

Application of Salivary Alpha-1 Antitrypsin in the Diagnosis of Rheumatoid Arthritis: A Pilot Study


Abstract
1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Clinical Variables
2.3. Statistical Analysis
3. Result
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Firestein, G.S. Evolving concepts of rheumatoid arthritis. Nature 2003, 423, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S.; Breedveld, F.C.; Burmester, G.R.; Bykerk, V.; Dougados, M.; Emery, P.; Kvien, T.K.; Navarro-Compán, M.V.; Oliver, S.; Schoels, M.; et al. Treating rheumatoid arthritis to target: 2014 update of the recommendations of an international task force. Ann. Rheum. Dis. 2016, 75, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., III; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. Rheumatoid arthritis classification criteria: An American college of rheumatology/ European league against rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, S.C. Biomarkers in rheumatoid arthritis. Cureus 2021, 13, e15063. [Google Scholar] [CrossRef] [PubMed]
- Carrell, R.W.; Jeppsson, J.O.; Vaughan, L.; Brennan, S.O.; Owen, M.C.; Boswell, D.R. Human alpha 1-antitrypsin: Carbohydrate attachment and sequence homology. FEBS Lett. 1981, 135, 301–303. [Google Scholar] [CrossRef] [PubMed]
- Perlmutter, D.H.; Joslin, G.; Nelson, P.; Schasteen, C.; Adams, S.P.; Fallon, R.J. Endocytosis and degradation of alpha 1-antitrypsin-protease complexes is mediated by the serpin-enzyme complex (SEC) receptor. J. Biol. Chem. 1990, 265, 16713–16716. [Google Scholar] [CrossRef] [PubMed]
- Joslin, G.; Fallon, R.J.; Bullock, J.; Adams, S.P.; Perlmutter, D.H. The SEC receptor recognizes a pentapeptide neodomain of alpha 1-antitrypsin-protease complexes. J. Biol. Chem. 1991, 266, 11282–11288. [Google Scholar] [CrossRef] [PubMed]
- Adonogianaki, E.; Mooney, J.; Kinane, D.F. Detection of stable and active periodontitis sites by clinical assessment and gingival crevicular acute-phase protein levels. J. Periodontal Res. 1996, 31, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Janciauskiene, S.M.; Bals, R.; Koczulla, R.; Vogelmeier, C.; Welte, T. The discovery of α1-antitrypsin and its role in health and disease. Respir. Med. 2011, 105, 1129–1139. [Google Scholar] [CrossRef]
- Cox, D.W.; Huber, O. Rheumatoid arthritis and alpha-1-antitrypsin. Lancet 1976, 1, 1216–1217. [Google Scholar]
- Cox, D.W.; Huber, O. Association of severe rheumatoid arthritis with heterozygosity for alpha 1-antitrypsin deficiency. Clin. Genet. 1980, 17, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Kaneva, M.K.; Muley, M.M.; Krustev, E.; Reid, A.R.; Souza, P.R.; Dell’Accio, F.; McDougall, J.J.; Perretti, M. Alpha-1-antitrypsin reduces inflammation and exerts chondroprotection in arthritis. FASEB J. 2021, 35, e21472. [Google Scholar] [CrossRef]
