
Clinical Outcomes of Three versus Four Mini-Implants Retaining Mandibular Overdenture: A 5-Year Randomized Clinical Trial
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
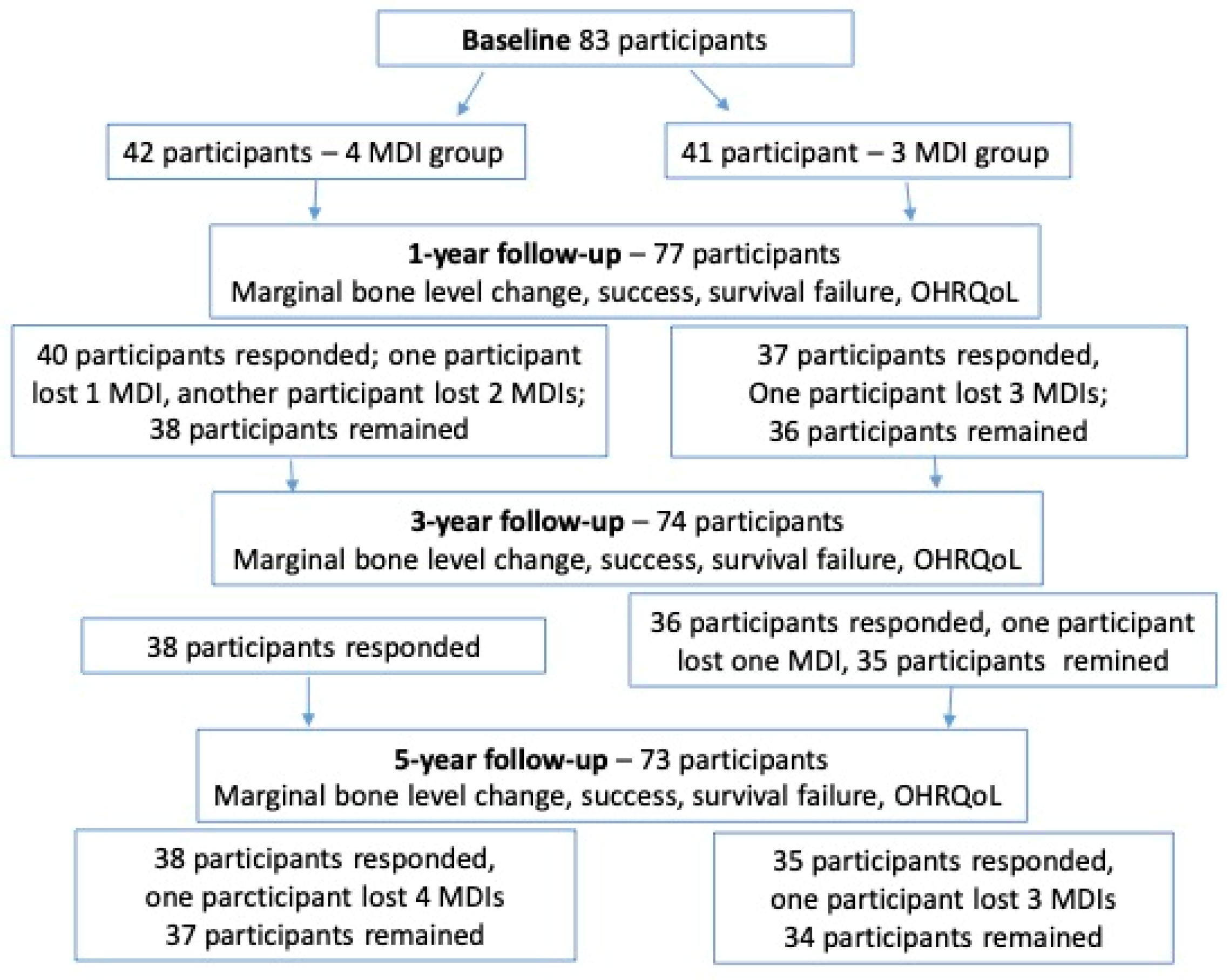
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Sample Size Calculation
2.4. Surgical Procedures
2.5. Prosthodontic Protocol
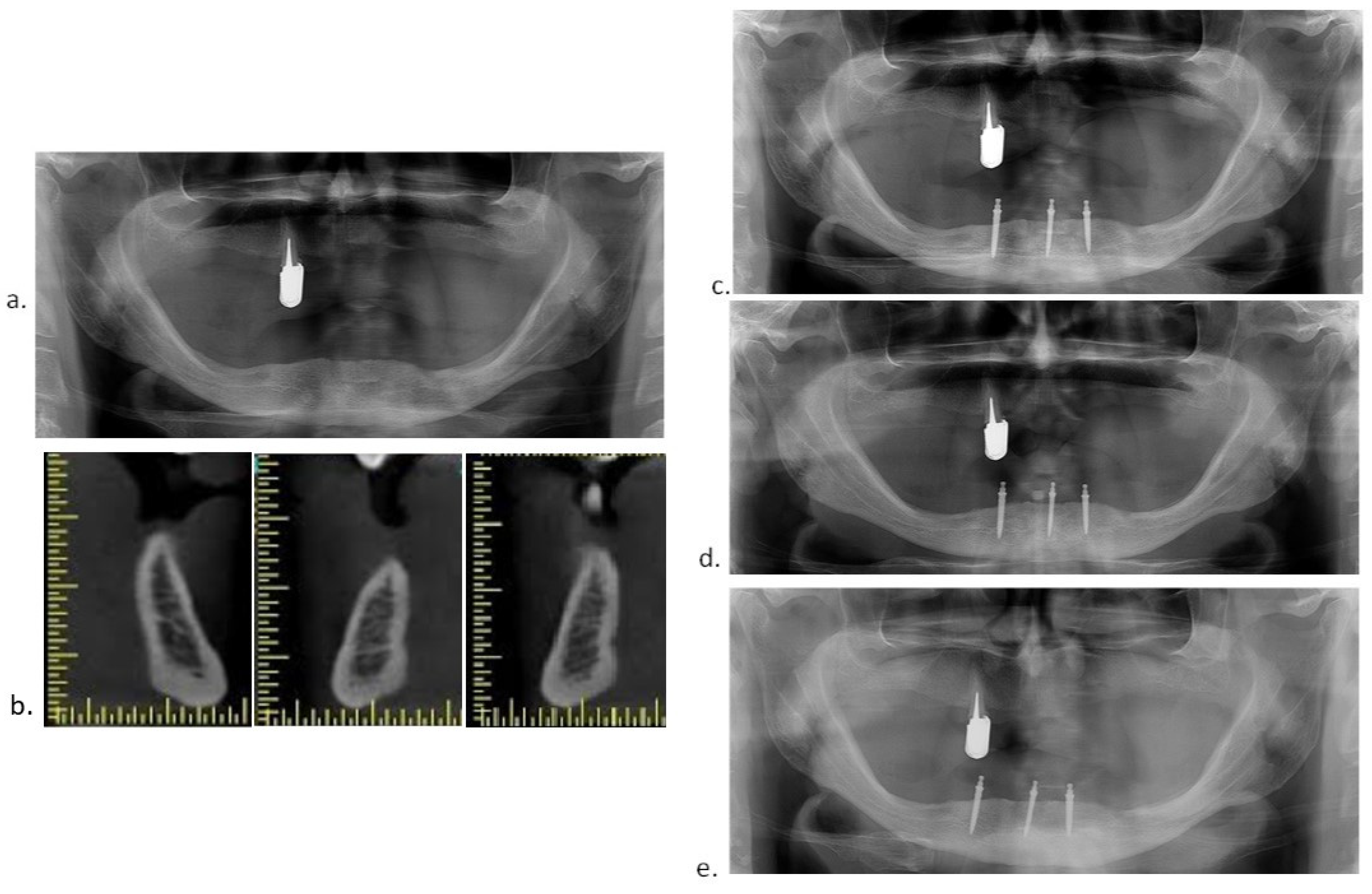
2.6. Radiographic Evaluation
2.7. Implant Success and Survival Rates
2.8. Prosthetic Complications and Maintenance
2.9. Statistical Analysis
3. Results
3.1. Marginal Bone Level (MBL) Change
3.2. Success, Survival, and Failure Rates
3.3. Prosthetic Complications and Maintenance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bulard, R.A.; Vance, J.B. Multi-clinic evaluation using mini-dental implants for long-term denture stabilization: A preliminary biometric evaluation. Compend. Contin. Educ. Dent. 2005, 26, 892–897. [Google Scholar] [PubMed]
- Griffitts, T.M.; Collins, C.P.; Collins, P.C. Mini dental implants: An adjunct for retention, stability, and comfort for the edentulous patient. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, e81–e84. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, D. Rationale for Mini Dental Implant Treatment. J. Oral Implantol. 2021, 47, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Topić, J.; Poljak-Guberina, R.; Persic-Kirsic, S.; Kovacic, I.; Petricevic, N.; Popovac, A.; Čelebić, A. Adaptation to New Dentures and 5 Years of Clinical Use: A Comparison between Complete Denture and Mini-implant Mandibular Overdenture Patients based on Oral Health-Related Quality of Life (OHRQoL) and Orofacial Esthetics. Acta Stomatol. Croat. 2022, 56, 132–142. [Google Scholar] [CrossRef] [PubMed]
- de Souza, R.F.; Ribeiro, A.B.; Della Vecchia, M.P.; Costa, L.; Cunha, T.R.; Reis, A.C.; Albuquerque, R.F., Jr. Mini vs. Standard Implants for Mandibular Overdentures: A Randomized Trial. J. Dent. Res. 2015, 94, 1376–1384. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Shin, S.W.; Lee, J.Y. Mini-implant mandibular overdentures under a two-step immediate loading protocol: A 4–6-year retrospective study. Gerodontology 2023, 40, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Al-Nawas, B.; Araujo, M.; Avila-Ortiz, G.; Barter, S.; Brodala, N.; Chappuis, V.; Chen, B.; De Souza, A.; Almeida, R.F.; et al. Group 1 ITI Consensus Report: The influence of implant length and design and medications on clinical and patient-reported outcomes. Clin. Oral Implants Res. 2018, 29 (Suppl. S16), 69–77. [Google Scholar] [CrossRef] [PubMed]
