
Optimising Percutaneous Coronary Interventions: The Impact of Stent Type and Diameter on Long-Term Clinical Outcomes in Large Coronary Arteries

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
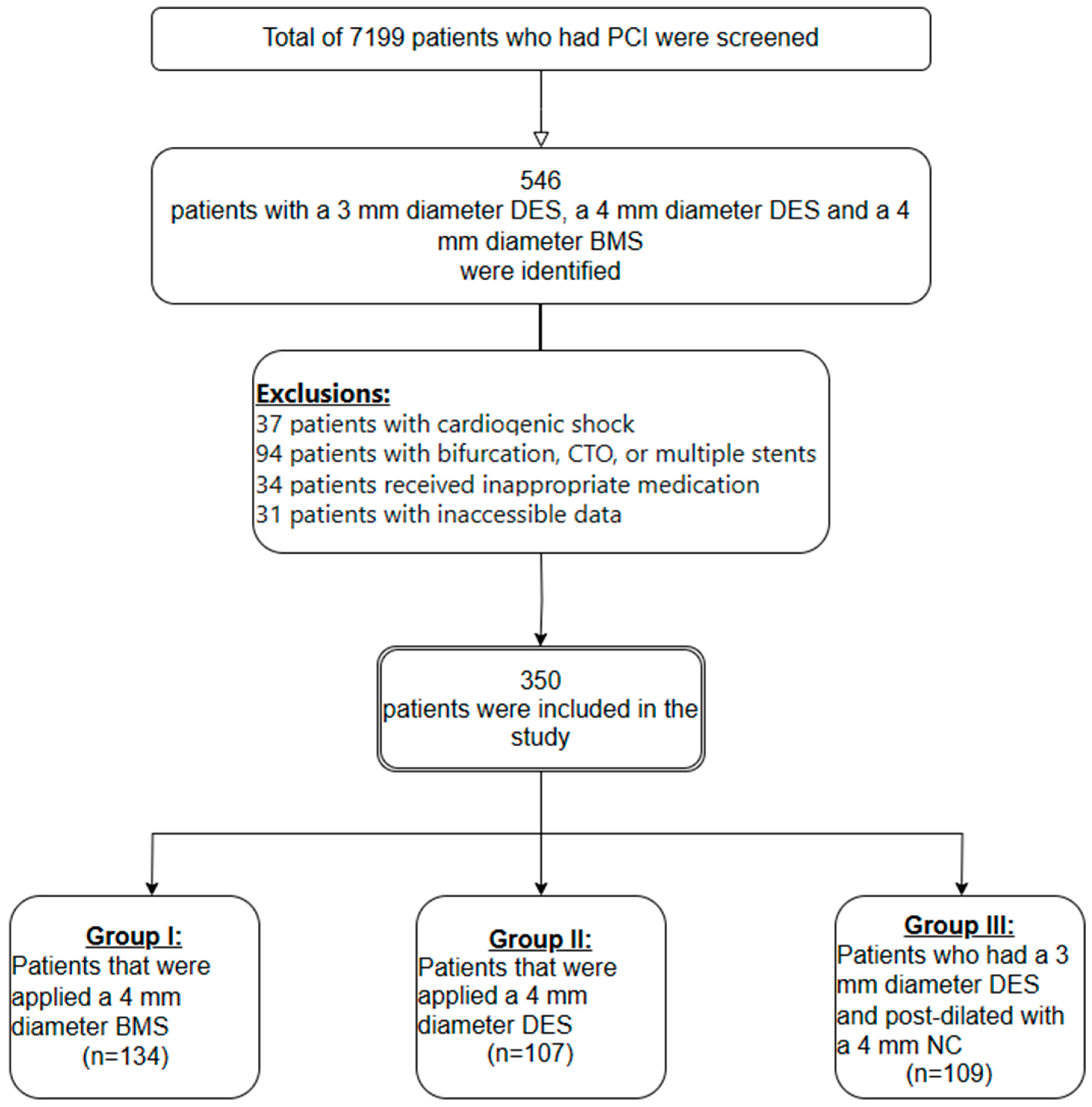
2.1. Study Population
2.2. Angiographic Analysis
2.3. Definitions
2.4. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Zbinden, R.; von Felten, S.; Wein, B.; Tueller, D.; Kurz, D.J.; Reho, I.; Galatius, S.; Alber, H.; Conen, D.; Pfisterer, M.; et al. Impact of stent diameter and length on in-stent restenosis after DES vs. BMS implantation in patients needing large coronary stents-A clinical and health-economic evaluation. Cardiovasc. Ther. 2017, 36, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Ellis, S.G.; Cannon, L.; Mann, J.T.; Greenberg, J.D.; Spriggs, D.; O’Shaughnessy, C.D.; DeMaio, S.; Hall, P.; Popma, J.J.; et al. Comparison of a polymer-based paclitaxel-eluting stent with a bare metal stent in patients with complex coronary artery disease: A randomized controlled trial. JAMA 2005, 294, 1215–1223. [Google Scholar] [CrossRef] [PubMed]
- Stettler, C.; Wandel, S.; Allemann, S.; Kastrati, A.; Morice, M.C.; Schömig, A.; Pfisterer, M.E.; Stone, G.W.; Leon, M.B.; de Lezo, J.S.; et al. Outcomes associated with drug-eluting and bare-metal stents: A collaborative network meta-analysis. Lancet 2007, 370, 937–948. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Clinical Excellence. Drug-Eluting Stents for the Treatment of Coronary Artery Disease NICE Technology Appraisal Guidance [TA152]; National Institute for Clinical Excellence: London, UK, 2008. [Google Scholar]
- Lagerqvist, B.; James, S.K.; Stenestrand, U.; Lindbäck, J.; Nilsson, T.; Wallentin, L. Long-term outcomes with drug-eluting stents versus bare-metal stents in Sweden. N. Engl. J. Med. 2007, 356, 1009–1019. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, C.; Galatius, S.; Erne, P.; Eberli, F.; Alber, H.; Rickli, H.; Pedrazzini, G.; Hornig, B.; Bertel, O.; Bonetti, P.; et al. Drug-eluting versus bare-metal stents in large coronary arteries. N. Engl. J. Med. 2010, 363, 2310–2319. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.T.; Nam, C.W.; Hur, S.H.; Kim, K.B.; Lee, S.H.; Hong, G.R.; Park, J.S.; Kim, Y.J.; Kim, U.; Yang, T.H.; et al. Two-Year Clinical Outcomes After Large Coronary Stent (4.0 mm) Placement: Comparison of Bare-Metal Stent Versus Drug-Eluting Stent. Clin. Cardiol. 2010, 33, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Cox, D.; Hermiller, J.B.; Cannon, L. Are DES beneficial in large vessels compared to BMS? Data from the TAXUS IV and V randomised clinical trials. J. Am. Coll. Cardiol. 2008, 51, B109. [Google Scholar]
