

Association between Periodontal Disease and Obesity: Umbrella Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
- − Population: people of all ages.
- − Exposure: people with obesity (BMI ≥ 30 or ≥95th percentile) and/or overweight (BMI ≥ 25 or ≥85th percentile).
- − Comparison: people with normal weight (BMI ≥ 18.5 or ≥5th percentile).
- − Outcomes: association with periodontal disease.
2.2. Eligibility Criteria and Results of Interest
2.3. Sources of Information, Search Strategy, and Additional Search for Primary Studies
2.4. Data Management and Selection Process
2.5. Data Collection Process
2.6. Assessment of Methodological Quality, Quality of Evidence, and Meta-Bias
2.7. Summary of Measures
2.8. Summary of Results
3. Results
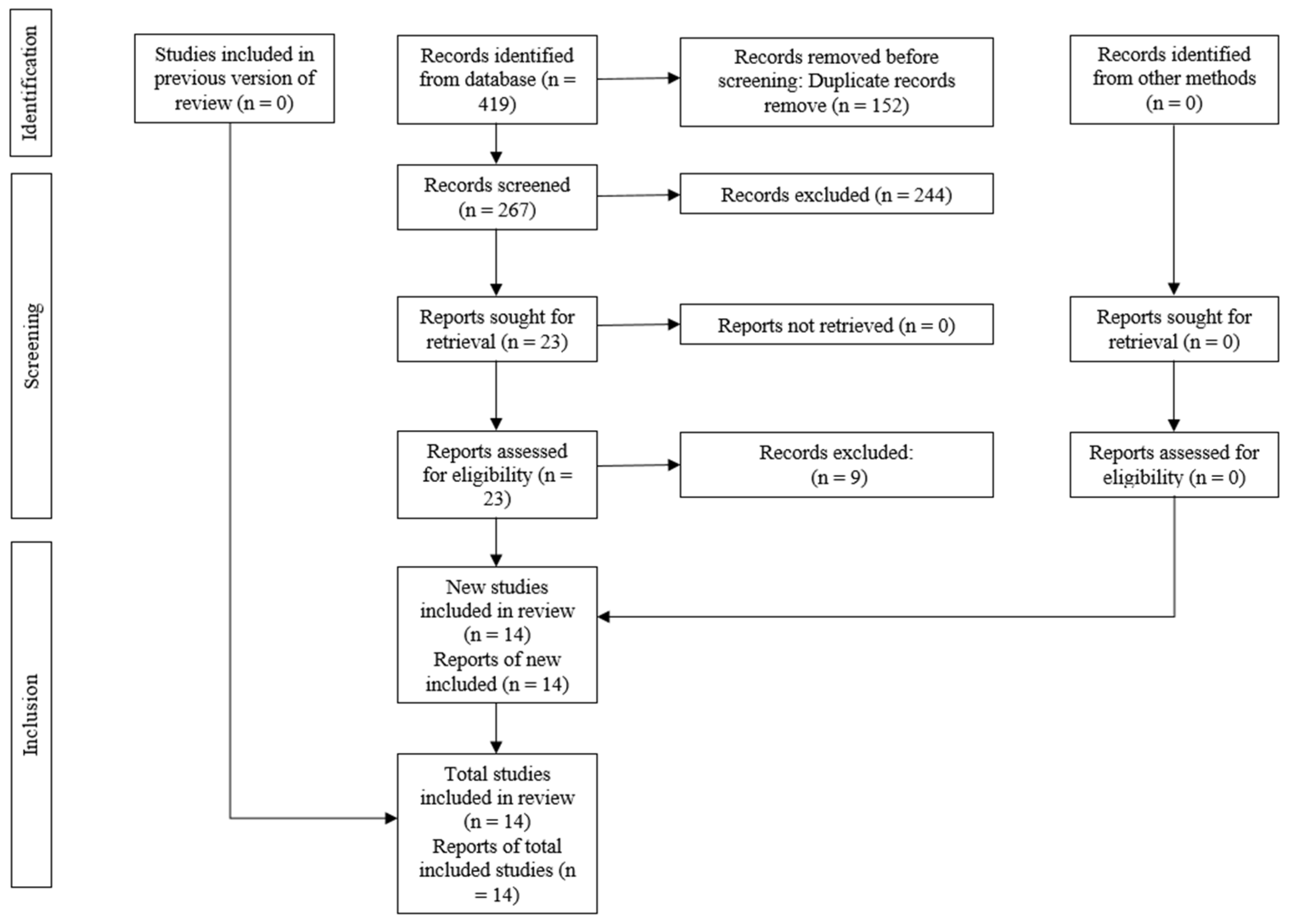
3.1. Review and Selection of Primary Studies
3.2. Review and Characteristics of Included Studies
3.3. Assessment of Methodological Quality and Quality of Evidence
3.4. Overlapping
3.5. Synthesis of Results
3.5.1. General Association
3.5.2. Age
3.5.3. Sex
3.5.4. Country or Continent
3.5.5. Obese
3.5.6. Overweight
3.5.7. Smoker and Non-Smoker
3.5.8. Bleeding on Probing
3.5.9. Gingival Index
3.5.10. Plaque Index
3.5.11. Probing Depth
3.5.12. Subgingival Calculus
3.5.13. Supragingival Calculus
4. Discussion
4.1. Evidence Summary
4.2. Implications for Clinical Practice
4.3. Implications for Research
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lavigne, S.E. Evolving evidence for relationships between periodontitis and systemic diseases: Position paper from the Canadian Dental Hygienists Association. Can. J. Dent. Hyg. 2022, 56, 155–171. [Google Scholar] [PubMed]
- Lavigne, S.E.; Forrest, J.L. An umbrella review of systematic reviews of the evidence of a causal relationship between periodontal disease and cardiovascular diseases: Position paper from the Canadian Dental Hygienists Association. Can. J. Dent. Hyg. 2020, 54, 32–41. [Google Scholar] [PubMed]
- Lavigne, S.E.; Forrest, J.L. An umbrella review of systematic reviews of the evidence of a causal relationship between periodontal disease and adverse pregnancy outcomes: A position paper from the Canadian Dental Hygienists Association. Can. J. Dent. Hyg. 2020, 54, 92–100. [Google Scholar] [PubMed]
- Lavigne, S.E.; Forrest, J.L. An umbrella review of systematic reviews of the evidence of a causal relationship between periodontal microbes and respiratory diseases: Position paper from the Canadian Dental Hygienists Association. Can. J. Dent. Hyg. 2020, 54, 144–155. [Google Scholar] [PubMed]
- Lavigne, S.E.; Forrest, J.L. An umbrella review of systematic reviews examining the relationship between type 2 diabetes and periodontitis: Position paper from the Canadian Dental Hygienists Association. Can. J. Dent. Hyg. 2021, 55, 57–67. [Google Scholar]
- Tonetti, M.S.; Van Dyke, T.E.; Working Group 1 of the Joint EFP/AAP Workshop. Periodontitis and atherosclerotic cardiovascular disease: Consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 84, S24–S29. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.C.; Genco, R.; Working Group 2 of the Joint EFP/AAP Workshop. Diabetes and periodontal diseases: Consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 84, S106–S112. [Google Scholar] [CrossRef]
- Sanz, M.; Kornman, K.; Working Group 3 of the Joint EFP/AAP Workshop. Periodontitis and adverse pregnancy outcomes: Consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 84, S164–S169. [Google Scholar] [CrossRef] [PubMed]
- Linden, G.J.; Herzberg, M.C.; Working Group 4 of the Joint EFP/AAP Workshop. Periodontitis and systemic diseases: A record of discussions of working group 4 of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Clin. Periodontol. 2013, 40, S20–S23. [Google Scholar] [CrossRef]
- Linden, G.J.; Lyons, A.; Scannapieco, F.A. Periodontal systemic associations: Review of the evidence. J. Clin. Periodontol. 2013, 40, S8–S19. [Google Scholar] [CrossRef]
- Monsarrat, P.; Blaizot, A.; Kémoun, P.; Ravaud, P.; Nabet, C.; Sixou, M.; Vergnes, J.-N. Clinical research activity in periodontal medicine: A systematic mapping of trial registers. J. Clin. Periodontol. 2016, 43, 390–400. [Google Scholar] [CrossRef] [PubMed]
- Ebbeling, C.B.; Pawlak, D.B.; Ludwig, D.S. Childhood obesity: Public-health crisis, common sense cure. Lancet 2002, 360, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Issrani, R.; Reddy, J.; Bader, A.K.; Albalawi, R.F.H.; Alserhani, E.D.M.; Alruwaili, D.S.R.; Alanazi, G.R.A.; Alruwaili, N.S.R.; Sghaireen, M.G.; Rao, K. Exploring an Association between Body Mass Index and Oral Health—A Scoping Review. Diagnostics 2023, 13, 902. [Google Scholar] [CrossRef] [PubMed]
- Seidell, J.C.; Flegal, K.M. Assessing obesity: Classification and epidemiology. Br. Med. Bull. 1997, 53, 238–252. [Google Scholar] [CrossRef] [PubMed]
- Idrees, M.; Hammad, M.; Faden, A.; Kujan, O. Influence of body mass index on severity of dental caries: Cross-sectional study in healthy adults. Ann. Saudi Med. 2017, 37, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Adams, K.F.; Schatzkin, A.; Harris, T.B.; Kipnis, V.; Mouw, T.; Ballard-Barbash, R.; Hollenbeck, A.; Leitzmann, M.F. Overweight, Obesity, and Mortality in a Large Prospective Cohort of Persons 50 to 71 Years Old. N. Engl. J. Med. 2006, 355, 763–778. [Google Scholar] [CrossRef] [PubMed]
- Zeb, A.; Sivarajan Froelicher, E.; Pienaar, A.J.; Dhamani, K. Effectiveness of Community-based Obesity Intervention for Body Weight, Body Mass Index, and Waist Circumference: Meta-analysis. Iran. J. Nurs. Midwifery Res. 2024, 29, 16–22. [Google Scholar] [PubMed]
- Carullo, N.; Zicarelli, M.; Michael, A.; Faga, T.; Battaglia, Y.; Pisani, A.; Perticone, M.; Costa, D.; Ielapi, N.; Coppolino, G.; et al. Childhood Obesity: Insight into Kidney Involvement. Int. J. Mol. Sci. 2023, 24, 17400. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, N.C.; Amrutiya, M.R. Obesity and oral health—Is there a link? An observational study. J. India Soc. Periodontol. 2017, 21, 229. [Google Scholar] [CrossRef]
- Prospective Studies Collaboration; Whitlock, G.; Lewington, S.; Sherliker, P.; Clarke, R.; Emberson, J.; Halsey, J. Body-mass index and cause-specific mortality in 900 000 adults: Collaborative analyses of 57 prospective studies. Lancet 2009, 373, 1083–1096. [Google Scholar] [CrossRef]
- Galgani, J.; Ravussin, E. Energy metabolism, fuel selection and body weight regulation. Int. J. Obes. 2008, 32, S109–S119. [Google Scholar] [CrossRef] [PubMed]
- Suvan, J.; Petrie, A.; Moles, D.R.; Nibali, L.; Patel, K.; Darbar, U.; Donos, N.; Tonetti, M.; D’Aiuto, F. Body Mass Index as a Predictive Factor of Periodontal Therapy Outcomes. J. Dent. Res. 2014, 93, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Eknoyan, G. Adolphe Quetelet (1796–1874)—The average man and indices of obesity. Nephrol. Dial. Transplant. 2008, 23, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Kapila, Y.L. Oral health’s inextricable connection to systemic health: Special populations bring to bear multimodal relationships and factors connecting periodontal disease to systemic diseases and conditions. Periodontology 2000 2021, 87, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Finucane, M.M.; Stevens, G.A.; Cowan, M.J.; Danaei, G.; Lin, J.K.; Paciorek, C.J.; Singh, G.M.; Gutierrez, H.R.; Lu, Y.; Bahalim, A.N.; et al. National, regional, and global trends in body-mass index since 1980: Systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9·1 million participants. Lancet 2011, 377, 557–567. [Google Scholar] [CrossRef] [PubMed]
