
Integrating Clinical Neuropsychology and Psychotic Spectrum Disorders: A Systematic Analysis of Cognitive Dynamics, Interventions, and Underlying Mechanisms




Abstract
:1. Introduction
2. Literature Review
2.1. Neurobiological Pattern in Psychotic Spectrum
2.2. Neurocognitive Pattern in Psychotic Spectrum
2.3. Neuropsychological Functioning of Dementia Patients with Psychosis
2.4. Adverse Childhood Events as Cognitive Neuromarkers in Psychosis
2.5. Neuropsychological Interventions and Rehabilitation in Psychotic Spectrum
- [RQ1—Cognitive Impairments and Brain Abnormalities] How do psychotic spectrum disorders affect memory, attention, and executive function, and how do they relate to prefrontal cortex, hippocampus, and thalamus abnormalities?
- [RQ2—Diagnostic Importance of Neuropsychological Tests] What role do neuropsychological tests play in diagnosing cognitive deficits, and how can they predict psychotic disorders?
- [RQ3—Effectiveness of Intervention Strategies] How effective are current cognitive rehabilitation interventions and therapies for psychotic spectrum disorder patients, and what is the potential for future research?
- [RQ4—Role of Genetic and Environmental Factors] What role do genetic and environmental factors play in schizophrenia and risks of other psychotic spectrum disorders?
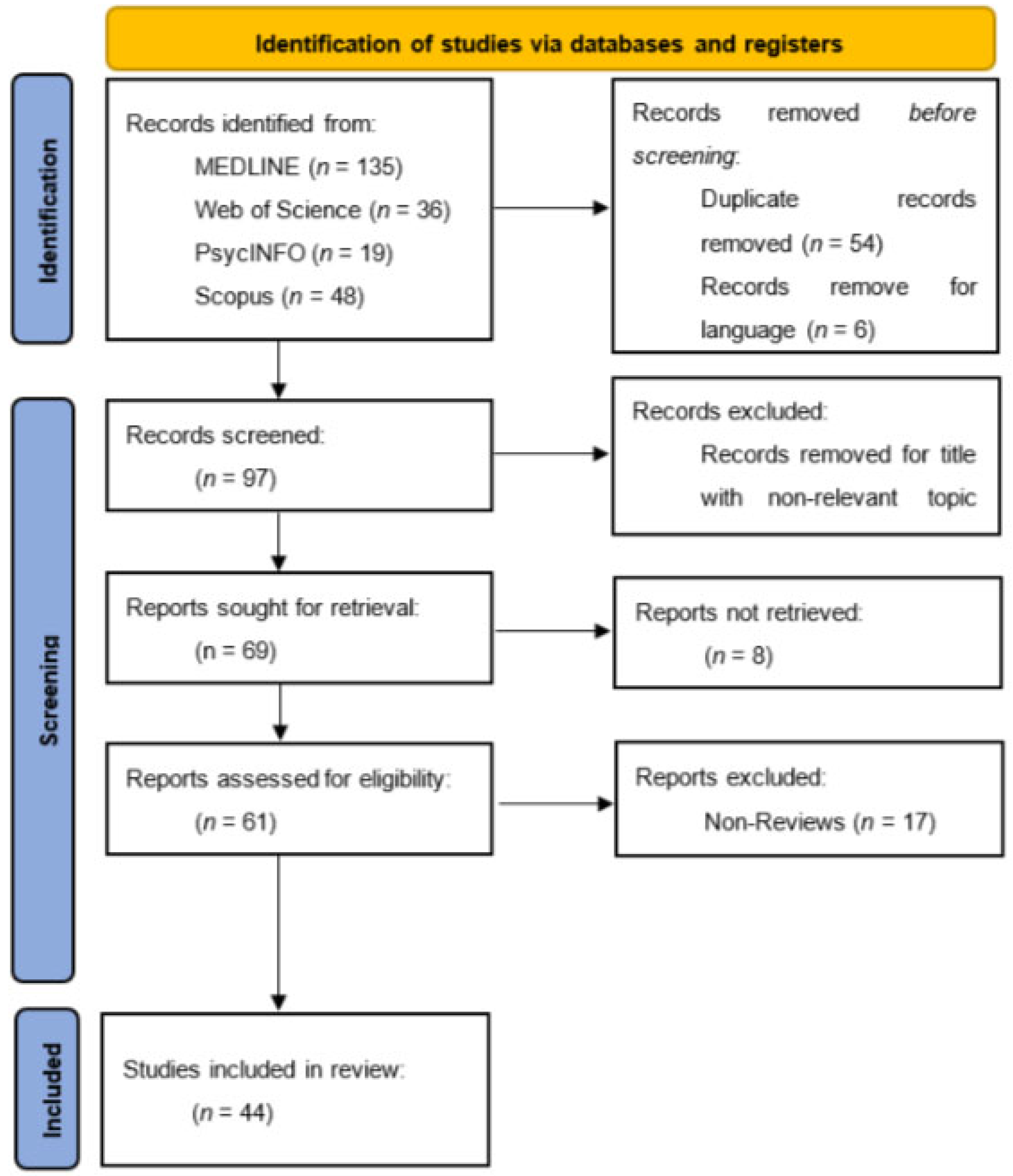
3. Materials and Methods
Query String: TITLE-ABS-KEY (“psychotic spectrum” OR “schizophrenia” OR “bipolar disorder” OR “depression”) AND (“clinical neuropsychology” OR “cognitive neuropsychology”) AND (“memory” OR “attention” OR “executive function”) AND (“brain regions” OR “neurobiology” OR “neuroimaging”)
4. Results
- In individuals with a high familial risk, psychotic symptoms were linked to a smaller cross-sectional surface area and progressive cortical thinning. This suggests the illness’s brain structure changes may start in childhood and adolescence.
- Early overlap in the occipital cortex between schizophrenia (SzO) and bipolar (BpO) offspring suggests shared neurodevelopmental pathways.
- Both individuals with psychotic spectrum symptoms and those without showed a lesser decrease in total surface area, suggesting different trajectories of surface area change over time for familial risk for schizophrenia versus bipolar.
- Both a history of psychosis and a diagnosis of BD-I were associated with more pronounced global cognitive impairment compared to BD-II and NPBD.
- Individuals with BD-I underperformed in specific cognitive domains, such as verbal memory, processing speed, executive function (EF) speed, and EF accuracy, compared to those with BD-II.
- Psychotic BD was associated with significantly impaired cognition compared to NPBD across various cognitive domains.
- Patients with acute psychosis had significantly higher plasma concentrations of proinflammatory markers such as CRP, CCL2, IL1RA, IL6, IL8, and TNFα and lower concentrations of neuroendocrine pathway markers such as KA and KA/Kyn. These markers normalized after treatment.
- The levels of nitrite, another immune marker, increased sharply after the initiation of antipsychotic medication.
