
An Effectiveness Evaluation of Nucleo-Annuloplasty for Lumbar Discogenic Lesions Using Disc-FX: A Scoping Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Data Extraction
2.3. Quality Assessment
2.4. Surgical Technique
3. Results
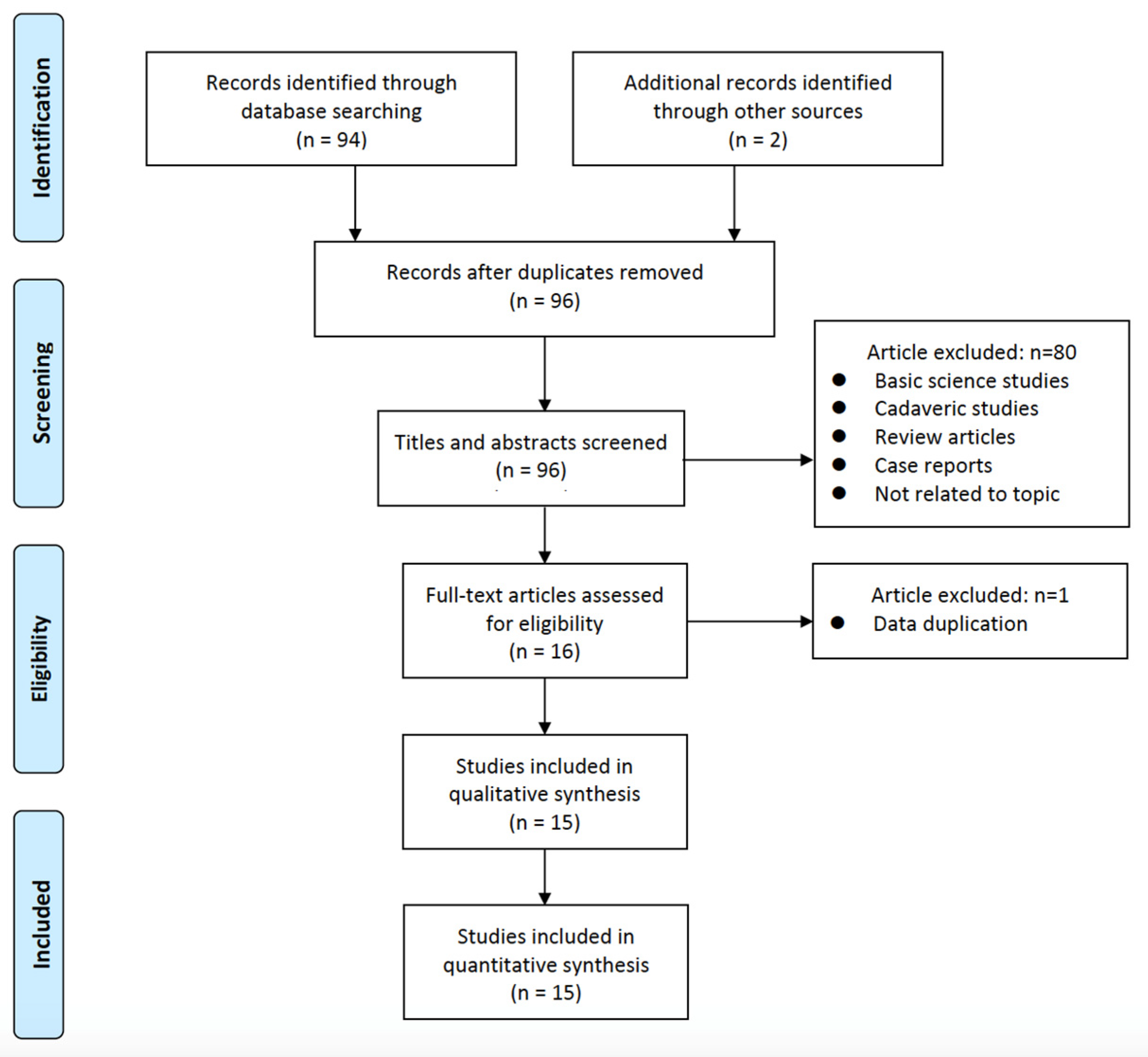
3.1. Selection of Studies and Quality Evaluation
3.2. Study Characteristics and Outcomes
3.3. Complications
4. Discussion
4.1. Mechanism and Diagnosis of Diskogenic Pain
4.2. Features and Advantages of the Disc-FX System
4.3. Indications, Contraindications, and Limitations of the Disc-FX System
4.4. Management and Prevention of Complications
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lin, G.X.; Xu, W.B.; Kotheeranurak, V.; Chen, C.M.; Deng, Z.H.; Zhu, M.T. Comparison of oblique and transforaminal approaches to lumbar interbody fusion for lumbar degenerative disease: An updated meta-analysis. Front. Surg. 2022, 9, 1004870. [Google Scholar] [CrossRef] [PubMed]
- Berthelot, J.M.; Delecrin, J.; Maugars, Y.; Passuti, N. Contribution of centralization phenomenon to the diagnosis, prognosis, and treatment of diskogenic low back pain. Jt. Bone Spine 2007, 74, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Maus, T.P.; Aprill, C.N. Lumbar diskogenic pain, provocation diskography, and imaging correlates. Radiol. Clin. N. Am. 2012, 50, 681–704. [Google Scholar] [CrossRef] [PubMed]
- Ravikanth, R. A review of discogenic pain management by interventional techniques. J. Craniovertebr. Junction Spine 2020, 11, 4–8. [Google Scholar] [CrossRef]
- Gushcha, A.O.; Yusupova, A.R. Minimally invasive surgery and modern view on the treatment of degenerative spine diseases. Zh Vopr. Neirokhir Im. N. N. Burdenko 2021, 85, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.M.L.; Nguyen, D.T.D. Minimally Invasive Treatment for Degenerative Lumbar Spine. Tech. Vasc. Interv. Radiol. 2020, 23, 100700. [Google Scholar] [CrossRef] [PubMed]
- Eksi, M.S.; Ozcan-Eksi, E.E.; Orhun, O.; Turgut, V.U.; Pamir, M.N. Proposal for a new scoring system for spinal degeneration: Mo-Fi-Disc. Clin. Neurol. Neurosurg. 2020, 198, 106120. [Google Scholar] [CrossRef]
- Teichtahl, A.J.; Urquhart, D.M.; Wang, Y.; Wluka, A.E.; O’Sullivan, R.; Jones, G.; Cicuttini, F.M. Lumbar disc degeneration is associated with modic change and high paraspinal fat content—A 3.0T magnetic resonance imaging study. BMC Musculoskelet. Disord. 2016, 17, 439. [Google Scholar] [CrossRef] [Green Version]
- Clark, A.J.; Safaee, M.M.; Khan, N.R.; Brown, M.T.; Foley, K.T. Tubular microdiscectomy: Techniques, complication avoidance, and review of the literature. Neurosurg. Focus. 2017, 43, E7. [Google Scholar] [CrossRef] [Green Version]
