
Meditation Moderates the Relationship between Insecure Attachment and Loneliness: A Study of Long-Term Care Residents in Thailand
 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.2.1. The 18-Item Experiences of Close Relationships—Revised (ECR-R-18)
2.2.2. The 6-Item Revised University of California Los Angeles Loneliness Scale (RULS-6)
2.2.3. The Inner Strength-Based Inventory (i-SBI)
2.3. Statistical Analysis
3. Results
3.1. Demographic Information
3.2. Attachment, Meditation, and Loneliness Scores
3.3. Correlation of Variables
4. Discussion
4.1. Clinical Implications
4.2. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ong, A.D.; Uchino, B.N.; Wethington, E. Loneliness and Health in Older Adults: A Mini-Review and Synthesis. Gerontology 2016, 62, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Mansfield, J.; Hazan, H.; Lerman, Y.; Shalom, V. Correlates and predictors of loneliness in older-adults: A review of quantitative results informed by qualitative insights. Int. Psychogeriatr. 2016, 28, 557–576. [Google Scholar] [CrossRef]
- Singh, A.; Misra, N. Loneliness, depression and sociability in old age. Ind. Psychiatry J. 2009, 18, 51–55. [Google Scholar] [CrossRef]
- Peplau, L.A.; Perlman, D. Perspectives on loneliness. In Loneliness: A Sourcebook of Current Theory, Research and Therapy; Peplau, L.A., Perlman, D., Eds.; John Wiley & Sons: New York, NY, USA, 1982; pp. 1–18. [Google Scholar]
- de Jong-Gierveld, J. Developing and testing a model of loneliness. J. Pers. Soc. Psychol. 1987, 53, 119–128. [Google Scholar] [CrossRef]
- World Health Organization. Mental Health of Older Adults. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-health-of-older-adults (accessed on 14 March 2024).
- Huang, P.-H.; Wang, S.-Y.; Hu, S.H.; Chuang, Y.-H. Older residents’ perceptions of loneliness in long-term care facilities: A qualitative study. Int. J. Ment. Health Nurs. 2022, 31, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Hawkley, L.C.; Masi, C.M.; Berry, J.D.; Cacioppo, J.T. Loneliness is a unique predictor of age-related differences in systolic blood pressure. Psychol. Aging 2006, 21, 152. [Google Scholar] [CrossRef] [PubMed]
- Leigh-Hunt, N.; Bagguley, D.; Bash, K.; Turner, V.; Turnbull, S.; Valtorta, N.; Caan, W. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health 2017, 152, 157–171. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Hawkley, L.C.; Berntson, G.G. The anatomy of loneliness. Curr. Dir. Psychol. Sci. 2003, 12, 71–74. [Google Scholar] [CrossRef]
- Brown, E.G.; Gallagher, S.; Creaven, A.-M. Loneliness and acute stress reactivity: A systematic review of psychophysiological studies. Psychophysiology 2018, 55, e13031. [Google Scholar] [CrossRef] [PubMed]
- Lara, E.; Caballero, F.F.; Rico-Uribe, L.A.; Olaya, B.; Haro, J.M.; Ayuso-Mateos, J.L.; Miret, M. Are loneliness and social isolation associated with cognitive decline? Int. J. Geriatr. Psychiatry 2019, 34, 1613–1622. [Google Scholar] [CrossRef]
- Wilson, R.S.; Krueger, K.R.; Arnold, S.E.; Schneider, J.A.; Kelly, J.F.; Barnes, L.L.; Tang, Y.; Bennett, D.A. Loneliness and risk of Alzheimer disease. Arch. Gen. Psychiatry 2007, 64, 234–240. [Google Scholar] [CrossRef]
- Liu, J.; Wei, W.; Peng, Q.; Xue, C.; Yang, S. The roles of life satisfaction and community recreational facilities in the relationship between loneliness and depression in older adults. Clin. Gerontol. 2022, 45, 376–389. [Google Scholar] [CrossRef]
