


Adherence to the Mediterranean Diet in Saudi Arabia and Its Association with Socioeconomic Status and Depression

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
- -
- n is the required sample size;
- -
- Z is the Z-score corresponding to the desired confidence level (e.g., for a 95% confidence level, Z ≈ 1.96);
- -
- p is the estimated prevalence;
- -
- E is the desired margin of error (expressed as a proportion).
2.2. Data Collection
2.3. Study Outcomes
2.4. Variables and Data Analysis
2.5. Ethical Considerations
3. Results
3.1. Factors Associated with Adherence to the MedDiet
3.2. Adherence to the MedDiet and Objective Material Status
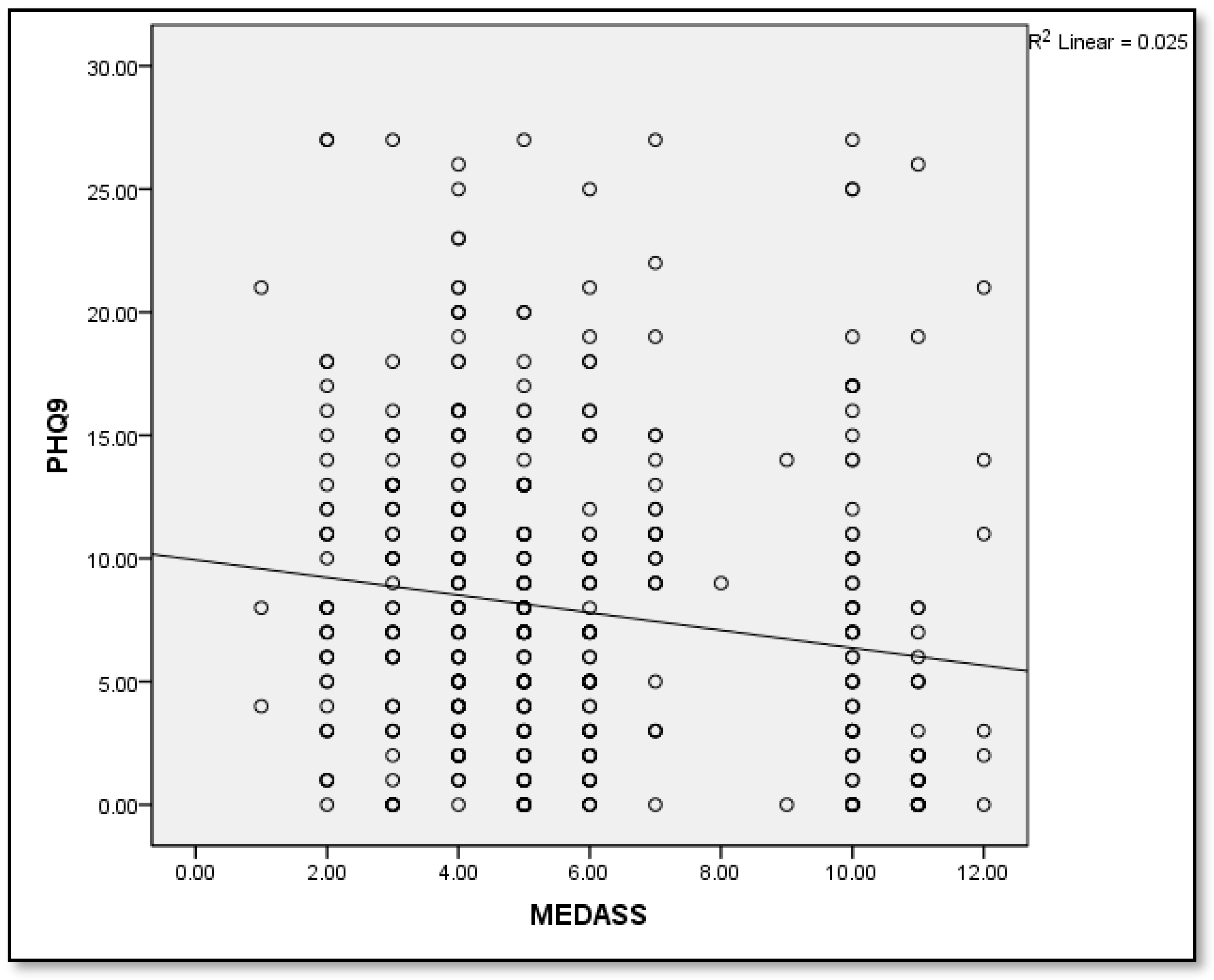
3.3. Adherence to the Meddiet and Mental Health Status
3.4. Association between Adherence to the Mediterranean Diet and Chronic Diseases
4. Discussion
5. Conclusions and Prospectives
6. Limitations of This Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Frost, J.C.; Baldwin, A.J. ‘Food for thought’: The importance of nutrition to patient care and the role of the junior doctor. Clin. Med. 2021, 21, e272–e274. [Google Scholar] [CrossRef] [PubMed]
- Ruthsatz, M.; Candeias, V. Non-communicable disease prevention, nutrition and aging. Acta Biomed. 2020, 11, 379–388. [Google Scholar] [CrossRef]
- Serin, Y.; Akbulut, G.; Yaman, M. Investigating bioaccessibility of advanced glycation product precursors in gluten-free foods using in vitro gastrointestinal system. Medicina 2023, 59, 1578. [Google Scholar] [CrossRef] [PubMed]
- Russell, M. Registered dietitian nutritionists should be included in patient health care teams. Am. Fam. Physician 2019, 1, 142–143. [Google Scholar]
- van den Brink, A.C.; Brouwer-Brolsma, E.M.; Berendsen, A.A.M.; van de Rest, O. The Mediterranean Dietary Approaches to Stop Hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) diets are associated with less cognitive decline and a lower risk of Alzheimer’s disease—A review. Adv. Nutr. 2019, 10, 1040–1065. [Google Scholar] [CrossRef] [PubMed]