- Hoff-Olsen, P.; Wiberg, J. Small bowel perforation as a complication of microsurgical lumbar diskectomy. A case report and brief review of the literature. Am. J. Forensic Med. Pathol. 2001, 22, 319–321. [Google Scholar] [CrossRef]
- Aiyer, R.; Noori, S.; Schirripa, F.; Schirripa, M.; Jain, S.; Aboud, T.; Mehta, N.; Elowitz, E.; Pahuta, M.; Datta, S. A systematic review of full endoscopic versus micro-endoscopic or open discectomy for lumbar disc herniation. Pain Manag. 2022, 12, 87–104. [Google Scholar] [CrossRef] [PubMed]
- Li, X.C.; Zhong, C.F.; Deng, G.B.; Liang, R.W.; Huang, C.M. Full-Endoscopic Procedures Versus Traditional Discectomy Surgery for Discectomy: A Systematic Review and Meta-analysis of Current Global Clinical Trials. Pain Physician 2016, 19, 103–118. [Google Scholar] [PubMed]
- Kumar, N.; Zaw, A.S.; Kumar, N.; Sonawane, D.; Hey, H.W.D.; Kumar, A. Annulo-Nucleoplasty Using Disc-Fx in the Management of Degenerative Lumbar Disc Pathology: How Long Can the Effect Last? Glob. Spine J. 2018, 8, 365–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, N.; Kumar, A.; Siddharth, M.S.; Sambhav, P.S.; Tan, J. Annulo-nucleoplasty using Disc-FX in the management of lumbar disc pathology: Early results. Int. J. Spine Surg. 2014, 8, 18. [Google Scholar] [CrossRef] [Green Version]
- Beyaz, S.G.; Inanmaz, M.E.; Zengin, E.S.; Ulgen, A.M. Combined Use of High Radiofrequency Disk Ablation, Annulus Modulation, and Manual Nucleotomy in a Patient with Extruded Disk Herniation. Pain Pract. 2016, 16, E74–E80. [Google Scholar] [CrossRef]
- Bai, Y.; Xi, C.; Zhao, W.; Mu, X.; Tan, F.; Wang, L.; Ma, Y. Analysis of clinical efficacy on percutaneous discectomy combined with radiofrequency ablation by Disc-FX in contained lumbar disc herniation. Chin. J. Pain Med. 2011, 17, 280–283. [Google Scholar]
- Chen, S.Y.Y.; Mei, W. Disc-FX system for minimally invasive treatment of accommodative lumbar disc herniation. Chin. Orthop. 2014, 26, 46–47. [Google Scholar]
- Hirano, Y.P.S.; Bansil, R.; Watnabe, K. Advantages of Endoscope-Assisted Disc-FX in Surgical Management of Lumbar Disc Herniation: A Report of 10 Cases. J. Spine 2018, S7, 1–4. [Google Scholar]
- Lu, Z.Y.Y.; Fan, F.; Chen, S.; Zheng, S.; Sun, Y.; Bao, C.; Wang, Y. Clinical analysis of the 3-in-1 technique of Disc-FX system for discogenic low back pain. Chin. J. Parct. Med. 2013, 40, 65–67. [Google Scholar]
- Liao, X.J.J.; Xiong, D.; Yi, W.; Zhang, Q.; Zheng, H.; Luo, Y.; Linag, H.; Zhang, D. The comparison of clinical outcomes of percutaneous lumbar discectomy with Disc-FX system with fenestration and decompression for contained lumbar disc herniation with radicular pain. Chin. J. Pain Med. 2011, 17, 25–29. [Google Scholar]