- Hsieh, M.-J.; Chen, C.-C.; Chang, S.-H.; Wang, C.-Y.; Lee, C.-H.; Lin, F.-C.; Chang, C.-J.; Hsieh, I.-C. Long-term outcomes of drug-eluting stents versus bare-metal stents in large coronary arteries. Int. J. Cardiol. 2013, 168, 3785–3790. [Google Scholar] [CrossRef] [PubMed]
- De Luca, G.; Dirksen, M.T.; Spaulding, C.; Kelbaek, H.; Schalij, M.; Thuesen, L.; Van Der Hoeven, B.; Vink, M.A.; Kaiser, C.; Musto, C.; et al. Drug-eluting vs bare-metal stents in primary angioplasty: A pooled patient-level meta-analysis of randomised trials. Arch. Intern. Med. 2012, 172, 611–621. [Google Scholar] [CrossRef]
- Bangalore, S.; Kumar, S.; Fusaro, M.; Amoroso, N.; Attubato, M.J.; Feit, F.; Bhatt, D.L.; Slater, J. Short-and long-term outcomes with drug-eluting and bare-metal coronary stents: A mixed-treatment comparison analysis of 117,762 patient-years of follow-up from randomised trials. Circulation 2012, 125, 2873–2891. [Google Scholar] [CrossRef]
- Palmerini, T.; Biondi-Zoccai, G.; Della Riva, D.; Stettler, C.; Sangiorgi, D.; D’Ascenzo, F.; Kimura, T.; Briguori, C.; Sabatè, M.; Kim, H.-S.; et al. Stent thrombosis with drug-eluting and bare-metal stents: Evidence from a comprehensive network meta-analysis. Lancet 2012, 379, 1393–1402. [Google Scholar] [CrossRef] [PubMed]
- Abe, D.; Sato, A.; Hoshi, T.; Maruta, S.; Misaki, M.; Kakefuda, Y.; Watabe, H.; Hiraya, D.; Sakai, S.; Kawabe, M.; et al. Drug-eluting versus bare-metal stents in large coronary arteries of patients with ST-segment elevation myocardial infarction: Findings from the ICAS registry. J. Cardiol. 2014, 64, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, D.H.; Mishra, S.; Javaid, A.; Slottow, T.L.P.; Buch, A.N.; Roy, P.; Okabe, T.; Smith, K.A.; Torguson, R.; Xue, Z.; et al. Comparison of effectiveness of bare metal stents versus drug-eluting stents in large (≥3.5 mm) coronary arteries. Am. J. Cardiol. 2007, 99, 599–602. [Google Scholar] [CrossRef] [PubMed]
- Sabate, M.; Cequier, A.; Iñiguez, A.; Serra, A.; Hernandez-Antolin, R.; Mainar, V.; Valgimigli, M.; Tespili, M.; Heijer, P.D.; Bethencourt, A.; et al. Everolimus-eluting stent versus bare-metal stent in ST-segment elevation myocardial infarction (EXAMINATION): 1-year results of a randomised controlled trial. Lancet 2012, 380, 1482–1490. [Google Scholar] [CrossRef] [PubMed]
- Fokkema, M.L.; James, S.K.; Albertsson, P.; Akerblom, A.; Calais, F.; Eriksson, P.; Jensen, J.; Nilsson, T.; de Smet, B.J.; Sjögren, I.; et al. Population trends in percutaneous coronary intervention: 20-year results from the SCAAR (Swedish Coronary Angiography and Angioplasty Registry). J. Am. Coll. Cardiol. 2013, 61, 1222–1230. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.; Brugaletta, S.; Pernigotti, A.; Flores-Ulmanzor, E.; Ortega-Paz, L.; Cequier, A.; Iniguez, A.; Serra, A.; Jimenez-Quevedo, P.; Mainar, V.; et al. Does Large Vessel Size Justify Use of Bare-Metal Stents in Primary Percutaneous Coronary Intervention? Insights From the EXAMINATION Trial. Circ. Cardiovasc. Interv. 2019, 12, e007705. [Google Scholar] [CrossRef] [PubMed]
