
Ruptured Ovarian Cystic Teratoma: A Rare Diagnosis, Easily to Be Confused with Peritoneal Carcinomatosis

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
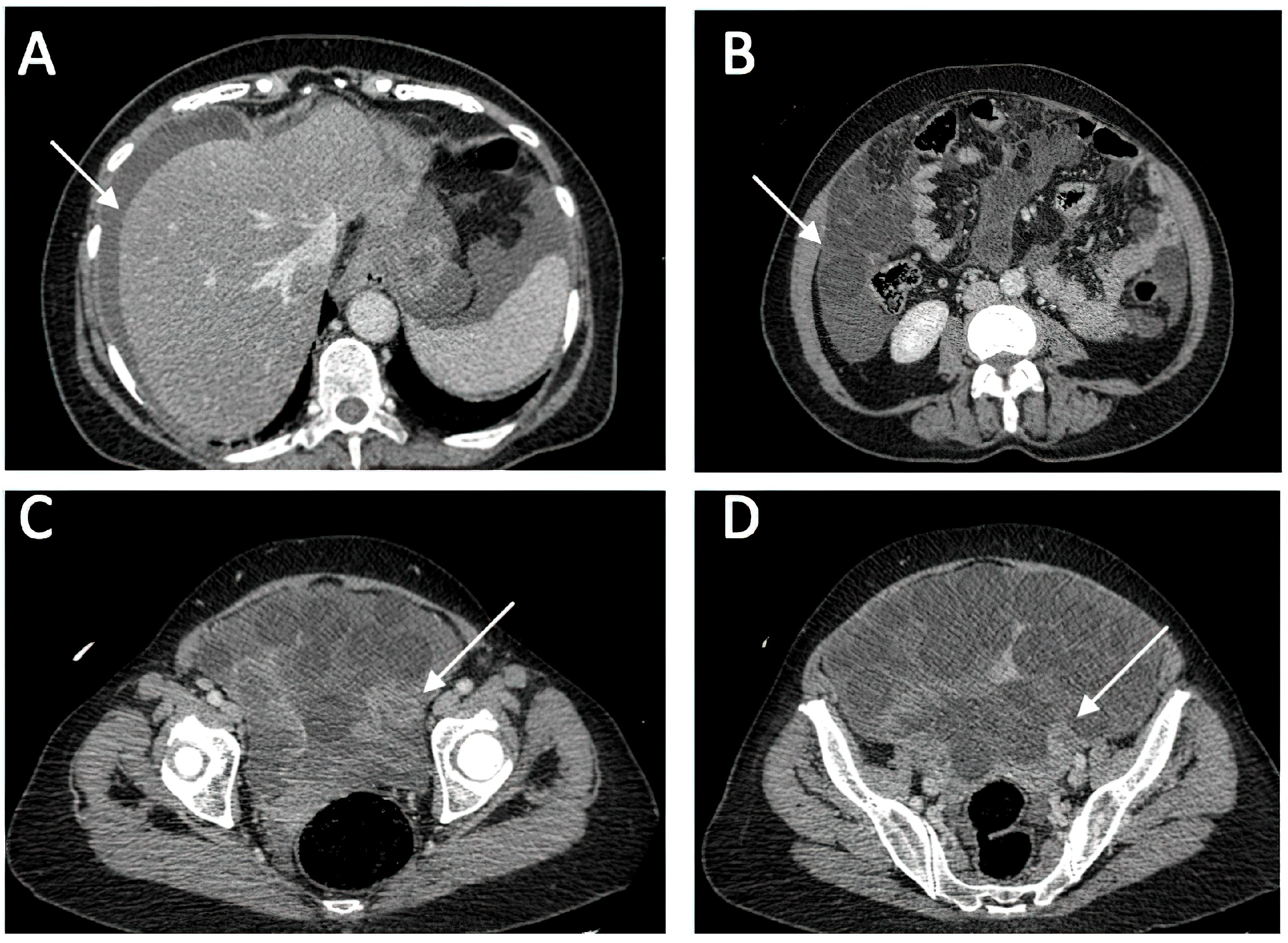
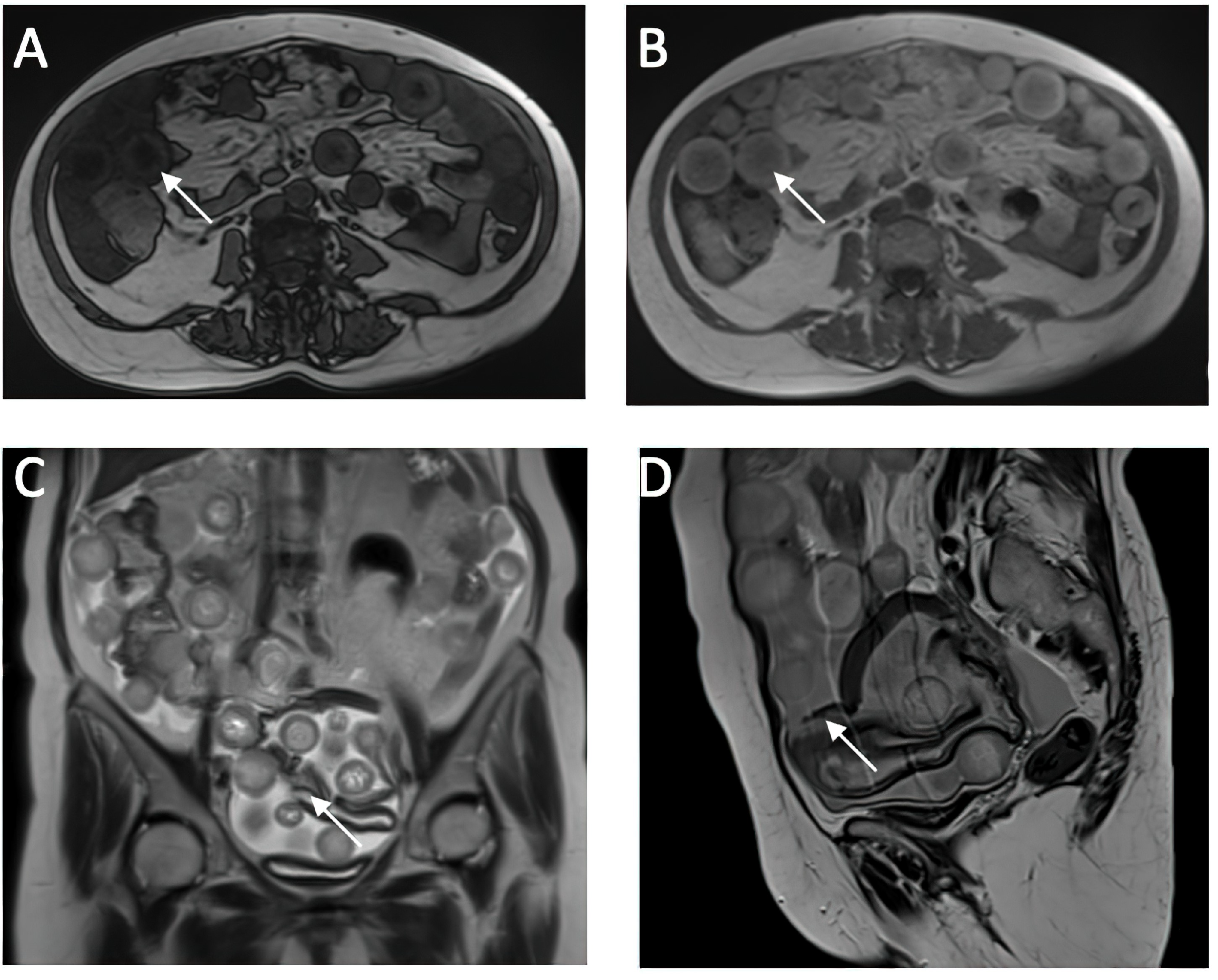
