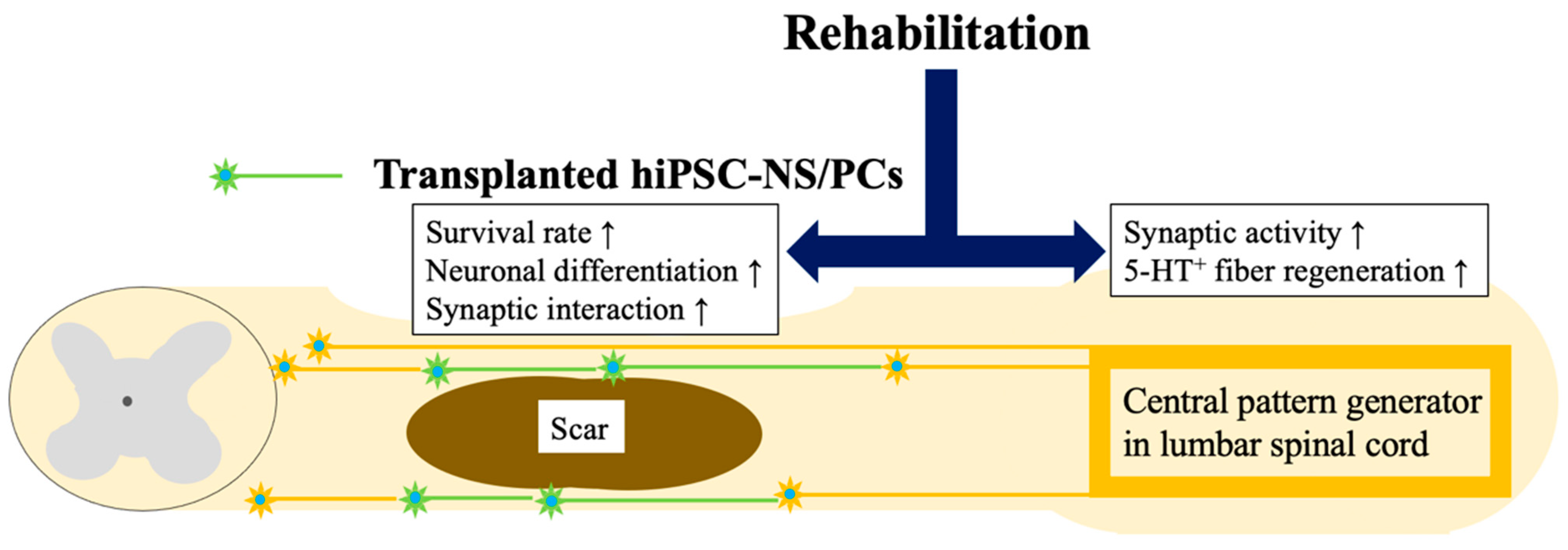
6.2. Combination of hiPSC-NS/PC Transplantation and Rehabilitation
7. Combination of Regenerative Therapy and Drugs or Biomaterials
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Shinozaki, M.; Nagoshi, N.; Nakamura, M.; Okano, H. Mechanisms of Stem Cell Therapy in Spinal Cord Injuries. Cells 2021, 10, 2676. [Google Scholar] [CrossRef] [PubMed]
- Okano, H.; Kaneko, S.; Okada, S.; Iwanami, A.; Nakamura, M.; Toyama, Y. Regeneration-based therapies for spinal cord injuries. Neurochem. Int. 2007, 51, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Yamanaka, S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell 2006, 126, 663–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsuji, O.; Miura, K.; Okada, Y.; Fujiyoshi, K.; Mukaino, M.; Nagoshi, N.; Kitamura, K.; Kumagai, G.; Nishino, M.; Tomisato, S.; et al. Therapeutic potential of appropriately evaluated safe-induced pluripotent stem cells for spinal cord injury. Proc. Natl. Acad Sci. USA 2010, 107, 12704–12709. [Google Scholar] [CrossRef]
- Nori, S.; Okada, Y.; Yasuda, A.; Tsuji, O.; Takahashi, Y.; Kobayashi, Y.; Fujiyoshi, K.; Koike, M.; Uchiyama, Y.; Ikeda, E.; et al. Grafted human-induced pluripotent stem-cell-derived neurospheres promote motor functional recovery after spinal cord injury in mice. Proc. Natl. Acad Sci. USA 2011, 108, 16825–16830. [Google Scholar] [CrossRef]
- Nishimura, S.; Yasuda, A.; Iwai, H.; Takano, M.; Kobayashi, Y.; Nori, S.; Tsuji, O.; Fujiyoshi, K.; Ebise, H.; Toyama, Y.; et al. Time-dependent changes in the microenvironment of injured spinal cord affects the therapeutic potential of neural stem cell transplantation for spinal cord injury. Mol. Brain 2013, 6, 3. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, H.; Sakai, T. Current Concepts of Stem Cell Therapy for Chronic Spinal Cord Injury. Int. J. Mol. Sci. 2021, 22, 7435. [Google Scholar] [CrossRef]
- Tsuji, O.; Sugai, K.; Yamaguchi, R.; Tashiro, S.; Nagoshi, N.; Kohyama, J.; Iida, T.; Ohkubo, T.; Itakura, G.; Isoda, M.; et al. Concise Review: Laying the Groundwork for a First-In-Human Study of an Induced Pluripotent Stem Cell-Based Intervention for Spinal Cord Injury. Stem. Cells 2019, 37, 6–13. [Google Scholar] [CrossRef] [Green Version]
- Karimi-Abdolrezaee, S.; Eftekharpour, E.; Wang, J.; Morshead, C.M.; Fehlings, M.G. Delayed transplantation of adult neural precursor cells promotes remyelination and functional neurological recovery after spinal cord injury. J. Neurosci. 2006, 26, 3377–3389. [Google Scholar] [CrossRef] [Green Version]
- Ahuja, C.S.; Fehlings, M. Concise Review: Bridging the Gap: Novel Neuroregenerative and Neuroprotective Strategies in Spinal Cord Injury. Stem. Cells Transl. Med. 2016, 5, 914–924. [Google Scholar] [CrossRef] [Green Version]
- Okano, H. Stem cell biology of the central nervous system. J. Neurosci. Res. 2002, 69, 698–707. [Google Scholar] [CrossRef]
- Ogawa, Y.; Sawamoto, K.; Miyata, T.; Miyao, S.; Watanabe, M.; Nakamura, M.; Bregman, B.S.; Koike, M.; Uchiyama, Y.; Toyama, Y.; et al. Transplantation of in vitro-expanded fetal neural progenitor cells results in neurogenesis and functional recovery after spinal cord contusion injury in adult rats. J. Neurosci. Res. 2002, 69, 925–933. [Google Scholar] [CrossRef]