- Ma, Y.W.P. Analysis of changes in serum substance P and inflammatory factors before and after minimally invasive Disc-FX surgery for discogenic low back pain and evaluation of early efficacy. J. Cervicodynia Lumbodynia 2021, 42, 386–388. [Google Scholar]
- Ou, J. Clinical efficacy of the treatment of discectomy, radiofrequency ablation and annulus fibrosus angioplasty under the guidance of Disc-FX system for contained lumbar disc herniation. Chin. J. Mod. Med. 2013, 23, 91–93. [Google Scholar]
- Park, C.H.; Lee, S.H. Efficacy of Nucleo-Annuloplasty Using Disc-Fx in Lumbar Disc Herniation. J. Spine 2015, 4, 1–4. [Google Scholar]
- Park, C.H.; Lee, K.K.; Lee, S.H. Efficacy of transforaminal laser annuloplasty versus intradiscal radiofrequency annuloplasty for discogenic low back pain. Korean J. Pain 2019, 32, 113–119. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.Z.; Xia, Q.; Zheng, B.; Shi, K.; Ma, W.; Liu, J. Efficacy of lumbar discectomy radiofrequency ablation and annuloplasty with Disc-FX system. Chin. J. Anesthesiol. 2013, 33, 430–432. [Google Scholar]
- Xi, J.M.; Hu, M.; Chui, X.; Zhao, W.; Mu, X. Early clinical efficacy analysis of Disc-FX system percutaneous disc removal and radiofrequency ablation for inclusive lumbar disc herniation. Chin. J. Bone Jt. Surg. 2012, 5, 252–254. [Google Scholar]
- Yam, J.O.; Cheung, P.; Chiang, L.F.; Wan, S.Y.S.; Mok, W.Y. Efficacy and safety of nucleo-annuloplasty using radiofrequency ablation for discogenic back pain in a local Hong Kong population. J. Orthop. Trauma Rehabil. 2021, 1–8. [Google Scholar] [CrossRef]
- Zhang, W.W.; Jiao, J.; Wang, Y.; Yang, D.; Ding, W.; Shen, Y. Primary results of the 3-in-1 technique of Disc-FX system for the discogenic low back pain. Chin. J. Orthop. 2011, 31, 1049–1055. [Google Scholar]
- Zhang, J.S.; Su, S.; Lin, D. Disc-FX system-assisted percutaneous nucleus pulposus clamping with radiofrequency ablation for discogenic low back pain. J. Spinal Surg. 2015, 13, 7–10. [Google Scholar]
- Kim, H.S.; Wu, P.H.; Jang, I.T. Lumbar Degenerative Disease Part 1: Anatomy and Pathophysiology of Intervertebral Discogenic Pain and Radiofrequency Ablation of Basivertebral and Sinuvertebral Nerve Treatment for Chronic Discogenic Back Pain: A Prospective Case Series and Review of Literature. Int. J. Mol. Sci. 2020, 21, 1483. [Google Scholar]
- Simon, J.; McAuliffe, M.; Shamim, F.; Vuong, N.; Tahaei, A. Discogenic low back pain. Phys. Med. Rehabil. Clin. N. Am. 2014, 25, 305–317. [Google Scholar] [CrossRef] [PubMed]
- Urits, I.; Burshtein, A.; Sharma, M.; Testa, L.; Gold, P.A.; Orhurhu, V.; Viswanath, O.; Jones, M.R.; Sidransky, M.A.; Spektor, B.; et al. Low Back Pain, a Comprehensive Review: Pathophysiology, Diagnosis, and Treatment. Curr. Pain Headache Rep. 2019, 23, 23. [Google Scholar] [CrossRef] [PubMed]