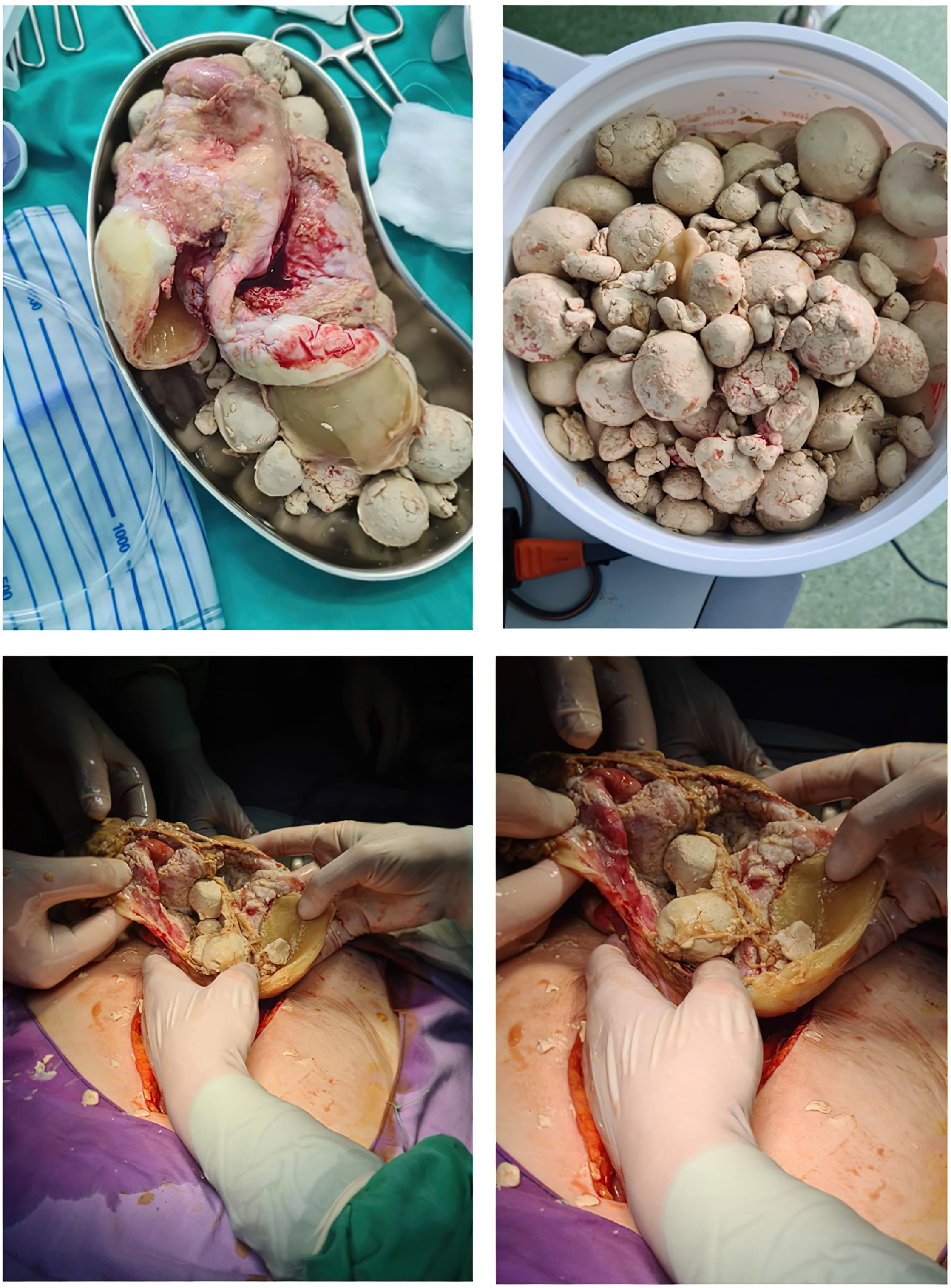
3. Case Presentation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gaillard, F. Mature Cystic Ovarian Teratoma. Available online: https://radiopaedia.org/articles/mature-cystic-ovarian-teratoma-1?lang=us (accessed on 12 January 2024).
- Weerakkody, Y. Struma Ovarii Tumor. Available online: https://radiopaedia.org/articles/struma-ovarii-tumour?lang=us (accessed on 12 January 2024).
