
Correlation between Radiological Characteristics, PET-CT and Histological Subtypes of Primary Lung Adenocarcinoma—A 102 Case Series Analysis

 , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
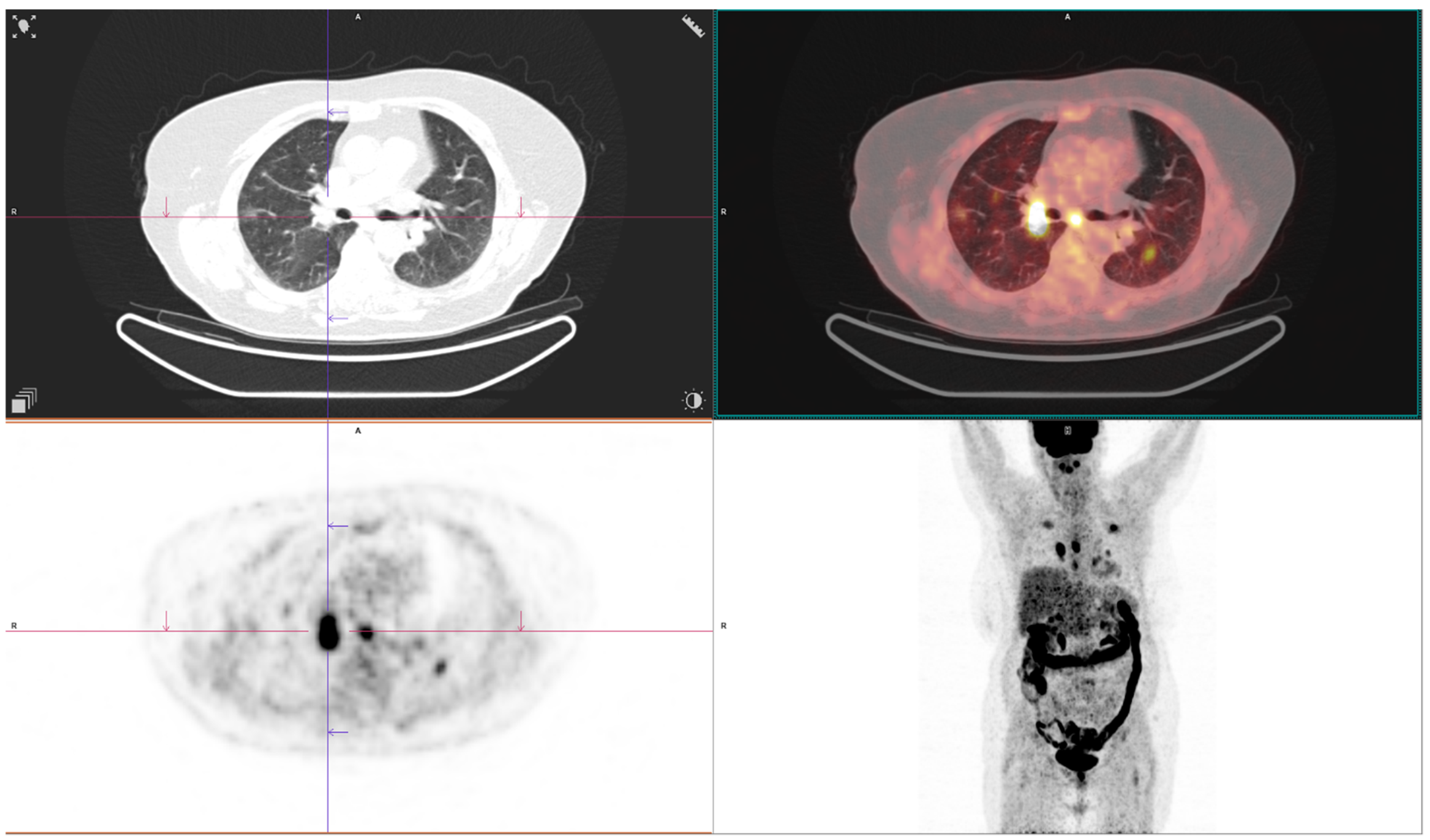
2.2. CT and FDG PET CT Image Acquisition
Acquisition and Interpretation of 18F-FDG PET/CT Findings
2.3. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cohen, J.G.; Reymond, E.; Jankowski, A.; Brambilla, E.; Arbib, F.; Lantuejoul, S.; Ferretti, G.R. Adénocarcinomes pulmonaires: Corrélations entre TDM et histopathologie. J. Radiol. Diagn. Interv. 2016, 97, 375–384. [Google Scholar] [CrossRef]
- Lantuejoul, S.; Rouquette, I.; Brambilla, E.; Travis, W.D. Nouvelle classification OMS 2015 des adénocarcinomes pulmonaires et prénéoplasies. Ann. Pathol. 2016, 36, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Brambilla, E.; Noguchi, M.; Nicholson, A.G.; Geisinger, K.R.; Yatabe, Y.; Powell, C.A.; Beer, D.G.; Riely, G.J.; Garg, K.; et al. International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society: International Multidisciplinary Classification of Lung Adenocarcinoma: Executive Summary. Proc. Am. Thorac. Soc. 2011, 5, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Yanagawa, M.; Johkoh, T.; Noguchi, M.; Morii, E.; Shintani, Y.; Okumura, M.; Hata, A.; Fujiwara, M.; Honda, O.; Tomiyama, N. Radiological prediction of tumor invasiveness of lung adenocarcinoma on thin-section CT. Medicine 2017, 96, e6331. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.G.; Reymond, E.; Jankowski, A.; Brambilla, E.; Arbib, F.; Lantuejoul, S.; Ferretti, G.R. Lung adenocarcinomas: Correlation of computed tomography and pathology findings. Diagn. Interv. Imaging 2016, 97, 955–963. [Google Scholar] [CrossRef] [PubMed]
- Underwood, C.; Musick, A.; Glass, C. Adenocarcinoma Overview. Available online: https://www.pathologyoutlines.com/topic/lungtumoradenocarcinoma.html (accessed on 14 December 2023).
- Kao, T.N.; Hsieh, M.S.; Chen, L.W.; Yang, C.F.J.; Chuang, C.C.; Chiang, X.H.; Chen, Y.C.; Lee, Y.H.; Hsu, H.H.; Chen, C.M.; et al. CT-Based Radiomic Analysis for Preoperative Prediction of Tumor Invasiveness in Lung Adenocarcinoma Presenting as Pure Ground-Glass Nodule. Cancers 2022, 14, 5888. [Google Scholar] [CrossRef]