- Positive symptoms during the acute episode correlated with proinflammatory markers, while negative symptoms correlated inversely with IDO pathway markers.
5. Discussion
- [RQ1] Cognitive impairments in memory, attention, and executive function are significantly more pronounced in individuals with psychotic spectrum disorders compared to the general population, and these impairments are correlated with structural and functional abnormalities in specific brain regions such as the prefrontal cortex, hippocampus, and thalamus.
- [RQ2] Neuropsychological tests are reliable diagnostic tools that can identify cognitive deficiencies early in the disease process of psychotic disorders and can predict the onset and progression of these conditions.
- [RQ3] Intervention strategies focused on cognitive rehabilitation can significantly improve cognitive functions in patients with psychotic spectrum disorders, highlighting the potential for new therapeutic approaches based on neuroplasticity and cognitive training.
- [RQ4] Genetic predispositions, combined with environmental stressors, significantly increase the risk of developing psychotic spectrum disorders, suggesting that early intervention and prevention strategies should target high-risk individuals with a familial history of these disorders.
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Heinrichs, R.W.; Zakzanis, K.K. Neurocognitive Deficit in Schizophrenia: A Quantitative Review of the Evidence. Neuropsychology 1998, 12, 426–445. [Google Scholar] [CrossRef] [PubMed]
- Hill, S.; Reilly, J.P.; Harris, M.S.; Rosen, C.; Marvin, R.S.; DeLeon, O.; Sweeney, J.A. A Comparison of Neuropsychological Dysfunction in First-episode Psychosis Patients with Unipolar Depression, Bipolar Disorder, and Schizophrenia. Schizophr. Res. 2009, 113, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Bilder, R.M.; Goldman, R.; Robinson, D.; Reiter, G.; Bell, L.M.; Bates, J.A.; Lieberman, J.A. Neuropsychology of First-episode Schizophrenia: Initial Characterization and Clinical Correlates. Am. J. Psychiatry 2000, 157, 549–559. [Google Scholar] [CrossRef]
- Gkintoni, E.; Pallis, E.G.; Bitsios, P.; Giakoumaki, S.G. Neurocognitive performance, psychopathology and social functioning in individuals at high risk for schizophrenia or psychotic bipolar disorder. J. Affect. Disord. 2017, 208, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Harvey, P.D.; Keefe, R.S. Studies of Cognitive Change in Patients with Schizophrenia Following Novel Antipsychotic Treatment. Am. J. Psychiatry 2001, 158, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Mwesiga, E.K.; Akena, D.; Koen, N.; Senono, R.; Ea, O.; Gumikiriza, J.L.; Robbins, R.N.; Nakasujja, N.; Stein, D.J. A Systematic Review of Brief Neuropsychological Tests in Use Among Patients with Psychotic Disorders in Low and Middle Income Countries. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Gaebel, W.; Zielasek, J. Focus on psychosis. Dialogues Clin. Neurosci. 2015, 17, 9–18. [Google Scholar] [CrossRef] [PubMed]
- González, L.E.; López-Carrilero, R.; Barrigón, M.L.; Grasa, E.; Barajas, A.; Pousa, E.; González-Higueras, F.; Ruiz-Delgado, I.; Cid, J.; Lorente-Rovira, E.; et al. Neuropsychological functioning and jumping to conclusions in recent onset psychosis patients. Schizophr. Res. 2018, 195, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Hart, M.; Lewine, R.R. Rethinking thought disorder. Schizophr. Bull. 2017, 43, 514–522. [Google Scholar] [CrossRef]
- Gkintoni, E. Clinical neuropsychological characteristics of bipolar disorder, with a focus on cognitive and linguistic pattern: A conceptual analysis. F1000Research 2023, 12, 1235. [Google Scholar] [CrossRef]
- Howes, O.D.; Kapur, S. The Dopamine Hypothesis of Schizophrenia: Version Iii--the Final Common Pathway. Schizophr. Bull. 2009, 35, 549–562. [Google Scholar] [CrossRef]
- Sheffield, J.M.; Kandala, S.; Tamminga, C.A.; Pearlson, G.D.; Keshavan, M.S.; Sweeney, J.A.; Clementz, B.A.; Lerman-Sinkoff, D.B.; Hill, S.K.; Deanna, M. Transdiagnostic Associations Between Functional Brain Network Integrity and Cognition. JAMA Psychiatry 2017, 74, 605. [Google Scholar] [CrossRef]
- Sheffield, J.M.; Karcher, N.R.; Deanna, M. Cognitive Deficits in Psychotic Disorders: A Lifespan Perspective. Neuropsychol. Rev. 2018, 28, 509–533. [Google Scholar] [CrossRef]
- Velakoulis, D.; Wood, S.J.; Wong, M.H.; McGorry, P.D.; Yung, A.R.; Phillips, L.J.; Smith, D.; Brewer, W.; Proffitt, T.; Desmond, P.; et al. Hippocampal and Amygdala Volumes According to Psychosis Stage and Diagnosis. Arch. Gen. Psychiatry 2006, 63, 139. [Google Scholar] [CrossRef]
- Devenney, E.; Tu, K.; Caga, J.; Ahmed, R.M.; Ramsey, E.; Zoing, M.C.; Kwok, J.; Halliday, G.M.; Piguet, O.; Hodges, J.R.; et al. Neural Mechanisms of Psychosis Vulnerability and Perceptual Abnormalities in the Als-ftd Spectrum. Ann. Clin. Transl. Neurol. 2021, 8, 1576–1591. [Google Scholar] [CrossRef]
- Östling, S.; Gustafson, D.; Blennow, K.; Börjesson-Hanson, A.; Waern, M. Psychotic Symptoms in a Population-based Sample of 85-year-old Individuals with Dementia. J. Geriatr. Psychiatry Neurol. 2010, 24, 3–8. [Google Scholar] [CrossRef]
- Bora, E.; Binnur Akdede, B.; Alptekin, K. Neurocognitive impairment in deficit and non-deficit schizophrenia: A meta-analysis. Psychol. Med. 2017, 47, 2401–2413. [Google Scholar] [CrossRef]
- Mesholam-Gately, R.I.; Giuliano, A.J.; Goff, K.P.; Faraone, S.V.; Seidman, L.J. Neurocognition in First-episode Schizophrenia: A Meta-analytic Review. Neuropsychology 2009, 23, 315–336. [Google Scholar] [CrossRef]
- Reilly, J.P.; Sweeney, J.A. Generalized and Specific Neurocognitive Deficits in Psychotic Disorders: Utility for Evaluating Pharmacological Treatment Effects and as Intermediate Phenotypes for Gene Discovery. Schizophr. Bull. 2014, 40, 516–522. [Google Scholar] [CrossRef]
- Bora, E.; Murray, R.M. Meta-analysis of Cognitive Deficits in Ultra-high Risk to Psychosis and First-episode Psychosis: Do the Cognitive Deficits Progress Over, Or After, the Onset of Psychosis? Schizophr. Bull. 2013, 40, 744–755. [Google Scholar] [CrossRef]