- McMurray, R.G.; Soares, J.; Caspersen, C.J.; McCurdy, T. Examining variations of resting metabolic rate of adults: A public health perspective. Med. Sci. Sports Exerc. 2014, 46, 1352–1358. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Jeon, J.; Kim, J.-W.; Song, T.-J.; Kim, J. Association between Findings in Oral Health Screening and Body Mass Index: A Nation-Wide Longitudinal Study. Int. J. Environ. Res. Public Health 2021, 18, 11062. [Google Scholar] [CrossRef]
- Wood, N.; Johnson, R.B.; Streckfus, C.F. Comparison of body composition and periodontal disease using nutritional assessment techniques: Third National Health and Nutrition Examination Survey (NHANES III). J. Clin. Periodontol. 2003, 30, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.; Clarke, M.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. An international registry of systematic-review protocols. Lancet 2011, 377, 108–109. [Google Scholar] [CrossRef]
- Bougioukas, K.I.; Liakos, A.; Tsapas, A.; Ntzani, E.; Haidich, A.-B. Preferred reporting items for overviews of systematic reviews including harms checklist: A pilot tool to be used for balanced reporting of benefits and harms. J. Clin. Epidemiol. 2018, 93, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Paranhos, K.; Oliveira, S.; Bonato, R.; Niknami, N.; Vinayak, S.; Loomer, P. The impact of obesity on the outcome of periodontal disease treatment: Systematic review and meta-analysis. Dent. Res. J. 2023, 20, 108. [Google Scholar]
- Zhang, Y.; Jia, R.; Zhang, Y.; Sun, X.; Mei, Y.; Zou, R.; Niu, L.; Dong, S. Effect of non-surgical periodontal treatment on cytokines/adipocytokines levels among periodontitis patients with or without obesity: A systematic review and meta-analysis. BMC Oral Health 2023, 23, 717. [Google Scholar] [CrossRef] [PubMed]
- Joseph, P.; Prabhakar, P.; Holtfreter, B.; Pink, C.; Suvan, J.; Kocher, T.; Pitchika, V. Systematic review and meta-analysis of randomized controlled trials evaluating the efficacy of non-surgical periodontal treatment in patients with concurrent systemic conditions. Clin. Oral Investig. 2023, 28, 21. [Google Scholar] [CrossRef] [PubMed]
- Akram, Z.; Safii, S.H.; Vaithilingam, R.D.; Baharuddin, N.A.; Javed, F.; Vohra, F. Efficacy of non-surgical periodontal therapy in the management of chronic periodontitis among obese and non-obese patients: A systematic review and meta-analysis. Clin. Oral Investig. 2016, 20, 903–914. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, G.G.; Leite, F.R.M.; Correa, M.B.; Peres, M.A.; Demarco, F.F. Does periodontal treatment have an effect on clinical and immunological parameters of periodontal disease in obese subjects? A systematic review and meta-analysis. Clin. Oral Investig. 2016, 20, 639–647. [Google Scholar] [CrossRef]
- Gerber, F.A.; Sahrmann, P.; Schmidlin, O.A.; Heumann, C.; Beer, J.H.; Schmidlin, P.R. Influence of obesity on the outcome of non-surgical periodontal therapy—A systematic review. BMC Oral Health 2016, 16, 90. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, S.N.; Reichert, C.; Jaeger, A.; Deschner, J. Effect of overweight/obesity on response to periodontal treatment: Systematic review and a meta-analysis. J. Clin. Periodontol. 2015, 42, 247–261. [Google Scholar] [CrossRef]
- Deng, Q.; Wong, H.M.; Peng, S. Salivary and gingival crevicular fluid biomarkers of periodontal health and/or obesity among children and adolescents: A systematic review and meta-analysis. Heliyon 2024, 10, e23782. [Google Scholar] [CrossRef]
- Akram, Z.; Abduljabbar, T.; Abu Hassan, M.I.; Javed, F.; Vohra, F. Cytokine Profile in Chronic Periodontitis Patients with and without Obesity: A Systematic Review and Meta-Analysis. Dis. Markers 2016, 2016, 4801418. [Google Scholar] [CrossRef]
- Foratori-Junior, G.A.; Pereira, P.R.; Gasparoto, I.A.; de Sales-Peres, S.H.C.; de Souza, J.M.S.; Khan, S. Is overweight associated with periodontitis in pregnant women? Systematic review and meta-analysis. Jpn. Dent. Sci. Rev. 2022, 58, 41–51. [Google Scholar] [CrossRef]
- Da Silva, F.G.; Pola, N.M.; Casarin, M.; de Silva, C.F.; Muniz, F.W.M.G. Association between clinical measures of gingival inflammation and obesity in adults: Systematic review and meta-analyses. Clin. Oral Investig. 2021, 25, 4281–4298. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, G.G.; Leite, F.R.M.; Do, L.G.; Peres, K.G.; Correa, M.B.; Demarco, F.F.; Peres, M.A. Is weight gain associated with the incidence of periodontitis? A systematic review and meta-analysis. J. Clin. Periodontol. 2015, 42, 495–505. [Google Scholar] [CrossRef]
- De Moura-Grec, P.G.; Marsicano, J.A.; Paz de Carvalho, C.A.; de Carvalho Sales-Peres, S.H. Obesity and periodontitis: Systematic review and meta-analysis. Cien Saude Colet. 2014, 19, 1763–1772. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.M.; Lee, S.; Hwang, W.; Son, E.; Kim, T.W.; Kim, K.; Kim, Y.H. Obesity and periodontitis: A systematic review and updated meta-analysis. Front. Endocrinol. 2022, 13, 999455. [Google Scholar] [CrossRef] [PubMed]
- Abu-Shawish, G.; Betsy, J.; Anil, S. Is Obesity a Risk Factor for Periodontal Disease in Adults? A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 12684. [Google Scholar] [CrossRef] [PubMed]
- Khairunnisa, L.; Dewi, Y.L.R.; Pamungkasari, E.P. Meta-Analysis the Association between Obesity and Periodontitis in Adults. J. Epidemiol. Public Health 2021, 6, 201–210. [Google Scholar] [CrossRef]
- Khan, S.; Barrington, G.; Bettiol, S.; Barnett, T.; Crocombe, L. Is overweight/obesity a risk factor for periodontitis in young adults and adolescents?: A systematic review. Obes. Rev. 2018, 19, 852–883. [Google Scholar] [CrossRef]
- Martens, L.; De Smet, S.; Yusof, M.Y.P.M.; Rajasekharan, S. Association between overweight/obesity and periodontal disease in children and adolescents: A systematic review and meta-analysis. Eur. Arch. Paediatr. Dent. 2017, 18, 69–82. [Google Scholar] [CrossRef]
- Martinez-Herrera, M.; Silvestre-Rangil, J.; Silvestre, F.-J. Association between obesity and periodontal disease. A systematic review of epidemiological studies and controlled clinical trials. Med. Oral Patol. Oral Cir. Bucal 2017, 22, E708–E715. [Google Scholar] [CrossRef] [PubMed]
- Keller, A.; Rohde, J.F.; Raymond, K.; Heitmann, B.L. Association Between Periodontal Disease and Overweight and Obesity: A Systematic Review. J. Periodontol. 2015, 86, 766–776. [Google Scholar] [CrossRef] [PubMed]
- Li, L.-W.; Wong, H.M.; Sun, L.; Wen, Y.F.; McGrath, C.P. Anthropometric Measurements and Periodontal Diseases in Children and Adolescents: A Systematic Review and Meta-Analysis. Adv. Nutr. 2015, 6, 828–841. [Google Scholar] [CrossRef] [PubMed]
- Suvan, J.; D’Aiuto, F.; Moles, D.R.; Petrie, A.; Donos, N. Association between overweight/obesity and periodontitis in adults. A systematic review. Obes. Rev. 2011, 12, e381–e404. [Google Scholar] [CrossRef] [PubMed]
- Chaffee, B.W.; Weston, S.J. Association Between Chronic Periodontal Disease and Obesity: A Systematic Review and Meta-Analysis. J. Periodontol. 2010, 81, 1708–1724. [Google Scholar] [CrossRef]
- Khader, Y.S.; Bawadi, H.A.; Haroun, T.F.; Alomari, M.; Tayyem, R.F. The association between periodontal disease and obesity among adults in Jordan. J. Clin. Periodontol. 2009, 36, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Kongstad, J.; Hvidtfeldt, U.A.; Grønbaek, M.; Stoltze, K.; Holmstrup, P. The relationship between body mass index and periodontitis in the Copenhagen City Heart Study. J. Periodontol. 2009, 80, 1246–1253. [Google Scholar] [CrossRef] [PubMed]