- Kovačić, I.; Peršić, S.; Disha, V.; Rener-Sitar, K.; Čelebić, A. Short-Term Postoperative Pain and Swelling Associated with Mini and Standard-Size Implants in the Same Patients. Int. J. Prosthodont. 2018, 31, 117–119. [Google Scholar] [CrossRef]
- Kahn, A.; Masri, D.; Shalev, T.; Meir, H.; Sebaoun, A.; Chaushu, L. Patients’ Perception of Recovery after Dental Implant Placement. Medicina 2021, 57, 1111. [Google Scholar] [CrossRef]
- Jawad, S.; Clarke, P.T. Survival of Mini Dental Implants Used to Retain Mandibular Complete Overdentures: Systematic Review. Int. J. Oral Maxillofac. Implants 2019, 34, 343–356. [Google Scholar] [CrossRef]
- Enkling, N.; Haueter, M.; Worni, A.; Müller, F.; Leles, C.R.; Schimmel, M. A prospective cohort study on survival and success of one-piece mini-implants with associated changes in oral function: Five-year outcomes. Clin. Oral Implants Res. 2019, 30, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Čelebić, A.; Peršić, S.; Kovačić, I.; Buković, D.; Lešić, N.; Rener-Sitar, K. Comparison of Three Prosthodontic Treatment Modalities for Patients with Periodontally Compromised Anterior Mandibular Teeth: A 2-year follow-up study. Acta Stomatol. Croat. 2019, 53, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Peršić, S.; Ćelić, R.; Vojvodić, D.; Petričević, N.; Kranjčić, J.; Zlatarić, D.K.; Čelebić, A. Oral Health-Related Quality of Life in Different Types of Mandibular Implant Overdentures in Function Longer Than 3 Years. Int. J. Prosthodont. 2016, 29, 28–30. [Google Scholar] [CrossRef] [PubMed]
- Borges, G.A.; Codello, D.J.; Del Rio Silva, L.; Dini, C.; Barão, V.A.R.; Mesquita, M.F. Factors and clinical outcomes for standard and mini-implants retaining mandibular overdentures: A systematic review and meta-analysis. J. Prosthet. Dent. 2023, 130, 677–689. [Google Scholar] [CrossRef] [PubMed]
- Kovačić, I.; Peršić, S.; Kranjčić, J.; Celebic, A. A cohort study on short mini-implants for mandibular overdentures compared to those of standard length. Clin. Oral Implants Res. 2020, 31, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Kovacic, I.; Persic, S.; Kranjcic, J.; Lesic, N.; Celebic, A. Rehabilitation of an Extremely Resorbed Edentulous Mandible by Short and Narrow Dental Implants. Case Rep. Dent. 2018, 2018, 7597851. [Google Scholar] [CrossRef] [PubMed]
- Ćorić, A.; Kovačić, I.; Kiršić, S.P.; Čelebić, A. Are Mini Dental Implants Suitable for Support of Crowns or Small Bridges in the Mandibular Incisor Region? A 5-year Longitudinal Study. J. Oral Maxillofac. Surg. 2022, 80, 1811–1826. [Google Scholar] [CrossRef] [PubMed]