- Castro, C.Y.; Coffey, D.M.; Medeiros, L.J.; Cagle, P.T. Prognostic significance of percentage of bronchioloalveolar pattern in adenocarcinomas of the lung. Ann. Diagn. Pathol. 2001, 5, 274–284. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.W.; Chen, W.F.; He, W.J.; Yang, Z.M.; Li, M.; Xiao, L.; Hua, Y.Q. CT features differentiating pre- and minimally invasive from invasive adenocarcinoma appearing as mixed ground-glass nodules: Mass is a potential imaging biomarker. Clin. Radiol. 2018, 73, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Nakazono, T.; Sakao, Y.; Yamaguchi, K.; Imai, S.; Kumazoe, H.; Kudo, S. Subtypes of peripheral adenocarcinoma of the lung: Differentiation by thin-section CT. Eur. Radiol. 2005, 15, 1563–1568. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, E.; Morbini, P.; Cancellieri, A.; Damiani, S.; Cavazza, A.; Comin, C.E. Adenocarcinoma classification: Patterns and prognosis. Pathologica 2018, 110, 5–11. [Google Scholar] [PubMed]
- Tsutani, Y.; Miyata, Y.; Mimae, T.; Kushitani, K.; Takeshima, Y.; Yoshimura, M.; Okada, M. The prognostic role of pathologic invasive component size, excluding lepidic growth, in stage I lung adenocarcinoma. J. Thorac. Cardiovasc. Surg. 2013, 146, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Woodruff, H.C.; Shen, J.; Refaee, T.; Sanduleanu, S.; Ibrahim, A.; Leijenaar, R.T.H.; Wang, R.; Xiong, J.; Bian, J.; et al. Diagnosis of Invasive Lung Adenocarcinoma Based on Chest CT Radiomic Features of Part-Solid Pulmonary Nodules: A Multicenter Study. Radiology 2020, 297, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, H.M.; Knipe, H.C.; Pascoe, D.; Heinze, S.B. The many faces of lung adenocarcinoma: A pictorial essay. J. Med. Imaging Radiat. Oncol. 2018, 62, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Yang, Y.; Liu, X.; Deng, J.; Wu, J.; Hou, L.; Wu, C.; She, Y.; Sun, X.; Xie, D.; et al. Primary Invasive Mucinous Adenocarcinoma of the Lung: Prognostic Value of CT Imaging Features Combined with Clinical Factors. Korean J. Radiol. 2021, 22, 652–662. [Google Scholar] [CrossRef] [PubMed]
- Kuriyama, K.; Yanagawa, M. CT Diagnosis of Lung Adenocarcinoma: Radiologic-Pathologic Correlation and Growth Rate. Radiology 2020, 297, 199–200. [Google Scholar] [CrossRef] [PubMed]
- Shao, X.; Niu, R.; Jiang, Z.; Shao, X.; Wang, Y. Role of PET/CT in Management of Early Lung Adenocarcinoma. AJR Am. J. Roentgenol. 2020, 214, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.Y.; Chen, T.X.; Chang, C.; Teng, H.H.; Xie, C.; Ruan, M.M.; Lei, B.; Liu, L.; Wang, L.H.; Yang, Y.H.; et al. SUVmax of 18FDG PET/CT Predicts Histological Grade of Lung Adenocarcinoma. Acad. Radiol. 2021, 28, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Mogavero, A.; Bironzo, P.; Righi, L.; Merlini, A.; Benso, F.; Novello, S.; Passiglia, F. Deciphering Lung Adenocarcinoma Heterogeneity: An Overview of Pathological and Clinical Features of Rare Subtypes. Life 2023, 13, 1291. [Google Scholar] [CrossRef] [PubMed]