- Ekuni, D.; Yamamoto, T.; Koyama, R.; Tsuneishi, M.; Naito, K.; Tobe, K. Relationship between body mass index and periodontitis in young Japanese adults. J. Periodontal Res. 2008, 43, 417–421. [Google Scholar] [CrossRef]
- Dalla Vecchia, C.F.; Susin, C.; Rösing, C.K.; Oppermann, R.V.; Albandar, J.M. Overweight and obesity as risk indicators for periodontitis in adults. J. Periodontol. 2005, 76, 1721–1728. [Google Scholar] [CrossRef]
- Al-Zahrani, M.S.; Bissada, N.F.; Borawskit, E.A. Obesity and periodontal disease in young, middle-aged, and older adults. J. Periodontol. 2003, 74, 610–615. [Google Scholar] [CrossRef]
- Pataro, A.L.; Costa, F.O.; Cortelli, S.C.; Cortelli, J.R.; Abreu, M.H.N.G.; Costa, J.E. Association between severity of body mass index and periodontal condition in women. Clin. Oral Investig. 2012, 16, 727–734. [Google Scholar] [CrossRef]
- Han, D.-H.; Lim, S.-Y.; Sun, B.-C.; Paek, D.-M.; Kim, H.-D. Visceral fat area-defined obesity and periodontitis among Koreans. J. Clin. Periodontol. 2010, 37, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Saxlin, T.; Ylöstalo, P.; Suominen-Taipale, L.; Aromaa, A.; Knuuttila, M. Overweight and obesity weakly predict the development of periodontal infection. J. Clin. Periodontol. 2010, 37, 1059–1067. [Google Scholar] [CrossRef]
- Haffajee, A.D.; Socransky, S.S. Relation of body mass index, periodontitis and Tannerella forsythia. J. Clin. Periodontol. 2009, 36, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Linden, G.; Patterson, C.; Evans, A.; Kee, F. Obesity and periodontitis in 60–70-year-old men. J. Clin. Periodontol. 2007, 34, 461–466. [Google Scholar] [CrossRef]
- Saito, T.; Shimazaki, Y.; Koga, T.; Tsuzuki, M.; Ohshima, A. Relationship between upper body obesity and periodontitis. J. Dent. Res. 2001, 80, 1631–1636. [Google Scholar] [CrossRef] [PubMed]
- Ekuni, D.; Mizutani, S.; Kojima, A.; Tomofuji, T.; Irie, K.; Azuma, T.; Yoneda, T.; Furuta, M.; Eshima, N.; Iwasaki, Y.; et al. Relationship between increases in BMI and changes in periodontal status: A prospective cohort study. J. Clin. Periodontol. 2014, 41, 772–778. [Google Scholar] [CrossRef]
- Amin, H.E.-S. Relationship between overall and abdominal obesity and periodontal disease among young adults. East. Mediterr. Health J. 2010, 16, 429–433. [Google Scholar] [CrossRef]
- Dumitrescu, A.L.; Kawamura, M. Involvement of psychosocial factors in the association of obesity with periodontitis. J. Oral. Sci. 2010, 52, 115–124. [Google Scholar] [CrossRef]
- Furuta, M.; Ekuni, D.; Yamamoto, T.; Irie, K.; Koyama, R.; Sanbe, T.; Yamanaka, R.; Morita, M.; Kuroki, K.; Tobe, K. Relationship between periodontitis and hepatic abnormalities in young adults. Acta Odontol. Scand. 2010, 68, 27–33. [Google Scholar] [CrossRef]
- Kumar, S.; Dagli, R.J.; Dhanni, C.; Duraiswamy, P. Relationship of body mass index with periodontal health status of green marble mine laborers in Kesariyaji, India. Braz. Oral Res. 2009, 23, 365–369. [Google Scholar] [CrossRef] [PubMed]
- Kushiyama, M.; Shimazaki, Y.; Yamashita, Y. Relationship between metabolic syndrome and periodontal disease in Japanese adults. J. Periodontol. 2009, 80, 1610–1615. [Google Scholar] [CrossRef]
- Sarlati, F.; Akhondi, N.; Ettehad, T.; Neyestani, T.; Kamali, Z. Relationship between obesity and periodontal status in a sample of young Iranian adults. Int. Dent. J. 2008, 58, 36–40. [Google Scholar] [PubMed]
- Borges-Yáñez, S.A.; Irigoyen-Camacho, M.E.; Maupomé, G. Risk factors and prevalence of periodontitis in community-dwelling elders in Mexico. J. Clin. Periodontol. 2006, 33, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Reeves, A.F.; Rees, J.M.; Schiff, M.; Hujoel, P. Total body weight and waist circumference associated with chronic periodontitis among adolescents in the United States. Arch. Pediatr. Adolesc. Med. 2006, 160, 894–899. [Google Scholar] [CrossRef]
- Genco, R.J.; Grossi, S.G.; Ho, A.; Nishimura, F.; Murayama, Y. A proposed model linking inflammation to obesity, diabetes, and periodontal infections. J. Periodontol. 2005, 76, 2075–2084. [Google Scholar] [CrossRef] [PubMed]
- Saito, T.; Shimazaki, Y.; Kiyohara, Y.; Kato, I.; Kubo, M.; Iida, M.; Yamashita, Y. Relationship between obesity, glucose tolerance, and periodontal disease in Japanese women: The Hisayama study. J. Periodontal Res. 2005, 40, 346–353. [Google Scholar] [CrossRef]
- Torrungruang, K.; Tamsailom, S.; Rojanasomsith, K.; Sutdhibhisal, S.; Nisapakultorn, K.; Vanichjakvong, O.; Prapakamol, S.; Premsirinirund, T.; Pusiri, T.; Jaratkulangkoon, O.; et al. Risk indicators of periodontal disease in older Thai adults. J. Periodontol. 2005, 76, 558–565. [Google Scholar] [CrossRef]
- Gulati, N.N.; Masamatti, S.S.; Chopra, P. Association between obesity and its determinants with chronic periodontitis: A cross-sectional study. J. Indian. Soc. Periodontol. 2020, 24, 167–172. [Google Scholar] [CrossRef]
- Buduneli, N.; Bıyıkoğlu, B.; Ilgenli, T.; Buduneli, E.; Nalbantsoy, A.; Saraç, F.; Kinane, D.F. Is obesity a possible modifier of periodontal disease as a chronic inflammatory process? A case-control study. J. Periodontal Res. 2014, 49, 465–471. [Google Scholar] [CrossRef]
- Fadel, H.T.; Pliaki, A.; Gronowitz, E.; Mårild, S.; Ramberg, P.; Dahlèn, G.; Yucel-Lindberg, T.; Heijl, L.; Birkhed, D. Clinical and biological indicators of dental caries and periodontal disease in adolescents with or without obesity. Clin. Oral Investig. 2014, 18, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Altay, U.; Gürgan, C.A.; Ağbaht, K. Changes in inflammatory and metabolic parameters after periodontal treatment in patients with and without obesity. J. Periodontol. 2013, 84, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Irigoyen-Camacho, M.E.; Sanchez-Perez, L.; Molina-Frechero, N.; Velazquez-Alva, C.; Zepeda-Zepeda, M.; Borges-Yanez, A. The relationship between body mass index and body fat percentage and periodontal status in Mexican adolescents. Acta Odontol. Scand. 2014, 72, 48–57. [Google Scholar] [CrossRef]
- Al-Zahrani, M.S.; Alghamdi, H.S. Effect of periodontal treatment on serum C-reactive protein level in obese and normal-weight women affected with chronic periodontitis. Saudi Med. J. 2012, 33, 309–314. [Google Scholar] [PubMed]
- De Castilhos, E.D.; Horta, B.L.; Gigante, D.P.; Demarco, F.F.; Peres, K.G.; Peres, M.A. Association between obesity and periodontal disease in young adults: A population-based birth cohort. J. Clin. Periodontol. 2012, 39, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Gorman, A.; Kaye, E.K.; Apovian, C.; Fung, T.T.; Nunn, M.; Garcia, R.I. Overweight and Obesity Predict Time to Periodontal Disease Progression in Men. J. Clin. Periodontol. 2012, 39, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, M.; Hu, F.B.; Marino, M.; Li, Y.; Joshipura, K.J. Prospective Associations Between Measures of Adiposity and Periodontal Disease. Obesity 2012, 20, 1718–1725. [Google Scholar] [CrossRef] [PubMed]
- Zeigler, C.C.; Persson, G.R.; Wondimu, B.; Marcus, C.; Sobko, T.; Modéer, T. Microbiota in the oral subgingival biofilm is associated with obesity in adolescence. Obesity 2012, 20, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Franchini, R.; Petri, A.; Migliario, M.; Rimondini, L. Poor oral hygiene and gingivitis are associated with obesity and overweight status in paediatric subjects. J. Clin. Periodontol. 2011, 38, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Modéer, T.; Blomberg, C.; Wondimu, B.; Lindberg, T.Y.; Marcus, C. Association between obesity and periodontal risk indicators in adolescents. Int. J. Pediatr. Obes. 2011, 6, e264–e270. [Google Scholar] [CrossRef]