- Mundt, T.; Heinemann, F.; Müller, J.; Schwahn, C.; Al Jaghsi, A. Survival and stability of strategic mini-implants with immediate or delayed loading under removable partial dentures: A 3-year randomized controlled clinical trial. Clin. Oral. Investig. 2023, 27, 1767–1779. [Google Scholar] [CrossRef]
- Celebic, A.; Kovacic, I.; Petricevic, N.; Puljic, D.; Popovac, A.; Kirsic, S.P. Mini-Implants Retaining Removable Partial Dentures in Subjects without Posterior Teeth: A 5-Year Prospective Study Comparing the Maxilla and the Mandible. Medicina 2023, 59, 237. [Google Scholar] [CrossRef]
- Mundt, T.; Schwahn, C.; Heinemann, F.; Schimmel, M.; Lucas, C.; Al Jaghsi, A. Stabilizing Removable Partial Dentures by Immediate or Delayed Loading of Mini-implants: Chewing Efficiency in a Randomized Controlled Clinical Trial. Int. J. Oral Maxillofac. Implants 2020, 35, 178–186. [Google Scholar] [CrossRef]
- Güven, S.Ş.; Cabbar, F.; Güler, N. Local and systemic factors associated with marginal bone loss around dental implants: A retrospective clinical study. Quintessence Int. 2020, 52, 128–141. [Google Scholar] [CrossRef]
- Albrektsson, T.; Chrcanovic, B.; Östman, P.O.; Sennerby, L. Initial and long-term crestal bone responses to modern dental implants. Periodontology 2000 2017, 73, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Koller, C.D.; Pereira-Cenci, T.; Boscato, N. Parameters Associated with Marginal Bone Loss around Implant after Prosthetic Loading. Braz. Dent J. 2016, 27, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Moreno, P.; Catena, A.; Lopez-Chaichio, L.; Borges, T.; O’Valle, F.; Torrecillas-Martínez, L.; Padial-Molina, M. The Influence of History of Severe Periodontitis on Estimated Long-Term Marginal Bone Loss around Implants Restored with Fixed Segmented Full-Arch Rehabilitation. J. Clin. Med. 2023, 12, 6665. [Google Scholar] [CrossRef] [PubMed]
- Kullar, A.S.; Miller, C.S. Are There Contraindications for Placing Dental Implants? Dent. Clin. N. Am. 2019, 63, 345–362. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E.; Perel, M.L.; Wang, H.-L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti, A.; Pikos, M.A.; et al. Implant Success, Survival, and Failure: The International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant Dent. 2008, 17, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Della Vecchia, M.P.; Leles, C.R.; Cunha, T.R.; Ribeiro, A.B.; Sorgini, D.B.; Muglia, V.A.; Reis, A.C.; Albuquerque, R.F., Jr.; de Souza, R.F. Mini-Implants for Mandibular Overdentures: Cost-Effectiveness Analysis alongside a Randomized Trial. JDR Clin. Trans. Res. 2018, 3, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Catalán, A.; Martínez, A.; Marchesani, F.; González, U. Mandibular Overdentures Retained by Two Mini-Implants: A Seven-Year Retention and Satisfaction Study. J. Prosthodont. 2016, 25, 364–370. [Google Scholar] [CrossRef]