- Sheffield, J.M.; Kandala, S.; Burgess, G.C.; Harms, M.P.; Deanna, M. Cingulo-opercular Network Efficiency Mediates the Association Between Psychotic-like Experiences and Cognitive Ability in the General Population. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2016, 1, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Brandl, F.; Knolle, F.; Meng, C.; Borgwardt, S. Editorial: Specific Macroscopic Brain Changes in Psychotic Disorders. Front. Hum. Neurosci. 2023, 17, 1141866. [Google Scholar] [CrossRef]
- Engen, M.J.; Lyngstad, S.H.; Ueland, T.; Simonsen, C.; Vaskinn, A.; Smeland, O.B.; Bettella, F.; Lagerberg, T.V.; Djurovic, S.; Andreassen, O.A.; et al. Polygenic Scores for Schizophrenia and General Cognitive Ability: Associations with Six Cognitive Domains, Premorbid Intelligence, and Cognitive Composite Score in Individuals with A Psychotic Disorder and in Healthy Controls. Transl. Psychiatry 2020, 10, 46. [Google Scholar] [CrossRef]
- Deanna, M.; Ceaser, A. Cognition in Schizophrenia: Core Psychological and Neural Mechanisms. Trends Cogn. Sci. 2012, 16, 27–34. [Google Scholar] [CrossRef]
- Green, M.F. What Are the Functional Consequences of Neurocognitive Deficits in Schizophrenia? Am. J. Psychiatry 1996, 153, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, M.W.; Libon, D.J. Neuropsychological functioning of dementia patients with psychosis. Arch. Clin. Neuropsychol. 2005, 20, 771–783. [Google Scholar] [CrossRef]
- Pessoa, R.M.d.P.; Maximiano-Barreto, M.A.; Leite, É.D.M.; Chagas, M.H.N. The Frequency of Psychotic Symptoms in Types of Dementia: A Systematic Review. Dement. Neuropsychol. 2023, 17, e20220044. [Google Scholar] [CrossRef]
- Creese, B.; Arathimos, R.; Aarsland, D.; Ballard, C.; Brooker, H.; Hampshire, A.; Corbett, A.; Ismail, Z. Late-life Onset Psychotic Symptoms and Incident Cognitive Impairment in People without Dementia: Modification by Genetic Risk for Alzheimer’s Disease. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2023, 9, e12386. [Google Scholar] [CrossRef]
- Naimark, D.M.; Jackson, E.; Rockwell, E.; Jeste, D.V. Psychotic Symptoms in Parkinson’s Disease Patients with Dementia. J. Am. Geriatr. Soc. 1996, 44, 296–299. [Google Scholar] [CrossRef]
- Ballard, C.; Lana, M.; Theodoulou, M.; Douglas, S.; McShane, R.; Jacoby, R.; Kossakowski, K.; Yu, L.-M.; Juszczak, E. A Randomised, Blinded, Placebo-controlled Trial in Dementia Patients Continuing or Stopping Neuroleptics (the Dart-ad Trial). PLoS Med. 2008, 5, e76. [Google Scholar] [CrossRef]
- Liew, T.M. Neuropsychiatric Symptoms in Cognitively Normal Older Persons, and the Association with Alzheimer’s and Non-alzheimer’s Dementia. Alzheimer’s Res. Ther. 2020, 12, 35. [Google Scholar] [CrossRef] [PubMed]
- D’Antonio, F.; Di Vita, A.; Zazzaro, G.; Brusà, E.; Trebbastoni, A.; Campanelli, A.; Ferracuti, S.; de Lena, C.; Guariglia, C.; Boccia, M. Psychosis of Alzheimer’s disease: Neuropsychological and neuroimaging longitudinal study. Int. J. Geriatr. Psychiatry 2019, 34, 1689–1697. [Google Scholar] [CrossRef] [PubMed]
- Gurrera, R.J.; Moye, J.; Karel, M.J.; Azar, A.; Armesto, J.C. Cognitive Performance Predicts Treatment Decisional Abilities in Mild to Moderate Dementia. Neurology 2006, 66, 1367–1372. [Google Scholar] [CrossRef] [PubMed]
- Sideli, L. Effect of childhood abuse on cognitive function in first-episode psychosis patients and community controls. Schizophr. Res. 2012, 136, S24. [Google Scholar] [CrossRef]
- Sahin, S.; Ucok, A.; Gode, E.; Yuksel, C. Childhood trauma may be related to transition to psychosis in ultra high risk individuals. Schizophr. Res. 2010, 117, 204. [Google Scholar] [CrossRef]
- Lardinois, M.; Lataster, T.; Mengelers, R.; Van Os, J.; Myin-Germeys, I. Childhood trauma and increased stress sensitivity in psychosis. Acta Psychiatr. Scand. 2010, 123, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Sarchiapone, M.; Carli, V.; Cuomo, C.; Marchetti, M.; Roy, A. Association between childhood trauma and aggression in male prisoners. Psychiatry Res. 2009, 165, 187–192. [Google Scholar] [CrossRef]
- Amador, X.F.; David, A.S. (Eds.) Inside knowledge: Cultural constructions of insight in psychosis. In Insight and Psychosis; Oxford University Press: Oxford, UK, 2004; pp. 197–230. [Google Scholar] [CrossRef]
- David, A.; Kemp, R. Five Perspectives on the Phenomenon of Insight in Psychosis. Psychiatr. Ann. 1997, 27, 791–797. [Google Scholar] [CrossRef]
- Bendall, S.; Alvarez-Jimenez, M.; Nelson, B.; McGorry, P. Childhood trauma and psychosis: New perspectives on aetiology and treatment. Early Interv. Psychiatry 2013, 7, 1–4. [Google Scholar] [CrossRef]
- Krabbendam, L. Childhood psychological trauma and psychosis. Psychol. Med. 2008, 38, 1405–1408. [Google Scholar] [CrossRef]
- Ahmed-Leitao, F.; Rosenstein, D.; Marx, M.; Young, S.; Korte, K.; Seedat, S. Posttraumatic stress disorder, social anxiety disorder and childhood trauma: Differences in hippocampal subfield volume. Psychiatry Res. Neuroimaging 2019, 284, 45–52. [Google Scholar] [CrossRef]
- Misiak, B.; Krefft, M.; Bielawski, T.; Moustafa, A.A.; Sąsiadek, M.M.; Frydecka, D. Toward a unified theory of childhood trauma and psychosis: A comprehensive review of epidemiological, clinical, neuropsychological and biological findings. Neurosci. Biobehav. Rev. 2017, 75, 393–406. [Google Scholar] [CrossRef]
- Erlich, M.D.; Smith, T.E.; Horwath, E.; Cournos, F. Schizophrenia and Other Psychotic Disorders. In Oxford Medicine Online; Oxford University Press: Oxford, UK, 2014. [Google Scholar] [CrossRef]
- Farah, W.; Alsawas, M.; Mainou, M.; Alahdab, F.; Farah, M.H.; Ahmed, A.T.; Ahmed, A.T.; Mohamed, E.A.; Almasri, J.; Gionfriddo, M.R.; et al. Non-pharmacological Treatment of Depression: A Systematic Review and Evidence Map. Evid. Based Med. 2016, 21, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Gkintoni, E.; Ortiz, P.S. Neuropsychology of Generalized Anxiety Disorder in Clinical Setting: A Systematic Evaluation. Healthcare 2023, 11, 2446. [Google Scholar] [CrossRef]
