
Cutaneous Calcified Mass of Foot in Pseudohypoparathyoidism: Case Report


Abstract
1. Introduction
2. Case Presentation
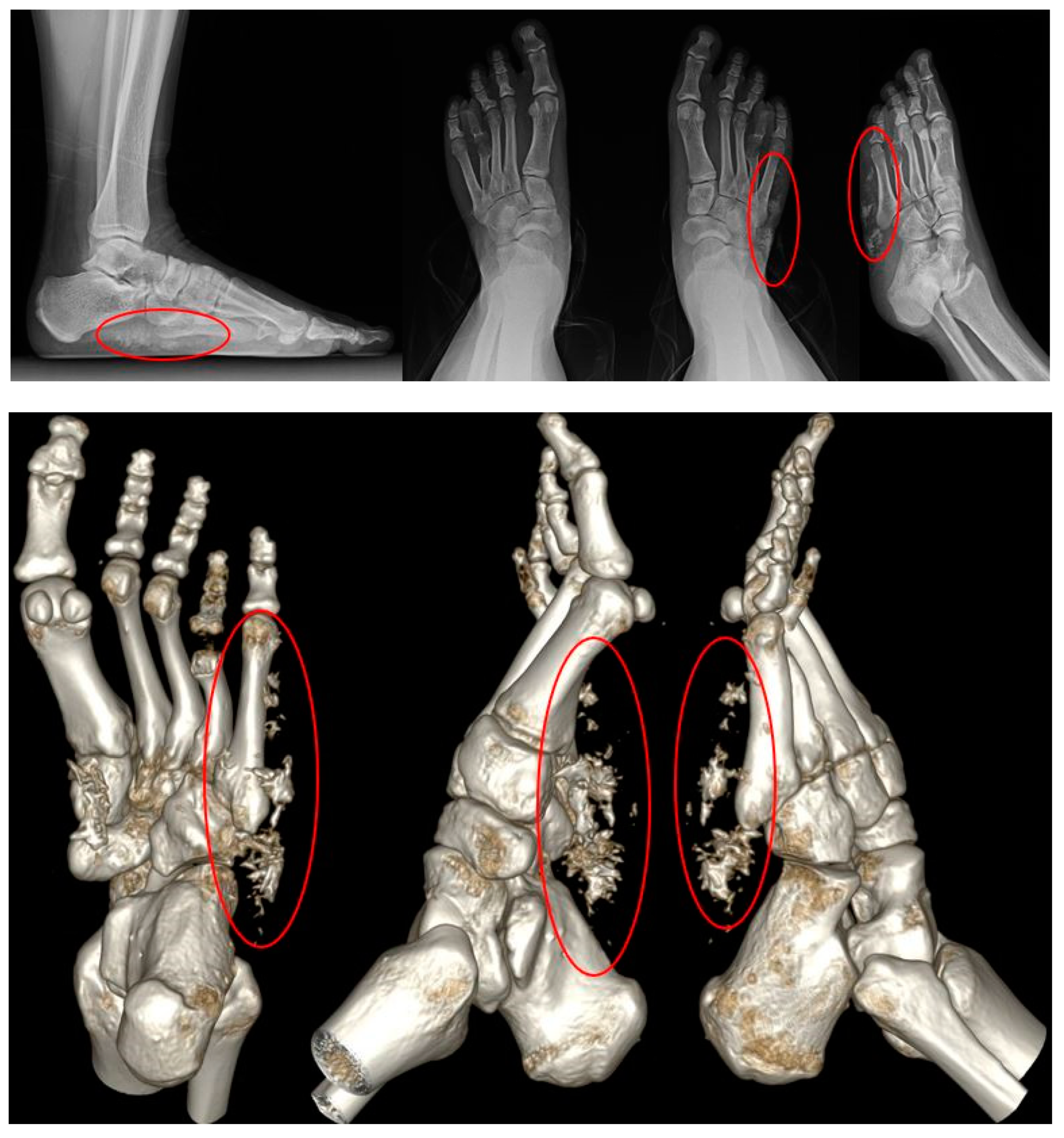
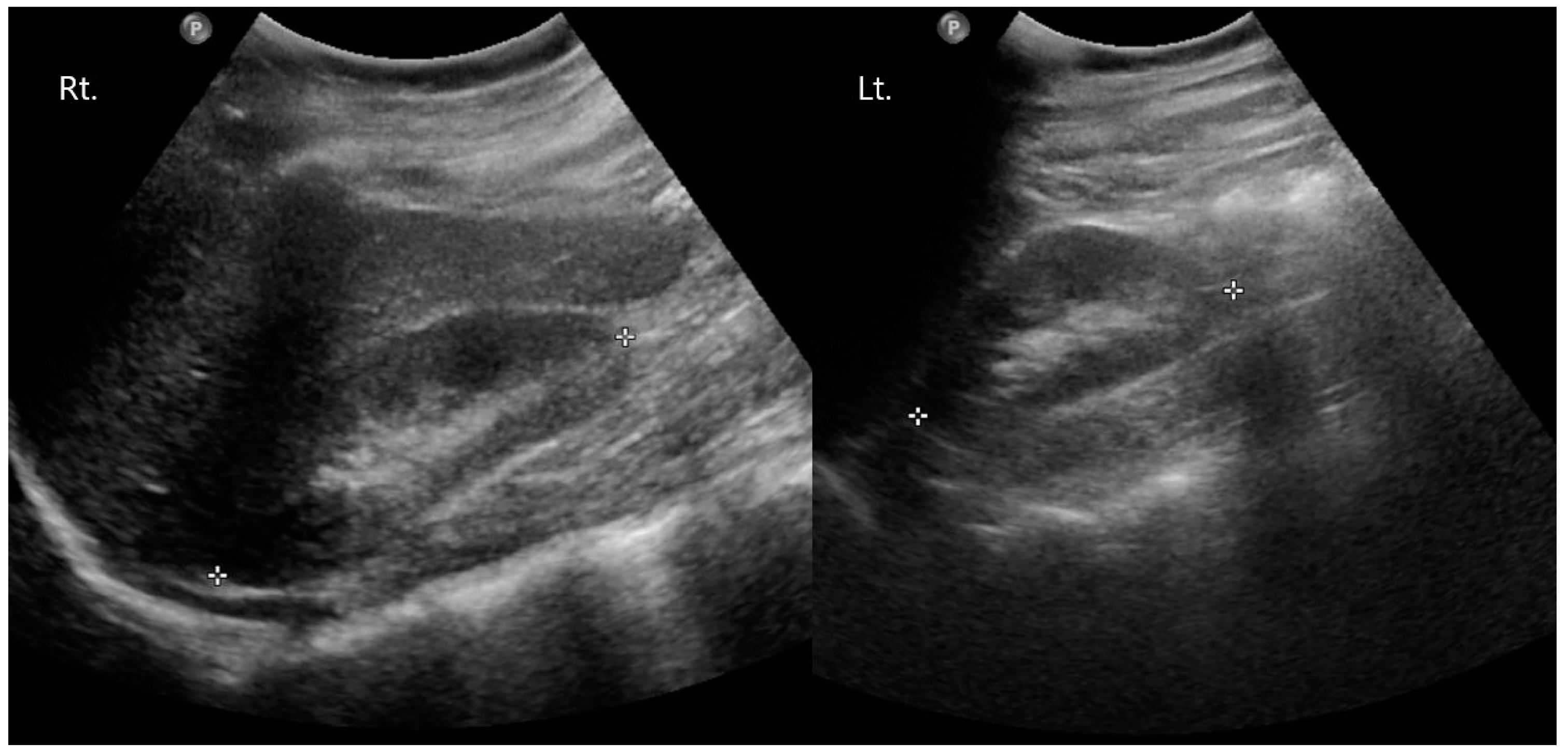
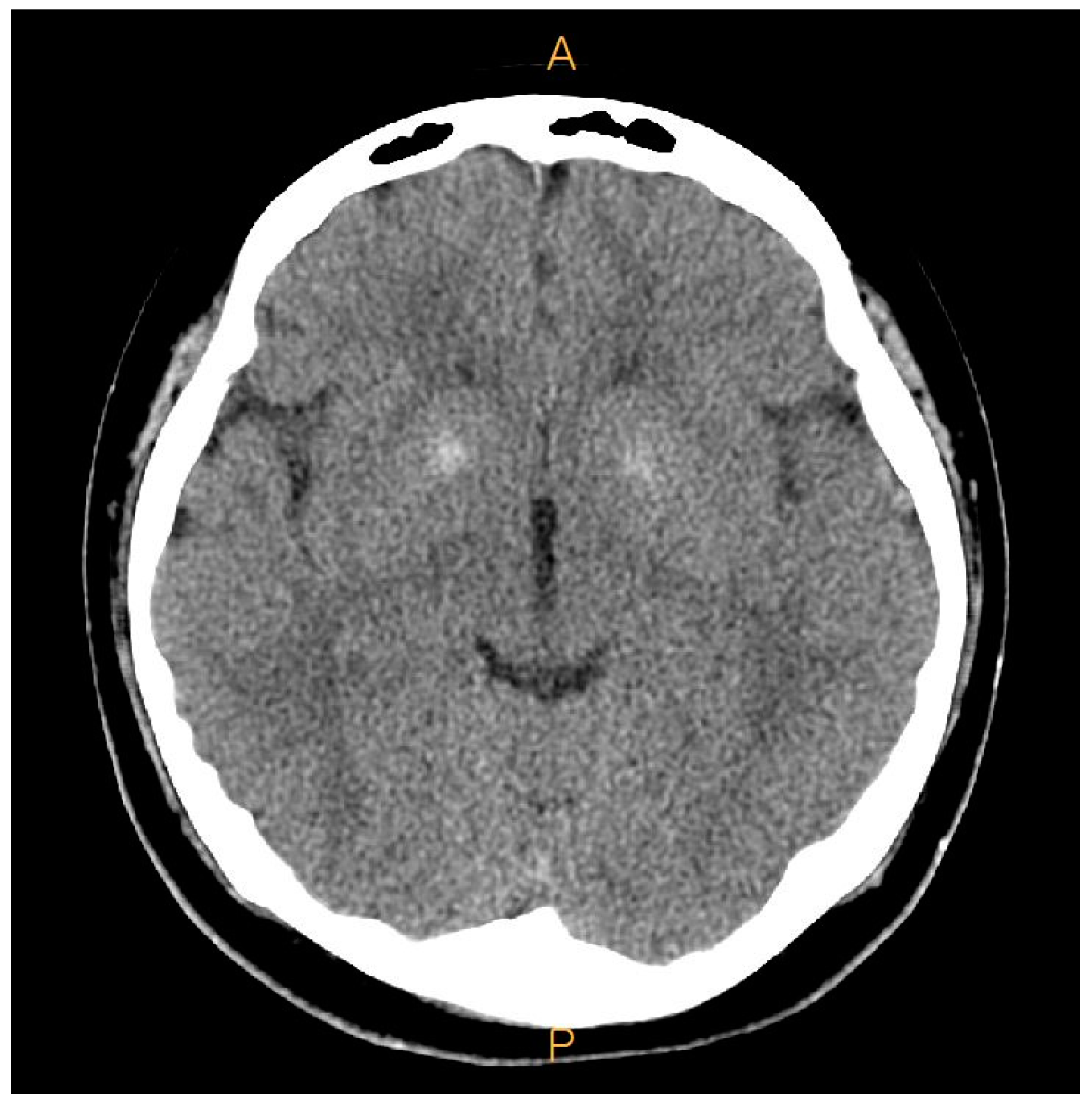
2.1. Preoperative Evaluation
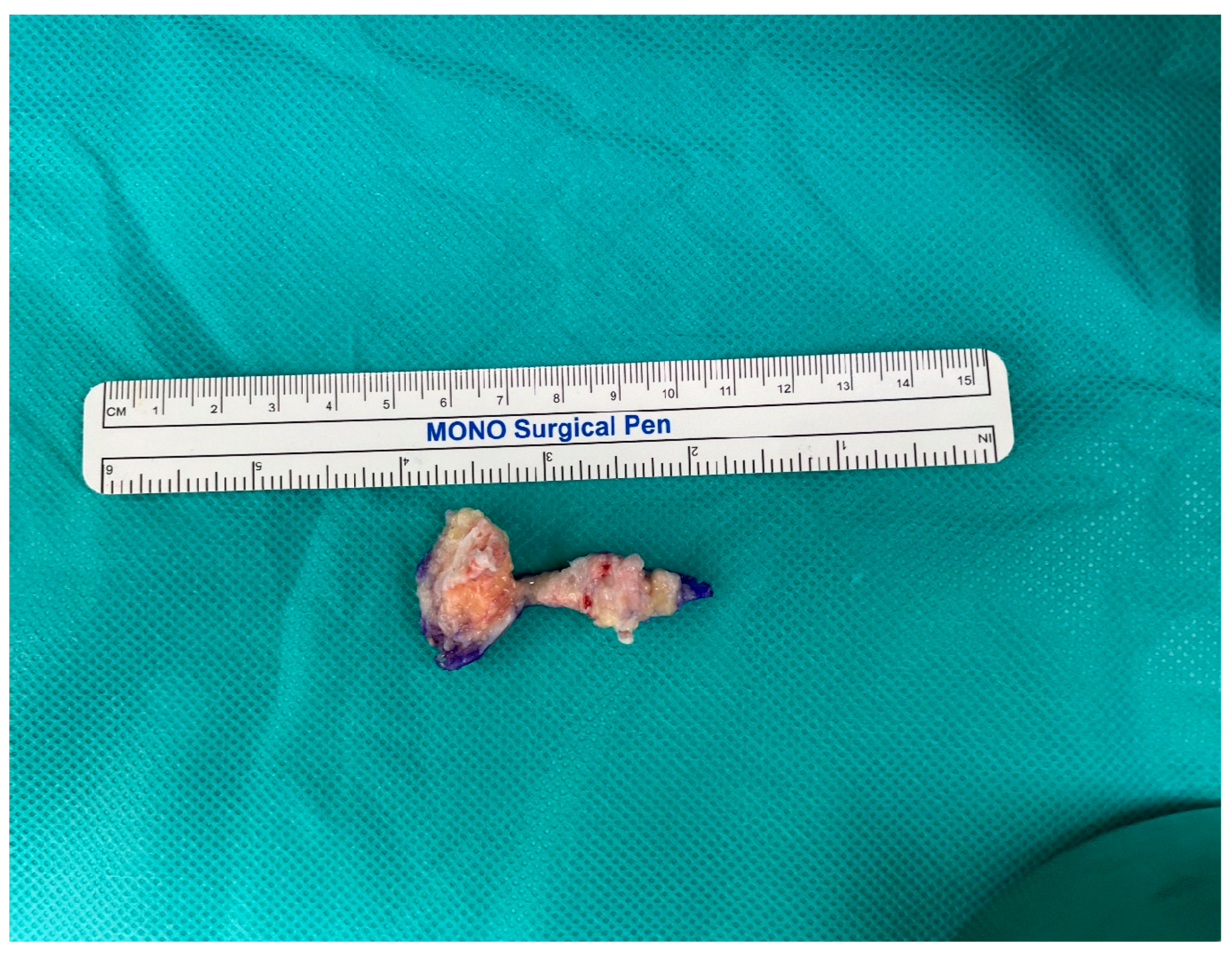
2.2. Surgical Procedure
2.3. Postoperative Care
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lofrese, J.J.; Basit, H.; Lappin, S.L. Physiology, parathyroid. In StatPearls [Internet]; StatPearls Publishing: St. Petersburg, FL, USA, 2022. [Google Scholar]
- Jeong, K.-H.; Lew, B.-L.; Sim, W.-Y. Osteoma cutis as the presenting feature of Albright hereditary osteodystrophy associated with pseudopseudohypoparathyroidism. Ann. Dermatol. 2009, 21, 154. [Google Scholar] [CrossRef] [PubMed]
- Adegbite, N.; Xu, M.; Kaplan, F.; Shore, E.; Pignolo, R. Diagnostic and mutational spectrum of progressive osseous heteroplasia (POH) and other forms of GNAS-based heterotopic ossification. Am. J. Med. Genet. Part A 2008, 146, 1788–1796. [Google Scholar] [CrossRef] [PubMed]
- Freire, V.; Moser, T.P.; Lepage-Saucier, M. Radiological identification and analysis of soft tissue musculoskeletal calcifications. Insights Imaging 2018, 9, 477–492. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Liu, L.; Rosen, C.J. PTH and the Regulation of Mesenchymal Cells within the Bone Marrow Niche. Cells 2024, 13, 406. [Google Scholar] [CrossRef] [PubMed]