- Bogduk, N.; Aprill, C.; Derby, R. Lumbar discogenic pain: State-of-the-art review. Pain Med. 2013, 14, 813–836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, S.; Boudier-Reveret, M.; Chang, M.C. Use of Pulsed Radiofrequency for the Treatment of Discogenic Back Pain: A Narrative Review. Pain Pract. 2021, 21, 594–601. [Google Scholar] [CrossRef]
- Zhao, L.; Manchikanti, L.; Kaye, A.D.; Abd-Elsayed, A. Treatment of Discogenic Low Back Pain: Current Treatment Strategies and Future Options-a Literature Review. Curr. Pain Headache Rep. 2019, 23, 86. [Google Scholar] [CrossRef]
- Gelalis, I.; Gkiatas, I.; Spiliotis, A.; Papadopoulos, D.; Pakos, E.; Vekris, M.; Korompilias, A. Current Concepts in Intradiscal Percutaneous Minimally Invasive Procedures for Chronic Low Back Pain. Asian J. Neurosurg. 2019, 14, 657–669. [Google Scholar] [CrossRef]
- Liu, Z.; Ma, R.; Fan, C.; Chen, J.; Zhang, R.; Zheng, Z.; Xu, Y.; Liu, Z.; Zhao, Q.; Li, Q. Sinuvertebral nerve block treats discogenic low back pain: A retrospective cohort study. Ann. Transl. Med. 2022, 10, 1219. [Google Scholar] [CrossRef]
- Zhang, C.; Li, Z.; Yu, K.; Wang, Y. A Postoperative Phenomenon of Percutaneous Endoscopic Lumbar Discectomy: Rebound Pain. Orthop. Surg. 2021, 13, 2196–2205. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]

{kind=link}
| Studies | Selection | Comparability | Exposure | Total Scores (of 9) | |||||
|---|---|---|---|---|---|---|---|---|---|
| Is the Case Definition Adequate? | Representativeness of the Cases | Selection of Controls | Definition of Controls | Comparability of Cases and Controls on the Basis of the Design or Analysis | Ascertainment of Exposure | Same Method of Ascertainment for Cases and Controls | Non-Response Rate | ||
| Bai et al. [16], 2011 | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | 8☆ | |
| Chen et al. [17], 2014 | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7☆ | |
| Hirano et al. [18], 2018 | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7☆ | |
| Kumar et al. [13], 2018 | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | ☆ | 9☆ |
| Lu et al. [19], 2013 | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7☆ | |
| Liao et al. [20], 2011 | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | 8☆ | |
| Ma et al. [21], 2021 | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | 8☆ | |
| Ou et al. [22], 2013 | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | ☆ | 9☆ |
| Park et al. [23], 2015 | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | 8☆ | |
| Park et al. [24], 2019 | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | 8☆ | |
| Wang et al. [25], 2013 | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | 8☆ | |
| Xi et al. [26], 2012 | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | ☆ | 9☆ |