- Morita, I.; Okamoto, Y.; Yoshii, S.; Nakagaki, H.; Mizuno, K.; Sheiham, A.; Sabbah, W. Five-year incidence of periodontal disease is related to body mass index. J. Dent. Res. 2011, 90, 199–202. [Google Scholar] [CrossRef]
- Zuza, E.P.; Barroso, E.M.; Carrareto, A.L.V.; Pires, J.R.; Carlos, I.Z.; Theodoro, L.H.; Toledo, B.E.C. The role of obesity as a modifying factor in patients undergoing non-surgical periodontal therapy. J. Periodontol. 2011, 82, 676–682. [Google Scholar] [CrossRef]
- Morita, T.; Ogawa, Y.; Takada, K.; Nishinoue, N.; Sasaki, Y.; Motohashi, M.; Maeno, M. Association Between Periodontal Disease and Metabolic Syndrome. J. Public Health Dent. 2009, 69, 248–253. [Google Scholar] [CrossRef]
- Saxlin, T.; Suominen-Taipale, L.; Leiviskä, J.; Jula, A.; Knuuttila, M.; Ylöstalo, P. Role of serum cytokines tumour necrosis factor-alpha and interleukin-6 in the association between body weight and periodontal infection. J. Clin. Periodontol. 2009, 36, 100–105. [Google Scholar] [CrossRef]
- Wang, T.-T.; Chen, T.H.-H.; Wang, P.-E.; Lai, H.; Lo, M.-T.; Chen, P.Y.-C.; Chiu, S.Y.-H. A population-based study on the association between type 2 diabetes and periodontal disease in 12,123 middle-aged Taiwanese (KCIS No. 21). J. Clin. Periodontol. 2009, 36, 372–379. [Google Scholar] [CrossRef]
- D’Aiuto, F.; Sabbah, W.; Netuveli, G.; Donos, N.; Hingorani, A.D.; Deanfield, J.; Tsakos, G. Association of the Metabolic Syndrome with Severe Periodontitis in a Large U.S. Population-Based Survey. J. Clin. Endocrinol. Metab. 2008, 93, 3989–3994. [Google Scholar] [CrossRef]
- Saxlin, T.; Suominen-Taipale, L.; Kattainen, A.; Marniemi, J.; Knuuttila, M.; Ylöstalo, P. Association between serum lipid levels and periodontal infection. J. Clin. Periodontol. 2008, 35, 1040–1047. [Google Scholar] [CrossRef]
- Ylöstalo, P.; Suominen-Taipale, L.; Reunanen, A.; Knuuttila, M. Association between body weight and periodontal infection. J. Clin. Periodontol. 2008, 35, 297–304. [Google Scholar] [CrossRef]
- Shimazaki, Y.; Saito, T.; Yonemoto, K.; Kiyohara, Y.; Iida, M.; Yamashita, Y. Relationship of metabolic syndrome to periodontal disease in Japanese women: The Hisayama Study. J. Dent. Res. 2007, 86, 271–275. [Google Scholar] [CrossRef]
- Machado, A.C.P.; de Quirino, M.R.S.; Nascimento, L.F.C. Relation between chronic periodontal disease and plasmatic levels of triglycerides, total cholesterol and fractions. Braz. Oral. Res. 2005, 19, 284–289. [Google Scholar] [CrossRef]
- Caracho, R.A.; Foratori-Junior, G.A.; Fusco, N.D.S.; Jesuino, B.G.; Missio, A.L.T.; Sales-Peres, S.H. de C. Systemic conditions and oral health-related quality of life of pregnant women of normal weight and who are overweight. Int. Dent. J. 2020, 70, 287–295. [Google Scholar] [CrossRef]
- Foratori-Junior, G.A.; da Silva, B.M.; da Silva Pinto, A.C.; Honório, H.M.; Groppo, F.C.; de Carvalho Sales-Peres, S.H. Systemic and periodontal conditions of overweight/obese patients during pregnancy and after delivery: A prospective cohort. Clin. Oral Investig. 2020, 24, 157–165. [Google Scholar] [CrossRef]
- Fusco, N.D.S.; Foratori-Junior, G.A.; Missio, A.L.T.; Jesuino, B.G.; Sales-Peres, S.H. de C. Systemic and oral conditions of pregnant women with excessive weight assisted in a private health system. Int. Dent. J. 2019, 69, 472–479. [Google Scholar] [CrossRef]
- Kim, Y.-S.; Kim, J.-H. Body mass index and oral health status in Korean adults: The Fifth Korea National Health and Nutrition Examination Survey. Int. J. Dent. Hyg. 2017, 15, 172–178. [Google Scholar] [CrossRef]
- Martinez-Herrera, M.; Silvestre, F.J.; Silvestre-Rangil, J.; Bañuls, C.; Rocha, M.; Hernández-Mijares, A. Involvement of insulin resistance in normoglycaemic obese patients with periodontitis: A cross-sectional study. J. Clin. Periodontol. 2017, 44, 981–988. [Google Scholar] [CrossRef]
- Nascimento, G.G.; Peres, K.G.; Mittinty, M.N.; Mejia, G.C.; Silva, D.A.; Gonzalez-Chica, D.; Peres, M.A. Obesity and Periodontal Outcomes: A Population-Based Cohort Study in Brazil. J. Periodontol. 2017, 88, 50–58. [Google Scholar] [CrossRef]
- Al Habashneh, R.; Azar, W.; Shaweesh, A.; Khader, Y. The relationship between body mass index and periodontitis among postmenopausal women. Obes. Res. Clin. Pract. 2016, 10, 15–23. [Google Scholar] [CrossRef]
- Balli, U.; Ongoz Dede, F.; Bozkurt Dogan, S.; Gulsoy, Z.; Sertoglu, E. Chemerin and interleukin-6 levels in obese individuals following periodontal treatment. Oral Dis. 2016, 22, 673–680. [Google Scholar] [CrossRef]
- Öngöz Dede, F.; Bozkurt Doğan, Ş.; Ballı, U.; Avcı, B.; Durmuşlar, M.C. The effect of initial periodontal treatment on plasma, gingival crevicular fluid and salivary levels of 8-hydroxy-deoxyguanosine in obesity. Arch. Oral Biol. 2016, 62, 80–85. [Google Scholar] [CrossRef]
- Bouaziz, W.; Davideau, J.-L.; Tenenbaum, H.; Huck, O. Adiposity Measurements and Non-Surgical Periodontal Therapy Outcomes. J. Periodontol. 2015, 86, 1030–1037. [Google Scholar] [CrossRef]
- Gonçalves, T.E.D.; Feres, M.; Zimmermann, G.S.; Faveri, M.; Figueiredo, L.C.; Braga, P.G.; Duarte, P.M. Effects of scaling and root planing on clinical response and serum levels of adipocytokines in patients with obesity and chronic periodontitis. J. Periodontol. 2015, 86, 53–61. [Google Scholar] [CrossRef]
- Peng, S.M.; McGrath, C.; Wong, H.M.; King, N.M. The relationship between oral hygiene status and obesity among preschool children in Hong Kong. Int. J. Dent. Hyg. 2014, 12, 62–66. [Google Scholar] [CrossRef]
- Nascimento, G.G.; Seerig, L.M.; Vargas-Ferreira, F.; Correa, F.O.B.; Leite, F.R.M.; Demarco, F.F. Are obesity and overweight associated with gingivitis occurrence in Brazilian schoolchildren? J. Clin. Periodontol. 2013, 40, 1072–1078. [Google Scholar] [CrossRef]
- Scorzetti, L.; Marcattili, D.; Pasini, M.; Mattei, A.; Marchetti, E.; Marzo, G. Association between obesity and periodontal disease in children. Eur. J. Paediatr. Dent. 2013, 14, 181–184. [Google Scholar]
- Benguigui, C.; Bongard, V.; Ruidavets, J.-B.; Sixou, M.; Chamontin, B.; Ferrières, J.; Amar, J. Evaluation of oral health related to body mass index. Oral Dis. 2012, 18, 748–755. [Google Scholar] [CrossRef]
- Kim, E.-J.; Jin, B.-H.; Bae, K.-H. Periodontitis and obesity: A study of the Fourth Korean National Health and Nutrition Examination Survey. J. Periodontol. 2011, 82, 533–542. [Google Scholar] [CrossRef]
- Modéer, T.; Blomberg, C.C.; Wondimu, B.; Julihn, A.; Marcus, C. Association between obesity, flow rate of whole saliva, and dental caries in adolescents. Obesity 2010, 18, 2367–2373. [Google Scholar] [CrossRef]
- Shimazaki, Y.; Egami, Y.; Matsubara, T.; Koike, G.; Akifusa, S.; Jingu, S.; Yamashita, Y. Relationship between obesity and physical fitness and periodontitis. J. Periodontol. 2010, 81, 1124–1131. [Google Scholar] [CrossRef]
- Li, P.; He, L.; Sha, Y.-Q.; Luan, Q.-X. Relationship of metabolic syndrome to chronic periodontitis. J. Periodontol. 2009, 80, 541–549. [Google Scholar] [CrossRef]
- Pitiphat, W.; Savetsilp, W.; Wara-Aswapati, N. C-reactive protein associated with periodontitis in a Thai population. J. Clin. Periodontol. 2008, 35, 120–125. [Google Scholar] [CrossRef]