- Shibata, R.; Nagoshi, N.; Kajikawa, K.; Ito, S.; Shibata, S.; Shindo, T.; Khazaei, M.; Nori, S.; Kohyama, J.; Fehlings, M.G.; et al. Administration of C5a Receptor Antagonist Improves the Efficacy of Human Induced Pluripotent Stem Cell-Derived Neural Stem/Progenitor Cell Transplantation in the Acute Phase of Spinal Cord Injury. J. Neurotrauma 2022, 39, 667–682. [Google Scholar] [CrossRef] [PubMed]
- Kwon, B.K.; Soril, L.J.; Bacon, M.; Beattie, M.S.; Blesch, A.; Bresnahan, J.C.; Bunge, M.B.; Dunlop, S.A.; Fehlings, M.G.; Ferguson, A.R.; et al. Demonstrating efficacy in preclinical studies of cellular therapies for spinal cord injury—How much is enough? Exp. Neurol. 2013, 248, 30–44. [Google Scholar] [CrossRef]
- Nori, S.; Nakamura, M.; Okano, H. Plasticity and regeneration in the injured spinal cord after cell transplantation therapy. Prog. Brain Res. 2017, 231, 33–56. [Google Scholar] [CrossRef] [PubMed]
- Kawai, M.; Imaizumi, K.; Ishikawa, M.; Shibata, S.; Shinozaki, M.; Shibata, T.; Hashimoto, S.; Kitagawa, T.; Ago, K.; Kajikawa, K.; et al. Long-term selective stimulation of transplanted neural stem/progenitor cells for spinal cord injury improves locomotor function. Cell Rep. 2021, 37, 110019. [Google Scholar] [CrossRef] [PubMed]
- Sugai, K.; Sumida, M.; Shofuda, T.; Yamaguchi, R.; Tamura, T.; Kohzuki, T.; Abe, T.; Shibata, R.; Kamata, Y.; Ito, S.; et al. First-in-human clinical trial of transplantation of iPSC-derived NS/PCs in subacute complete spinal cord injury: Study protocol. Regen. Ther. 2021, 18, 321–333. [Google Scholar] [CrossRef]
- Kusano, K.; Enomoto, M.; Hirai, T.; Tsoulfas, P.; Sotome, S.; Shinomiya, K.; Okawa, A. Transplanted neural progenitor cells expressing mutant NT3 promote myelination and partial hindlimb recovery in the chronic phase after spinal cord injury. Biochem. Biophys. Res. Commun. 2010, 393, 812–817. [Google Scholar] [CrossRef]
- Okubo, T.; Nagoshi, N.; Kohyama, J.; Tsuji, O.; Shinozaki, M.; Shibata, S.; Kase, Y.; Matsumoto, M.; Nakamura, M.; Okano, H. Treatment with a Gamma-Secretase Inhibitor Promotes Functional Recovery in Human iPSC—Derived Transplants for Chronic Spinal Cord Injury. Stem Cell Rep. 2018, 11, 1416–1432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tashiro, S.; Nakamura, M.; Okano, H. The prospects of regenerative medicine combined with rehabilitative approaches for chronic spinal cord injury animal models. Neural Regen. Res. 2017, 12, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Battistuzzo, C.R.; Callister, R.J.; Callister, R.; Galea, M.P. A systematic review of exercise training to promote locomotor recovery in animal models of spinal cord injury. J. Neurotrauma 2012, 29, 1600–1613. [Google Scholar] [CrossRef] [Green Version]