- Mollon, J.; David, A.S.; Morgan, C.; Frissa, S.; Glahn, D.; Pilecka, I.; Hatch, S.L.; Hotopf, M.; Reichenberg, A. Psychotic experiences and neuropsychological functioning in a population-based sample. JAMA Psychiatry 2016, 73, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Farmakopoulou, I.; Lekka, M.; Gkintoni, E. Clinical Symptomatology of Anxiety and Family Function in Adolescents—The Self-Esteem Mediator. Children 2024, 11, 338. [Google Scholar] [CrossRef]
- Koutsopoulou, I.; Grace, E.; Gkintoni, E.; Olff, M. Validation of the Global Psychotrauma Screen for adolescents in Greece. Eur. J. Trauma Dissociation 2024, 8, 100384. [Google Scholar] [CrossRef]
- Wirgenes, K.V.; Smeland, O.B.; Andreassen, O.A. Genetics of psychotic disorders with focus on early-onset psychosis. In Adolescent Psychosis; Academic Press: Cambridge, MA, USA, 2023; pp. 51–80. [Google Scholar] [CrossRef]
- Cowman, M.; Holleran, L.; Lonergan, E.; O’Connor, K.; Birchwood, M.; Donohoe, G. Cognitive Predictors of Social and Occupational Functioning in Early Psychosis: A Systematic Review and Meta-analysis of Cross-sectional and Longitudinal Data. Schizophr. Bull. 2021, 47, 1243–1253. [Google Scholar] [CrossRef]
- Coutinho, E.; Harrison, P.; Vincent, A. Do Neuronal Autoantibodies Cause Psychosis? A Neuroimmunological Perspective. Biol. Psychiatry 2014, 75, 269–275. [Google Scholar] [CrossRef]
- Northoff, G. Is Our Brain An Open or Closed System? Prediction Model of Brain and World–brain Relation. In The Spontaneous Brain; MIT Press: Cambridge, MA, USA, 2018; pp. 55–76. [Google Scholar] [CrossRef]
- Menkes, M.W.; Armstrong, K.; Heckers, S.; Woodward, N.D. Neuropsychological Functioning in Early and Chronic Stages of Schizophrenia and Psychotic Bipolar Disorder. Schizophr. Res. 2019, 206, 413–419. [Google Scholar] [CrossRef]
- Gkintoni, E.; Vantaraki, F.; Skoulidi, C.; Anastassopoulos, P.; Vantarakis, A. Promoting Physical and Mental Health among Children and Adolescents via Gamification—A Conceptual Systematic Review. Behav. Sci. 2024, 14, 102. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Liu, C.; Chen, Y.; Zhang, Y. Cognitive Dysfunction Following Cerebellar Stroke: Insights Gained from Neuropsychological and Neuroimaging Research. Neural Plast. 2022, 2022, 3148739. [Google Scholar] [CrossRef]
- Carey, M.P.; Carey, K.B.; Maisto, S.A.; Gordon, C.J.; Schroder, K.E.E.; Vanable, P.A. Reducing Hiv-risk Behavior Among Adults Receiving Outpatient Psychiatric Treatment: Results from a Randomized Controlled Trial. J. Consult. Clin. Psychol. 2004, 72, 252–268. [Google Scholar] [CrossRef] [PubMed]
- Oikonomou, V.; Gkintoni, E.; Halkiopoulos, C.; Karademas, E.C. Quality of Life and Incidence of Clinical Signs and Symptoms among Caregivers of Persons with Mental Disorders: A Cross-Sectional Study. Healthcare 2024, 12, 269. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Keshavan, M.S.; Kelly, S.; Hall, M.-H. The Core Deficit of “Classical” Schizophrenia Cuts Across the Psychosis Spectrum. Can. J. Psychiatry 2020, 65, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Nelson, B.; Lavoie, S.; Gawęda, Ł.; Li, E.; Sass, L.A.; Koren, D.; McGorry, P.D.; Jack, B.N.; Parnas, J.; Polari, A.; et al. The neurophenomenology of early psychosis: An integrative empirical study. Conscious. Cogn. 2020, 77, 102845. [Google Scholar] [CrossRef] [PubMed]
- Lewandowski, K.; Bouix, S.; Ongur, D.; Shenton, M. Neuroprogression across the Early Course of Psychosis. J. Psychiatry Brain Sci. 2020, 5, e200002. [Google Scholar] [CrossRef]
- Culbreth, A.J.; Foti, D.; Barch, D.M.; Hajcak, G.; Kotov, R. Electrocortical Responses to Emotional Stimuli in Psychotic Disorders: Comparing Schizophrenia Spectrum Disorders and Affective Psychosis. Front. Psychiatry 2018, 9, 586. [Google Scholar] [CrossRef]
- Sugranyes, G.; de la Serna, E.; Ilzarbe, D.; Pariente, J.C.; Borras, R.; Romero, S.; Rosa, M.; Baeza, I.; Moreno, M.D.; Bernardo, M.; et al. Brain structural trajectories in youth at familial risk for schizophrenia or bipolar disorder according to development of psychosis spectrum symptoms. J. Child Psychol. Psychiatry 2020, 62, 780–789. [Google Scholar] [CrossRef]
- Bora, E. Neurocognitive features in clinical subgroups of bipolar disorder: A meta-analysis. J. Affect. Disord. 2018, 229, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Tian, F.; Wang, S.; Cheng, B.; Qiu, L.; He, M.; Wang, H.; Duan, M.; Dai, J.; Jia, Z. Gray matter bases of psychotic features in adult bipolar disorder: A systematic review and voxel-based meta-analysis of neuroimaging studies. Hum. Brain Mapp. 2018, 39, 4707–4723. [Google Scholar] [CrossRef] [PubMed]
- McCleery, A.; Nuechterlein, K.H. Cognitive impairment in psychotic illness: Prevalence, profile of impairment, developmental course, and treatment considerations. Dialogues Clin. Neurosci. 2019, 21, 239–248. [Google Scholar] [CrossRef]
- Vargas, T.; Lam, P.H.; Azis, M.; Osborne, K.J.; Lieberman, A.; Mittal, V.A. Childhood Trauma and Neurocognition in Adults with Psychotic Disorders: A Systematic Review and Meta-analysis. Schizophr. Bull. 2018, 45, 1195–1208. [Google Scholar] [CrossRef] [PubMed]
- Widmayer, S.; Borgwardt, S.; Lang, U.E.; Stieglitz, R.-D.; Huber, C.G. Functional Neuroimaging Correlates of Aggression in Psychosis: A Systematic Review with Recommendations for Future Research. Front. Psychiatry 2019, 9, 386206. [Google Scholar] [CrossRef]
- Smucny, J.; Lesh, T.A.; Iosif, A.-M.; Niendam, T.A.; Tully, L.M.; Carter, C.S. Longitudinal stability of cognitive control in early psychosis: Nondegenerative deficits across diagnoses. J. Abnorm. Psychol. 2018, 127, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Hallford, D.J.; Sharma, M.K. Anticipatory pleasure for future experiences in schizophrenia spectrum disorders and major depression: A systematic review and meta-analysis. Br. J. Clin. Psychol. 2019, 58, 357–383. [Google Scholar] [CrossRef]