- Bellia, E.; Boggione, L.; Terzini, M.; Manzella, C.; Menicucci, G. Immediate Loading of Mandibular Overdentures Retained by Two Mini-Implants: A Case Series Preliminary Report. Int. J. Prosthodont. 2018, 31, 558–564. [Google Scholar] [CrossRef]
- Jofré, J.; Hamada, T.; Nishimura, M.; Klattenhoff, C. The effect of maximum bite force on marginal bone loss of mini-implants supporting a mandibular overdenture: A randomized controlled trial. Clin. Oral Implants Res. 2010, 21, 243–249. [Google Scholar] [CrossRef]
- Roy, S.; Maji, S.; Paul, R.; Bhattacharyya, J.; Goel, P. A comparison of cost and cost-effectiveness analysis of two- implant-retained overdentures versus other removable prosthodontic treatment options for edentulous mandible: A systematic review. J. Indian Prosthodont. Soc. 2020, 20, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Mifsud, D.P.; Cortes, A.R.G.; Zarb, M.J.; Attard, N.J. Maintenance and risk factors for fractures of overdentures using immediately loaded conventional diameter or mini implants with Locator abutments: A cohort study. Clin. Implant Dent. Relat. Res. 2020, 22, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.G.; Caprioglio, A.; Levrini, L.; Farronato, D.; Zecca, P.A.; Mangano, C. Immediate loading of mandibular overdentures supported by one-piece, direct metal laser sintering mini-implants: A short-term prospective clinical study. J. Periodontol. 2015, 86, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Lemos, C.A.; Verri, F.R.; Batista, V.E.; Júnior, J.F.; Mello, C.C.; Pellizzer, E.P. Complete overdentures retained by mini implants: A systematic review. J. Dent. 2017, 57, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Schiegnitz, E.; Al-Nawas, B. Narrow-diameter implants: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29 (Suppl. S16), 21–40. [Google Scholar] [CrossRef]
- Hussein, M.O.; Alruthea, M.S. Marginal Bone Level Changes and Oral Health Impact Profile (14) Score of Smokers Treated by Mandibular Mini Implant Overdentures: A 5-Year Follow-up Study. Eur. J. Dent. 2020, 14, 590–597. [Google Scholar] [CrossRef]
- Mundt, T.; Schwahn, C.; Biffar, R.; Heinemann, F. Changes in Bone Levels Around Mini-Implants in Edentulous Arches. Int. J. Oral Maxillofac. Implants 2015, 30, 1149–1155. [Google Scholar] [CrossRef]