- Damirov, F.; Stoleriu, M.G.; Manapov, F.; Büsing, K.; Michels, J.D.; Preissler, G.; Hatz, R.A.; Hohenberger, P.; Roessner, E.D. Histology of the Primary Tumor Correlates with False Positivity of Integrated 18F-FDG-PET/CT Lymph Node Staging in Resectable Lung Cancer Patients. Diagnostics 2023, 13, 1893. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.Y.; Chen, P.H.; Chen, K.C.; Hsu, H.H.; Chen, J.S. Computed Tomography-Guided Localization and Extended Segmentectomy for Non-Small Cell Lung Cancer. Diagnostics 2022, 12, 2043. [Google Scholar] [CrossRef] [PubMed]
- Divisi, D.; Rinaldi, M.; Necozione, S.; Curcio, C.; Rea, F.; Zaraca, F.; De Vico, A.; Zaccagna, G.; Di Leonardo, G.; Crisci, R.; et al. Is It Possible to Establish a Reliable Correlation between Maximum Standardized Uptake Value of 18-Fluorine Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography and Histological Types of Non-Small Cell Lung Cancer? Analysis of the Italian VATS Group Database. Diagnostics 2021, 11, 1901. [Google Scholar] [CrossRef] [PubMed]
- Nakada, T.; Takahashi, Y.; Sakakura, N.; Iwata, H.; Ohtsuka, T.; Kuroda, H. Prognostic Radiological Tools for Clinical Stage IA Pure Solid Lung Cancer. Curr. Oncol. 2021, 28, 3846–3856. [Google Scholar] [CrossRef] [PubMed]
- Kudura, K.; Ritz, N.; Kutzker, T.; Hoffmann, M.H.K.; Templeton, A.J.; Foerster, R.; Kreissl, M.C.; Antwi, K. Predictive Value of Baseline FDG-PET/CT for the Durable Response to Immune Checkpoint Inhibition in NSCLC Patients Using the Morphological and Metabolic Features of Primary Tumors. Cancers 2022, 14, 6095. [Google Scholar] [CrossRef] [PubMed]
- Carter, B.W.; Halpenny, D.F.; Ginsberg, M.S.; Papadimitrakopoulou, V.A.; de Groot, P.M. Immunotherapy in Non-Small Cell Lung Cancer Treatment: Current Status and the Role of Imaging. J. Thorac. Imaging. 2017, 32, 300–312. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Shi, Y.; Niu, R.; Shao, X.; Shao, X. Association Analysis of Maximum Standardized Uptake Values Based on 18F-FDG PET/CT and EGFR Mutation Status in Lung Adenocarcinoma. J. Pers. Med. 2023, 13, 396. [Google Scholar] [CrossRef] [PubMed]
- Cha, H.K.; Lim, J.H.; Ryu, W.K.; Kim, L.; Ryu, J.-S. Solitary Uncommon Metastasis in Non-Small Cell Lung Cancer. Reports 2023, 6, 8. [Google Scholar] [CrossRef]
- Dunn, B.; Pierobon, M.; Wei, Q. Automated Classification of Lung Cancer Subtypes Using Deep Learning and CT-Scan Based Radiomic Analysis. Bioengineering 2023, 10, 690. [Google Scholar] [CrossRef] [PubMed]