- Fouad, K.; Tetzlaff, W. Rehabilitative training and plasticity following spinal cord injury. Exp. Neurol. 2012, 235, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Loy, K.; Bareyre, F.M. Rehabilitation following spinal cord injury: How animal models can help our understanding of exercise-induced neuroplasticity. Neural Regen. Res. 2019, 14, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Goldshmit, Y.; Lythgo, N.; Galea, M.P.; Turnley, A.M. Treadmill training after spinal cord hemisection in mice promotes axonal sprouting and synapse formation and improves motor recovery. J. Neurotrauma 2008, 25, 449–465. [Google Scholar] [CrossRef]
- Hayashibe, M.; Homma, T.; Fujimoto, K.; Oi, T.; Yagi, N.; Kashihara, M.; Nishikawa, N.; Ishizumi, Y.; Abe, S.; Hashimoto, H.; et al. Locomotor improvement of spinal cord-injured rats through treadmill training by forced plantar placement of hind paws. Spinal Cord 2016, 54, 521–529. [Google Scholar] [CrossRef] [Green Version]
- Heng, C.; de Leon, R.D. Treadmill training enhances the recovery of normal stepping patterns in spinal cord contused rats. Exp. Neurol. 2009, 216, 139–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magnuson, D.S.; Smith, R.R.; Brown, E.H.; Enzmann, G.; Angeli, C.; Quesada, P.M.; Burke, D. Swimming as a model of task-specific locomotor retraining after spinal cord injury in the rat. Neurorehabil. Neural Repair 2009, 23, 535–545. [Google Scholar] [CrossRef] [PubMed]
- Ryu, Y.; Ogata, T.; Nagao, M.; Kitamura, T.; Morioka, K.; Ichihara, Y.; Doi, T.; Sawada, Y.; Akai, M.; Nishimura, R.; et al. The swimming test is effective for evaluating spasticity after contusive spinal cord injury. PLoS ONE 2017, 12, e0171937. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Ventura, J.; Gimenez-Llort, L.; Penas, C.; Udina, E. Voluntary wheel running preserves lumbar perineuronal nets, enhances motor functions and prevents hyperreflexia after spinal cord injury. Exp. Neurol. 2021, 336, 113533. [Google Scholar] [CrossRef]
- Shah, P.K.; Garcia-Alias, G.; Choe, J.; Gad, P.; Gerasimenko, Y.; Tillakaratne, N.; Zhong, H.; Roy, R.R.; Edgerton, V.R. Use of quadrupedal step training to re-engage spinal interneuronal networks and improve locomotor function after spinal cord injury. Brain 2013, 136, 3362–3377. [Google Scholar] [CrossRef] [Green Version]
- Sliwinski, C.; Nees, T.A.; Puttagunta, R.; Weidner, N.; Blesch, A. Sensorimotor Activity Partially Ameliorates Pain and Reduces Nociceptive Fiber Density in the Chronically Injured Spinal Cord. J. Neurotrauma 2018, 35, 2222–2238. [Google Scholar] [CrossRef] [PubMed]
- Tashiro, S.; Nishimura, S.; Shinozaki, M.; Takano, M.; Konomi, T.; Tsuji, O.; Nagoshi, N.; Toyama, Y.; Liu, M.; Okano, H.; et al. The Amelioration of Pain-Related Behavior in Mice with Chronic Spinal Cord Injury Treated with Neural Stem/Progenitor Cell Transplantation Combined with Treadmill Training. J. Neurotrauma 2018, 35, 2561–2571. [Google Scholar] [CrossRef] [PubMed]
- Hwang, D.H.; Shin, H.Y.; Kwon, M.J.; Choi, J.Y.; Ryu, B.Y.; Kim, B.G. Survival of neural stem cell grafts in the lesioned spinal cord is enhanced by a combination of treadmill locomotor training via insulin-like growth factor-1 signaling. J. Neurosci. 2014, 34, 12788–12800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tashiro, S.; Shinozaki, M.; Mukaino, M.; Renault-Mihara, F.; Toyama, Y.; Liu, M.; Nakamura, M.; Okano, H. BDNF Induced by Treadmill Training Contributes to the Suppression of Spasticity and Allodynia After Spinal Cord Injury via Upregulation of KCC2. Neurorehabil. Neural Repair 2015, 29, 677–689. [Google Scholar] [CrossRef]