- Ward, S.; Sugo, E.; Verge, C.F.; Wargon, O. Three cases of osteoma cutis occurring in infancy. A brief overview of osteoma cutis and its association with pseudo-pseudohypoparathyroidism. Australas. J. Dermatol. 2011, 52, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Pignolo, R.J.; Ramaswamy, G.; Fong, J.T.; Shore, E.M.; Kaplan, F.S. Progressive osseous heteroplasia: Diagnosis, treatment, and prognosis. Appl. Clin. Genet. 2015, 8, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Banks, K.P.; Bui-Mansfield, L.T.; Chew, F.S.; Collinson, F. A compartmental approach to the radiographic evaluation of soft-tissue calcifications. In Seminars in Roentgenology; Elsevier: Amsterdam, The Netherlands, 2005; pp. 391–407. [Google Scholar]
- Goltzman, D. Physiology of parathyroid hormone. Endocrinol. Metab. Clin. 2018, 47, 743–758. [Google Scholar] [CrossRef]
- Leung, E.K.Y. Parathyroid hormone. In Advances in Clinical Chemistry; Elsevier: Amsterdam, The Netherlands, 2021; pp. 41–93. [Google Scholar]
- Esbrit, P.; Alcaraz, M.J. Current perspectives on parathyroid hormone (PTH) and PTH-related protein (PTHrP) as bone anabolic therapies. Biochem. Pharmacol. 2013, 85, 1417–1423. [Google Scholar] [CrossRef]
- Martin, T.J. PTH1R actions on bone using the cAMP/protein kinase a pathway. Front. Endocrinol. 2022, 12, 833221. [Google Scholar] [CrossRef]
- Kužma, M.; Jackuliak, P.; Killinger, Z.; Payer, J. Parathyroid hormone-related changes of bone structure. Physiol. Res. 2021, 70, S3. [Google Scholar] [CrossRef]
