
Predictive Model of Recovery to Prefracture Activities-of-Daily-Living Status One Year after Fragility Hip Fracture
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
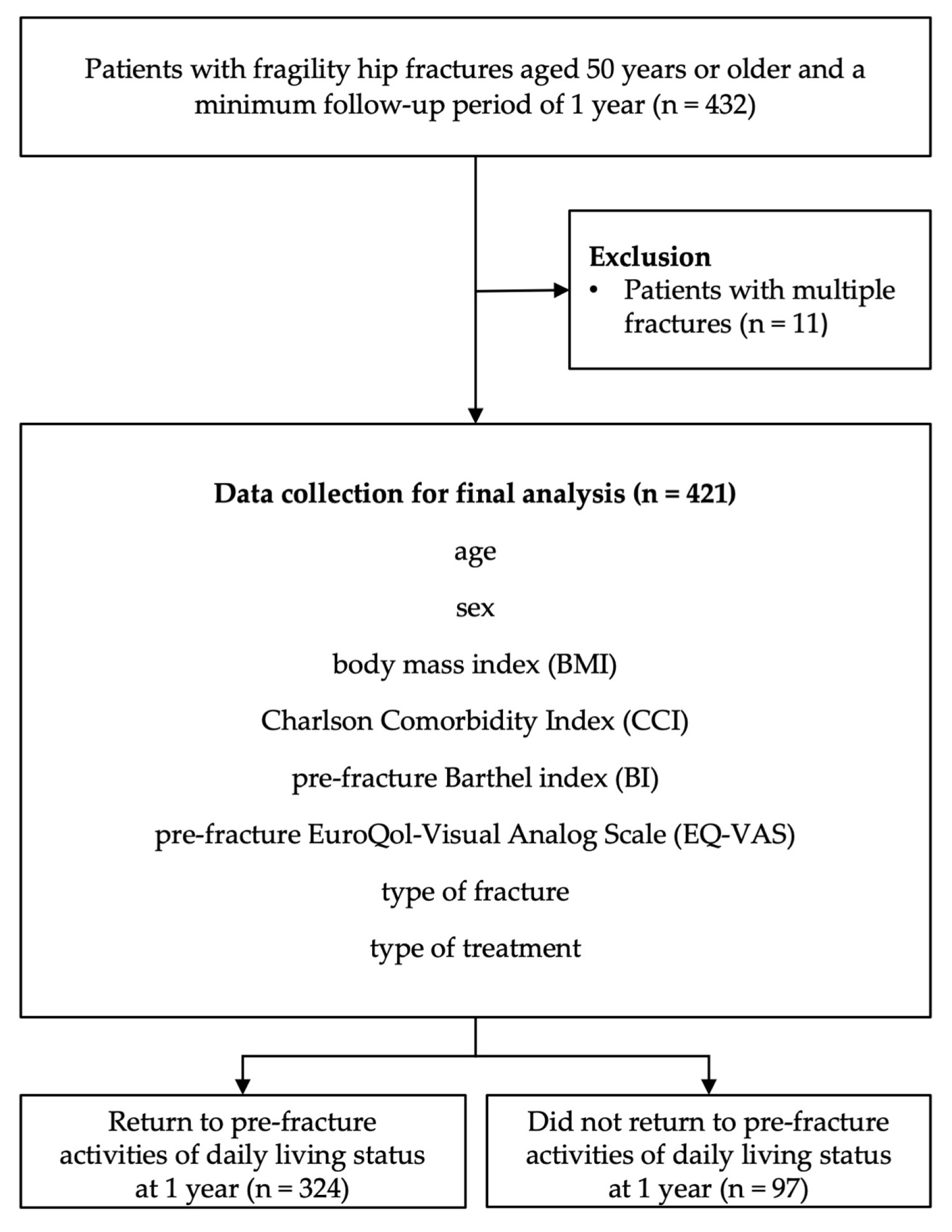
2.2. Study Patients
2.3. Treatment Protocol
2.4. Data Collection
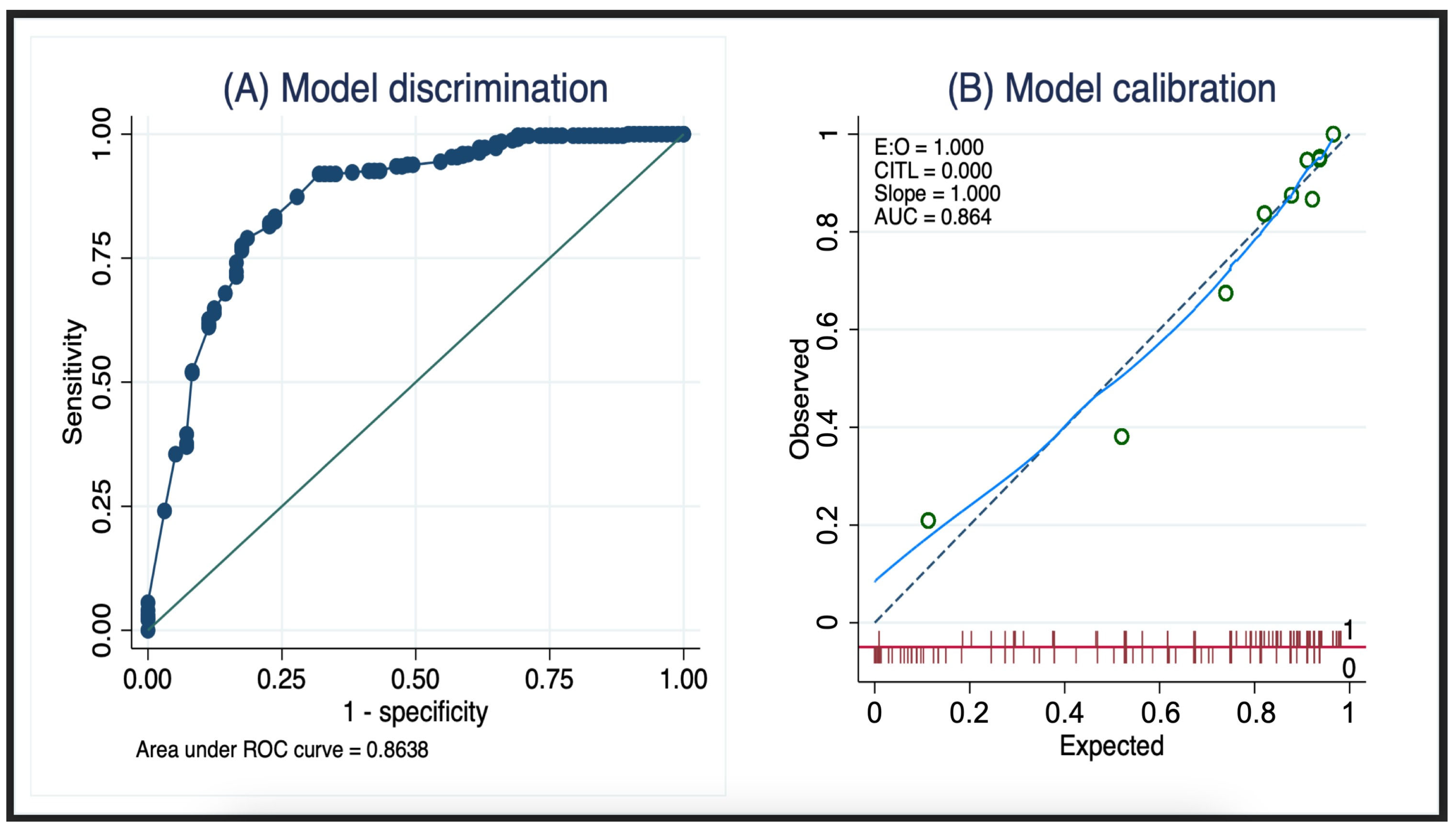
2.5. Statistical Analysis
3. Results
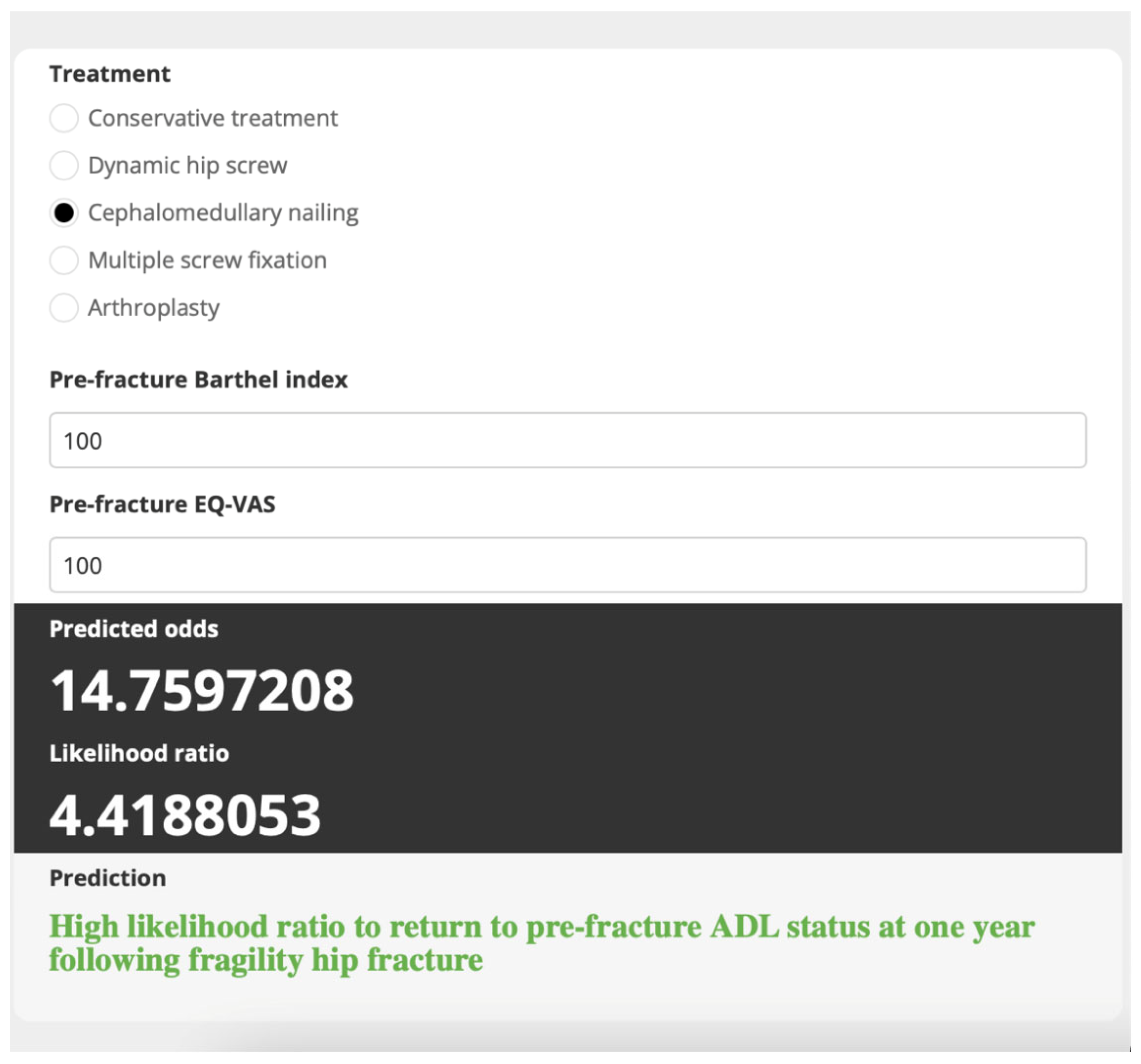
- Scenario 1:
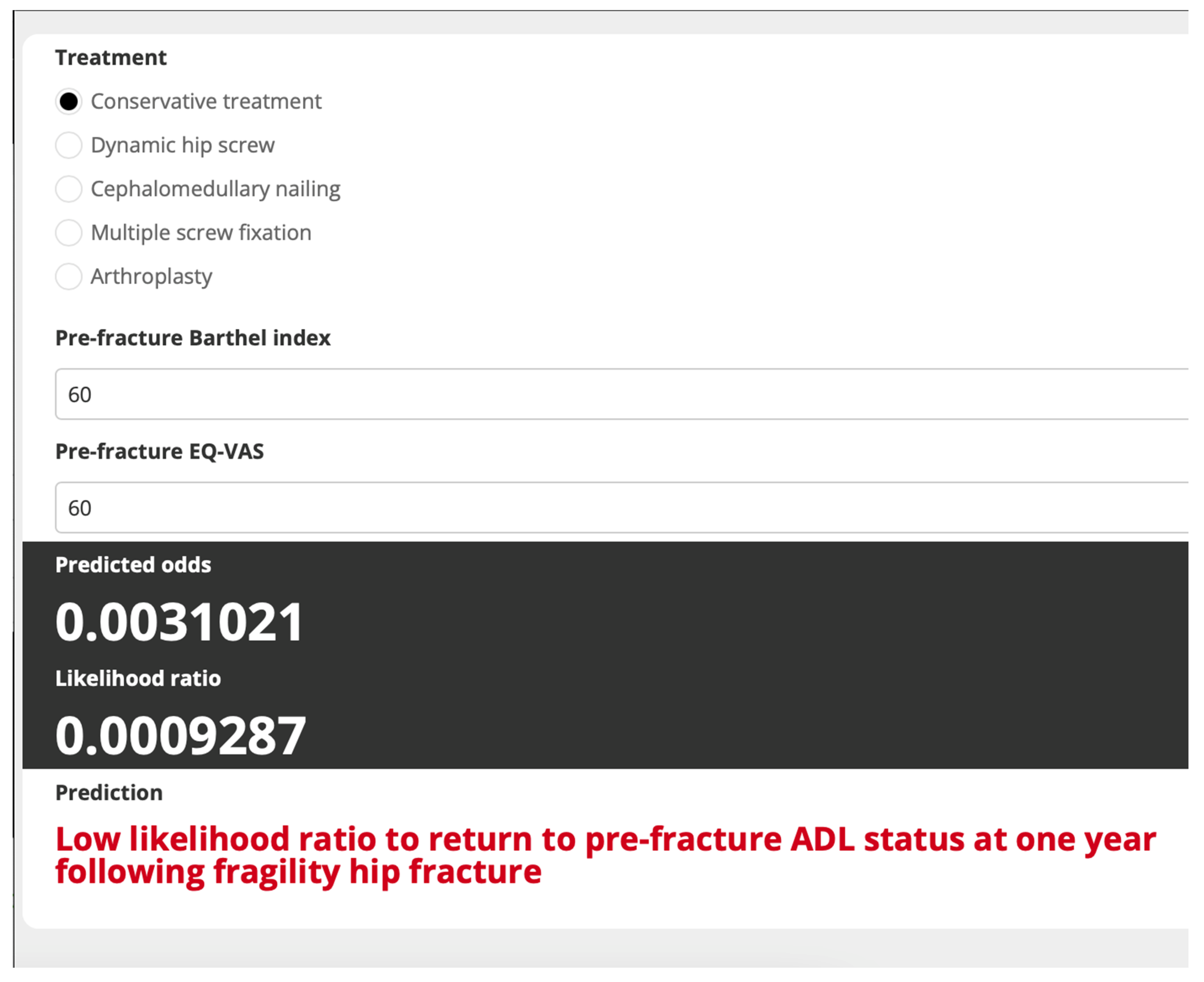
- Scenario 2:
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kanis, J.A.; McCloskey, E.V.; Johansson, H.; Cooper, C.; Rizzoli, R.; Reginster, J.Y. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos. Int. 2013, 24, 23–57. [Google Scholar] [CrossRef] [PubMed]
- Chapurlat, R.D.; Bauer, D.C.; Nevitt, M.; Stone, K.; Cummings, S.R. Incidence and risk factors for a second hip fracture in elderly women. The Study of Osteoporotic Fractures. Osteoporos. Int. 2003, 14, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Center, J.R.; Nguyen, T.V.; Schneider, D.; Sambrook, P.N.; Eisman, J.A. Mortality after all major types of osteoporotic fracture in men and women: An observational study. Lancet 1999, 353, 878–882. [Google Scholar] [CrossRef] [PubMed]
- Peek-Asa, C.; Zwerling, C. Role of environmental interventions in injury control and prevention. Epidemiol. Rev. 2003, 25, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Vaseenon, T.; Luevitoonvechkij, S.; Wongtriratanachai, P.; Rojanasthien, S. Long-term mortality after osteoporotic hip fracture in Chiang Mai, Thailand. J. Clin. Densitom. 