- Zygogiannis, K.; Aartman, I.H.; Parsa, A.; Tahmaseb, A.; Wismeijer, D. Implant Mandibular Overdentures Retained by Immediately Loaded Implants: A 1-Year Randomized Trial Comparing the Clinical and Radiographic Outcomes Between Mini Dental Implants and Standard-Sized Implants. Int. J. Oral Maxillofac. Implants 2017, 32, 1377–1388. [Google Scholar] [CrossRef]
- Enkling, N.; Moazzin, R.; Geers, G.; Kokoschka, S.; Abou-Ayash, S.; Schimmel, M. Clinical Outcomes and Bone-Level Alterations around One-Piece Mini Dental Implants Retaining Mandibular Overdentures: 5-Year Follow-up of a Prospective Cohort Study. Clin. Oral Implants Res. 2020, 31, 549–556. [Google Scholar] [CrossRef]
- González-Gil, D.; Dib-Zaitum, I.; Flores-Fraile, J.; López-Marcos, J. Importance of Osseoperception and Tactile Sensibility during Masticatory Function in Different Prosthetic Rehabilitations: A Review. Medicina 2022, 58, 92. [Google Scholar] [CrossRef]
- Elsyad, M.A. Patient Satisfaction and Prosthetic Aspects with Mini-Implants Retained Mandibular Overdentures. A 5-Year Prospective Study. Clin. Oral Implants Res. 2016, 27, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Linkevicius, T.; Alkimavicius, J.; Linkevicius, R.; Gineviciute, E.; Linkeviciene, L. Effect of Ti-Base Abutment Gingival Height on Maintenance of Crestal Bone in Thick Biotype Patients: A Randomized Clinical Trial with 1-Year Follow-up. Int. J. Oral Maxillofac. Implants 2022, 37, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Tavelli, L.; Barootchi, S.; Avila-Ortiz, G.; Urban, I.A.; Giannobile, W.V.; Wang, H.L. Peri-implant soft tissue phenotype modification and its impact on peri-implant health: A systematic review and network meta-analysis. J. Periodontol. 2021, 92, 21–44. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.M.; Choi, B.H.; Li, J.; Xuan, F. The effect of thick mucosa on peri-implant tissues: An experimental study in dogs. J. Periodontol. 2008, 79, 2151–2155. [Google Scholar] [CrossRef]
- Peršić, S.; Čelebić, A. Influence of Different Prosthodontic Rehabilitation Options on Oral Health-Related Quality of Life, Orofacial Esthetics and Chewing Function Based on Patient-Reported Outcomes. Qual. Life Res. 2015, 24, 919–926. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MBL Change | Group | N | Mean (in mm) | SD | Minimum (in mm) | Maximum (in mm) | t | df | p |
|---|---|---|---|---|---|---|---|---|---|
| 1 year | 3 MDIs | 36 | −0.21 | 0.24 | 0.00 | −1.08 | 0.56 | 72 | 0.577 NS |
| 4 MDIs | 38 | −0.18 | 0.30 | 0.00 | −1.53 | ||||
| 3 years | 3 MDIs | 35 | −0.33 | 0.52 | 0.00 | −3.02 | 0.61 | 71 | 0.544 NS |
| 4 MDIs | 38 | −0.26 | 0.45 | 0.00 | −2.46 | ||||
| 5 years | 3 MDIs | 34 | −0.33 | 0.27 | 0.00 | −1.00 | 0.60 | 69 | 0.546 NS |