- Gomez-Pinilla, F.; Huie, J.R.; Ying, Z.; Ferguson, A.R.; Crown, E.D.; Baumbauer, K.M.; Edgerton, V.R.; Grau, J.W. BDNF and learning: Evidence that instrumental training promotes learning within the spinal cord by up-regulating BDNF expression. Neuroscience 2007, 148, 893–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cote, M.P.; Azzam, G.A.; Lemay, M.A.; Zhukareva, V.; Houle, J.D. Activity-dependent increase in neurotrophic factors is associated with an enhanced modulation of spinal reflexes after spinal cord injury. J. Neurotrauma 2011, 28, 299–309. [Google Scholar] [CrossRef] [Green Version]
- Jung, S.Y.; Seo, T.B.; Kim, D.Y. Treadmill exercise facilitates recovery of locomotor function through axonal regeneration following spinal cord injury in rats. J. Exerc. Rehabil. 2016, 12, 284–292. [Google Scholar] [CrossRef] [Green Version]
- Ying, Z.; Roy, R.R.; Edgerton, V.R.; Gomez-Pinilla, F. Exercise restores levels of neurotrophins and synaptic plasticity following spinal cord injury. Exp. Neurol. 2005, 193, 411–419. [Google Scholar] [CrossRef]
- Tashiro, S.; Tsuji, O.; Shinozaki, M.; Shibata, T.; Yoshida, T.; Tomioka, Y.; Unai, K.; Kondo, T.; Itakura, G.; Kobayashi, Y.; et al. Current progress of rehabilitative strategies in stem cell therapy for spinal cord injury: A review. NPJ Regen. Med. 2021, 6, 81. [Google Scholar] [CrossRef]
- Grau, J.W.; Baine, R.E.; Bean, P.A.; Davis, J.A.; Fauss, G.N.; Henwood, M.K.; Hudson, K.E.; Johnston, D.T.; Tarbet, M.M.; Strain, M.M. Learning to promote recovery after spinal cord injury. Exp. Neurol. 2020, 330, 113334. [Google Scholar] [CrossRef]
- Tashiro, S.; Mizuno, K.; Kawakami, M.; Takahashi, O.; Nakamura, T.; Suda, M.; Haruyama, K.; Otaka, Y.; Tsuji, T.; Liu, M. Neuromuscular electrical stimulation-enhanced rehabilitation is associated with not only motor but also somatosensory cortical plasticity in chronic stroke patients: An interventional study. Ther. Adv. Chronic. Dis. 2019, 10, 2040622319889259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Y.; Mao, Y.R.; Yuan, T.F.; Xu, D.S.; Cheng, L.M. Multimodal treatment for spinal cord injury: A sword of neuroregeneration upon neuromodulation. Neural Regen. Res. 2020, 15, 1437–1450. [Google Scholar] [CrossRef] [PubMed]
- Okawara, H.; Tashiro, S.; Sawada, T.; Sugai, K.; Matsubayashi, K.; Kawakami, M.; Nori, S.; Tsuji, O.; Nagoshi, N.; Matsumoto, M.; et al. Neurorehabilitation using a voluntary driven exoskeletal robot improves trunk function in patients with chronic spinal cord injury: A single-arm study. Neural Regen. Res. 2022, 17, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Shibata, T.; Tashiro, S.; Shinozaki, M.; Hashimoto, S.; Matsumoto, M.; Nakamura, M.; Okano, H.; Nagoshi, N. Treadmill training based on the overload principle promotes locomotor recovery in a mouse model of chronic spinal cord injury. Exp. Neurol. 2021, 345, 113834. [Google Scholar] [CrossRef]