- Chawla, K.; Kunonga, T.P.; Stow, D.; Barker, R.; Craig, D.; Hanratty, B. Prevalence of loneliness amongst older people in high-income countries: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0255088. [Google Scholar] [CrossRef]
- Wang, J.; Zhou, Y.; Zhang, Q.; Li, J.; Zhai, D.; Li, J.; Han, B.; Liu, Z. Loneliness among older Chinese individuals: The status quo and relationships with activity-related factors. BMC Geriatr. 2024, 24, 42. [Google Scholar] [CrossRef]
- Huang, P.H.; Chi, M.J.; Kuo, C.L.; Wu, S.V.; Chuang, Y.H. Prevalence of Loneliness and Related Factors Among Older Adults in Taiwan: Evidence From a Nationally Representative Survey. Inquiry 2021, 58, 469580211035745. [Google Scholar] [CrossRef]
- Victor, C.R. Loneliness in care homes: A neglected area of research? Aging Health 2012, 8, 637–646. [Google Scholar] [CrossRef]
- Elias, S.M.S. Prevalence of loneliness, anxiety, and depression among older people living in long-term care: A review. Int. J. Care Sch. 2018, 1, 39–43. [Google Scholar] [CrossRef]
- Gardiner, C.; Laud, P.; Heaton, T.; Gott, M. What is the prevalence of loneliness amongst older people living in residential and nursing care homes? A systematic review and meta-analysis. Age Ageing 2020, 49, 748–757. [Google Scholar] [CrossRef]
- Wongpakaran, N.; Wongpakaran, T. Prevalence of major depressive disorders and suicide in long-term care facilities: A report from northern Thailand. Psychogeriatrics 2012, 12, 11–17. [Google Scholar] [CrossRef]
- Dahlberg, L.; Agahi, N.; Lennartsson, C. Lonelier than ever? Loneliness of older people over two decades. Arch. Gerontol. Geriatr. 2018, 75, 96–103. [Google Scholar] [CrossRef]
- Spence, R.; Jacobs, C.; Bifulco, A. Attachment style, loneliness and depression in older age women. Aging Ment. Health 2020, 24, 837–839. [Google Scholar] [CrossRef] [PubMed]
- Zuo, S.; Lin, L.; Chen, S.; Wang, Z.; Tian, L.; Li, H.; Xu, Y. Influencing factors of loneliness among older adults in China: A systematic review and meta-analysis. Psychogeriatrics 2023, 23, 164–176. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R. An attachment perspective on loneliness. In The Handbook of Solitude: Psychological Perspectives on Social Isolation, Social Withdrawal, and Being Alone; Wiley Blackwell: Hoboken, NJ, USA, 2014; pp. 34–50. [Google Scholar]
- Arunrasameesopa, S.; Wongpakaran, N.; Wongpakaran, T. Influence of Attachment Anxiety on the Relationship between Loneliness and Depression among Long-Term Care Residents. Healthcare 2021, 9, 1675. [Google Scholar] [CrossRef]
- Bowlby, J. Attachment and Loss, Vol. 1: Attachment; Basic Books: New York, NY, USA, 1969. [Google Scholar]
- Brennan, K.A.; Clark, C.L.; Shaver, P.R. Self-report measurement of adult attachment: An integrative overview. In Attachment Theory and Close Relationships; The Guilford Press: New York, NY, USA, 1998; pp. 46–76. [Google Scholar]
- Karantzas, G.C.; Feeney, J.A.; Wilkinson, R. Is less more? Confirmatory factor analysis of the Attachment Style Questionnaires. J. Soc. Pers. Relat. 2010, 27, 749–780. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R.; Pereg, D. Attachment theory and affect regulation: The dynamics, development, and cognitive consequences of attachment-related strategies. Motiv. Emot. 2003, 27, 77–102. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R. Attachment in Adulthood: Structure, Dynamics, and Change; The Guilford Press: New York, NY, USA, 2007; p. 578. [Google Scholar]