- Colasanti, T.; Sabatinelli, D.; Mancone, C.; Giorgi, A.; Pecani, A.; Spinelli, F.R.; Di Giamberardino, A.; Navarini, L.; Speziali, M.; Vomero, M.; et al. Homocysteinylated alpha 1 antitrypsin as an antigenic target of autoantibodies in seronegative rheumatoid arthritis patientsa. J. Autoimmun. 2020, 13, 102470. [Google Scholar] [CrossRef] [PubMed]
- Arnett, F.C.; Edworthy, S.M.; Bloch, D.A.; Mcshane, D.J.; Fries, J.F.; Cooper, N.S.; Healey, L.A.; Kaplan, S.R.; Liang, M.H.; Luthra, H.S.; et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988, 31, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Priya, Y.; Prathibha, M. Methods of collection of saliva—A Review. Int. J. Oral Health Dent. 2017, 3, 149–153. [Google Scholar]
- Serdaroğlu, M.; Cakirbay, H.; Değer, O.; Cengiz, S.; Kul, S. The association of anti-CCP antibodies with disease activity in rheumatoid arthritis. Rheumatol. Int. 2008, 28, 965–970. [Google Scholar] [CrossRef] [PubMed]
- Turesson, C.; Jacobsson, L.T.; Sturfelt, G.; Matteson, E.L.; Mathsson, L.; Rönnelid, J. Rheumatoid factor and antibodies to cyclic citrullinated peptides are associated with severe extra-articular manifestations in rheumatoid arthritis. Ann. Rheum. Dis. 2007, 66, 59–64. [Google Scholar] [CrossRef]
- Bugatti, S.; Manzo, A.; Montecucco, C.; Caporali, R. The Clinical Value of Autoantibodies in Rheumatoid Arthritis. Front. Med. 2018, 5, 339. [Google Scholar] [CrossRef]
- Cheng, Z.; Meade, J.; Mankia, K.; Emery, P.; Devine, D.A. Periodontal disease and periodontal bacteria as triggers for rheumatoid arthritis. Best. Pract. Res. Clin. Rheumatol. 2017, 31, 19–30. [Google Scholar] [CrossRef]
- Li, R.; Tian, C.; Postlethwaite, A.; Jiao, Y.; Garcia-Godoy, F.; Pattanaik, D.; Wei, D.; Gu, W.; Li, J. Rheumatoid arthritis and periodontal disease: What are the similarities and differences? Int. J. Rheum. Dis. 2017, 20, 1887–1901. [Google Scholar] [CrossRef]
- Eriksson, K.; Fei, G.; Lundmark, A.; Benchimol, D.; Lee, L.; Hu, Y.O.; Kats, A.; Saevarsdottir, S.; Catrina, A.I.; Klinge, B.; et al. Periodontal Health and oral microbiota in patients with rheumatoid arthritis. J. Clin. Med. 2019, 8, 630. [Google Scholar] [CrossRef] [PubMed]
- Hitchon, C.A.; Chandad, F.; Ferucci, E.D.; Willemze, A.; Ioan-Facsinay, A.; van der Woude, D.; Markland, J.; Robinson, D.; Elias, B.; Newkirk, M.; et al. Antibodies to Porphyromonas gingivalisare associated with anticitrullinated protein antibodies in patients with rheumatoid arthritis and their relatives. J. Rheumatol. 2010, 37, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- Turino, G.M.; Senior, R.M.; Garg, B.D.; Keller, S.; Levi, M.M.; Mandl, I. Serum elastase inhibitor deficiency and agrl- antitrypsin deficiency in patients with obstructive emphysema. Science 1969, 165, 709–710. [Google Scholar] [CrossRef] [PubMed]