- Clarke, B.L. Bone disease in hypoparathyroidism. Arq. Bras. De Endocrinol. Metabol. 2014, 58, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Sikjaer, T.; Rejnmark, L.; Thomsen, J.S.; Tietze, A.; Brüel, A.; Andersen, G.; Mosekilde, L. Changes in 3-dimensional bone structure indices in hypoparathyroid patients treated with PTH (1-84): A randomized controlled study. J. Bone Miner. Res. 2012, 27, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Albright, F. Pseudohypoparathyroidism: An example of “Seabright-Bantam syndrome”. Endocrinology 1942, 30, 922–932. [Google Scholar]
- Song, C.-Y.; Zhao, Z.-X.; Li, W.; Sun, C.-C.; Liu, Y.-M. Pseudohypoparathyroidism with basal ganglia calcification: A case report of rare cause of reversible parkinsonism. Medicine 2017, 96, e6312. [Google Scholar] [CrossRef] [PubMed]
- Limaiem, F.; Sergent, S.R. Osteoma cutis. In StatPearls [Internet]; StatPearls Publishing: St. Petersburg, FL, USA, 2023. [Google Scholar]
- Potts, J.T. Parathyroid hormone: Past and present. J. Endocrinol. 2005, 187, 311–325. [Google Scholar] [CrossRef] [PubMed]
- Gensure, R.C.; Gardella, T.J.; Jüppner, H. Parathyroid hormone and parathyroid hormone-related peptide, and their receptors. Biochem. Biophys. Res. Commun. 2005, 328, 666–678. [Google Scholar] [CrossRef] [PubMed]
- Fazeli, P.; Harvell, J.; Jacobs, M.B. Osteoma cutis (cutaneous ossification). West. J. Med. 1999, 171, 243. [Google Scholar]