2010, 13, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Vochteloo, A.J.; Moerman, S.; Tuinebreijer, W.E.; Maier, A.B.; de Vries, M.R.; Bloem, R.M.; Nelissen, R.G.; Pilot, P. More than half of hip fracture patients do not regain mobility in the first postoperative year. Geriatr. Gerontol. Int. 2013, 13, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Colón-Emeric, C.; Kuchibhatla, M.; Pieper, C.; Hawkes, W.; Fredman, L.; Magaziner, J.; Zimmerman, S.; Lyles, K.W. The contribution of hip fracture to risk of subsequent fractures: Data from two longitudinal studies. Osteoporos. Int. 2003, 14, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Aubrun, F. Hip fracture surgery in the elderly patient: Epidemiological data and risk factors. Ann. Fr. Anesth. Reanim. 2011, 30, e37–e39. [Google Scholar] [CrossRef]
- Gullberg, B.; Johnell, O.; Kanis, J.A. World-wide projections for hip fracture. Osteoporos. Int. 1997, 7, 407–413. [Google Scholar] [CrossRef]
- Wongtriratanachai, P.; Luevitoonvechkij, S.; Songpatanasilp, T.; Sribunditkul, S.; Leerapun, T.; Phadungkiat, S.; Rojanasthien, S. Increasing incidence of hip fracture in Chiang Mai, Thailand. J. Clin. Densitom. 2013, 16, 347–352. [Google Scholar] [CrossRef]
- Sukchokpanich, P.; Anusitviwat, C.; Jarusriwanna, A.; Kitcharanant, N.; Unnanuntana, A. Quality of Life and Depression Status of Caregivers of Patients with Femoral Neck or Intertrochanteric Femoral Fractures during the First Year after Fracture Treatment. Orthop. Surg. 2023, 15, 1854–1861. [Google Scholar] [CrossRef] [PubMed]
- Scaf-Klomp, W.; van Sonderen, E.; Sanderman, R.; Ormel, J.; Kempen, G.I. Recovery of physical function after limb injuries in independent older people living at home. Age Ageing 2001, 30, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Magaziner, J.; Hawkes, W.; Hebel, J.R.; Zimmerman, S.I.; Fox, K.M.; Dolan, M.; Felsenthal, G.; Kenzora, J. Recovery from hip fracture in eight areas of function. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M498–M507. [Google Scholar] [CrossRef] [PubMed]