- Dwyer, D.B.; Kalman, J.L.; Budde, M.; Kambeitz, J.; Ruef, A.; Antonucci, L.A.; Kambeitz-Ilankovic, L.; Hasan, A.; Kondofersky, I.; Anderson-Schmidt, H.; et al. An Investigation of Psychosis Subgroups with Prognostic Validation and Exploration of Genetic Underpinnings. JAMA Psychiatry 2020, 77, 523. [Google Scholar] [CrossRef]
- O’Neill, A.; Mechelli, A.; Bhattacharyya, S. Dysconnectivity of Large-Scale Functional Networks in Early Psychosis: A Meta-analysis. Schizophr. Bull. 2018, 45, 579–590. [Google Scholar] [CrossRef]
- Connors, M.H.; Ames, D.; Woodward, M.; Brodaty, H. Psychosis and Clinical Outcomes in Alzheimer Disease: A Longitudinal Study. Am. J. Geriatr. Psychiatry 2018, 26, 304–313. [Google Scholar] [CrossRef]
- Dugré, J.R.; Radua, J.; Carignan-Allard, M.; Dumais, A.; Rubia, K.; Potvin, S. Neurofunctional abnormalities in antisocial spectrum: A meta-analysis of fMRI studies on Five distinct neurocognitive research domains. Neurosci. Biobehav. Rev. 2020, 119, 168–183. [Google Scholar] [CrossRef] [PubMed]
- Vaquerizo-Serrano, J.; Salazar de Pablo, G.; Singh, J.; Santosh, P. Autism Spectrum Disorder and Clinical High Risk for Psychosis: A Systematic Review and Meta-analysis. J. Autism Dev. Disord. 2021, 52, 1568–1586. [Google Scholar] [CrossRef] [PubMed]
- Jonas, K.; Lian, W.; Callahan, J.; Ruggero, C.J.; Clouston, S.; Reichenberg, A.; Carlson, G.A.; Bromet, E.J.; Kotov, R. The Course of General Cognitive Ability in Individuals with Psychotic Disorders. JAMA Psychiatry 2022, 79, 659. [Google Scholar] [CrossRef] [PubMed]
- Demro, C.; Shen, C.; Hendrickson, T.J.; Arend, J.L.; Disner, S.G.; Sponheim, S.R. Advanced Brain-Age in Psychotic Psychopathology: Evidence for Transdiagnostic Neurodevelopmental Origins. Front. Aging Neurosci. 2022, 14, 872867. [Google Scholar] [CrossRef] [PubMed]
- Voineskos, A.N.; Mulsant, B.H.; Dickie, E.W.; Neufeld, N.H.; Rothschild, A.J.; Whyte, E.M.; Meyers, B.S.; Alexopoulos, G.S.; Hoptman, M.J.; Lerch, J.P.; et al. Effects of Antipsychotic Medication on Brain Structure in Patients with Major Depressive Disorder and Psychotic Features. JAMA Psychiatry 2020, 77, 674. [Google Scholar] [CrossRef] [PubMed]
- Waszczuk, K.; Rek-Owodziń, K.; Tyburski, E.; Mak, M.; Misiak, B.; Samochowiec, J. Disturbances in White Matter Integrity in the Ultra-High-Risk Psychosis State—A Systematic Review. J. Clin. Med. 2021, 10, 2515. [Google Scholar] [CrossRef] [PubMed]
- Bloomfield, M.A.P.; Chang, T.; Woodl, M.J.; Lyons, L.M.; Cheng, Z.; Bauer-Staeb, C.; Hobbs, C.; Bracke, S.; Kennerley, H.; Isham, L.; et al. Psychological processes mediating the association between developmental trauma and specific psychotic symptoms in adults: A systematic review and meta-analysis. World Psychiatry 2021, 20, 107–123. [Google Scholar] [CrossRef] [PubMed]
- Viher, P.V.; Stegmayer, K.; Bracht, T.; Federspiel, A.; Bohlhalter, S.; Strik, W.; Wiest, R.; Walther, S. Neurological Soft Signs Are Associated with Altered White Matter in Patients with Schizophrenia. Schizophr. Bull. 2021, 48, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, L.; Werner, D.; Lincoln, T.M. The relevance of cognitive emotion regulation to psychotic symptoms—A systematic review and meta-analysis. Clin. Psychol. Rev. 2019, 72, 101746. [Google Scholar] [CrossRef]
- Wu, J.; Xiao, J. Effectiveness of the Neuroimaging Techniques in the Recognition of Psychiatric Disorders: A Systematic Review and Meta-analysis of RCTs. Curr. Med. Imaging Rev. 2023, 20. [Google Scholar] [CrossRef]
- Howes, O.; Jauhar, S.; Brugger, S.; Pepper, F. 9.2 Brain Structural and Neurochemical Heterogeneity and Homogeneity in Psychotic Disorders: Transdiagnostic PET and MRI Imaging Findings in Schizophrenia and Bipolar Affective Disorder. Schizophr. Bull. 2018, 44 (Suppl. S1), S13. [Google Scholar] [CrossRef]
- Gama Marques, J.; Ouakinin, S. Clinical profile in schizophrenia and schizoaffective spectrum: Relation with unconjugated bilirubin in a prospective and controlled study with psychopathological and psychosocial variables. CNS Spectr. 2019, 25, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Anteraper, S.A.; Guell, X.; Collin, G.; Qi, Z.; Ren, J.; Nair, A.; Seidman, L.J.; Keshavan, M.S.; Zhang, T.; Tang, Y.; et al. Abnormal Function in Dentate Nuclei Precedes the Onset of Psychosis: A Resting-State fMRI Study in High-Risk Individuals. Schizophr. Bull. 2021, 47, 1421–1430. [Google Scholar] [CrossRef] [PubMed]
- Koike, S.; Fujioka, M.; Takano, Y.; Iwashiro, N.; Satomura, Y.; Nagai, T.; Koshiyama, D.; Tada, M.; Natsubori, T.; Okada, N.; et al. Neurocognitive Deficits Mediate the Relationship between Structural Abnormalities and Clinical Outcomes in Individuals with Ultrahigh Risk for Psychosis: A Multimodal Neuroimaging and Longitudinal Neurocognitive Study. Schizophr. Bull. Open 2021, 2, sgab027. [Google Scholar] [CrossRef]
- Ruiz, I.; Raugh, I.M.; Bartolomeo, L.A.; Strauss, G.P. A Meta-Analysis of Neuropsychological Effort Test Performance in Psychotic Disorders. Neuropsychol. Rev. 2020, 30, 407–424. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.S.; Lee, T.Y.; Hwang, W.J.; Kwak, Y.B.; Kim, S.; Moon, S.-Y.; Lho, S.K.; Oh, S.; Kwon, J.S. White Matter Correlates of Theory of Mind in Patients with First-Episode Psychosis. Front. Psychiatry 2021, 12, 617683. [Google Scholar] [CrossRef]
- Torrent, C.; Reinares, M.; Martinez-Arán, A.; Cabrera, B.; Amoretti, S.; Corripio, I.; Contreras, F.; Sarró, S.; González-Pinto, A.; Lobo, A.; et al. Affective versus non-affective first episode psychoses: A longitudinal study. J. Affect. Disord. 2018, 238, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Stein, F.; Buckenmayer, E.; Brosch, K.; Meller, T.; Schmitt, S.; Ringwald, K.G.; Pfarr, J.K.; Steinsträter, O.; Enneking, V.; Grotegerd, D.; et al. Dimensions of Formal Thought Disorder and Their Relation to Gray- and White Matter Brain Structure in Affective and Psychotic Disorders. Schizophr. Bull. 2022, 48, 902–911. [Google Scholar] [CrossRef] [PubMed]