- Bergin, D.A.; Hurley, K.; McElvaney, N.G.; Reeves, E.P. Alpha-1 anti-trypsin: A potent anti-inflammatory and potential novel therapeutic agent. Arch. Immunol. Ther. Exp. 2012, 60, 81–97. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.; Sharma, S.; Saroha, A.; Bhakuni, D.S.; Malhotra, R.; Zahur, M.; Oellerich, M.; Das, H.R.; Asif, A.R. Identification of novel autoan-tigen in the synovial fluid of rheumatoid arthritis patients using an immunoproteomics approach. PLoS ONE 2013, 8, e56246. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.; Xu, Z.; Zhu, C.; Chen, T.; Muñoz, L.E.; Dai, L.; Zhao, Y. Alpha-1 antitrypsin in autoimmune diseases: Roles and therapeutic prospects. Int. Immunopharmacol. 2022, 110, 109001. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Suzuki, Y.; Saito, A.; Fukuda, K.; Hamanishi, C.; Munakata, H. Aggrecanase-1 (ADAMTS-4) interacts with alpha1-antitrypsin. Biochim. Biophys. Acta 2005, 1725, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Madhok, R.; Crilly, A.; Watson, J.; Capell, H.A. Serum interleukin 6 levels in rheumatoid arthritis: Correlations with clinical and laboratory indices of disease activity. Ann. Rheum. Dis. 1993, 52, 232–234. [Google Scholar] [CrossRef]
- Cush, J.J.; Splawski, J.B.; Thomas, R.; Mcfarlin, J.E.; Schulze-Koops, H.; Davis, L.S.; Fujita, K.; Lipsky, P.E. Elevated interleukin-10 levels in patients with rheumatoid arthritis. Arthritis Rheum. 1995, 38, 96–104. [Google Scholar] [CrossRef]
- Kaczyński, T.; Wroński, J.; Głuszko, P.; Kryczka, T.; Miskiewicz, A.; Górski, B.; Radkowski, M.; Strzemecki, D.; Grieb, P.; Górska, R. Salivary interleukin 6, interleukin 8, interleukin 17A, and tumour necrosis factor α levels in patients with periodontitis and rheumatoid arthritis. Cent. Eur. J. Immunol. 2019, 44, 269–276. [Google Scholar] [CrossRef]


{kind=link}
| RA (n = 60) | HC (n = 20) | p-Value | |
|---|---|---|---|
| Age, year | 56.58 ± 12.49 | 43.85 ± 7.87 | <0.001 |
| Sex | 0.161 | ||
| Male | 14 (23.3) | 8 (23.3) | |
| Female | 46 (76.7) | 12 (60.0) | |
| Saliva for 5 min (mL) | 3.47 ± 2.45 | 4.86 ± 2.37 | 0.035 |
| Comorbidities | |||
| HTN | 16 (26.7) | 4 (20.0) | 0.392 |
| Dyslipidemia | 22 (36.7) | 1 (5.0) | 0.004 |
| DM | 5 (8.3) | 1 (5.0) | 0.530 |
| COPD | 6 (10.0) | 0 (0) | 0.167 |
| Chronic liver disease | 2 (3.3) | 1 (3.8) | 0.583 |
| Laboratory data | |||
| ESR (mm/h) | 24.88 ± 19.77 | - | |
| CRP (mg/dL) | 0.59 ± 0.61 | - | |
| RF positive | 40 (66.7) | - | - |
| RF (IU/mL) | 124.48 ± 212.88 | - | |
| Anti-CCP positive, | 40 (66.7) | - | - |
| Anti-CCP (units/mL) | 268.82 ± 481.47 | - | |