- Huusko, T.M.; Karppi, P.; Avikainen, V.; Kautiainen, H.; Sulkava, R. Intensive geriatric rehabilitation of hip fracture patients: A randomized, controlled trial. Acta Orthop. Scand. 2002, 73, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Wawruch, M.; Krcmery, S.; Bozekova, L.; Wsolova, L.; Lassan, S.; Slobodova, Z.; Kriska, M. Factors influencing prognosis of pneumonia in elderly patients. Aging Clin. Exp. Res. 2004, 16, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Mahaisavariya, C.; Vanitcharoenkul, E.; Kitcharanant, N.; Chotiyarnwong, P.; Unnanuntana, A. Exploring the osteoporosis treatment gap after fragility hip fracture at a Tertiary University Medical Center in Thailand. BMC Geriatr. 2023, 23, 70. [Google Scholar] [CrossRef] [PubMed]
- Sinoff, G.; Ore, L. The Barthel activities of daily living index: Self-reporting versus actual performance in the old-old (> or = 75 years). J. Am. Geriatr. Soc. 1997, 45, 832–836. [Google Scholar] [CrossRef]
- Unnanuntana, A.; Jarusriwanna, A.; Nepal, S. Validity and responsiveness of Barthel index for measuring functional recovery after hemiarthroplasty for femoral neck fracture. Arch. Orthop. Trauma Surg. 2018, 138, 1671–1677. [Google Scholar] [CrossRef] [PubMed]
- Della Pietra, G.L.; Savio, K.; Oddone, E.; Reggiani, M.; Monaco, F.; Leone, M.A. Validity and reliability of the Barthel index administered by telephone. Stroke 2011, 42, 2077–2079. [Google Scholar] [CrossRef]
- Kim, S.; Won, C.W.; Kim, B.S.; Kim, S.; Yoo, J.; Byun, S.; Jang, H.C.; Cho, B.L.; Son, S.J.; Lee, J.H.; et al. EuroQol Visual Analogue Scale (EQ-VAS) as a Predicting Tool for Frailty in Older Korean Adults: The Korean Frailty an Aging Cohort Study (KFACS). J. Nutr. Health Aging 2018, 22, 1275–1280. [Google Scholar] [CrossRef]