- Garg, P.; Normand, S.L.T.; Silbaugh, T.S.; Wolf, R.E.; Zelevinsky, K.; Lovett, A.; Varma, M.R.; Zhou, Z.; Mauri, L. Drug-eluting or bare-metal stenting in patients with diabetes mellitus: Results from the Massachusetts Data Analysis Center Registry. Circulation 2008, 118, 2277–2285. [Google Scholar] [CrossRef] [PubMed]
- Foin, N.; Sen, S.; Allegria, E.; Petraco, R.; Nijjer, S.; Francis, D.P.; Di Mario, C.; Davies, J.E. Maximal expansion capacity with current DES platforms: A critical factor for stent selection in the treatment of left main bifurcations. EuroIntervention 2013, 8, 1315–1325. [Google Scholar] [CrossRef] [PubMed]
- Yin, D.; Li, J.; Yang, Y.J.; Wang, Y.; Zhao, Y.Y.; You, S.J.; Qiao, S.B.; Xu, B.; Dou, K.F. Nine-year clinical outcomes of drug-eluting stents vs. bare metal stents for large coronary vessel lesions. J. Geriatr. Cardiol. 2017, 14, 35–41. [Google Scholar] [PubMed]
- Piccolo, R.; Efthimiou, O.; Varenne, O.; Baldo, A.; Urban, P.; Kaiser, C.; Remkes, W.; Räber, L.; de Belder, A.; van’t Hof, A.W.J.; et al. Drug-eluting or bare-metal stents for percutaneous coronary intervention: A systematic review and individual patient data meta-analysis of randomised clinical trials. Lancet 2019, 393, 2503–2510. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, H.; Okada, K.; Kimura, T.; Yock, P.G.; Lansky, A.J.; Popma, J.J.; Yeung, A.C.; Fitzgerald, P.J.; Honda, Y. Impact of Stent Size Selection on Acute and Long-Term Outcomes After Drug-Eluting Stent Implantation in De Novo Coronary Lesions. Circ. Cardiovasc. Interv. 2017, 10, e004795. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Feng, B.; Zheng, Z.; Li, L.; Zeng, W.; Wang, D.; Zhang, L.; Li, H. Association of stent diameter and target vessel revascularisation in patients undergoing percutaneous coronary intervention: A secondary retrospective analysis based on a Chinese cohort study. BMC Cardiovasc. Disord. 2021, 21, 402. [Google Scholar] [CrossRef] [PubMed]
- Changal, K.H.; Mir, T.; Khan, S.; Nazir, S.; Elzanatey, A.; Meenakshisundaram, C.; Mubbasher, S.; Sheikh, M.A. Drug-Eluting Stents Versus Bare-Metal Stents in Large Coronary Artery Revascularization: Systematic Review and Meta-Analysis. Cardiovasc. Revascularization Med. 2021, 23, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Prajapati, J.; Singhal, R.; Patel, I.; Patel, C.; Sahoo, S. One-Year Clinical Outcomes of Drug-Eluting Stents versus Bare-Metal Stents in Large Coronary Arteries. J. Clin. Prev. Cardiol. 2020, 9, 56–60. [Google Scholar] [CrossRef]