- Şahin, H.; Akdoğan, A.I.; Ayaz, D.; Karadeniz, T.; Sancı, M. Utility of the “floating ball sign” in diagnosis of ovarian cystic teratoma. Turk. J. Obstet. Gynecol. 2019, 16, 118–123. [Google Scholar] [CrossRef]
- Muramatsu, Y.; Moriyama, N.; Takayasu, K.; Nawano, S.; Yamada, T. CT and MR imaging of cystic ovarian teratoma with intracystic fat balls. J. Comput. Assist. Tomogr. 1991, 15, 528–529. [Google Scholar]
- Otigbah, C.; Thompson, M.O.; Lowe, D.G.; Setchell, M. Mobile globules in benign cystic teratoma of the ovary. BJOG Int. J. Obstet. Gynaecol. 2000, 107, 135–138. [Google Scholar] [CrossRef]
- Rao, J.R.; Shah, Z.; Patwardhan, V.; Hanchate, V.; Thakkar, H.; Garg, A. Ovarian cystic teratoma: Determined phenotypic response of keratocytes and uncommon intracystic floating balls appearance on sonography and computed tomography. J. Ultrasound Med. 2002, 21, 687–691. [Google Scholar] [CrossRef]
- MR and Ultrasound Imaging of Floating Globules in Mature Ovarian Cystic Teratoma. Gynecol. Obstet. Investig. 2004, 58, 130–132. [CrossRef] [PubMed]
- Fujitoh, H.; Akiyosi, S.; Takoda, S.; Katsuki, K.; Okuda, K. Hepatobiliary and pancreatic imaging. Retroperitoneal mature cystic teratoma with a fat ball. J. Gastroenterol. Hepatol. 1998, 13, 540–549. [Google Scholar] [PubMed]
- Hession, P.R.; Simpson, W. Mobile fatty globules in benign cystic teratoma of the mediastinum. Br. J. Radiol. 1996, 69, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Kawamoto, S.; Sato, K.; Matsumoto, H.; Togo, Y.; Ueda, Y.; Tanaka, J.; Heshiki, A. Multiple Mobile Spherules in Mature Cystic Teratoma of the Ovary. Am. J. Roentgenol. 2001, 176, 1455–1457. [Google Scholar] [CrossRef] [PubMed]
- Donnadieu, A.C.; Deffieux, X.; Ray, C.L.; Mordefroid, M.; Frydman, R.; Fernandez, H. Unusual fast-growing ovarian cystic teratoma during pregnancy presenting with intracystic fat “floating balls” appearance. Fertil. Steril. 2006, 86, 1758–1759. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.D.; Feldstein, V.A.; Lipson, S.D.; Chen, D.C.; Filly, R.A. Cystic teratomas of the ovary: Diagnostic value of sonography. Am. J. Roentgenol. 1998, 171, 1061–1065. [Google Scholar] [CrossRef] [PubMed]
- Ovarian Teratomas: Tumor Types and Imaging Characteristics. Radiographics 2001, 21, 475–490. [CrossRef]
- Zeng, J.; Starost, M.F.; Mauda-Havakuk, M.; Mikhail, A.S.; Partanen, A.; Wood, B.J.; Karanian, J.W.; Pritchard, W.F. Ovarian teratoma in a woodchuck (Marmota monax) with hepatocellular carcinoma: Radiologic and pathologic features. BMC Vet. Res. 2020, 16, 451. [Google Scholar] [CrossRef]
- Pai, S.A. A Hairbrained Mature Cystic Ovarian Teratoma: With Bone Marrow, Meninges, and Intraglial Hair. Int. J. Surg. Pathol. 2021, 29, 404–405. [Google Scholar] [CrossRef]
- Ghasemian Dizajmehr, S.; Mohammadi Irvanlou, M.; Mohammadi, A.; Rashidi Fakari, F. Impact of Serum CA19-9 Level in Clinico-Pathological and Radiologic Feature of Mature Cystic Teratoma: A Case Series. J. Obstet. Gynecol. Cancer Res. 2023, 8, 294–299. [Google Scholar] [CrossRef]