- Muetzel, R.L.; Blanken, L.M.E.; van der Ende, J.; El Marroun, H.; Shaw, P.; Sudre, G.; van der Lugt, A.; Jaddoe, V.W.V.; Verhulst, F.C.; Tiemeier, H.; et al. Tracking Brain Development and Dimensional Psychiatric Symptoms in Children: A Longitudinal Population-Based Neuroimaging Study. Am. J. Psychiatry 2018, 175, 54–62. [Google Scholar] [CrossRef]
- Lepage, M.; Makowski, C.; Bodnar, M.; Chakravarty, M.M.; Joober, R.; Malla, A.K. Do Unremitted Psychotic Symptoms Have an Effect on the Brain? A 2-Year Follow-up Imaging Study in First-Episode Psychosis. Schizophr. Bull. Open 2020, 1, sgaa039. [Google Scholar] [CrossRef]
- Papanastasiou, E.; Mouchlianitis, E.; Joyce, D.W.; McGuire, P.; Banaschewski, T.; Bokde, A.L.W.; Bromberg, U.; Büchel, C.; Quinlan, E.B.; Desrivières, S.; et al. Examination of the Neural Basis of Psychoticlike Experiences in Adolescence During Reward Processing. JAMA Psychiatry 2018, 75, 1043. [Google Scholar] [CrossRef] [PubMed]
- De Picker, L.; Fransen, E.; Coppens, V.; Timmers, M.; de Boer, P.; Oberacher, H.; Fuchs, D.; Verkerk, R.; Sabbe, B.; Morrens, M. Immune and Neuroendocrine Trait and State Markers in Psychotic Illness: Decreased Kynurenines Marking Psychotic Exacerbations. Front. Immunol. 2020, 10, 2971. [Google Scholar] [CrossRef]
- Kuipers, J.; Moffa, G.; Kuipers, E.; Freeman, D.; Bebbington, P. Links between psychotic and neurotic symptoms in the general population: An analysis of longitudinal British National Survey data using Directed Acyclic Graphs. Psychol. Med. 2018, 49, 388–395. [Google Scholar] [CrossRef]
- Sánchez-Morla, E.M.; López-Villarreal, A.; Jiménez-López, E.; Aparicio, A.I.; Martínez-Vizcaíno, V.; Roberto, R.-J.; Vieta, E.; Santos, J.-L. Impact of number of episodes on neurocognitive trajectory in bipolar disorder patients: A 5-year follow-up study. Psychol. Med. 2018, 49, 1299–1307. [Google Scholar] [CrossRef] [PubMed]
- Chendo, I.; Silva, C.; Duarte, G.S.; Prada, L.; Voon, V.; Ferreira, J.J. Frequency and Characteristics of Psychosis in Parkinson’s Disease: A Systematic Review and Meta-Analysis. J. Park. Dis. 2022, 12, 85–94. [Google Scholar] [CrossRef]
- Gur, R.E.; McDonald-McGinn, D.M.; Moore, T.M.; Gallagher, R.S.; McClellan, E.; White, L.; Ruparel, K.; Hillman, N.; Crowley, T.B.; McGinn, D.E.; et al. Psychosis spectrum features, neurocognition and functioning in a longitudinal study of youth with 22q11.2 deletion syndrome. Psychol. Med. 2023, 53, 6763–6772. [Google Scholar] [CrossRef]
- Haukvik, U.K.; Tamnes, C.K.; Söderman, E.; Agartz, I. Neuroimaging hippocampal subfields in schizophrenia and bipolar disorder: A systematic review and meta-analysis. J. Psychiatr. Res. 2018, 104, 217–226. [Google Scholar] [CrossRef]
- Rössler, J.; Unterassner, L.; Wyss, T.; Haker, H.; Brugger, P.; Rössler, W.; Wotruba, D. Schizotypal Traits are Linked to Dopamine-Induced Striato-Cortical Decoupling: A Randomized Double-Blind Placebo-Controlled Study. Schizophr. Bull. 2018, 45, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, S.; Di Fazio, C.; Mazzà, M.; Tamietto, M.; Avenanti, A. Targeting Human Glucocorticoid Receptors in Fear Learning: A Multiscale Integrated Approach to Study Functional Connectivity. Int. J. Mol. Sci. 2024, 25, 864. [Google Scholar] [CrossRef]
- Battaglia, S.; Avenanti, A.; Vécsei, L.; Tanaka, M. Neural Correlates and Molecular Mechanisms of Memory and Learning. Int. J. Mol. Sci. 2024, 25, 2724. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Sample | Outcomes Measured | Main Findings |
|---|---|---|---|
| Keshavan et al., 2020 [60] | Total: 446 | The main or primary outcome measured in the study is the functional outcome in psychotic disorders, particularly related to cognitive impairments and mismatch negativity (MMN) as a biomarker of psychosis. |
|
| Nelson et al., 2020 [61] | Total: 123 (Ultra-high risk for psychosis: 50—First-episode psychosis: 39—Healthy controls: 34) | Examination of Anomalous Self-Experience (EASE) scores. The primary outcomes of this study offer valuable insights into the initial stages of psychosis, underscoring the significance of incorporating both neurobiological and phenomenological dimensions in both research and clinical settings. |
|
| Lewandowski et al., 2020 [62] | Total: 228 | Neuroprogressive trajectories of neurocognition, structural brain measures, and network connectivity over the first eight years of illness and their predictive utility on clinical and functional outcomes. |
|
| Culbreth et al., 2018 [63] | Total: 74 | The main or primary outcome measured in the study is the association between late positive potential (LPP) amplitude and symptom severity in individuals diagnosed with affective psychosis and individuals with schizophrenia, including concurrent and prospective associations with symptoms. |
|
| Sugranyes et al., 2020 [64] | Total: 128 (SzO: 33—BpO: 46—Controls: 49) | Longitudinal changes in measures of brain structure, including cortical thickness, surface area, and gray matter volume, in children and adolescents at familial high risk (FHR) for bipolar disorder or schizophrenia who experienced psychotic spectrum symptoms over time. |
|
| Bora, 2018 [65] | Total: 2047 (BD-I: 1211—BD-II: 836) Total: 1761 (PBD: 1017—NPBD: 744) | Cognitive impairment in different subgroups of bipolar disorder, including BD-I and BD-II, as well as subgroups based on history of psychosis (PBD and NPBD). |
|
| Wang et al., 2018 [66] | Total: 616 (PBD patients and 902 healthy subjects) | GMV differences between PBD patients and HC, specifically involving the prefronto-temporal and cingulate cortices, precentral gyrus, and insula. |
|
| McCleery and Nuechterlein, 2019 [67] | Total: 105 | The main or primary outcome measured in the study is not explicitly stated. However, based on the content of the paper, the main or primary outcome measured seems to be the prevalence, profile, and magnitude of cognitive impairment in psychotic disorders, as well as the longitudinal stability of cognitive impairment. |