- Kitcharanant, N.; Atthakomol, P.; Khorana, J.; Phinyo, P.; Unnanuntana, A. Prognostic Factors for Functional Recovery at 1-Year Following Fragility Hip Fractures. Clin. Orthop. Surg. 2024, 16, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Mathew, R.O.; Hsu, W.H.; Young, Y. Effect of comorbidity on functional recovery after hip fracture in the elderly. Am. J. Phys. Med. Rehabil. 2013, 92, 686–696. [Google Scholar] [CrossRef] [PubMed]
- Amarilla-Donoso, F.J.; Roncero-Martin, R.; Lavado-Garcia, J.M.; Toribio-Felipe, R.; Moran-Garcia, J.M.; Lopez-Espuela, F. Quality of life after hip fracture: A 12-month prospective study. PeerJ 2020, 8, e9215. [Google Scholar] [CrossRef] [PubMed]
- Shyu, Y.I.; Chen, M.C.; Liang, J.; Lu, J.F.; Wu, C.C.; Su, J.Y. Changes in quality of life among elderly patients with hip fracture in Taiwan. Osteoporos. Int. 2004, 15, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.E.; Huang, K.C.; Lin, T.C.; Tong, K.M.; Lee, M.H.; Chiu, Y.C. Integrated risk scoring model for predicting dynamic hip screw treatment outcome of intertrochanteric fracture. Injury 2016, 47, 2501–2506. [Google Scholar] [CrossRef] [PubMed]
- Phruetthiphat, O.A.; Pinijprapa, P.; Satravaha, Y.; Kitcharanant, N.; Pongchaiyakul, C. An innovative scoring system for predicting an excellent Harris hip score after proximal femoral nail anti-rotation in elderly patients with intertrochanteric fracture. Sci. Rep. 2022, 12, 19939. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, R.; Umehara, T.; Fujimura, T.; Ozawa, J. Clinical Prediction Rule for Declines in Activities of Daily Living at 6 Months After Surgery for Hip Fracture Repair. Arch. Phys. Med. Rehabil. 2016, 97, 2076–2084. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, K.J.; Williamson, L.; Alexander, J.; Filliter, C.; Sobolev, B.; Guy, P.; Bearne, L.M.; Sackley, C. Prognostic factors of functional outcome after hip fracture surgery: A systematic review. Age Ageing 2018, 47, 661–670. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.K.; Matchar, D.B.; Chong, J.L.; Yeo, W.; Howe, T.S.; Koh, J.S.B. Pre-discharge prognostic factors of physical function among older adults with hip fracture surgery: A systematic review. Osteoporos. Int. 2019, 30, 929–938. [Google Scholar] [CrossRef]
- Kim, J.L.; Jung, J.S.; Kim, S.J. Prediction of Ambulatory Status After Hip Fracture Surgery in Patients Over 60 Years Old. Ann. Rehabil. Med. 2016, 40, 666–674. [Google Scholar] [CrossRef]
- Malhotra, R.; Huq, S.S.; Chong, M.; Murphy, D.; Daruwalla, Z.J. Outcomes in Nonagenarians with Hip Fractures Treated Conservatively and Surgically. Malays. Orthop. J. 2021, 15, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Mayoral, A.P.; Ibarz, E.; Gracia, L.; Mateo, J.; Herrera, A. The use of Barthel index for the assessment of the functional recovery after osteoporotic hip fracture: One year follow-up. PLoS ONE 2019, 14, e0212000. [Google Scholar] [CrossRef] [PubMed]
- Bliemel, C.; Sielski, R.; Doering, B.; Dodel, R.; Balzer-Geldsetzer, M.; Ruchholtz, S.; Buecking, B. Pre-fracture quality of life predicts 1-year survival in elderly patients with hip fracture-development of a new scoring system. Osteoporos. Int. 2016, 27, 1979–1987. [Google Scholar] [CrossRef] [PubMed]
- Trovarelli, G.; Crimì, A.; Mori, F.; De Martini, N.F.; Cerchiaro, M.C.; Ruggieri, P. Proximal femur fractures in elderly patients: Gender-related differences in survival and functional outcomes. J. Sex-Gend.-Specif. Med. 2023, 9, 69–75. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Return to Prefracture Activities-of-Daily-Living Status (n = 324) | Did Not Return to Prefracture Activities-of-Daily-Living Status (n = 97) | Odds Ratio | 95% CI | p-Value | auROC |