- Han, N.Y.; Sung, D.J.; Park, B.J.; Kim, M.J.; Cho, S.B.; Kim, K.A.; Song, J.Y. Imaging Features of Growing Teratoma Syndrome Following a Malignant Ovarian Germ Cell Tumor. J. Comput. Assist. Tomogr. 2014, 38, 551. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M.D.; Navarrete, S.V.; Pena, R.J.; Leon, M.C.E. Primary ovarian carcinoid tumor arising within a mature cystic teratoma in a 32-years-old patient. Gynecol. Reprod. Endocrinol. 2018, 2, 2–4. [Google Scholar] [CrossRef]
- Guerriero, S.; Alcazar, J.L.; Pascual, M.A.; Ajossa, S.; Gerada, M.; Bargellini, R.; Virgilio, B.; Melis, G.B. Diagnosis of the Most Frequent Benign Ovarian Cysts: Is Ultrasonography Accurate and Reproducible? J. Women’s Health 2009, 18, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Reginelli, A.; Giacobbe, G.; Del Canto, M.T.; Alessandrella, M.; Balestrucci, G.; Urraro, F.; Russo, G.M.; Gallo, L.; Danti, G.; Frittoli, B.; et al. Peritoneal Carcinosis: What the Radiologist Needs to Know. Diagnostics 2023, 13, 1974. [Google Scholar] [CrossRef] [PubMed]
- Lai, P.F.; Hsieh, S.C.; Chien, J.C.W.; Fang, C.L.; Chan, W.P.; Yu, C. Malignant transformation of an ovarian mature cystic teratoma: Computed tomography findings. Arch. Gynecol. Obstet. 2005, 271, 355–357. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.W.; Chan, C.Y.; Lim, K.E.; Chang, H.C. Ruptured Ovarian Cystic Teratoma with Peritoneal Reaction: A Case Report. J. Radiol. Sci. 2015, 40, 61–64. [Google Scholar]
- Ruptured ovarian teratoma with granulomatous peritonitis. Hong Kong Med. J. 2019, 25, e1–e2.
- Kishore, R.; Lambodari, P.; Verma, K.; Khan, A.; Singh, N. A huge mesenteric teratoma in reproductive age woman: A case report. Int. J. Reprod. Contracept. Obstet. Gynecol. 2021, 10, 4590–4592. [Google Scholar] [CrossRef]
- Kim, N.R.; Ha, S.Y.; Shin, J.W.; Lim, S.; Park, C.Y.; Cho, H.Y. Primary ovarian mixed strumal and mucinous carcinoid arising in an ovarian mature cystic teratoma. J. Obstet. Gynaecol. Res. 2016, 42, 211–216. [Google Scholar] [CrossRef]
- Skaane, P.; Huebener, K.H. Computed Tomography of Cystic Ovarian Teratomas with Gravity-Dependent Layering. J. Comput. Assist. Tomogr. 1983, 7, 837. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.H.; Kim, S.S. Peritoneal Carcinomatosis and Its Mimics: Review of CT Findings for Differential Diagnosis. J. Belg. Soc. Radiol. 2020, 104, 8. [Google Scholar] [CrossRef]
- Gagliardi, T.; Adejolu, M.; deSouza, N.M. Diffusion-Weighted Magnetic Resonance Imaging in Ovarian Cancer: Exploiting Strengths and Understanding Limitations. J. Clin. Med. 2022, 11, 1524. [Google Scholar] [CrossRef]
- Ferenc, T.; Popić, J.; Vidjak, V. Magnetic resonance imaging in the diagnosis of malignant gynaecological tumours. Med. Flum. 2022, 58, 100–112. [Google Scholar] [CrossRef] [PubMed]
- Gaillard, F. Peritoneal Metastases. Available online: https://radiopaedia.org/articles/peritoneal-metastases?lang=us (accessed on 15 January 2024). [CrossRef]
- Low, R.N.; Gurney, J. Diffusion-weighted MRI (DWI) in the oncology patient: Value of breathhold DWI compared to unenhanced and gadolinium-enhanced MRI. J. Magn. Reson. Imaging 2007, 25, 848–858. [Google Scholar] [CrossRef]
- Bicchetti, M.; Simone, G.; Giannarini, G.; Girometti, R.; Briganti, A.; Brunocilla, E.; Cardone, G.; De Cobelli, F.; Gaudiano, C.; Del Giudice, F.; et al. A novel pathway to detect muscle-invasive bladder cancer based on integrated clinical features and VI-RADS score on MRI: Results of a prospective multicenter study. La Radiol. Med. 2022, 127, 881–890. [Google Scholar] [CrossRef]