- Saito, T. Obesity may be Associated with Periodontitis in Elderly Men. J. Evid. Based Dent. Pract. 2008, 8, 97–98. [Google Scholar] [CrossRef]
- Saito, T.; Yamaguchi, N.; Shimazaki, Y.; Hayashida, H.; Yonemoto, K.; Doi, Y.; Kiyohara, Y.; Iida, M.; Yamashita, Y. Serum levels of resistin and adiponectin in women with periodontitis: The Hisayama study. J. Dent. Res. 2008, 87, 319–322. [Google Scholar] [CrossRef]
- Wood, N.; Johnson, R.B. The relationship between smoking history, periodontal screening and recording (PSR) codes and overweight/obesity in a Mississippi dental school population. Oral Health Prev. Dent. 2008, 6, 67–74. [Google Scholar]
- Alabdulkarim, M.; Bissada, N.; Al-Zahrani, M.; Ficara, A.; Siegel, B. Alveolar bone loss in obese subjects. J. Int. Acad. Periodontol. 2005, 7, 34–38. [Google Scholar]
- Chapper, A.; Munch, A.; Schermann, C.; Piacentini, C.C.; Fasolo, M.T.M. Obesity and periodontal disease in diabetic pregnant women. Braz. Oral Res. 2005, 19, 83–87. [Google Scholar] [CrossRef]
- Nishida, N.; Tanaka, M.; Hayashi, N.; Nagata, H.; Takeshita, T.; Nakayama, K.; Morimoto, K.; Shizukuishi, S. Determination of smoking and obesity as periodontitis risks using the classification and regression tree method. J. Periodontol. 2005, 76, 923–928. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D. Periodontal microbial ecology. Periodontology 2005, 38, 135–187. [Google Scholar] [CrossRef]
- Lundin, M.; Yucel-Lindberg, T.; Dahllöf, G.; Marcus, C.; Modéer, T. Correlation between TNFalpha in gingival crevicular fluid and body mass index in obese subjects. Acta Odontol. Scand. 2004, 62, 273–277. [Google Scholar] [CrossRef]
- Buhlin, K.; Gustafsson, A.; Pockley, A.G.; Frostegård, J.; Klinge, B. Risk factors for cardiovascular disease in patients with periodontitis. Eur. Heart J. 2003, 24, 2099–2107. [Google Scholar] [CrossRef]
- Suvan, J.E.; Finer, N.; D’Aiuto, F. Periodontal complications with obesity. Periodontology 2018, 78, 98–128. [Google Scholar] [CrossRef]
- Amar, S.; Zhou, Q.; Shaik-Dasthagirisaheb, Y.; Leeman, S. Diet-induced obesity in mice causes changes in immune responses and bone loss manifested by bacterial challenge. Proc. Natl. Acad. Sci. USA 2007, 104, 20466–20471. [Google Scholar] [CrossRef]
- Maciel, S.S.; Feres, M.; Gonçalves, T.E.D.; Zimmermann, G.S.; da Silva, H.D.P.; Figueiredo, L.C.; Duarte, P.M. Does obesity influence the subgingival microbiota composition in periodontal health and disease? J. Clin. Periodontol. 2016, 43, 1003–1012. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Kompoti, M. Obesity and infection. Lancet Infect. Dis. 2006, 6, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.-P.; Yu, H.-C.; Lin, T.-H.; Wang, Y.-H.; Chang, Y.-C. Association between obesity and chronic periodontitis. Medicine 2021, 100, e27506. [Google Scholar] [CrossRef] [PubMed]
- Moher, D. The problem of duplicate systematic reviews. BMJ 2013, 347, f5040. [Google Scholar] [CrossRef] [PubMed]
- Mizia, S.; Felińczak, A.; Włodarek, D.; Syrkiewicz-Świtała, M. Evaluation of Eating Habits and Their Impact on Health among Adolescents and Young Adults: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 3996. [Google Scholar] [CrossRef]
- Bogaard, L. Parent Influences on the Dietary Habits of Young Adults. Berkeley Undergr. J. 2023, 37, 1–14. [Google Scholar] [CrossRef]
- Mao, L.; Xu, J.; Zou, J. Effects of follicle-stimulating hormone on fat metabolism and cognitive impairment in women during menopause. Front. Physiol. 2022, 13, 1043237. [Google Scholar] [CrossRef] [PubMed]
- Palla, G.; Ramírez-Morán, C.; Montt-Guevara, M.M.; Salazar-Pousada, D.; Shortrede, J.; Simoncini, T.; Grijalva-Grijalva, I.; Pérez-López, F.R.; Chedraui, P. Perimenopause, body fat, metabolism and menopausal symptoms in relation to serum markers of adiposity, inflammation and digestive metabolism. J. Endocrinol. Investig. 2020, 43, 809–820. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.M. Lipid metabolism in women. Proc. Nutr. Soc. 2004, 63, 153–160. [Google Scholar] [CrossRef]
- Ferretti, F.; Mariani, M.; Sarti, E. Is the development of obesogenic food environments a self-reinforcing process? Evidence from soft drink consumption. Glob. Health 2021, 17, 91. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Database | Search Strategy | Number of Studies |
|---|---|---|
| Pubmed | ((“periodontitis”) OR (“periodontal disease”) OR (“furcation defect”) OR (“gingival disease”) OR (“gingivitis”) OR (“tooth loss”) OR (“tooth migration”) OR (“tooth mobility”) OR (“missing teeth”) OR (“periodontal inflammation”) OR (“gum disease”) OR (“gum inflammation”)) AND ((“Obesity”) OR (“overweight”) OR (“body weight”) OR (“body mass index”) OR (“abdominal fat”) OR (“obese”) OR (“BMI”)) AND ((“systematic review”) OR (“meta-analysis”)) | 76 |
| Cochrane database | #1 MeSH descriptor: [Periodontal Diseases] explode all trees | 42 |
| #2 MeSH descriptor: [Periodontitis] in all MeSH products | ||
| #3 MeSH descriptor: [Furcation Defects] explode all trees | ||
| #4 MeSH descriptor: [Gingival Diseases] explode all trees | ||
| #5 MeSH descriptor: [Gingivitis] explode all trees | ||
| #6 MeSH descriptor: [Tooth Loss] explode all trees | ||
| #7 MeSH descriptor: [Tooth Migration] explode all trees | ||
| #8 MeSH descriptor: [Tooth Mobility] explode all trees | ||
| #9 (“periodontitis”) OR (“periodontal disease”) OR (“furcation defect”) OR (“gingival disease”) OR (“gingivitis”) OR (“tooth loss”) OR (“tooth migration”) OR (“tooth mobility”) OR (“missing teeth”) OR (“periodontal inflammation”) OR (“gum disease”) OR (“gum inflammation”) (Word variations have been searched) | ||
| #10 #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 | ||
| #11 MeSH descriptor: [Obesity] explode all trees | ||
| #12 MeSH descriptor: [Overweight] explode all trees | ||
| #13 MeSH descriptor: [Body Weight] explode all trees | ||
| #14 MeSH descriptor: [Body Mass Index] explode all trees | ||
| #15 MeSH descriptor: [Abdominal Fat] explode all trees | ||
| #16 (“obesity”) OR (“overweight”) OR (“body weight”) OR (“body mass index”) OR (“abdominal fat”) (Word variations have been searched) OR (“obese”) OR (“BMI”) (Word variations have been searched) | ||
| #17 #11 OR #12 OR #13 OR #14 OR #15 OR #16 | ||
| #18 MeSH descriptor: [Systematic Reviews as Topic] explode all trees | ||
| #19 MeSH descriptor: [Meta-Analysis as Topic] explode all trees | ||
| #20 (“systematic review”) OR (“meta-analysis”) (Word variations have been searched) | ||
| #21 #18 OR #19 OR #20; #22 #10 AND #17 AND #21 | ||
| Scielo | ((((“periodontitis”) OR (“periodontal disease”) OR (“furcation defect”) OR (“gingival disease”) OR (“gingivitis”) OR (“tooth loss”) OR (“tooth migration”) OR (“tooth mobility”) OR (“missing teeth”) OR (“periodontal inflammation”) OR (“gum disease”) OR (“gum inflammation”))) AND (((“Obesity”) OR (“overweight”) OR (“body weight”) OR (“body mass index”) OR (“abdominal fat”) OR (“obese”) OR (“BMI”)))) AND (((“systematic review”) OR (“meta-analysis”))) | 3 |
| Scopus | (TITLE-ABS-KEY (((“periodontitis”) OR (“periodontal disease”) OR (“furcation defect”) OR (“gingival disease”) OR (“gingivitis”) OR (“tooth loss”) OR (“tooth migration”) OR (“tooth mobility”) OR (“missing teeth”) OR (“periodontal inflammation”) OR (“gum disease”) OR (“gum inflammation”))) AND TITLE-ABS-KEY (((“Obesity”) OR (“overweight”) OR (“body weight”) OR (“body mass index”) OR (“abdominal fat”) OR (“obese”) OR (“BMI”))) AND TITLE-ABS-KEY (((“systematic review”) OR (“meta-analysis”)))) AND (LIMIT-TO (DOCTYPE, “re”) OR LIMIT-TO (DOCTYPE, “ar”)) AND (LIMIT-TO (PUBSTAGE, “final”)) AND (LIMIT-TO (SRCTYPE, “j”)) | 174 |