|---|---|---|---|---|---|---|
| Age (y), mean ± SD | 77.33 ± 9.65 | 81.35 ± 8.39 | 0.95 | [0.93–0.98] | <0.001 | 0.61 [0.55–0.67] |
| Female sex, n (%) | 242 (74.69%) | 76 (78.35%) | 0.82 | [0.47–1.41] | 0.463 | 0.52 [0.47–0.57] |
| Body mass index (kg/m2), mean ± SD | 22.68 ± 4.11 | 22.12 ± 4.02 | 1.03 | [0.98–1.10] | 0.24 | 0.54 [0.47–0.60] |
| Charlson comorbidity index score, n (%) | ||||||
| –<5 | 178 (54.94%) | 31 (31.96%) | 2.6 | [1.61–4.19] | <0.001 | 0.61 [0.56–0.67] |
| Type of fracture, n (%) | ||||||
| –Femoral neck fracture | 178 (54.94%) | 46 (47.42%) | 1.35 | [0.86–2.13] | 0.19 | 0.54 [0.48–0.59] |
| Treatment, n (%) | ||||||
| –Conservative treatment | 3 (0.93%) | 14 (14.43%) | 0.60 [0.53–0.66] | |||
| –Dynamic hip screw | 21 (6.48%) | 6 (6.19%) | 16.33 | [3.49–76.35] | <0.001 | |
| –Cephalomedullary nailing | 133 (41.05%) | 40 (41.24%) | 15.52 | [4.25–56.71] | <0.001 | |
| –Multiple screw fixation | 14 (4.32%) | 2 (2.06%) | 32.67 | [4.71–226.52] | <0.001 | |
| –Arthroplasty | 153 (47.22%) | 35 (36.08%) | 20.4 | [5.56–74.85] | <0.001 | |
| Prefracture BI, mean ± SD | 96.7 ± 6.02 | 80.72 ± 17.79 | 1.16 | [1.12–1.20] | <0.001 | 0.83 [0.79–0.88] |
| Prefracture EQ-VAS, mean ± SD | 92.48 ± 7.75 | 79.18 ± 16.29 | 1.11 | [1.08–1.14] | <0.001 | 0.76 [0.70–0.82] |
| Predictors | Terms | df | Formula | Log Odds Ratio | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| Intercept | 0.26 | −1.25, 1.76 | 0.739 | |||
| Age | Out | 0 | – | – | – | – |
| CCI | Out | 0 | – | – | – | – |
| Treatment | Linear | 1 | ||||