- Ikegami, T.; Nakamura, M.; Yamane, J.; Katoh, H.; Okada, S.; Iwanami, A.; Watanabe, K.; Ishii, K.; Kato, F.; Fujita, H.; et al. Chondroitinase ABC combined with neural stem/progenitor cell transplantation enhances graft cell migration and outgrowth of growth-associated protein-43-positive fibers after rat spinal cord injury. Eur. J. Neurosci. 2005, 22, 3036–3046. [Google Scholar] [CrossRef]
- Kaneko, S.; Iwanami, A.; Nakamura, M.; Kishino, A.; Kikuchi, K.; Shibata, S.; Okano, H.J.; Ikegami, T.; Moriya, A.; Konishi, O.; et al. A selective Sema3A inhibitor enhances regenerative responses and functional recovery of the injured spinal cord. Nat. Med. 2006, 12, 1380–1389. [Google Scholar] [CrossRef]
- Rosenzweig, E.S.; Salegio, E.A.; Liang, J.J.; Weber, J.L.; Weinholtz, C.A.; Brock, J.H.; Moseanko, R.; Hawbecker, S.; Pender, R.; Cruzen, C.L.; et al. Chondroitinase improves anatomical and functional outcomes after primate spinal cord injury. Nat. Neurosci. 2019, 22, 1269–1275. [Google Scholar] [CrossRef]
- Wang, D.; Ichiyama, R.M.; Zhao, R.; Andrews, M.R.; Fawcett, J.W. Chondroitinase combined with rehabilitation promotes recovery of forelimb function in rats with chronic spinal cord injury. J. Neurosci. 2011, 31, 9332–9344. [Google Scholar] [CrossRef]
- Shinozaki, M.; Iwanami, A.; Fujiyoshi, K.; Tashiro, S.; Kitamura, K.; Shibata, S.; Fujita, H.; Nakamura, M.; Okano, H. Combined treatment with chondroitinase ABC and treadmill rehabilitation for chronic severe spinal cord injury in adult rats. Neurosci. Res. 2016, 113, 37–47. [Google Scholar] [CrossRef]
- Bartus, K.; James, N.D.; Didangelos, A.; Bosch, K.D.; Verhaagen, J.; Yanez-Munoz, R.J.; Rogers, J.H.; Schneider, B.L.; Muir, E.M.; Bradbury, E.J. Large-scale chondroitin sulfate proteoglycan digestion with chondroitinase gene therapy leads to reduced pathology and modulates macrophage phenotype following spinal cord contusion injury. J. Neurosci. 2014, 34, 4822–4836. [Google Scholar] [CrossRef] [Green Version]
- Keyvan-Fouladi, N.; Raisman, G.; Li, Y. Functional repair of the corticospinal tract by delayed transplantation of olfactory ensheathing cells in adult rats. J. Neurosci. 2003, 23, 9428–9434. [Google Scholar] [CrossRef] [Green Version]
- Ruitenberg, M.J.; Levison, D.B.; Lee, S.V.; Verhaagen, J.; Harvey, A.R.; Plant, G.W. NT-3 expression from engineered olfactory ensheathing glia promotes spinal sparing and regeneration. Brain 2005, 128, 839–853. [Google Scholar] [CrossRef] [Green Version]
- Sun, T.; Ye, C.; Zhang, Z.; Wu, J.; Huang, H. Cotransplantation of olfactory ensheathing cells and Schwann cells combined with treadmill training promotes functional recovery in rats with contused spinal cords. Cell Transpl. 2013, 22 (Suppl. S1), S27–S38. [Google Scholar] [CrossRef]
- Cheng, Z.; Wang, R.; Cao, K.; Wang, G.; Qin, J.; Li, H.; Li, J.; Wang, D.; He, X. Ten years of clinical observation of olfactory ensheathing cell transplantation in patients with spinal cord injury. J. Neurorestoratology 2021, 9, 106–116. [Google Scholar] [CrossRef]