- Alsaffar, H.; Attia, N.; Senniappan, S. Subcutaneous calcification and fixed flexion deformity of the right elbow joint in a child with a GNAS mutation: A case report. Int. J. Endocrinol. Metab. 2021, 19, e110792. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, G. Pseudohypoparathyroidism: Diagnosis and treatment. J. Clin. Endocrinol. Metab. 2011, 96, 3020–3030. [Google Scholar] [CrossRef]
- Tamada, Y.; Kanda, S.; Suzuki, H.; Tajima, T.; Nishiyama, T. A pseudohypoparathyroidism type Ia patient with normocalcemia. Endocr. J. 2008, 55, 169–173. [Google Scholar] [CrossRef]
- Farfel, Z. FRIEDMANE Mental deficiency in pseudohypoparathyroidism type I is associated with Ns-protein deficiency. Ann. Intern. Med. 1986, 105, 197–199. [Google Scholar] [CrossRef] [PubMed]
- Garavelli, L.; Pedori, S.; Zanacca, C.; Caselli, G.; Loiodice, A.; Mantovani, G.; Ammenti, A.; Virdis, R.; Banchini, G. Albright’s hereditary osteodystrophy (pseudohypoparathyroidism type Ia): Clinical case with a novel mutation of GNAS1. Acta Biomed. 2005, 76, 45–48. [Google Scholar] [PubMed]
- Albujar, P.; Hunter, R.; Dayan, A. The brain in pseudohypoparathyroidism. Rev. De Neuro-Psiquiatr. 2003, 66, 129–133. [Google Scholar] [CrossRef]
- Faria LLd Babler, F.; Ferreira, L.C.; Noronha Junior OAd Marsolla, F.L.; Ferreira, D.L. Soft tissue calcifications: A pictorial essay. Radiol. Bras. 2020, 53, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Laasri, K.; Halfi, I.M.; Nassar, I.; Billah, N.M. A rare case of idiopathic tumoral calcinosis: Case report. Radiol. Case Rep. 2022, 17, 4350–4353. [Google Scholar] [CrossRef]