- Shaver, P.R.; Mikulincer, M. Adult Attachment Strategies and the Regulation of Emotion. In Handbook of Emotion Regulation; Gross, J.J., Ed.; The Guilford Press: New York, NY, USA, 2007; pp. 446–465. [Google Scholar]
- Teo, R.H.; Cheng, W.H.; Cheng, L.J.; Lau, Y.; Lau, S.T. Global prevalence of social isolation among community-dwelling older adults: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2023, 107, 104904. [Google Scholar] [CrossRef] [PubMed]
- Klangrit, S.; Perrodin, D.D.; Siripaprapakon, Y.; Choudhry, F.R.; Intaranggkul, T.; Pratoomkaew, S.; Khemsiri, K.; Saengrung, K.; Vachirayano, W. Religion and mental health among older adults in Thailand: A national survey study. Ment. Health Rev. J. 2021, 26, 380–391. [Google Scholar] [CrossRef]
- Bond, K.; Ospina, M.B.; Hooton, N.; Bialy, L.; Dryden, D.M.; Buscemi, N.; Shannahoff-Khalsa, D.; Dusek, J.; Carlson, L.E. Defining a complex intervention: The development of demarcation criteria for “meditation”. Psychol. Relig. Spiritual. 2009, 1, 129–137. [Google Scholar] [CrossRef]
- Matko, K.; Sedlmeier, P. What Is Meditation? Proposing an Empirically Derived Classification System. Front. Psychol. 2019, 10, 2276. [Google Scholar] [CrossRef]
- Komariah, M.; Ibrahim, K.; Pahria, T.; Rahayuwati, L.; Somantri, I. Effect of Mindfulness Breathing Meditation on Depression, Anxiety, and Stress: A Randomized Controlled Trial among University Students. Healthcare 2022, 11, 26. [Google Scholar] [CrossRef]
- DeMaranville, J.; Wongpakaran, T.; Wongpakaran, N.; Wedding, D. The Mediating Role of Precepts and Meditation on Attachment and Depressive Symptoms in Adolescents. Healthcare 2023, 11, 1923. [Google Scholar] [CrossRef]
- Schoemann, A.M.; Boulton, A.J.; Short, S.D. Monte Carlo Power Analysis for Indirect Effects. Available online: https://schoemanna.shinyapps.io/mc_power_med/ (accessed on 14 March 2024).
- Schoemann, A.M.; Boulton, A.J.; Short, S.D. Determining power and sample size for simple and complex mediation models. Soc. Psychol. Personal. Sci. 2017, 8, 379–386. [Google Scholar] [CrossRef]
- Fraley, R.C.; Waller, N.G.; Brennan, K.A. An item response theory analysis of self-report measures of adult attachment. J. Personal. Soc. Psychol. 2000, 78, 350. [Google Scholar] [CrossRef] [PubMed]
- Wongpakaran, T.; Wongpakaran, N. A short version of the revised ‘Experience of Close Relationships Questionnaire’: Investigating non-clinical and clinical samples. Clin. Pract. Epidemiol. Ment. Health 2012, 8, 36. [Google Scholar] [CrossRef]
- Russell, D.; Peplau, L.A.; Cutrona, C.E. The revised UCLA Loneliness Scale: Concurrent and discriminant validity evidence. J. Personal. Soc. Psychol. 1980, 39, 472–480. [Google Scholar] [CrossRef]
- Wongpakaran, N.; Wongpakaran, T.; Pinyopornpanish, M.; Simcharoen, S.; Suradom, C.; Varnado, P.; Kuntawong, P. Development and validation of a 6-item Revised UCLA Loneliness Scale (RULS-6) using Rasch analysis. Br. J. Health Psychol. 2020, 25, 233–256. [Google Scholar] [CrossRef]
- Buddhaghosa, H. The Path of Purification: Visuddhimaga (tr. by Ñānamoli, 794 p); Buddhist Publication Society: Kandy, Sri Lanka, 2010. [Google Scholar]
- Wongpakaran, N.; Wongpakaran, T.; Kuntawong, P. Development and validation of the (inner) Strength-Based Inventory. Ment. Health Relig. Cult. 2020, 23, 263–273. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Press: New York, NY, USA, 2018; p. xvii, 507. [Google Scholar]
- Soper, D.; Interaction. Interaction–Home—Windows Software for Graphing and Analyzing Statistical Interactions. Available online: https://danielsoper.com (accessed on 16 March 2024).