- Monaco, L.; De Bernardi, E.; Bono, F.; Cortinovis, D.; Crivellaro, C.; Elisei, F.; L’Imperio, V.; Landoni, C.; Mathoux, G.; Musarra, M.; et al. The “digital biopsy” in non-small cell lung cancer (NSCLC): A pilot study to predict the PD-L1 status from radiomicsfeatures of [18F]FDG PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 3401–3411. [Google Scholar] [CrossRef] [PubMed]
- Succony, L.; Rassl, D.M.; Barker, A.P.; McCaughan, F.M.; Rintoul, R.C. Adenocarcinoma spectrum lesions of the lung: Detection, pathology and treatment strategies. Cancer Treat. Rev. 2021, 99, 102237. [Google Scholar] [CrossRef]
- Chiu, T.H.; Lin, C.Y.; Hsieh, M.H.; Lin, S.M.; Fang, Y.F. Prognostic Factors in Lung Adenocarcinoma with Bone Metastasis Treated with EGFR-TKIs. Medicina 2021, 57, 967. [Google Scholar] [CrossRef] [PubMed]
- Marghescu, A.-Ș.; Leonte, D.G.; Radu, A.D.; Măgheran, E.D.; Tudor, A.V.; Teleagă, C.; Țigău, M.; Georgescu, L.; Costache, M. Atypical Histopathological Aspects of Common Types of Lung Cancer—Our Experience and Literature Review. Medicina 2024, 60, 112. [Google Scholar] [CrossRef] [PubMed]
- Lai, W.A.; Huang, Y.S.; Chang, K.C.; Yang, S.F.; Yang, C.J.; Liu, Y.W.; Chen, H.D. Next-Generation Sequencing in Lung Cancers—A Single-Center Experience in Taiwan. Medicina 2024, 60, 236. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Acinar | Papillary | Lepidic | Solid | AIS-MIA | p Value | Comparison Group * | Post Hoc p Value ¥ | |
|---|---|---|---|---|---|---|---|---|
| n = 32 (31.4%) | n = 28 (27.5%) | n = 19 (18.6%) | n = 13 (12.7%) | n = 10 (9.8%) | ||||
| Age, mean ± SD | 62.8 ± 7.0 | 62.7 ± 7.0 | 61.8 ± 7.4 | 63.7 ± 7.2 | 61.0 ± 5.6 | 0.893 | ||
| Gender, n (%) | ||||||||
| Male | 21 (65.6) | 14 (50.0) | 4 (21.1) | 9 (69.2) | 5 (50.0) | 0.024 | Acinar vs. Lepidic | 0.003 |
| Female | 11 (34.4) | 14 (50.0) | 15 (78.9) | 4 (30.8) | 5 (50.0) | |||
| p value | p > 0.005 | p > 0.005 | p > 0.005 | p > 0.005 | p > 0.005 | |||
| Smoking status, n (%) | ||||||||
| Non-smoker | 10 (31.3) | 16 (57.1) | 5 (26.3) | 7 (53.8) | 1 (10.0) | 0.052 | ||
| Former smoker | 8 (25.0) | 2 (7.1) | 2 (10.5) | 1 (7.7) | 1 (10.0) | |||
| Current smoker | 14 (43.8) | 10 (35.7) | 12 (63.2) | 5 (38.5) | 8 (80.0) | |||
| p value | p > 0.005 | p > 0.005 | p > 0.005 | p > 0.005 | p > 0.005 |
| Acinar | Papillary | Lepidic | Solid | AIS-MIA | Overall p Value | Comparison Group | Mean Difference | |
|---|---|---|---|---|---|---|---|---|
| n = 32 | n = 28 | n = 19 | n = 13 | n = 10 | ||||
| Tumor size, mean ± SD | 37.2 ± 7.6 | 41.8 ± 8.6 | 38.2 ± 6.0 | 47.7 ± 12.6 | 24.9 ± 3.7 | <0.001 | Acinar vs. Solid | 10.44 |
| Acinar vs. AIS-MIA | 12.35 | |||||||
| Papillary vs. AIS-MIA | 16.89 | |||||||