- Cipollari, S.; Pecoraro, M.; Forookhi, A.; Laschena, L.; Bicchetti, M.; Messina, E.; Lucciola, S.; Catalano, C.; Panebianco, V. Biparametric prostate MRI: Impact of a deep learning-based software and of quantitative ADC values on the inter-reader agreement of experienced and inexperienced readers. La Radiol. Med. 2022, 127, 1245–1253. [Google Scholar] [CrossRef] [PubMed]
- Pfannenberg, C.; Schwenzer, N.F.; Bruecher, B.L. State-of-the-art imaging of peritoneal carcinomatosis. RoFo 2012, 184, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Rathod, K.; Kale, H.; Narlawar, R.; Hardikar, J.; Kulkarni, V.; Joseph, J. Unusual “floating balls” appearance of an ovarian cystic teratoma: Sonographic and CT findings. J. Clin. Ultrasound 2001, 29, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.Y.; Sun, D.C.; Ohliger, M.A.; Abuzahriyeh, T.; Choi, H.H. Boba sign: A novel sign for floating balls within a mature cystic teratoma. Abdom. Radiol. 2020, 45, 2931–2933. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Laboratory Test | Conventional Units | Value | Reference Range Value |
|---|---|---|---|
| WBC (White Blood Cells) | L | 8.2 | 4–9.5 |
| Erythrocytes | L | 4.49 | 4–5.5 |
| Hemoglobin | g/dL | 13.12 | 11.5–15 |
| Thrombocytes | L | 252 | 150–400 |
| Creatinine | g/dL | 0.8 | 0.7–1.2 |
| Blood Glucose | g/dL | 106 | 75–110 |
| ALT (Alanine Aminotransferase) | U/L | 24 | 0–35 |
| AST (Aspartate Aminotransferase) | U/L | 24 | 14–36 |
| Imaging Technique | Ovarian Teratoma Findings | Peritoneal Carcinomatosis Findings |
|---|---|---|
| Ultrasound (USG) |
|
|
| Computed Tomography (CT) |
|
|
| Magnetic Resonance Imaging (MRI) |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costachescu, D.; Motofelea, A.C.; Malita, D.; Birsasteanu, F.; Ionita, I.; Motofelea, N.; Jura, C.A.-M.; Bacila, I.-F.; Bacila, M.; Motoi, S. Ruptured Ovarian Cystic Teratoma: A Rare Diagnosis, Easily to Be Confused with Peritoneal Carcinomatosis. Medicina 2024, 60, 460. https://doi.org/10.3390/medicina60030460
Costachescu D, Motofelea AC, Malita D, Birsasteanu F, Ionita I, Motofelea N, Jura CA-M, Bacila I-F, Bacila M, Motoi S. Ruptured Ovarian Cystic Teratoma: A Rare Diagnosis, Easily to Be Confused with Peritoneal Carcinomatosis. Medicina. 2024; 60(3):460. https://doi.org/10.3390/medicina60030460
Chicago/Turabian StyleCostachescu, Dan, Alexandru Catalin Motofelea, Daniel Malita, Florica Birsasteanu, Ioana Ionita, Nadica Motofelea, Cristina Ana-Maria Jura, Ioana-Flavia Bacila, Mihai Bacila, and Sorin Motoi. 2024. "Ruptured Ovarian Cystic Teratoma: A Rare Diagnosis, Easily to Be Confused with Peritoneal Carcinomatosis" Medicina 60, no. 3: 460. https://doi.org/10.3390/medicina60030460
APA StyleCostachescu, D., Motofelea, A. C., Malita, D., Birsasteanu, F., Ionita, I., Motofelea, N., Jura, C. A.-M., Bacila, I.-F., Bacila, M., & Motoi, S. (2024). Ruptured Ovarian Cystic Teratoma: A Rare Diagnosis, Easily to Be Confused with Peritoneal Carcinomatosis. Medicina, 60(3), 460. https://doi.org/10.3390/medicina60030460