- West, T.N.; Don, B.P.; Fredrickson, B.L. Attachment insecurity moderates emotion responses to mindfulness and loving-kindness meditation in adults raised in low socioeconomic status households. Emotion 2022, 22, 1101–1118. [Google Scholar] [CrossRef]
- Saini, G.K.; Haseeb, S.B.; Taghi-Zada, Z.; Ng, J.Y. The effects of meditation on individuals facing loneliness: A scoping review. BMC Psychol. 2021, 9, 88. [Google Scholar] [CrossRef] [PubMed]
- Pandya, S.P. Meditation program mitigates loneliness and promotes wellbeing, life satisfaction and contentment among retired older adults: A two-year follow-up study in four South Asian cities. Aging Ment. Health 2021, 25, 286–298. [Google Scholar] [CrossRef] [PubMed]
- Garofalo, C.; Bogaerts, S. Attachment and Personality Disorders Among Child Molesters: The Role of Trust. Sex. Abus. 2019, 31, 97–124. [Google Scholar] [CrossRef]
- Keng, S.L.; Tan, H.H. Effects of brief mindfulness and loving-kindness meditation inductions on emotional and behavioral responses to social rejection among individuals with high borderline personality traits. Behav. Res. Ther. 2018, 100, 44–53. [Google Scholar] [CrossRef]
- Bremer, B.; Wu, Q.; Mora Álvarez, M.G.; Hölzel, B.K.; Wilhelm, M.; Hell, E.; Tavacioglu, E.E.; Torske, A.; Koch, K. Mindfulness meditation increases default mode, salience, and central executive network connectivity. Sci. Rep. 2022, 12, 13219. [Google Scholar] [CrossRef] [PubMed]
- Preece, D.A.; Goldenberg, A.; Becerra, R.; Boyes, M.; Hasking, P.; Gross, J.J. Loneliness and emotion regulation. Personal. Individ. Differ. 2021, 180, 110974. [Google Scholar] [CrossRef]