| Yam et al. [27], 2021 | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | ☆ | 9☆ |
| Zhang et al [28].,2011 | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | 8☆ | |
| Zhang et al. [29], 2015 | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | ☆ | 9☆ |
| Authors and Year | Study Type | Study Period | No. of Patients (Levels) | Operated Levels | Age (Years), Mean; Range | Sex (M:F) | Follow-Up Period (mo) | Complications (n) |
|---|---|---|---|---|---|---|---|---|
| Bai et al. [16], 2011 | Retrospective | 2010.07–2010.10 | 36 (NR) | NR | 47.5; 18–77 | 16:20 | 6 | None |
| Chen et al. [17], 2014 | Retrospective | 2011.10–2013.02 | 36 (36) | L3–4 (5); L4–5 (21); L5–S1 (10) | 43.5; 26–65 | 21:15 | 6–12 | None |
| Hirano et al. [18], 2018 | Retrospective | NR | 10 (10) | L1–2 (1); L3–4 (2); L4–5 (6); L5–S1 (2) | 47.2; 30–72 | 8:2 | 6 | None |
| Kumar et al. [13], 2018 | Prospective | 2010.09–2014.12 | 51 (66) | L2–3 (1); L3–4 (8); L4–5 (27); L5–S1 (30) | 41: 20–63 | 38:13 | 24 | Infection (1), postoperative transient pain (16) |
| Lu et al. [19], 2013 | Retrospective | 2011.02–2012.05 | 35 (35) | NR | 36.5; 27–56 | 23:12 | 14.8 | Recurrent (1) |
| Liao et al. [20], 2011 | Retrospective | 2008.05–2010.05 | 25 (NR) | NR | NR | NR | 12 | None |
| Ma et al. [21], 2021 | Retrospective | 2013.01–2015.12 | 56 (NR) | NR | 51.2 ± 12.4; 43–65 | 32:24 | 3 | Recurrent (5), nerve root injury (2); postoperative transient pain (8) |
| Ou et al. [22], 2013 | Retrospective | 2010.09–2011.10 | 62 (70) | L3–4 (5); L4–5 (36); L5–S1 (29) | 45.3 ± 16.9: 21–75 | 25:37 | 6 | None |
| Park et al. [23], 2015 | Retrospective | NR | 43 (NR) | NR | 44.9; 22–77 | 30:13 | 6 | None |
| Park et al. [24], 2019 | Retrospective | NR | 43 (NR) | NR | 56.7 ± 14.1; NR | 20:23 | 6 | None |
| Wang et al. [25], 2013 | Retrospective | NR | 28 (NR) | NR | NR; 27–73 | NR | 2 | Recurrent (2), lumbar venous plexus injury (1) |
| Xi et al. [26], 2012 | Retrospective | 2010.07–2011.06 | 36 (73) | L2–3 (4); L3–4 (13); L4–5 (32); L5–S1 (24) | 56; 18–77 | 16:20 | 12 | Infection (1), postoperative hematoma (1), postoperative transient pain (26) |
| Yam et al. [27], 2021 | Retrospective | 2017–2019 | 16 (24) | L2–3 (1); L3–4 (3); L4–5 (12); L5–S1 (8) | NR; 23–69 | 13:3 | >6 | Re-operation (1) |
| Zhang et al [28], 2011 | Retrospective | 2010.02–2011.02 | 40 (47) | L3–4 (3); L4–5 (23); L5–S1 (21) | 38.7; 32–58 | 22:18 | 13.8 (6–18) | Recurrent (1) |
| Zhang et al. [29], 2015 | Retrospective | 2010.06–2011.05 | 53 (NR) | NR | NR; 29–56 | 24:29 | 24 | None |
| Authors and Year | Operative Time (mins) | Blood Loss (mL) | Preoperative | Final Follow-Up | Macnab | ||
|---|---|---|---|---|---|---|---|