|
| Vargas et al., 2018 [68] | Total: 3315 | Association between childhood trauma and overall neurocognitive function in individuals with psychotic disorders. Relationship between childhood trauma and working memory in individuals with psychotic disorders. |
|
| Widmayer et al., 2019 [69] | Total: 334 patients and 113 controls (236 patients and 92 HC subjects) | Through the comparison of brain imaging data across different groups, the study sought to unveil the specific neural correlates of aggression in psychosis. |
|
| Smucny et al., 2018 [70] | Total: 193 (SZ: 65—Schizophreniform: 2—Schizoaffective: 13—BD type I with psychotic features: 27—Healthy controls: 86) | Using advanced neurocognitive assessments and longitudinal study designs, researchers can delve deeper into the nature of cognitive impairments and their effects on individuals across different diagnostic categories. |
|
| Hallford and Sharma, 2019 [71] | Total: 4221 (Schizophrenia spectrum: 3300—Major depression: 921) | Self-reported anticipatory pleasure in individuals with psychiatric disorders compared to control groups. |
|
| Dwyer et al., 2020 [72] | Total: 1223 (Discovery sample: 765—Validation sample: 458) | Subtype-specific illness courses including psychosis symptoms, depression symptoms, global functioning, and quality of life; polygenic scores for schizophrenia, bipolar disorder, major depression disorder, and educational achievement. |
|
| O’Neill et al., 2018 [73] | Total: 526 (combined HC groups), 420 (combined patient groups) | Functional connectivity (FC) of the default mode (DMN), salience (SN), and central executive networks (CENs) in patients with first-episode psychosis (FEP) compared to healthy controls. |
|
| Connors et al., 2018 [74] | Total: 445 | The main or primary outcome measured in the study includes neuropsychiatric symptoms, dementia severity, cognition, function, caregiver burden, medication use, and mortality. |
|
| Dugré et al., 2020 [75] | Total: 2555 | Functional brain deficits in individuals with conduct problems (CPs) and their adult form, adult antisocial behaviors, across distinct neurocognitive domains, including acute threat response, social cognition, cognitive control, and punishment and reward processing. |
|
| Vaquerizo-Serrano et al., 2021 [76] | Total: 16,474 (CHR-P: 875) | The primary outcome measured in the study is the presence of ASD in CHR-P individuals. |
|
| Jonas et al., 2022 [77] | Total: 428 | Preadmission cognitive scores extracted from school and medical records and postonset cognitive scores based on neuropsychological testing at 6-month, 24-month, 20-year, and 25-year follow-ups. |
|
| D’Antonio et al., 2019 [32] | Total: 40 (AD + P: 20—AD-P: 20—HC: 20) | Impairment in specific cognitive domains predicting the onset of psychosis in AD patients, gray matter alterations, their location, and the rate of atrophy associated with psychosis of AD. |
|
| Demro et al., 2022 [78] | Total: 332 (Schizophrenia: 105—Schizoaffective: 17—Bipolar I disorder with psychotic features: 41—First-degree biological relatives: 103—Controls: 66—Completed both studies: 42—Bipolar I disorder without psychosis: 15—Relatives of individuals with bipolar I disorder without psychosis: 7) | Advanced brain age measured using the Brain-Age Regression Analysis and Computation Utility Software (BARACUS, v1.1.2) prediction model, compared between individuals with a primary psychotic disorder and people with bipolar I disorder with a history of psychotic symptoms, as well as their biological first-degree relatives. The study also examined the association between advanced brain age and cognitive functioning, general functioning, and clinical diagnostic boundaries. |
|
| Voineskos et al., 2020 [79] | Total: 88 | Primary outcome: cortical thickness in gray matter. Secondary outcome: microstructural integrity of white matter. |
|
| Waszczuk et al., 2021 [80] | Total: 881 | The presence of subtle abnormalities in white matter tracts connecting the frontal and temporal lobes, especially the SLF, ILF, and IFOF. |
|
| Bloomfield et al., 2021 [81] | Total: 24,793 (Clinical: 1639—Nonclinical: 23,154) | The potential roles of psychological processes in the associations between developmental trauma and specific psychotic experiences (i.e., hallucinations, delusions, and paranoia) in adulthood. |
|
| Viher et al., 2021 [82] | Total: 83 | Association between neurological soft signs (NSSs) and white matter alterations in adults with schizophrenia. |
|
| Ludwig et al., 2019 [83] | Total: 2498 | Effectiveness of emotion regulation strategies in patients with psychotic disorders, specifically the association between maladaptive strategies and positive symptoms. |
|
| Wu and Xiao, 2023 [84] | Total: 655 | The primary outcome measured in the study is detecting brain abnormalities in diverse psychiatric illnesses with neuroimaging versus conventional methods. |
|
| Howes et al., 2018 [85] | Total: 38 (Schizophrenia: 16—Bipolar affective disorder: 22) | Striatal dopamine synthesis capacity (Kicer), correlation of Kicer with positive psychotic symptom severity. |
|
| Gama Marques and Ouakinin, 2019 [86] | Total: 192 (SCZ: 44—SAF: 44—Bipolar controls: 44—Follow-up patients: 60—SCZ: 30—SAF: 30) | Assessment of unconjugated bilirubin (UCB) as a biomarker for schizophrenia (SCZ) and schizoaffective (SAF) spectrum disorder during relapse and partial remission. |
|
| Anteraper et al., 2021 [87] | Total: 237 (CHR-: 144— CHR+: 23—HC: 93) | Resting-state functional connectivity (RsFc) differences in the dentate nuclei (DN) that may precede the onset of psychosis in individuals at risk of developing schizophrenia. |
|
| Koike et al., 2021 [88] | Total: 50 (Female: 23) | The relationship between neurocognitive deficits and improvements in UHR individuals and their association with symptom severity outcomes, as well as the paths from brain structural and functional characteristics to neurocognitive function and symptom severity outcomes. |