- Christoffersen, L.A.; Helenius, D.; Schwinn, M.; Erikstrup, C.; Hjalgrim, H.; Nissen, J.; Banasik, K.; Nielsen, K.; Kaspersen, K.A.; Dinh, K.M.; et al. Experience of loneliness during the COVID-19 pandemic: A cross-sectional study of 50,968 adult Danes. BMJ Open 2023, 13, e064033. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | n | % |
|---|---|---|
| Age: mean ± SD | 73.52 ± 7.32 | |
| Sex | ||
| Female | 136 | 57.6 |
| Male | 100 | 42.4 |
| Marital Status | ||
| Single | 109 | 46.4 |
| Married | 14 | 6.0 |
| Divorced | 29 | 12.3 |
| Widowed | 83 | 35.3 |
| Education | ||
| Unschooled | 18 | 7.6 |
| Primary School | 124 | 52.5 |
| High School | 53 | 22.5 |
| Bachelor’s Degree | 39 | 16.5 |
| Postgraduate | 2 | 0.8 |
| Instruments | Mean ± SD or n (%) |
|---|---|
| ECR-R Avoidance (1–7) | 3.46 ± 1.28 |
| ECR-R Anxiety (1–7) | 3.92 ± 1.40 |
| RULS Loneliness (1–6) | 13.64 ± 4.17 |
| i-SBI Meditation (1–5) | 2.92 ± 1.17 |
| Rarely if ever | 25 (10.6) |
| Occasionally | 73 (30.9) |
| Often but not daily | 56 (23.7) |
| Everyday | 59 (25.0) |
| Daily multiple times | 23 (9.7) |
| Items | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| 1. Age | - | |||||||
| 2. Sex (Female) | 0.270 ** | - | ||||||
| (0.147, 0.384) | ||||||||
| 3. Marital status (Married) | −0.0092 | −0.031 | - | |||||
| (−0.217, 0.036) | (−0.158, 0.097) | |||||||
| 4. Education (Higher) | 0.012 | −0.073 | 0.114 | - | ||||
| (−0.116, 0.140) | (−0.199, 0.055) | (−0.014, 0.239) | ||||||
| 5. ECR-R Avoidance (1–7) | 0.013 | −0.028 | 0.047 | 0.027 | - | |||
| (−0.115, 0.140) | (−0.156, 0.100) | (−0.081, 0.174) | (−0.101, 0.154) | |||||
| 6. ECR-R Anxiety (1–7) | −0.187 ** | −0.163 * | 0.002 | −0.055 | −0.428 ** | - | ||
| (−0.307, −0.061) | (−0.285, −0.306) | (−0.126, 0.130) | (−0.181, 0.074) | (−0.527, −0.318) | ||||
| 7. RULS Loneliness (1–6) | 0.105 | 0.005 | −0.088 | −0.028 | 0.011 | 0.199 ** | - | |