| Web of Science | (TS=(“periodontitis”) OR TS=(“periodontal disease”) OR TS=(“furcation defect”) OR TS=(“gingival disease”) OR TS=(“gingivitis”) OR TS=(“tooth loss”) OR TS=(“tooth migration”) OR TS=(“tooth mobility”) OR TS=(“missing teeth”) OR TS=(“periodontal inflammation”) OR TS=(“gum disease”) OR TS=(“gum inflammation”)) AND (TS=(“obesity”) OR TS=(“overweight”) OR TS=(“body weight”) OR TS=(“body mass index”) OR TS=(“abdominal fat”) OR TS=(“obese”) OR TS=(“BMI”)) AND (TS=(“systematic review”) OR TS=(“meta-analysis”)) | 79 |
| Google Scholar | allintitle: ((“periodontal disease”) OR (“periodontitis”)) + ((“Obesity”) OR (“overweight”)) + ((“systematic review”) OR (“meta-analysis”)) | 22 |
| Proquest Dissertations and Theses | ((“periodontal disease”) OR (“periodontitis”)) AND ((“Obesity”) OR (“overweight”)) AND ((“systematic review”) OR (“meta-analysis”)) AND NOT ((“cardiovascular”) OR (“obstructive sleep apnea”) OR (“cancer”) OR (“pregnant”) OR (“dementia”) OR (“in vitro”) OR (“dental caries”) OR (“fractures”) OR (“rat”) OR (“diabetes mellitus”) OR (“periodontal treatment”) OR (“pulpotomy”) OR (“treatment”)) | 23 |
| OpenGrey | ((“periodontitis”) OR (“periodontal disease”) OR (“furcation defect”) OR (“gingival disease”) OR (“gingivitis”) OR (“tooth loss”) OR (“tooth migration”) OR (“tooth mobility”) OR (“missing teeth”) OR (“periodontal inflammation”) OR (“gum disease”) OR (“gum inflammation”)) AND ((“Obesity”) OR (“overweight”) OR (“body weight”) OR (“body mass index”) OR (“abdominal fat”) OR (“obese”) OR (“BMI”)) AND ((“systematic review”) OR (“meta-analysis”)) | 0 |
| Author | Reason for Exclusion |
|---|---|
| Paranhos et al. [33] | They associated obesity with periodontal treatment |
| Zhang et al. [34] | |
| Joseph et al. [35] | |
| Akram et al. [36] | |
| Nascimento et al. [37] | |
| Gerber et al. [38] | |
| Papageorgiou et al. [39] | |
| Deng et al. [40] | They associated obesity with salivary biomarkers of PD |
| Akram et al. [41] |
| Authors | Year | Study Design | Country | Included Study Design | Number of Studies in the Qualitative Analysis | Number of Studies in the Quantitative Analysis | Outcomes | Conclusions | |
|---|---|---|---|---|---|---|---|---|---|
| Foratori-Junior et al. [42] | 2022 | SR with MA | Brazil | CS, C, and CC | 11 | 11 | General | RR = 2.21 (1.53–3.17) | There is an association between overweight/obesity and periodontitis during pregnancy. |
| Kim et al. [46] | 2022 | SR with MA | South Korea | CS, C, and CC | 37 | 29 | General | OR = 1.35 (1.05–1.75) | A positive association was found between obesity and periodontitis regardless of country or age. |
| 18–34 years | OR = 2.21 (1.26–3.89) | ||||||||
| 35–54 years | OR = 1.53 (1.17–2.00) | ||||||||
| ≥ 55 years | OR = 1.82 (1.16–2.83) | ||||||||
| United States | OR = 0.59 (0.19–1.65) | ||||||||
| Brazil | OR = 1.70 (0.78–3.72) | ||||||||
| European countries | OR = 2.46 (1.11–5.46) | ||||||||
| Korea | OR = 1.34 (1.00–1.80) | ||||||||
| Japan | OR = 1.75 (1.48–2.06) | ||||||||
| Other Asian countries | OR = 0.98 (0.49–1.95) | ||||||||
| Abu-Shawish et al. [47] | 2022 | SR | Qatar | CS, C, and CC | 15 | 0 | General | OR = 1.77–3.25 | This SR found a positive association between obesity in terms of increased BMI and periodontitis in adults. |
| RR = 1.64–1.84 | |||||||||
| Khairunnisa et al. [48] | 2021 | SR with MA | Indonesia | CS | 11 | 11 | General | OR = 1.23 (1.15–1.33) | Obesity increases periodontitis in adults. |
| da Silva et al. [43] | 2021 | SR with MA | Brazil | CS, CT, C, and CC | 90 | 90 | Obese | SMD = 0.05 (−0.20–0.29) | Higher measures of gingival inflammation can be expected for those with higher BMI. |
| Overweight | SMD = 0.30 (−0.03–0.62) | ||||||||
| Overweight or obese | SMD = 0.20 (−0.09–0.48) | ||||||||
| BOP (obese) | SMD = 0.03 (−0.23–0.28) | ||||||||
| BOP (Overweight) | SMD = 0.13 (−0.04–0.30) | ||||||||
| BOP (Overweight or obese) | SMD = 0.20 (−0.05–0.45) | ||||||||
| GI (obese) | SMD = 0.35 (−0.21–0.91) | ||||||||
| GI (Overweigh) | SMD = 0.97 (0.45–1.49) | ||||||||
| GI (Overweight or obese) | SMD = 0.22 (−0.24–0.68) | ||||||||
| Obese—G | SMD = 1.10 (0.14–2.05) | ||||||||
| Overweight—G | SMD = 2.08 (−0.60–4.77) | ||||||||
| Overweight or obese—G | SMD = 2.91 (−0.89–6.72) | ||||||||
| BOP (obese)—G | SMD = 0.64 (−0.37–1.65) | ||||||||
| BOP (Overweight)—G | SMD = 0.78 (0.52–1.03) | ||||||||
| BOP (Overweight or obese)—G | SMD = 1.02 (0.77–1.27) | ||||||||
| GI (obese)—G | SMD = 2.13 (−1.51–5.77) | ||||||||
| GI (Overweight)—G | SMD = 3.52 (2.32–4.71) | ||||||||
| GI (Overweight or obese)—G | SMD = 4.91 (3.64–6.17) | ||||||||
| Khan et al. [49] | 2018 | SR | Australia | CS, C, and CC | 25 | 0 | General | OR = 1.1–4.5 | There was evidence to suggest that obesity is associated with periodontitis in adolescents and young adults. |
| Martens et al. [50] | 2017 | SR with MA | Belgium | CS, C, and CC | 12 | 7 | General | OR = 1.46 (1.20–1.77) | The available evidence suggests a significantly positive association between periodontal disease and obesity in children. |
| Martinez-Herrera et al. [51] | 2017 | SR | Spain | C, CC, and CT | 28 | 0 | General | OR = 0.99–4.3 | The association between obesity and periodontitis was consistent with a compelling pattern of increased risk of periodontitis in overweight or obese individuals. |
| HR = 1.03–3.24 | |||||||||
| RR = 0.99–5.4 | |||||||||
| Nascimento et al. [44] | 2015 | SR with MA | Brazil | O | 5 | 5 | Overweight | RR = 1.13 (1.06–1.20) | A clear positive association between weight gain and new cases of periodontitis was found. |
| Obese | RR = 1.34 (1.21–1.47) | ||||||||
| Keller et al. [52] | 2015 | SR | Denmark | C and CT | 13 | 0 | Age (obese) | HR = 1.30–3.24 | Overweight and obesity can be risk factors for the development or worsening of periodontal health. |
| IRR = 1.3 | |||||||||
| PR = 1.01 | |||||||||
| Age (overweight) | HR = 1.09–1.70 | ||||||||
| IRR = 1.2 | |||||||||
| PR = 0.99 | |||||||||
| Li et al. [53] | 2015 | SR with MA | China | CS and CC | 16 | 5 | PI > 25% | OR = 4.75 (2.42–9.34) | Obesity is associated with some signs of periodontal disease in children and adolescents. |
| BOP > 25% | OR = 5.41 (2.75–10.63) | ||||||||
| SBC | OR = 3.07 (1.10–8.62) | ||||||||
| SPC | OR = 1.08 (0.60–1.94) | ||||||||
| PD > 4 mm | OR = 14.15 (5.10–39.25) | ||||||||
| de Moura-Grec et al. [45] | 2014 | SR with MA | Brazil | CS | 31 | 31 | General | OR = 1.30 (1.25–1.35) | Obesity was associated with periodontitis; however, the risk factors that aggravate these diseases should be better clarified to elucidate the direction of this association. |
| Suvan et al. [54] | 2011 | SR with MA | United Kingdom | CS, C, and CC | 33 | 19 | Obese | OR = 1.81 (1.42–2.30) | These results support an association between BMI overweight and obesity and periodontitis although the magnitude is unclear. |
| Overweight | OR = 1.27 (1.06–1.51) | ||||||||
| Overweight and obese | OR = 2.13 (1.40–3.26) | ||||||||
| Chaffee et al. [55] | 2010 | SR with MA | United States | O | 70 | 28 | General | OR = 1.35 (1.23–1.47) | There is a positive association between periodontal disease and obesity, which was consistent and coherent with a biologically plausible role of obesity in the development of periodontal disease. |
| Obese | OR = 1.52 (1.26–1.83) | ||||||||
| Overweight | OR = 1.18 (1.00–1.39) | ||||||||