| Pain Rating Scale | Functional Rating Scale | Pain Rating Scale | Functional Rating Scale | ||||
| Bai et al. [16], 2011 | 15–20 | 0–5 | VAS: 6.5 ± 1.8 | JOA: 19.3 ± 3.6; ODI: 18.7 ± 11.8 | VAS: 2.5 ± 2.2 | JOA: 25.5 ± 3.2; ODI: 9.1 ± 8.5 | 81.3% |
| Chen et al. [17], 2014 | 15–30 | 5 | VAS: 8.5 ± 1.4 | JOA: 12.3 ± 1.2 | VAS: 2.1 ± 0.8 | JOA: 25.5 ± 2.1 | NR |
| Hirano et al. [18], 2018 | NR | NR | VAS: 8.0 | JOA: 13.0 | VAS: 1.2 | JOA: 25.9 | NR |
| Kumar et al. [13], 2018 | NR | NR | VAS: 6.69 ± 0.93 | ODI: 47.80 ± 17.92 | VAS: 2.85 ± 1.76 | ODI: 19.63 ± 14.14 | 78.4% |
| Lu et al. [19], 2013 | 29 | NR | VAS: 6.70 ± 1.26 | ODI: 19.9 ± 6.8 | VAS: 1.05 ± 0.66 | ODI: 8.6 ± 4.5 | NR |
| Liao et al. [20], 2011 | 30 ± 5 | 2 ± 1 | VAS: 7.8 ± 0.4 | ODI: 39.1 ± 3.9 | VAS: 2.0 ± 0.1 | ODI: 11.4 ± 1.6 | NR |
| Ma et al. [21], 2021 | NR | NR | VAS: 6.2 ± 1.5 | JOA: 17.4 ± 3.8 | VAS: 2.2 ± 1.3 | JOA: 25.9 ± 1.3 | 89.3% |
| Ou et al. [22], 2013 | 25.16 ± 3.21 | 0–5 | VASB: 3.07 ± 1.15; VASL: 6.72 ± 1.26 | NR | VASB: 0.98 ± 0.54; VASL: 0.97 ± 0.58 | NR | 95.2% |
| Park et al. [23], 2015 | NR | NR | NRS: 7.4 ± 0.8 | NR | NRS: 3.7 ± 1.9 | NR | NR |
| Park et al. [24], 2019 | NR | NR | NRS: 7.3 ± 0.8 | ODI: 57.2 ±10.0 | NRS: 3.6 ± 1.8 | ODI: 22.1 ± 8.4 | NR |
| Wang et al. [25], 2013 | NR | NR | VAS: 8.0 ± 1.2 | NR | VAS: 1.2 ± 0.8 | NR | 93% |
| Xi et al. [26], 2012 | 18 | 0–5 | VAS: 6.5 ± 1.8 | JOA: 19.3 ± 3.6; ODI: 18.7 ± 11.8 | VAS: 2.1 ± 1.7 | JOA: 26.6 ± 2.4; ODI: 7.7 ± 6.5 | 78.9% |
| Yam et al. [27], 2021 | NR | NR | NRS: 6.25 | ODI: 46.25 | NRS: 4.4 | ODI: 24.12 | NR |
| Zhang et al [28], 2011 | 26 | <0 | VASB: 6.60 ± 1.47; VASL: 0.95 ± 0.63 | NR | VASB: 3.05 ± 1.23; VASL: 0.95 ± 0.54 | NR | 92.5% |
| Zhang et al. [29], 2015 | 35–60 | NR | VAS: 7.3 ± 1.1 | NR | VAS: 0.9 ± 0.2 | NR | 92.4% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, G.-X.; Jhang, S.-W.; Chen, C.-M. An Effectiveness Evaluation of Nucleo-Annuloplasty for Lumbar Discogenic Lesions Using Disc-FX: A Scoping Review. Medicina 2023, 59, 1291. https://doi.org/10.3390/medicina59071291
Lin G-X, Jhang S-W, Chen C-M. An Effectiveness Evaluation of Nucleo-Annuloplasty for Lumbar Discogenic Lesions Using Disc-FX: A Scoping Review. Medicina. 2023; 59(7):1291. https://doi.org/10.3390/medicina59071291
Chicago/Turabian StyleLin, Guang-Xun, Shang-Wun Jhang, and Chien-Min Chen. 2023. "An Effectiveness Evaluation of Nucleo-Annuloplasty for Lumbar Discogenic Lesions Using Disc-FX: A Scoping Review" Medicina 59, no. 7: 1291. https://doi.org/10.3390/medicina59071291
APA StyleLin, G.-X., Jhang, S.-W., & Chen, C.-M. (2023). An Effectiveness Evaluation of Nucleo-Annuloplasty for Lumbar Discogenic Lesions Using Disc-FX: A Scoping Review. Medicina, 59(7), 1291. https://doi.org/10.3390/medicina59071291