| 4 MDIs | 37 | −0.36 | 0.74 | 0.00 | −4.38 |
| Successful Implants | 95% Confidence Interval (Time in Months) | |||||
|---|---|---|---|---|---|---|
| Group | Number of implants | Number of events (failure and compromised survival) | n | Rate (%) (success and satisfactory survival) | Lower bound | Upper bound |
| 3-MDI | 108 | 9 (8.3%) | 99 | 91.7 | 56.23 | 50.10 |
| 4-MDI | 160 | 10 (6.2%) | 150 | 93.8 | 57.6 | 60.17 |
| Overall | 268 | 19 (7.1%) | 249 | 92.9 | 57.53 | 59.67 |
| Chi-Square | df | p | |
|---|---|---|---|
| Log-rank (Mantel–Cox) | 0.373 | 1 | 0.541 NS |
| Successful Implants | 95% Confidence Interval (Time in Months) | |||||
|---|---|---|---|---|---|---|
| Group | Number of implants | Number of events (failure and compromised survival) | n | Rate (%) (success and satisfactory survival) | Lower bound | Upper bound |
| 3-MDI | 37 | 3 (8.1%) | 34 | 91.9 | 57.58 | 60.91 |
| 4-MDI | 40 | 4 (10.0%) | 36 | 90.0 | 52.62 | 61.58 |
| Overall | 77 | 7 (9.1%) | 70 | 90.9 | 55.85 | 60.43 |
| Chi-Square | df | p | |
|---|---|---|---|
| Log-rank (Mantel–Cox) | 0.091 | 1 | 0.762 NS |
| OD Complications and Maintenance | ||
|---|---|---|
| OD relining | ||
| 3-MDI group | 4-MDI group | |
| 1st year | 1 | 1 |
| 3rd year | 1 | 1 |
| 5th year | 4 | 3 |
| Metal housing loosening from acrylic resin | ||
| 3-MDI group | 4-MDI group | |
| 1st year | 1 | 2 |
| 3rd year | 2 | 1 |
| 5th year | 2 | 3 |
| Retentive elements change | ||
| 3-MDI group | 4-MDI group | |
| 1st year | 7 | 3 |
| 3rd year | 34 | 24 |
| 5th year | 30 | 24 |
| Artificial tooth detachment or fracture | ||
| 3-MDI group | 4-MDI group | |
| 1st year | 1 | 1 |
| 3rd year | 0 | 1 |
| 5th year | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Celebic, A.; Kovacic, I.; Petricevic, N.; Alhajj, M.N.; Topic, J.; Junakovic, L.; Persic-Kirsic, S. Clinical Outcomes of Three versus Four Mini-Implants Retaining Mandibular Overdenture: A 5-Year Randomized Clinical Trial. Medicina 2024, 60, 17. https://doi.org/10.3390/medicina60010017
Celebic A, Kovacic I, Petricevic N, Alhajj MN, Topic J, Junakovic L, Persic-Kirsic S. Clinical Outcomes of Three versus Four Mini-Implants Retaining Mandibular Overdenture: A 5-Year Randomized Clinical Trial. Medicina. 2024; 60(1):17. https://doi.org/10.3390/medicina60010017
Chicago/Turabian StyleCelebic, Asja, Ines Kovacic, Nikola Petricevic, Mohammed Nasser Alhajj, Jolanda Topic, Luka Junakovic, and Sanja Persic-Kirsic. 2024. "Clinical Outcomes of Three versus Four Mini-Implants Retaining Mandibular Overdenture: A 5-Year Randomized Clinical Trial" Medicina 60, no. 1: 17. https://doi.org/10.3390/medicina60010017