| (−0.023, 0.230) | (−0.123, 0.133) | (−0.214, 0.040) | (−0.155, 0.100) | (−0.117, 0.138) | (0.098, 0.157) | |||
| 8. i-SBI Meditation (1–5) | 0.020 | 0.054 | −0.041 | 0.001 | −0.226 ** | 0.030 | −0.177 ** | |
| (−0.108, 0.147) | (−0.074, 0.181) | (−0.168, 0.087) | (−0.126, 0.129) | (−0.344, −0.101) | (−0.098, 0.157) | (−0.298, −0.051) |
| Model | B | SE | t | p-Value | LLCI | ULCI | |
|---|---|---|---|---|---|---|---|
| 1 | Constant | 11.322 | 0.795 | 14.238 | <0.001 | ||
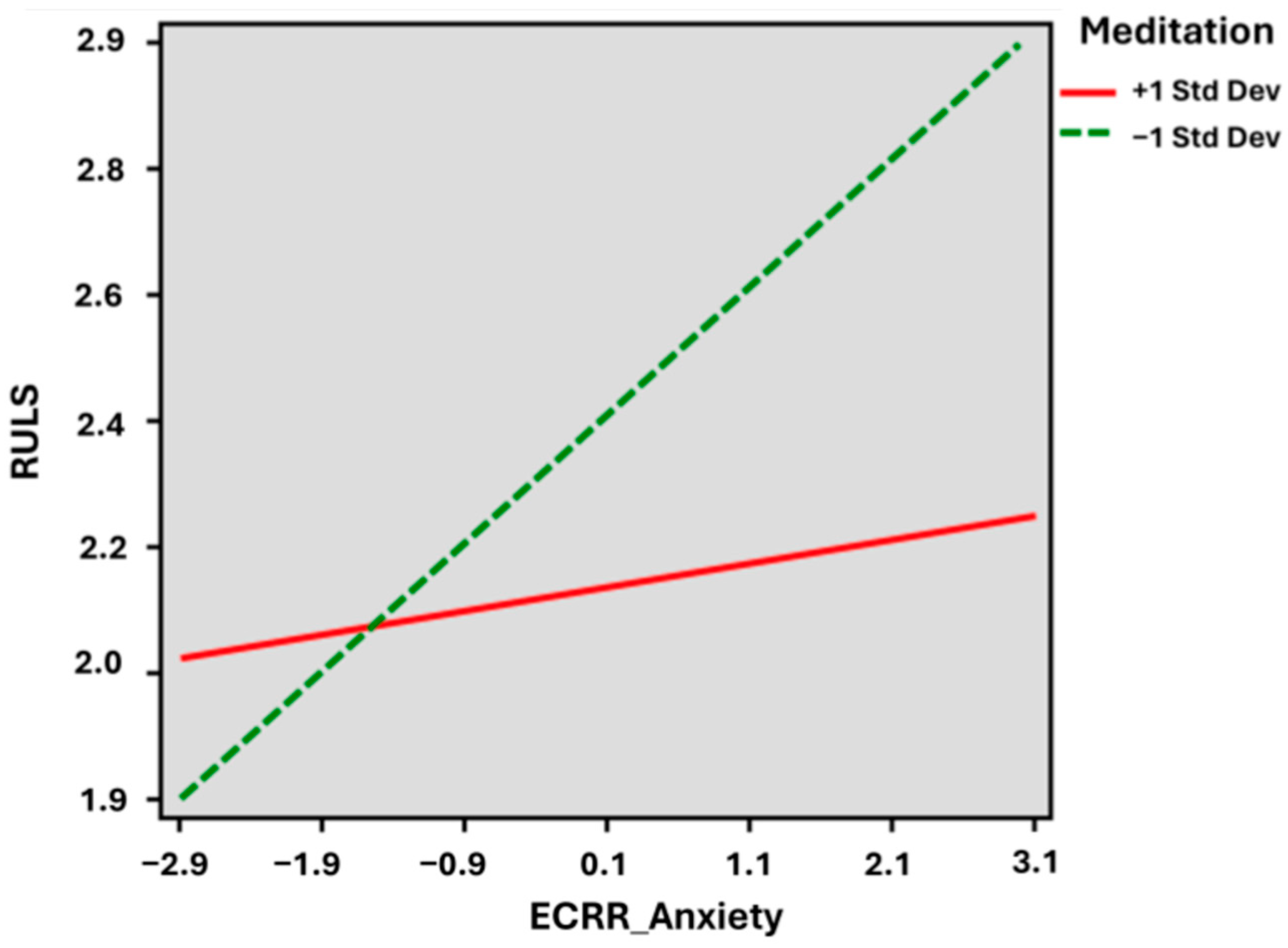
| R2 = 0.039 | (X) ECR-R Anxiety | 0.592 | 0.191 | 3.100 | 0.002 | ||
| 2 | Constant | 8.583 | 2.214 | 3.877 | <0.001 | ||
| R2 = 0.092 | (X) ECR-R Anxiety | 1.724 | 0.527 | 3.267 | 0.001 | 0.6545 | 2.764 |
| (W) i-SBI Meditation | 0.868 | 0.769 | 1.129 | 0.260 | −0.647 | 2.382 | |
| XW [Interaction] | −0.368 | 0.174 | −2.111 | 0.036 | −0.712 | −0.025 | |
| 3 | Constant | 3.297 | 3.517 | 0.937 | 0.350 | −3.634 | 10.229 |
| R2 = 0.119 | (X) ECR-R Anxiety | 1.729 | 0.528 | 3.274 | 0.001 | 0.689 | 2.771 |
| (W) i-SBI Meditation | 0.741 | 0.753 | 0.983 | 0.327 | −0.744 | 2.226 | |
| XW [Interaction] | −0.344 | 0.171 | −2.064 | 0.040 | −0.672 | −0.016 | |
| Age | 0.075 | 0.038 | 2.066 | 0.039 | 0.003 | 0.147 | |
| Gender (Female) | 0.102 | 0.517 | 0.197 | 0.844 | −0.917 | 1.121 | |
| Marital Status (Married) | −0.687 | 0.507 | −1.354 | 0.177 | −1.687 | 0.313 | |
| Education (Higher school) | −0.086 | 0.516 | −0.161 | 0.867 | −1.102 | 0.929 |
| Model | B | SE | t | p-Value | LLCI | ULCI | |
|---|---|---|---|---|---|---|---|
| 1 | Constant | 13.524 | 0.784 | 17.251 | <0.001 | ||
| R2 =−0.004 | (X) ECR-R Avoidance | 0.035 | 0.213 | 0.164 | 0.870 | ||
| 2 | Constant | 20.052 | 2.255 | 8.893 | 0.000 | 15.609 | 24.494 |
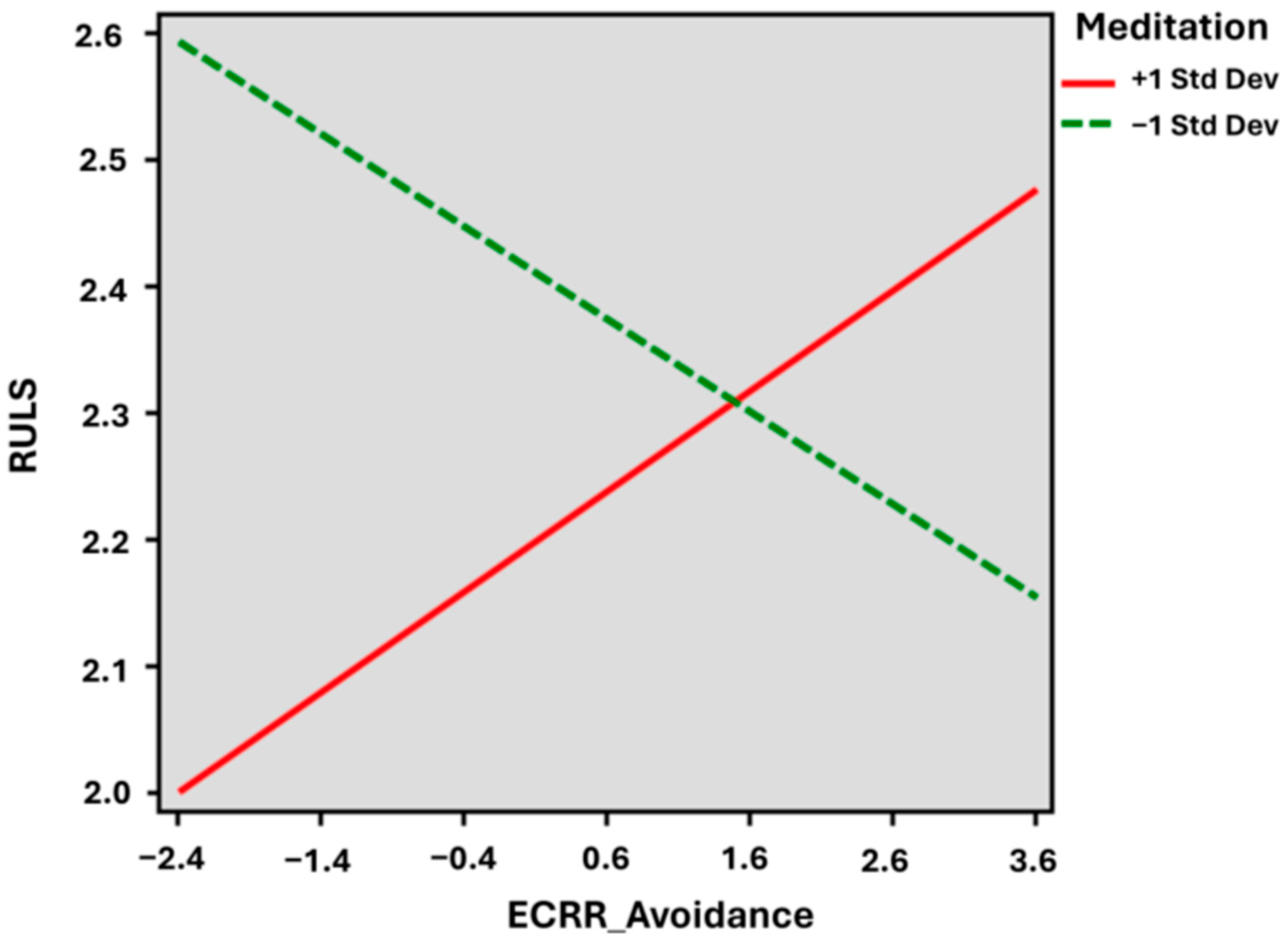