- Snarskaya, E.S.; Teplyuk, N.P.; Vasileva, K.D.; Vertieva, E.Y. What do we know about osteoma cutis? Literature review. Clinical cases. Russ. J. Ski. Vener. Dis. 2021, 24, 133–144. [Google Scholar] [CrossRef]
- Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Rodriguez-Sanz, D. Static and dynamic plantar pressures in children with and without sever disease: A case-control study. Phys. Ther. 2014, 94, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.; Dalbeth, N.; Vandal, A.C.; Rome, K. Spatiotemporal gait parameters and plantar pressure distribution during barefoot walking in people with gout and asymptomatic hyperuricemia: Comparison with healthy individuals with normal serum urate concentrations. J. Foot Ankle Res. 2016, 9, 15. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.; Dalbeth, N.; McNair, P.; Parmar, P.; Gow, P.; Rome, K. The effect of good and poor walking shoe characteristics on plantar pressure and gait in people with gout. Clin. Biomech. 2014, 29, 1158–1163. [Google Scholar] [CrossRef]
- Wang, X.L. Osteoma cutis in pseudohypoparathyroidism type 1A. QJM Int. J. Med. 2024; corrected proof. [Google Scholar] [CrossRef]
- Sethuraman, G.; Malhotra, A.K.; Khaitan, B.K.; Kumar, R.; Sharma, V.K.; Kabra, M.; Singh, M.K. Osteoma cutis in pseudohypoparathyroidism. Clin. Exp. Dermatol. 2006, 31, 225–227. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Preop | POD 6m | POD 1yr |
|---|---|---|---|
| AOFAS | 40 | 90 | 100 |
| VAS | 7 | 2 | 0 |
| FAOS | 136 | 62 | 42 |
| Study | This Case | X.L. Wang [32] | G. Sethuraman et al. [33] | Ki-Heon Jeong et al. [2] |