| Lepidic vs. AIS-MIA | 13.26 | |||||||
| Solid vs. AIS-MIA | 22.79 | |||||||
| Component n (%) | ||||||||
| Solid | 32 (100) | 28 (100) | 19 (100) | 13 (100) | 9 (90.0) | 0.054 | ||
| Necrosis | 3 (9.4) | 9 (32.1) | 5 (26.3) | 4 (30.8) | 0 (0.0) | 0.074 | ||
| Ground glass | 3 (9.4) | 0 (0.0) | 1 (5.3) | 1 (7.7) | 3 (30.0) | 0.051 | ||
| p value | p > 0.005 | p > 0.005 | p > 0.005 | p > 0.005 | p > 0.005 | p > 0.005 | ||
| Edges n (%) | ||||||||
| Round | 19 (59.4) | 14 (50.0) | 14 (73.7) | 7 (53.8) | 5 (50.0) | 0.244 | ||
| Lobular | 4 (12.5) | 4 (14.3) | 2 (10.5) | 5 (38.5) | 3 (30.0) | |||
| Spiculated | 9 (28.1) | 10 (35.7) | 3 (15.8) | 1 (7.7) | 2 (20.0) | |||
| p value | p > 0.005 | p > 0.005 | p > 0.005 | p > 0.005 | p > 0.005 |
| Acinar | Papillary | Lepidic | Solid | AIS-MIA | Overall p Value | |
|---|---|---|---|---|---|---|
| n = 32 | n = 28 | n = 19 | n = 13 | n = 10 | ||
| Pleural involvement, n (%) | 11 (34.4) | 15 (53.6) | 5 (26.3) | 8 (61.5) | 2 (20.0) | 0.084 |
| Bronchial cut-off, n (%) | 12 (37.5) | 13 (46.4) | 10 (52.6) | 9 (69.2) | 5 (50.0) | 0.41 |
| Vascular invasion, n (%) | 11 (34.4) | 16 (57.1) | 9 (47.4) | 6 (46.2) | 3 (30.0) | 0.397 |
| No lymph node involvement | 9 (28.1) | 4 (14.3) | 9 (47.7) | 2 (15.4) | 7 (70.0) | 0.049 |
| Ipsilateral lymph node involvement | 18 (56.3) | 18 (64.3) | 8 (42.1) | 9 (69.2) | 3 (30.3) | |
| Contralateral lymph node involvement | 5 (15.6) | 6 (21.4) | 2 (10.5) | 2 (15.4) | 0 (0.0) | |
| p values | p > 0.005 | p > 0.005 | p > 0.005 | p > 0.005 | p > 0.005 |
| Acinar | Papillary | Lepidic | Solid | AIS-MIA | Overall p Value | Comparison Group | Mean Difference | 95%CI ** | Post Hoc p Value ¥ | |
|---|---|---|---|---|---|---|---|---|---|---|
| n = 32 | n = 28 | n = 19 | n = 13 | n = 10 | ||||||
| Metastases present, n (%) | 3 (9.4%) | 7 (25.0%) | 0 (0.0%) | 8 (61.5%) | 0 (0.0%) | <0.001 | Acinar vs. solid | na | na | 0.001 |
| Lepidic vs. solid | na | na | <0.001 | |||||||
| Solid vs. AIS-MIA | na | na | 0.003 | |||||||
| SUVmax, mean ± SD | 4.9 ± 1.1 | 5.3 ± 1.3 | 5.1 ± 0.7 | 6.3 ± 0.8 | 3.3 ± 0.8 | <0.001 | Acinar vs. solid | −1.35 | −1.89 to −0.76 | 0.001 |
| Acinar vs. AIS-MIA | 1.65 | 1.00 to 2.28 | <0.001 | |||||||
| Papillary vs. AIS-MIA | 2.01 | 1.35 to 2.72 | <0.001 | |||||||
| Lepidic vs. AIS-MIA | 1.83 | 1.23 to 2.38 | <0.001 | |||||||
| Solid vs. AIS-MIA | −3 | 2.32 vs. 3.59 | <0.001 |
| Acinar | Papillary | Lepidic | Solid | AIS-MIA | |
|---|---|---|---|---|---|
| n = 32 | n = 28 | n = 19 | n = 13 | n = 10 | |
| Characteristic | OR (95%CI) | OR (95%CI) | OR (95%CI) | OR (95%CI) | OR (95%CI) |