{kind=link}
| Group I (4 mm BMS) (n = 134) Mean ± SD Median (min–max.) | Group II (4 mm DES) (n = 105) Mean ± SD Median (min–max.) | Group III (3 mm DES, 4 mm NC) (n = 104) Mean ± SD Median (min–max.) | p Value | ||
|---|---|---|---|---|---|
| Age (year) | 62 ± 10.8 | 61 ± 10.1 | 62 ± 9.8 | 0.653 | |
| Gender | Men, n (%) | 116 (86.6) | 88 (83.2) | 86 (82.6) | 0.648 |
| Women, n (%) | 18 (13.4) | 17 (16.8) | 18 (17.4) | ||
| Diabetes mellitus, n (%) | 35 (26.1) | 33 (30.8) | 4 (31.2) | 0.617 | |
| Hypertension, n (%) | 69 (51.5) | 54 (50.5) | 51 (46.8) | 0.614 | |
| Cigarette, n (%) | 69 (51.5) | 57 (53.3) | 52 (47.7) | 0.543 | |
| Family history, n (%) | 41 (30.6) | 31 (29) | 25 (22.9) | 0.390 | |
| Previous MI, n (%) | 39 (29.1) | 27 (25.2) | 34 (31.2) | 0.515 | |
| Previous PCI, n (%) | 25 (18.7) | 15 (14) | 28 (25.7) | 0.092 | |
| Previous CABG operation, n (%) | 15 (11.2) | 12 (11.2) | 9 (8.3) | 0.703 | |
| STEMI | 37 (27.61) | 22 (20.56) | 25 (23.85) | 0.444 | |
| NSTEMI | 82 (61.2) | 66 (62.6) | 63 (59.6) | 0.904 | |
| Stable CAD | 15 (11.19) | 17 (16.82) | 16 (16.51) | 0.369 | |
| LDL (mg/dL) | 109 ± 35.5 | 107 ± 45.6 | 112 ± 43.7 | 0.645 | |
| Creatinine (mg/dL) | 1.0 ± 0.3 | 1.1 ± 1.2 | 1.1 ± 1.1 | 0.519 | |
| Haemoglobin (gr/dL) | 13.7 ± 1.9 | 13.7 ± 2.1 | 13.8 ± 1.7 | 0.866 | |
| EF (%) | 50 (25–70) | 53 (23–66) | 54 (30–72) | <0.001 | |
| EF (%) | <%40, n (%) | 20 (15) | 13 (13.1) | 6 (5.5) | 0.058 |
| ≥%40, n (%) | 114 (85) | 92 (86.9) | 98 (94.5) | ||
| Group I (4 mm BMS) (n = 134) Mean ± SD Median (min–max.) | Group II (4 mm DES) (n = 105) Mean ± SD Median (min–max.) | Group III (3 mm DES, 4 mm NC) (n = 104) Mean ± SD Median (min–max.) | p Value | ||
|---|---|---|---|---|---|
| LAD, n (%) | 23 (17.2) | 27 (25.2) | 33 (30.3) | 0.052 | |
| CX, n (%) | 21 (15.7) | 15 (14) | 14 (12.8) | 0.818 | |
| RCA, n (%) | 79 (59) | 49 (45.8) | 55 (50.5) | 0.114 | |
| Saphenous graft, n (%) | 6 (4.5) | 3 (2.8) | 3 (2.7) | 0.697 | |
| Osteal lesion | Yes | 17 (12.7) | 17 (15.9) | 9 (8.3) | 0.229 |
| No | 117 (87.3) | 90 (84.1) | 100 (91.7) | ||
| TIMI 1, n (%) | 5 (3.7) | 2 (1.9) | 3 (2.7) | 0.687 | |
| TIMI 2, n (%) | 10 (7.5) | 5 (4.7) | 8 (7.3) | 0.786 | |
| TIMI 3, n (%) | 119 (88.8) | 100 (93.5) | 98 (89.9) | 0.702 | |
| Dual antiplatelet duration (months) | 12 (1–24) | 12 (3–36) | 12 (1–24) | 0.501 | |
| Oral anticoagulant using n, (%) | Yes | 5 (3.7%) | 1 (0.9%) | 6 (5.5%) | 0.175 |
| No | 129 (96.3%) | 106 (99.1%) | 103 (94.5%) | ||
| Group I (n = 134) Median (min–max) | Group II (n = 105) Median (min–max) | Group III (n = 104) Median (min–max) | p Value | |
|---|---|---|---|---|