|---|---|---|---|---|
| Sex/Age (years) | F/15 | M/16 | M/7 | F/11 |
| Location | Lat. side of Lt. foot | Lat. side of Lt. 2nd & 3rd finger | Abdomen & extremities | Rt. palm, Lt. 5th finger, Lt. sole |
| Symptom | Lt. foot pain | Lt. finger pain | Asymptomatic | Rt. palm pain, Lt. finger pain, Lt. foot pain |
| Associated condition | PHP type 1A | PHP type 1A | PHP type 1A | PPHP |
| Genetic abnormalitiy | Heterozygous insertion of exon 5 | Heterozygous deletion of exon 2 | - | - |
| Brain lesion | O | O | - | - |
| Surgical removal | O | O | - | - |
| Histologic finding | Osteoma cutis | - | Osteoma cutis | Osteoma cutis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.H.; Kim, S.H.; Choi, S.J.; Lee, Y.K. Cutaneous Calcified Mass of Foot in Pseudohypoparathyoidism: Case Report. Medicina 2024, 60, 595. https://doi.org/10.3390/medicina60040595
Lee SH, Kim SH, Choi SJ, Lee YK. Cutaneous Calcified Mass of Foot in Pseudohypoparathyoidism: Case Report. Medicina. 2024; 60(4):595. https://doi.org/10.3390/medicina60040595
Chicago/Turabian StyleLee, Sang Heon, Sung Hwan Kim, Seung Jin Choi, and Young Koo Lee. 2024. "Cutaneous Calcified Mass of Foot in Pseudohypoparathyoidism: Case Report" Medicina 60, no. 4: 595. https://doi.org/10.3390/medicina60040595
APA StyleLee, S. H., Kim, S. H., Choi, S. J., & Lee, Y. K. (2024). Cutaneous Calcified Mass of Foot in Pseudohypoparathyoidism: Case Report. Medicina, 60(4), 595. https://doi.org/10.3390/medicina60040595