| Seronegative RA | 20 (33.3) | ||
| Anti Ro | 3 (14.3) | ||
| DAS28-ESR | 2.71 ± 0.96 | - | |
| DAS28-CRP | 2.12 ± 2.49 | - |
| Average Concentration of Studied Cytokines | RA | HC | p-Value |
|---|---|---|---|
| Salivary A1AT (ng/mL) | 2388.66 ± 1875.80 | 1579.06 ± 1067.06 | 0.021 |
| Serum A1AT (mg/mL) | 1.7879 ± 1.5933 | 1.5932 ± 3.7173 | 0.082 |
| Salivary IL-1β | 540.89 ± 777.05 | 488.25 ± 379.03 | 0.690 |
| Serum IL-1β | 1.5497 ± 0.1583 | 1.5780 ± 0.1388 | 0.451 |
| Salivary IL-6 | 8.6967 ± 12.9693 | 6.4845 ± 6.9939 | 0.338 |
| Serum IL-6 | 5.250 ± 9.4003 | 0.2100 ± 0.42323 | <0.001 |
| Salivary IL-10 | 1.9150 ± 3.1140 | 1.4365 ± 1.0244 | 0.304 |
| Serum IL-10 | 2.8665 ± 1.0448 | 1.3880 ± 0.1503 | <0.001 |
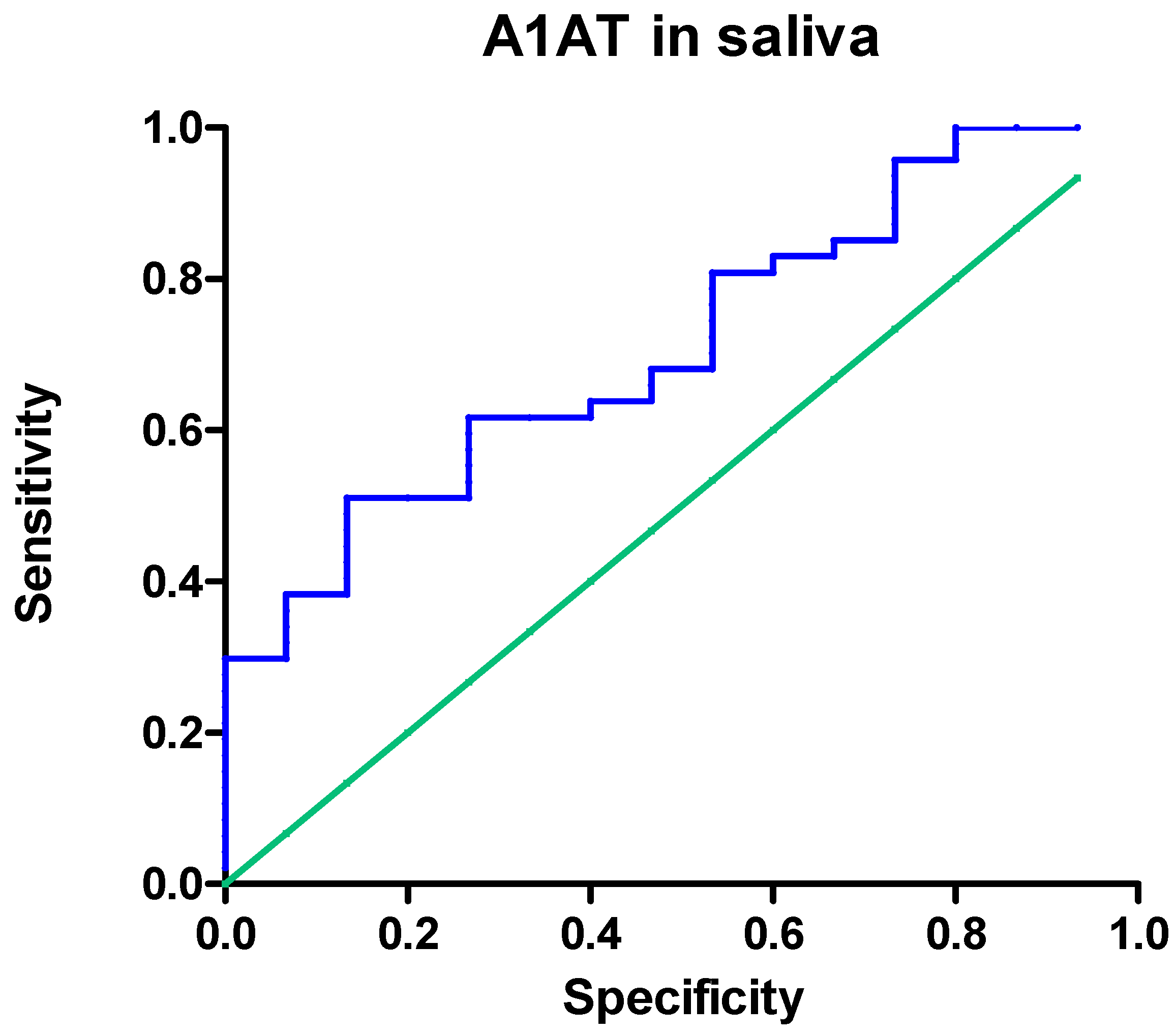
| Outcomes | AUC (95% CI) | p-Value | Cut-Off (ng/mL) | Sensitivity | Specificity | LR |
|---|---|---|---|---|---|---|
| α1-antitrypsin in saliva | 0.7135 (0.5741–0.8529) | 0.0134 | 1689.0 | 0.62 | 0.73 | 2.31 |
| Average Concentration of Studied Cytokines | Seropositive RA | Seronegative RA | HC | p-Value (SPRA vs. HC) | p-Value (SNRA vs. HC) |
|---|---|---|---|---|---|
| Salivary A1AT (ng/mL) | 2279.78 ± 1619.78 | 2715.32 ± 2535.79 | 1579.06 ± 1068.06 | 0.044 | 0.121 |
| Serum A1AT (mg/mL) | 1.7575 ± 5.8905 | 1.8793 ± 4.4631 | 1.5932 ± 3.7173 | 0.180 | 0.054 |
| Salivary IL-1β | 537.34 ± 727.79 | 551.57 ± 937.95 | 488.25 ± 379.03 | 0.723 | 0.808 |
| Serum IL-1β | 1.5460 ± 0.1579 | 1.5607 ± 0.1647 | 1.5780 ± 0.1388 | 0.416 | 0.745 |
| Salivary IL-6 | 8.7567 ± 14.6085 | 8.5167 ± 6.1728 | 6.4845 ± 6.9939 | 0.400 | 0.370 |
| Serum IL-6 | 5.2533 ± 5.3263 | 5.2400 ± 16.8295 | 0.2100 ± 0.42323 | <0.001 | 0.267 |
| Salivary IL-10 | 1.6487 ± 2.9711 | 2.7140 ± 3.4943 | 1.4365 ± 1.0244 | 0.672 | 0.189 |
| Serum IL-10 | 3.3182 ± 0.7851 | 1.5113 ± 0.1998 | 1.3880 ± 0.1503 | <0.001 | 0.056 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, S.W.; Hong, S.-J. Application of Salivary Alpha-1 Antitrypsin in the Diagnosis of Rheumatoid Arthritis: A Pilot Study. Medicina 2024, 60, 605. https://doi.org/10.3390/medicina60040605
Chung SW, Hong S-J. Application of Salivary Alpha-1 Antitrypsin in the Diagnosis of Rheumatoid Arthritis: A Pilot Study. Medicina. 2024; 60(4):605. https://doi.org/10.3390/medicina60040605
Chicago/Turabian StyleChung, Sang Wan, and Seung-Jae Hong. 2024. "Application of Salivary Alpha-1 Antitrypsin in the Diagnosis of Rheumatoid Arthritis: A Pilot Study" Medicina 60, no. 4: 605. https://doi.org/10.3390/medicina60040605
APA StyleChung, S. W., & Hong, S.-J. (2024). Application of Salivary Alpha-1 Antitrypsin in the Diagnosis of Rheumatoid Arthritis: A Pilot Study. Medicina, 60(4), 605. https://doi.org/10.3390/medicina60040605