| East Asia | OR = 1.32 (1.19–1.47) | ||||||||
| Europe and Middle East | OR = 1.87 (1.17–2.99) | ||||||||
| United States | OR = 1.30 (1.16–1.46) | ||||||||
| Men | OR = 1.50 (1.27–1.77) | ||||||||
| Women | OR = 1.75 (1.26–2.43) | ||||||||
| Young | OR = 1.35 (1.14–1.59) | ||||||||
| Older | OR = 1.21 (1.04–1.41) | ||||||||
| Smoker | OR = 1.36 (0.98–1.88) | ||||||||
| Non-smoker | OR = 2.08 (1.29–3.36) | ||||||||
| Authors | Year | AMSTAR-2 | Overall Confidence | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 * | 3 | 4 * | 5 | 6 | 7 * | 8 | 9 * | 10 | 11 * | 12 | 13 * | 14 | 15 * | 16 | |||
| Foratori-Junior et al. [42] | 2022 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Kim et al. [46] | 2022 | Yes | Yes | Yes | Yes partial | Yes | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Abu-Shawish et al. [47] | 2022 | Yes | Yes | Yes | Yes partial | Yes | Yes | No | Yes | Yes | Yes | No meta-analysis | Yes | Yes | No meta-analysis | Yes | Low | |
| Khairunnisa et al. [48] | 2021 | Yes | Yes partial | Yes | Yes partial | No | No | Yes partial | No | Yes partial | Yes | Yes | No | No | No | Yes | Yes | Low |
| da Silva et al. [43] | 2021 | Yes | Yes partial | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Khan et al. [49] | 2018 | Yes | Yes | Yes | Yes partial | Yes | Yes | Yes partial | Yes | Yes | Yes | No meta-analysis | Yes | Yes | No meta-analysis | Yes | High | |
| Martens et al. [50] | 2017 | Yes | Yes partial | Yes | Yes | Yes | Yes | No | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Martinez-Herrera et al. [51] | 2017 | Yes | Yes partial | Yes | Yes partial | No | No | No | Yes | No | No | No meta-analysis | No | No | No meta-analysis | Yes | Critically low | |
| Nascimento et al. [44] | 2015 | Yes | Yes partial | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Keller et al. [52] | 2015 | Yes | Yes partial | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes partial | Yes | No meta-analysis | Yes | Yes | No meta-analysis | Yes | High | |
| Li et al. [53] | 2015 | Yes | Yes partial | Yes | Yes partial | Yes | Yes | Yes partial | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| de Moura-Grec et al. [45] | 2014 | Yes | Yes partial | Yes | Yes partial | Yes | Yes | Yes partial | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | No | Low |
| Suvan et al. [54] | 2011 | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Chaffee et al. [55] | 2010 | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes partial | Yes | Yes partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Primary Studies | Systematic Reviews That Included the Primary Studies | Times That Primary Studies Were Included |
|---|---|---|
| Khader et al. [56] | Kim et al. [46], Abu-Shawish et al. [47], Khairunnisa et al. [48], da Silva et al. [43], de Moura-Grec et al. [45], Suvan et al. [54], Chaffee et al. [55] | 7 |
| Kongstad et al. [57] | Kim et al. [46], Khairunnisa et al. [48], Martínez-Herrera et al. [51], de Moura-Grec et al. [45], Suvan et al. [54], Chaffee et al. [55] | 6 |
| Ekuni et al. [58] | Kim et al. [46], Khairunnisa et al. [48], Khan et al. [49], de Moura-Grec et al. [45], Suvan et al. [54], Chaffee et al. [55] | 6 |
| Dalla Vecchia et al. [59] | Kim et al. [46], Abu-Shawish et al. [47], Khairunnisa et al. [48], de Moura-Grec et al. [45], Suvan et al. [54], Chaffee et al. [55] | 6 |
| Al-Zahrani et al. [60] | Kim et al. [46], Khan et al. [49], Martínez-Herrera et al. [51], de Moura-Grec et al. [45], Suvan et al. [54], Chaffee et al. [55] | 6 |
| Pataro et al. [61] | Kim et al. [46], Abu-Shawish et al. [47], Khairunnisa et al. [48], da Silva et al. [43], Martínez-Herrera et al. [51] | 5 |
| Han et al. [62] | Kim et al. [46], Khairunnisa et al. [48], de Moura-Grec et al. [45], Suvan et al. [54], Chaffee et al. [55] | 5 |
| Saxlin et al. [63] | Kim et al. [46], Martínez-Herrera et al. [51], Nascimento et al. [44], Keller et al. [52], de Moura-Grec et al. [45] | 5 |
| Haffajee et al. [64] | Kim et al. [46], da Silva et al. [43], de Moura-Grec et al. [45], Suvan et al. [54], Chaffee et al. [55] | 5 |
| Linden et al. [65] | Abu-Shawish et al. [47], Martínez-Herrera et al. [51], Keller et al. [52], Suvan et al. [54], Chaffee et al. [55] | 5 |
| Wood et al. [28] | Khan et al. [49], Martínez-Herrera et al. [51], de Moura-Grec et al. [45], Suvan et al. [54], Chaffee et al. [55] | 5 |
| Saito et al. [66] | Kim et al. [46], Martínez-Herrera et al. [51], de Moura-Grec et al. [45], Suvan et al. [54], Chaffee et al. [55] | 5 |
| Ekuni et al. [67] | da Silva et al. [43], Martínez-Herrera et al. [51], Nascimento et al. [44], Keller et al. [52] | 4 |
| Amin et al. [68] | Abu-Shawish et al. [47], da Silva et al. [43], Khan et al. [49], Chaffee et al. [55] | 4 |
| Dumitrescu et al. [69] | Kim et al. [46], da Silva et al. [43], de Moura-Grec et al. [45], Chaffee et al. [55] | 4 |
| Furuta et al. [70] | Kim et al. [46], Khan et al. [49], de Moura-Grec et al. [45], Chaffee et al. [55] | 4 |
| Kumar et al. [71] | Kim et al. [46], Khairunnisa et al. [48], de Moura-Grec et al. [45], Chaffee et al. [55] | 4 |
| Kushiyama et al. [72] | Kim et al. [46], de Moura-Grec et al. [45], Suvan et al. [54], Chaffee et al. [55] | 4 |
| Sarlati et al. [73] | Abu-Shawish et al. [47], Khan et al. [49], Suvan et al. [54], Chaffee et al. [55] | 4 |
| Borges-Yañez et al. [74] | Kim et al. [46], de Moura-Grec et al. [45], Suvan et al. [54], Chaffee et al. [55] | 4 |
| Reeves et al. [75] | Khan et al. [49], Martens et al. [50], Li et al. [53], Chaffee et al. [55] | 4 |
| Genco et al. [76] | Martínez-Herrera et al. [51], de Moura-Grec et al. [45], Suvan et al. [54], Chaffee et al. [55] | 4 |
| Saito et al. [77] | Martínez-Herrera et al. [51], de Moura-Grec et al. [45], Suvan et al. [54], Chaffee et al. [55] | 4 |
| Torrungruang et al. [78] | Kim et al. [46], de Moura-Grec et al. [45], Suvan et al. [54], Chaffee et al. [55] | 4 |
| Gulati et al. [79] | Kim et al. [46], Khairunnisa et al. [48], da Silva et al. [43] | 3 |
| Buduneli et al. [80] | Abu-Shawish et al. [47], da Silva et al. [43], Martínez-Herrera et al. [51] | 3 |
| Fadel et al. [81] | Khan et al. [49], Martens et al. [50], Li et al. [53] | 3 |
| Suvan et al. [22] | da Silva et al. [43], Martínez-Herrera et al. [51], Keller et al. [52] | 3 |
| Altay et al. [82] | da Silva et al. [43], Martínez-Herrera et al. [51], Keller et al. [52] | 3 |
| Irigoyen-Camacho et al. [83] | Khan et al. [49], Martens et al. [50], Li et al. [53] | 3 |
| Al-Zahrani et al. [84] | da Silva et al. [43], Martínez-Herrera et al. [51], Keller et al. [52] | 3 |
| de Castilhos et al. [85] | da Silva et al. [43], Khan et al. [49], Keller et al. [52] | 3 |
| Gorman et al. [86] | Martínez-Herrera et al. [51], Nascimento et al. [44], Keller et al. [52] | 3 |
| Jimenez et al. [87] | Martínez-Herrera et al. [51], Nascimento et al. [44], Keller et al. [52] | 3 |
| Zeigler et al. [88] | Khan et al. [49], Martens et al. [50], Li et al. [53] | 3 |
| Franchini et al. [89] | Khan et al. [49], Martens et al. [50], Li et al. [53] | 3 |
| Modéer et al. [90] | Khan et al. [49], Martens et al. [50], Li et al. [53] | 3 |
| Morita et al. [91] | Martínez-Herrera et al. [51], Nascimento et al. [44], Keller et al. [52] | 3 |
| Zuza et al. [92] | da Silva et al. [43], Martínez-Herrera et al. [51], Keller et al. [52] | 3 |
| Morita et al. [93] | Kim et al. [46], de Moura-Grec et al. [45], Chaffee et al. [55] | 3 |
| Saxlin et al. [94] | Kim et al. [46], de Moura-Grec et al. [45], Chaffee et al. [55] | 3 |