| Tumor size | 0.97 (0.92–1.02) | 1.04 (1.00–1.09) | 1.00 (0.95–1.05) | 1.11 (1.04–1.18) | 0.65 (0.51–0.83) |
| Necrosis | 0.27 (0.07–1.03) | 2.57 (0.90–7.37) | 1.69 (0.46–6.17) | 1.80 (0.47–6.96) | 0 |
| Ground glass | 1.25 (0.27–5.89) | 0 | 0.69 (0.07–6.59) | 1.00 (0.11–9.38) | 7.19 (1.35–38.34) |
| Round edges | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| Lobular edges | 0.62 (0.18–2.22) | 9.91 (0.25–3.22) | 0.32 (0.06–1.67) | 3.17 (0.83–12.19) | 2.28 (0.48–10.81) |
| Spiculated edges | 1.16 (0.42–3.16) | 2.16 (0.79–5.89) | 0.43 (0.11–1.74) | 0.28 (0.03–2.42) | 1.00 (0.18–5.62) |
| Pleural involvement | 0.62 (0.25–1.53) | 2.18 (0.89–5.34) | 0.52 (1.16–1.66) | 2.48 (0.73–8.43) | 0.35 (0.70–1.77) |
| Bronchial cut-off | 0.60 (0.25–1.48) | 0.87 (0.35–2.16) | 0.90 (0.31–2.62) | 3.53 (0.93–13.36) | 1.17 (0.30–4.56) |
| Vascular invasion | 0.55 (2.23–1.33) | 2.06 (0.85–4.99) | 1.17 (0.41–3.34) | 1.11 (0.34–3.60) | 0.52 (0.13–2.17) |
| No lymph node involvement | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 |
| Ipsilateral lymph node involvement | 1.08 (0.40–2.90) | 3.26 (0.98–10.80) | 0.43 (1.14–1.34) | 2.54 (0.50–12.98) | 0.20 (0.05–0.85) |
| Contralateral lymph node involvement | 1.32 (0.34–5.16) | 4.49 (1.02–19.73) | 0.30 (0.05–1.74) | 2.34 (0.29–19.04) | 0 |
| Metastases present | 0.34 (0.09–1.33) | 1.93 (0.65–5.72) | 0 | 14.09 (3.51–56.41) | 0 |
| SUVmax | 0.86 (0.59–1.23) | 1.21 (0.86–1.73) | 1.04 (0.69–1.57) | 2.64 (1.48–4.69) | 0.07 (0.02–0.29) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colic, N.; Stevic, R.; Stjepanovic, M.; Savić, M.; Jankovic, J.; Belic, S.; Petrovic, J.; Bogosavljevic, N.; Aleksandric, D.; Lukic, K.; et al. Correlation between Radiological Characteristics, PET-CT and Histological Subtypes of Primary Lung Adenocarcinoma—A 102 Case Series Analysis. Medicina 2024, 60, 617. https://doi.org/10.3390/medicina60040617
Colic N, Stevic R, Stjepanovic M, Savić M, Jankovic J, Belic S, Petrovic J, Bogosavljevic N, Aleksandric D, Lukic K, et al. Correlation between Radiological Characteristics, PET-CT and Histological Subtypes of Primary Lung Adenocarcinoma—A 102 Case Series Analysis. Medicina. 2024; 60(4):617. https://doi.org/10.3390/medicina60040617
Chicago/Turabian StyleColic, Nikola, Ruza Stevic, Mihailo Stjepanovic, Milan Savić, Jelena Jankovic, Slobodan Belic, Jelena Petrovic, Nikola Bogosavljevic, Dejan Aleksandric, Katarina Lukic, and et al. 2024. "Correlation between Radiological Characteristics, PET-CT and Histological Subtypes of Primary Lung Adenocarcinoma—A 102 Case Series Analysis" Medicina 60, no. 4: 617. https://doi.org/10.3390/medicina60040617