|
| Ruiz et al., 2020 [89] | Total: 2205 | Effort failure rate and moderators of effort test. A comprehensive analysis of neuropsychological effort test performance in individuals with psychotic disorders, providing valuable insights into their cognitive profiles. |
|
| Kim et al., 2021 [90] | Total: 64 (FEP: 35—Healthy Controls: 29) | The correlation between ToM strange story scores and the FA values of the left cingulum and left SLF in patients with FEP. |
|
| Torrent et al., 2018 [91] | Total: 192 (Nonaffective psychoses: 142—Affective psychoses: 50) | Functioning at follow-up, assessed by a regression model composed of PANSS total score and verbal fluency assessed by the FAS (COWAT). |
|
| Stein et al., 2022 [92] | Total: 1071 | Association of FTD dimensions with GMV and FA, establishment of a transdiagnostic factor model of FTD, and linking psychopathological factors to brain structural measures across disorders. |
|
| Muetzel et al., 2018 [93] | Total: 845 | Association between psychiatric symptoms (externalizing and internalizing) at baseline and the changes in subcortical gray matter volume and global fractional anisotropy over time. |
|
| Lepage et al., 2020 [94] | Total: 80 | Change in cortical thickness and volume of the hippocampus as a function of the duration of unremitted positive symptoms. |
|
| Papanastasiou et al., 2018 [95] | Total: 1434 (High PLEs: 149—Low PLEs: 149) | Brain activation during a monetary incentive delay reward task in healthy adolescents at ages 14 and 19 years old. |
|
| De Picker et al., 2020 [96] | Total: 101 (Patients: 49—Healthy control subjects: 52) | Identification of state and trait markers in the peripheral immune system and two immune-associated neuroendocrine pathways (IDO and GTP-CH1 pathways) in a longitudinal sample of psychosis patients. |
|
| Kuipers et al., 2018 [97] | Total: 8580 (Follow-up subsample: 2406) | Persecutory ideation, hallucinations, affective symptoms, effects of cannabis and problematic alcohol use. |
|
| Sánchez-Morla et al., 2018 [98] | Total: 139 (Euthymic bipolar patients: 99—Healthy controls: 40) | Change in neurocognitive composite index (NCI) over a 5-year follow-up period, specifically in relation to the number of manic and hypomanic episodes experienced by bipolar patients, as well as its association with working memory and visual memory. |
|
| Chendo et al., 2022 [99] | Total: 2919 for psychosis and 3161 for any form of hallucination | Frequency of psychosis and any form of hallucination in PD patients. |
|
| Gur et al., 2023 [100] | Total: 157 (PS+: 98—PS-: 59) | Differences in the trajectories of psychosis symptoms and neurocognitive performance between the PS+ and PS- groups and the impact on functional outcome. |
|
| Haukvik et al., 2018 [101] | Total: 2393 (Schizophrenia patients: 909—Bipolar disorder patients: 625—Healthy controls: 1089) | Hippocampal subfield volumes or shape in schizophrenia and bipolar disorder. |
|
| Rössler et al., 2018 [102] | Total: 54 (L-DOPA: 33—Placebo: 32) | The main or primary outcome measured in the study is the significant functional decoupling from the right ventral caudate to both occipital fusiform gyri. |
|
| Neuropsychological Test | Cognitive Domain Assessed | Relevance to Dementia and Psychosis |
|---|---|---|
| Wechsler Memory Scale (WMS) | Memory and learning | Essential for assessing both episodic and working memory deficits common in dementia and psychosis. |
| Trail Making Test (TMT) Parts A and B | Attention, processing speed, executive function | Useful for evaluating cognitive flexibility and processing speed, which are often impaired in both conditions. |
| Wisconsin Card Sorting Test (WCST) | Executive function, problem-solving | Helps in assessing abstract thinking and the ability to shift cognitive strategies in response to changing environmental contingencies, challenges seen in both dementia and psychosis. |
| Rey–Osterrieth Complex Figure Test (ROCFT) | Visuoconstructive abilities, memory | Assesses the ability to organize and remember complex visual information, reflecting on visuoperceptual and executive deficits. |
| Verbal Fluency Tests (Semantic and Phonemic) | Language, executive function | Evaluates language function and executive processes related to generating strategies for retrieval, often affected by both dementia and psychosis. |
| Digit Span Test (Forward and Backward) | Attention, working memory | Measures attentional capacity and working memory, crucial for understanding the extent of cognitive decline. |
| Stroop Color and Word Test | Attention, processing speed, executive function | Assesses cognitive flexibility and susceptibility to interference, a common issue in cognitive impairments associated with dementia and psychosis. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gkintoni, E.; Skokou, M.; Gourzis, P. Integrating Clinical Neuropsychology and Psychotic Spectrum Disorders: A Systematic Analysis of Cognitive Dynamics, Interventions, and Underlying Mechanisms. Medicina 2024, 60, 645. https://doi.org/10.3390/medicina60040645
Gkintoni E, Skokou M, Gourzis P. Integrating Clinical Neuropsychology and Psychotic Spectrum Disorders: A Systematic Analysis of Cognitive Dynamics, Interventions, and Underlying Mechanisms. Medicina. 2024; 60(4):645. https://doi.org/10.3390/medicina60040645
Chicago/Turabian StyleGkintoni, Evgenia, Maria Skokou, and Philippos Gourzis. 2024. "Integrating Clinical Neuropsychology and Psychotic Spectrum Disorders: A Systematic Analysis of Cognitive Dynamics, Interventions, and Underlying Mechanisms" Medicina 60, no. 4: 645. https://doi.org/10.3390/medicina60040645
APA StyleGkintoni, E., Skokou, M., & Gourzis, P. (2024). Integrating Clinical Neuropsychology and Psychotic Spectrum Disorders: A Systematic Analysis of Cognitive Dynamics, Interventions, and Underlying Mechanisms. Medicina, 60(4), 645. https://doi.org/10.3390/medicina60040645