| Wang et al. [95] | Martínez-Herrera et al. [51], Suvan et al. [54], Chaffee et al. [55] | 3 |
| D’aiuto et al. [96] | Kim et al. [46], de Moura-Grec et al. [45], Chaffee et al. [55] | 3 |
| Saxlin et al. [97] | Martínez-Herrera et al. [51], de Moura-Grec et al. [45], Chaffee et al. [55] | 3 |
| Ylöstalo et al. [98] | Martínez-Herrera et al. [51], Suvan et al. [54], Chaffee et al. [55] | 3 |
| Shimazaki et al. [99] | de Moura-Grec et al. [45], Suvan et al. [54], Chaffee et al. [55] | 3 |
| Machado et al. [100] | Kim et al. [46], de Moura-Grec et al. [45], Chaffee et al. [55] | 3 |
| Caracho et al. [101] | Foratori-Junior et al. [42], da Silva et al. [43] | 2 |
| Foratori-Junior et al. [102] | Foratori-Junior et al. [42], da Silva et al. [43] | 2 |
| Fusco et al. [103] | Foratori-Junior et al. [42], da Silva et al. [43] | 2 |
| Deshpande et al. [19] | Abu-Shawish et al. [47], da Silva et al. [43] | 2 |
| Kim et al. [104] | Kim et al. [46], Khairunnisa et al. [48] | 2 |
| Martínez-Herrera et al. [105] | Kim et al. [46], da Silva et al. [43] | 2 |
| Nascimento et al. [106] | Abu-Shawish et al. [47], da Silva et al. [43] | 2 |
| Al Habashneh et al. [107] | Kim et al. [46], da Silva et al. [43] | 2 |
| Balli et al. [108] | da Silva et al. [43], Martínez-Herrera et al. [51] | 2 |
| Öngöz Dede et al. [109] | da Silva et al. [43], Martínez-Herrera et al. [51] | 2 |
| Bouaziz et al. [110] | da Silva et al. [43], Martínez-Herrera et al. [51] | 2 |
| Gonçalves et al. [111] | da Silva et al. [43], Martínez-Herrera et al. [51] | 2 |
| Peng et al. [112] | Martens et al. [50], Li et al. [53] | 2 |
| Nascimento et al. [113] | Martens et al. [50], Li et al. [53] | 2 |
| Scorzetti et al. [114] | Martens et al. [50], Li et al. [53] | 2 |
| Benguigui et al. [115] | Kim et al. [46], da Silva et al. [43] | 2 |
| Kim et al. [116] | Khairunnisa et al. [48], Martínez-Herrera et al. [51] | 2 |
| Modéer et al. [117] | Martens et al. [50], Li et al. [53] | 2 |
| Shimazaki et al. [118] | Kim et al. [46], Chaffee et al. [55] | 2 |
| Li et al. [119] | Kim et al. [46], de Moura-Grec et al. [45] | 2 |
| Pitiphat et al. [120] | de Moura-Grec et al. [45], Chaffee et al. [55] | 2 |
| Saito [121] | Kim et al. [46], de Moura-Grec et al. [45] | 2 |
| Saito et al. [122] | Suvan et al. [54], Chaffee et al. [55] | 2 |
| Wood et al. [123] | de Moura-Grec et al. [45], Chaffee et al. [55] | 2 |
| Alabdulkarin et al. [124] | Suvan et al. [54], Chaffee et al. [55] | 2 |
| Chapper et al. [125] | Suvan et al. [54], Chaffee et al. [55] | 2 |
| Nishida et al. [126] | Suvan et al. [54], Chaffee et al. [55] | 2 |
| Socransky et al. [127] | Suvan et al. [54], Chaffee et al. [55] | 2 |
| Lundin et al. [128] | Khan et al. [49], de Moura-Grec et al. [45] | 2 |
| Buhlin et al. [129] | Suvan et al. [54], Chaffee et al. [55] | 2 |
| Authors | Outcome | Association | |
|---|---|---|---|
| Foratori-Junior et al. [42] | General | RR = 2.21 (1.53–3.17) | Yes |
| Kim et al. [46] | General | OR = 2.21 (1.26–3.89) | Yes |
| 18–34 years | OR = 1.35 (1.05–1.75) | Yes | |
| 35–54 years | OR = 1.53 (1.17–2.00) | Yes | |
| ≥55 years | OR = 1.82 (1.16–2.83) | Yes | |
| United States | OR = 0.59 (0.19–1.65) | No | |
| Brazil | OR = 1.70 (0.78–3.72) | No | |
| European countries | OR = 2.46 (1.11–5.46) | Yes | |
| Korea | OR = 1.34 (1.00–1.80) | Yes | |
| Japan | OR = 1.75 (1.48–2.06) | Yes | |
| Other Asian countries | OR = 0.98 (0.49–1.95) | No | |
| Abu-Shawish et al. [47] | General | OR = 1.77–3.25 | Yes |
| RR = 1.64–1.84 | Yes | ||
| Khairunnisa et al. [48] | General | OR = 1.23 (1.15–1.33) | Yes |
| da Silva et al. [43] | Obese | SMD = 0.05 (−0.20–0.29) | No |
| Overweight | SMD = 0.30 (−0.03–0.62) | No | |
| Overweight or obese | SMD = 0.20 (−0.09–0.48) | No | |
| BOP (obese) | SMD = 0.03 (−0.23–0.28) | No | |
| BOP (Overweight) | SMD = 0.13 (−0.04–0.30) | No | |
| BOP (Overweight or obese) | SMD = 0.20 (−0.05–0.45) | No | |
| GI (obese) | SMD = 0.35 (−0.21–0.91) | No | |
| GI (Overweight) | SMD = 0.97 (0.45–1.49) | Yes | |
| GI (Overweight or obese) | SMD = 0.22 (−0.24–0.68) | No | |
| Obese—G | SMD = 1.10 (0.14–2.05) | Yes | |
| Overweight—G | SMD = 2.08 (−0.60–4.77) | No | |
| Overweight or obese—G | SMD = 2.91 (−0.89–6.72) | No | |
| BOP (obese)—G | SMD = 0.64 (−0.37–1.65) | No | |
| BOP (Overweight)—G | SMD = 0.78 (0.52–1.03) | Yes | |
| BOP (Overweight or obese)—G | SMD = 1.02 (0.77–1.27) | Yes | |
| GI (obese)—G | SMD = 2.13 (−1.51–5.77) | No | |
| GI (Overweight)—G | SMD = 3.52 (2.32–4.71) | Yes | |
| GI (Overweight or obese)—G | SMD = 4.91 (3.64–6.17) | Yes | |
| Khan et al. [49] | General | OR = 1.1–4.5 | Yes |
| Martens et al. [50] | General | OR = 1.46 (1.20–1.77) | Yes |
| Martinez-Herrera et al. [51] | General | OR = 0.99–4.3 | Yes |
| HR = 1.03–3.24 | Yes | ||
| RR = 0.99–5.4 | Yes | ||
| Nascimento et al. [44] | Overweight | RR = 1.13 (1.06–1.20) | Yes |
| Obese | RR = 1.34 (1.21–1.47) | Yes | |
| Keller et al. [52] | Age (obese) | HR = 1.30–3.24 | Yes |
| IRR = 1.3 | Yes | ||
| PR = 1.01 | Yes | ||
| Age (overweight) | HR = 1.09–1.70 | Yes | |
| IRR = 1.2 | Yes | ||
| PR = 0.99 | Yes | ||
| Li et al. [53] | PI > 25% | OR = 4.75 (2.42–9.34) | Yes |
| BOP > 25% | OR = 5.41 (2.75–10.63) | Yes | |
| SBC | OR = 3.07 (1.10–8.62) | Yes | |
| SPC | OR = 1.08 (0.60–1.94) | No | |
| PD > 4 mm | OR = 14.15 (5.10–39.25) | Yes | |
| de Moura-Grec et al. [45] | General | OR = 1.30 (1.25–1.35) | Yes |
| Suvan et al. [54] | Obese | OR = 1.30 (1.25–1.35) | Yes |
| Overweight | OR = 1.81 (1.42–2.30) | Yes | |
| Overweight and obese | OR = 1.27 (1.06–1.51) | Yes | |
| Chaffee et al. [55] | General | OR = 1.35 (1.23–1.47) | Yes |
| Obese | OR = 1.52 (1.26–1 83) | Yes | |
| Overweight | OR = 1.18 (1.00–1.39) | Yes | |
| East Asia | OR = 1.32 (1.19–1.47) | Yes | |
| Europe and Middle East | OR = 1.87 (1.17–2.99) | Yes | |
| United States | OR = 1.30 (1.16–1.46) | Yes | |
| Men | OR = 1.50 (1.27–1.77) | Yes | |
| Women | OR = 1.75 (1.26–2.43) | Yes | |
| Young | OR = 1.35 (1.14–1.59) | Yes | |
| Older | OR = 1.21 (1.04–1.41) | Yes | |
| Smoker | OR = 1.36 (0.98–1.88) | No | |
| Non-smoker | OR = 2.08 (1.29–3.36) | Yes | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arbildo-Vega, H.I.; Cruzado-Oliva, F.H.; Coronel-Zubiate, F.T.; Aguirre-Ipenza, R.; Meza-Málaga, J.M.; Luján-Valencia, S.A.; Luján-Urviola, E.; Farje-Gallardo, C.A. Association between Periodontal Disease and Obesity: Umbrella Review. Medicina 2024, 60, 621. https://doi.org/10.3390/medicina60040621
Arbildo-Vega HI, Cruzado-Oliva FH, Coronel-Zubiate FT, Aguirre-Ipenza R, Meza-Málaga JM, Luján-Valencia SA, Luján-Urviola E, Farje-Gallardo CA. Association between Periodontal Disease and Obesity: Umbrella Review. Medicina. 2024; 60(4):621. https://doi.org/10.3390/medicina60040621
Chicago/Turabian StyleArbildo-Vega, Heber Isac, Fredy Hugo Cruzado-Oliva, Franz Tito Coronel-Zubiate, Rubén Aguirre-Ipenza, Joan Manuel Meza-Málaga, Sara Antonieta Luján-Valencia, Eduardo Luján-Urviola, and Carlos Alberto Farje-Gallardo. 2024. "Association between Periodontal Disease and Obesity: Umbrella Review" Medicina 60, no. 4: 621. https://doi.org/10.3390/medicina60040621
APA StyleArbildo-Vega, H. I., Cruzado-Oliva, F. H., Coronel-Zubiate, F. T., Aguirre-Ipenza, R., Meza-Málaga, J. M., Luján-Valencia, S. A., Luján-Urviola, E., & Farje-Gallardo, C. A. (2024). Association between Periodontal Disease and Obesity: Umbrella Review. Medicina, 60(4), 621. https://doi.org/10.3390/medicina60040621