| –Dynamic hip screw | 2.14 | 0.29, 3.98 | 0.02 | |||
| –Cephalomedullary nailing | 2.06 | 0.53, 3.6 | 0.01 | |||
| –Multiple screw fixation | 3.3 | 0.48, 6.12 | 0.02 | |||
| –Arthroplasty | 2.08 | 0.54, 3.62 | 0.01 | |||
| Prefracture Barthel index | Linear | 1 | Prefracture Barthel index-100 | 0.12 | 0.08, 0.16 | <0.001 |
| Prefracture EQ-VAS | Linear | 1 | Prefracture EQ-VAS-90 | 0.04 | 0.001, 0.07 | 0.045 |
| Categories | LHR to Return to Prefracture Activties-of-Daily-Living Status | Return to Prefracture Activities-of-Daily-Living Status | Did Not Return to Prefracture Activities-of-Daily-Living Status | LR+ | 95% CI of LR+ | PPV | 95% CI of PPV | p-Value | ||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | |||||||
| Low | <1.3 | 68 | 21 | 79 | 81.4 | 0.26 | 0.20 0.32 | 46.3% | 38.0% 54.7% | <0.001 |
| High | ≥1.3 | 256 | 79 | 18 | 18.6 | 4.26 | 2.80 6.48 | 93.4% | 89.8% 96.1% | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitcharanant, N.; Atthakomol, P.; Khorana, J.; Phinyo, P.; Unnanuntana, A. Predictive Model of Recovery to Prefracture Activities-of-Daily-Living Status One Year after Fragility Hip Fracture. Medicina 2024, 60, 615. https://doi.org/10.3390/medicina60040615
Kitcharanant N, Atthakomol P, Khorana J, Phinyo P, Unnanuntana A. Predictive Model of Recovery to Prefracture Activities-of-Daily-Living Status One Year after Fragility Hip Fracture. Medicina. 2024; 60(4):615. https://doi.org/10.3390/medicina60040615
Chicago/Turabian StyleKitcharanant, Nitchanant, Pichitchai Atthakomol, Jiraporn Khorana, Phichayut Phinyo, and Aasis Unnanuntana. 2024. "Predictive Model of Recovery to Prefracture Activities-of-Daily-Living Status One Year after Fragility Hip Fracture" Medicina 60, no. 4: 615. https://doi.org/10.3390/medicina60040615