- Yoshihara, H.; Shumsky, J.S.; Neuhuber, B.; Otsuka, T.; Fischer, I.; Murray, M. Combining motor training with transplantation of rat bone marrow stromal cells does not improve repair or recovery in rats with thoracic contusion injuries. Brain Res. 2006, 1119, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.M.; Jin, J.J.; Lee, S.J.; Seo, T.B.; Ji, E.S. Treadmill exercise with bone marrow stromal cells transplantation facilitates neuroprotective effect through BDNF-ERK1/2 pathway in spinal cord injury rats. J. Exerc. Rehabil. 2018, 14, 335–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younsi, A.; Zheng, G.; Scherer, M.; Riemann, L.; Zhang, H.; Tail, M.; Hatami, M.; Skutella, T.; Unterberg, A.; Zweckberger, K. Treadmill training improves survival and differentiation of transplanted neural precursor cells after cervical spinal cord injury. Stem Cell Res. 2020, 45, 101812. [Google Scholar] [CrossRef]
- Dugan, E.A.; Jergova, S.; Sagen, J. Mutually beneficial effects of intensive exercise and GABAergic neural progenitor cell transplants in reducing neuropathic pain and spinal pathology in rats with spinal cord injury. Exp. Neurol. 2020, 327, 113208. [Google Scholar] [CrossRef] [PubMed]
- Lu, P.; Freria, C.M.; Graham, L.; Tran, A.N.; Villarta, A.; Yassin, D.; Huie, J.R.; Ferguson, A.R.; Tuszynski, M.H. Rehabilitation combined with neural progenitor cell grafts enables functional recovery in chronic spinal cord injury. JCI Insight 2022, 7, e158000. [Google Scholar] [CrossRef]
- Tashiro, S.; Nishimura, S.; Iwai, H.; Sugai, K.; Zhang, L.; Shinozaki, M.; Iwanami, A.; Toyama, Y.; Liu, M.; Okano, H.; et al. Functional Recovery from Neural Stem/Progenitor Cell Transplantation Combined with Treadmill Training in Mice with Chronic Spinal Cord Injury. Sci. Rep. 2016, 6, 30898. [Google Scholar] [CrossRef] [Green Version]
- Shibata, T.; Tashiro, S.; Shibata, S.; Shinozaki, M.; Shindo, T.; Hashimoto, S.; Kawai, M.; Kitagawa, T.; Ago, K.; Matsumoto, M.; et al. Rehabilitative Training Enhances Therapeutic Effect of Human-iPSC-Derived Neural Stem/Progenitor Cells Transplantation in Chronic Spinal Cord Injury. Stem Cells Transl. Med. 2023, 12, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Nagoshi, N.; Khazaei, M.; Ahlfors, J.E.; Ahuja, C.S.; Nori, S.; Wang, J.; Shibata, S.; Fehlings, M.G. Human Spinal Oligodendrogenic Neural Progenitor Cells Promote Functional Recovery After Spinal Cord Injury by Axonal Remyelination and Tissue Sparing. Stem Cells Transl. Med. 2018, 7, 806–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, H.; Ahuja, C.S.; Salewski, R.P.; Li, L.; Satkunendrarajah, K.; Nagoshi, N.; Shibata, S.; Fehlings, M.G. Neural stem cell mediated recovery is enhanced by Chondroitinase ABC pretreatment in chronic cervical spinal cord injury. PLoS ONE 2017, 12, e0182339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Kaneko, S.; Kikuchi, K.; Sano, A.; Maeda, M.; Kishino, A.; Shibata, S.; Mukaino, M.; Toyama, Y.; Liu, M.; et al. Rewiring of regenerated axons by combining treadmill training with semaphorin3A inhibition. Mol. Brain 2014, 7, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashimoto, S.; Nagoshi, N.; Shinozaki, M.; Nakanishi, K.; Suematsu, Y.; Shibata, T.; Kawai, M.; Kitagawa, T.; Ago, K.; Kamata, Y.; et al. Microenvironmental modulation in tandem with human stem cell transplantation enhances functional recovery after chronic complete spinal cord injury. Biomaterials 2023, 295, 122002. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Author (Year) | SCI Animal Model | Cell Source | Training Type | Outcomes of Study |