| R2 = 0.051 | (X) ECR-R Avoidance | −1.276 | 0.584 | −2.184 | 0.030 | −2.4265 | −0.1257 |
| (W) i-SBI Meditation | −2.115 | 0.744 | −2.842 | 0.004 | −3.528 | −0.7080 | |
| XW [Interaction] | 0.429 | 0.212 | 2.026 | 0.044 | 0.012 | 0.845 | |
| 3 | Constant | 16.690 | 3.633 | 4.594 | 0.000 | 9.531 | 23.849 |
| R2 = 0.072 | (X) ECR-R Avoidance | −1.309 | 0.586 | −2.236 | 0.026 | −2.463 | −0.156 |
| (W) i-SBI Meditation | −2.182 | 0.718 | −3.039 | 0.003 | −3.643 | −0.719 | |
| XW [Interaction] | 0.444 | 0.210 | 2.113 | 0.036 | 0.030 | 0.857 | |
| Age | 0.057 | 0.037 | 1.525 | 0.129 | −0.017 | 0.131 | |
| Gender (female) | −0.125 | 0.530 | −0.236 | 0.813 | −1.170 | 0.919 | |
| Marital Status (married) | −0.750 | 0.528 | −1.422 | 0.156 | −1.789 | 0.289 | |
| Education (higher school) | −0.297 | 0.537 | −0.553 | 0.581 | −1.354 | 0.761 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khin Moe Myint; DeMaranville, J.; Wongpakaran, T.; Peisah, C.; Arunrasameesopa, S.; Wongpakaran, N. Meditation Moderates the Relationship between Insecure Attachment and Loneliness: A Study of Long-Term Care Residents in Thailand. Medicina 2024, 60, 622. https://doi.org/10.3390/medicina60040622
Khin Moe Myint, DeMaranville J, Wongpakaran T, Peisah C, Arunrasameesopa S, Wongpakaran N. Meditation Moderates the Relationship between Insecure Attachment and Loneliness: A Study of Long-Term Care Residents in Thailand. Medicina. 2024; 60(4):622. https://doi.org/10.3390/medicina60040622
Chicago/Turabian StyleKhin Moe Myint, Justin DeMaranville, Tinakon Wongpakaran, Carmelle Peisah, Suthikarn Arunrasameesopa, and Nahathai Wongpakaran. 2024. "Meditation Moderates the Relationship between Insecure Attachment and Loneliness: A Study of Long-Term Care Residents in Thailand" Medicina 60, no. 4: 622. https://doi.org/10.3390/medicina60040622