| Stent length (mm) | 18 (6–48) | 20 (8–38) | 23 (15–48) | <0.001 a,b |
| Stent diameter (mm) | 4 (4–4) | 4 (4–4) | 3 (3–3) | <0.001 b,c |
| NC balloon diameter (mm) | 4 (4–4) | 4 (4–4) | 4 (4–4) | 1.000 |
| Final stent diameter (mm) | 4.2 (4–4.4) | 4.2 (4–4.4) | 4.1 (4–4.4) | 0.987 |
| Group I (4 mm BMS) (n = 134) Mean ± SD Median (min–max.) * | Group II (4 mm DES) (n = 105) Mean ± SD Median (min–max.) * | Group III (3 mm DES, 4 mm NC) (n = 104) Mean ± SD Median (min–max.) * | p Value | |
|---|---|---|---|---|
| Target-vessel–associated MI, n (%) | 6 (4.5) | 4 (3.7) | 2 (1.8) | 0.519 |
| Target-lesion revascularization, n (%) | 4 (3) | 2 (1.9) | 1 (0.9) | 0.516 |
| Stent thrombosis, n (%) | 1 (25) | 0 (0) | 0 (0) | 0.646 |
| MI associated with other vessels, n (%) | 4 (3) | 4 (3.7) | 6 (5.5) | 0.600 |
| Major bleeding, n (%) | 2 (1.5) | 1 (0.9) | 0 (0) | 0.452 |
| Time to target-vessel–associated MI (months) | 22 (1–36) | 13 (1–24) | 21 (6–36) | 0.609 |
| Time to target-lesion revascularization (months) | 30 (1–40) | 13 (1–24) | 6 (6–6) | 0.558 |
| Time to MI associated with other vessels (months) | 32 (6–48) | 12 (12–24) | 16 (5–36) | 0.385 |
| Cardiac death, n (%) | 5 (3.7) | 2 (1.9) | 3 (2.7) | 0.687 |
| All-cause death, n (%) | 10 (7.5) | 6 (5.6) | 6 (5.5) | 0.473 |
| Follow-up period (months) | 48 (6–75) | 38 (7–54) | 33 (6–60) | <0.045 * |
| Time to cardiac death (months) | 16 (6–36) | 11 (4–18) | 15 (4–24) | 0.695 |
| Time to death from all causes (months) | 18 (6–46) | 18 (3–24) | 20 (4–59) | 0.621 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gök, G.; Akçay, M.; Yıldırım, U.; Çoksevim, M.; Soylu, K.; Şahin, M. Optimising Percutaneous Coronary Interventions: The Impact of Stent Type and Diameter on Long-Term Clinical Outcomes in Large Coronary Arteries. Medicina 2024, 60, 600. https://doi.org/10.3390/medicina60040600
Gök G, Akçay M, Yıldırım U, Çoksevim M, Soylu K, Şahin M. Optimising Percutaneous Coronary Interventions: The Impact of Stent Type and Diameter on Long-Term Clinical Outcomes in Large Coronary Arteries. Medicina. 2024; 60(4):600. https://doi.org/10.3390/medicina60040600
Chicago/Turabian StyleGök, Gökhan, Murat Akçay, Ufuk Yıldırım, Metin Çoksevim, Korhan Soylu, and Mahmut Şahin. 2024. "Optimising Percutaneous Coronary Interventions: The Impact of Stent Type and Diameter on Long-Term Clinical Outcomes in Large Coronary Arteries" Medicina 60, no. 4: 600. https://doi.org/10.3390/medicina60040600
APA StyleGök, G., Akçay, M., Yıldırım, U., Çoksevim, M., Soylu, K., & Şahin, M. (2024). Optimising Percutaneous Coronary Interventions: The Impact of Stent Type and Diameter on Long-Term Clinical Outcomes in Large Coronary Arteries. Medicina, 60(4), 600. https://doi.org/10.3390/medicina60040600