|---|---|---|---|---|
| Keyvan-Fouladi N (2003) | Late-subacute contusive rats | OECs | Forepaw reaching | Functional repair of corticospinal tracts. |
| Ruitenberg MJ (2005) | Late-subacute contusive rats | OECs | Forepaw reaching | Increase in the number of corticospinal axons. |
| Sun T (2013) | Subacute contusive rats | OECs + Schwann cells | Bipedal treadmill training | Enhancement of increased serotonin activity at lumbar enlargement. |
| Yoshihara H (2006) | Subacute contusive rats | Bone marrow stromal cells | Bicycle training | No difference in cell survival, evidence of axonal growth into grafts and lesion size. |
| Kim YM (2018) | Subacute contusive rats | Bone marrow stromal cells | Quadrupedal treadmill training | Increase expression of BDNF and TrkB and improvement motor function. |
| Hwang DH (2014) | Subacute contusive rats | NS/PCs | Quadrupedal treadmill training | Improvement in NS/PC survival and differentiation into neurons and oligodendrocytes. Attenuation in cellular stresses from reactive nitrogen and oxygen via IGF-1 signaling. |
| Younsi A (2020) | Subacute contusive rats | NS/PCs | Quadrupedal treadmill training | Graft survival, and differentiation into neurons and oligodendrocytes increased. Better functional recovery with synergistic effect. |
| Dugan EA (2020) | Late-subacute contusive rats | GABAergic -NS/PCs | Quadrupedal treadmill training | Enhancement of neuropathic pain reduction as assessed by allodynia and hyperalgesia. Restoration of GABAergic neuronal and process density. |
| Lu P (2022) | Late-subacute contusive rats | NS/PCs | Forepaw reaching | Increase host corticospinal axon regeneration into grafts and improvement of motor function. |
| Tashiro S (2016) | Chronic contusive mice | NS/PCs | Bipedal treadmill training | Facilitation of neuronal differentiation of transplanted cells. Enhancement of neurogenesis in lumbar enlargement. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shibata, T.; Tashiro, S.; Nakamura, M.; Okano, H.; Nagoshi, N. A Review of Treatment Methods Focusing on Human Induced Pluripotent Stem Cell-Derived Neural Stem/Progenitor Cell Transplantation for Chronic Spinal Cord Injury. Medicina 2023, 59, 1235. https://doi.org/10.3390/medicina59071235
Shibata T, Tashiro S, Nakamura M, Okano H, Nagoshi N. A Review of Treatment Methods Focusing on Human Induced Pluripotent Stem Cell-Derived Neural Stem/Progenitor Cell Transplantation for Chronic Spinal Cord Injury. Medicina. 2023; 59(7):1235. https://doi.org/10.3390/medicina59071235
Chicago/Turabian StyleShibata, Takahiro, Syoichi Tashiro, Masaya Nakamura, Hideyuki Okano, and Narihito Nagoshi. 2023. "A Review of Treatment Methods Focusing on Human Induced Pluripotent Stem Cell-Derived Neural Stem/Progenitor Cell Transplantation for Chronic Spinal Cord Injury" Medicina 59, no. 7: 1235. https://doi.org/10.3390/medicina59071235