- Yu, E.; Malik, V.S.; Hu, F.B. Cardiovascular disease prevention by diet modification: JACC health promotion series. J. Am. Coll. Cardiol. 2018, 72, 2951–2963. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.L.; Pei, W.; Chen, T.C.; Hsu, M.C.; Chen, P.C.; Kuo, H.M.; Hung, J.F.; Chen, Y.L. Optimized sugar-free citrus lemon juice fermentation efficiency and the lipid-lowering effects of the fermented juice. Nutrients 2023, 15, 5089. [Google Scholar] [CrossRef] [PubMed]
- Zou, S.F.; Jiang, B.; Wan, R.; Huang, Y. The adverse association of animal zinc intake with cardio-cerebrovascular and metabolic risk factors. Int. J. Cardiol. Cardiovasc. Risk Prev. 2023, 20, 200231. [Google Scholar] [CrossRef] [PubMed]
- Opie, R.S.; Itsiopoulos, C.; Parletta, N.; Sanchez-Villegas, A.; Akbaraly, T.N.; Ruusunen, A.; Jacka, F.N. Dietary recommendations for the prevention of depression. Nutr. Neurosci. 2017, 20, 161–171. [Google Scholar] [CrossRef]
- Visser, M.; Sealy, M.J.; Leistra, E.; Naumann, E.; van der Schueren, M.A.E.; Wittenaar, H.J. The Malnutrition Awareness Scale for community-dwelling older adults: Development and psychometric properties. Clin. Nutr. 2024, 43, 446–452. [Google Scholar] [CrossRef]
- Chen, W.; Zhang, S.; Hu, X.; Chen, F.; Li, D. A Review of Healthy Dietary Choices for Cardiovascular Disease: From Individual Nutrients and Foods to Dietary Patterns. Nutrients 2023, 15, 4898. [Google Scholar] [CrossRef]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Martinez-Lacoba, R.; Pardo-Garcia, I.; Amo-Saus, E.; Escribano-Sotos, F. Mediterranean diet and health outcomes: A systematic meta-review. Eur. J. Public Health 2018, 28, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Grajek, M.; Krupa-Kotara, K.; Bialek-Dratwa, A. Nutrition and mental health: A review of current knowledge about the impact of diet on mental health. Front. Nutr. 2022, 9, 943998. [Google Scholar] [CrossRef]
- Bayes, J.; Schloss, J.; Sibbritt, D. The effect of a Mediterranean diet on the symptoms of depression in young males (the “AMMEND: A Mediterranean Diet in MEN with Depression” study): A randomized controlled trial. Am. J. Clin. Nutr. 2022, 116, 572–580. [Google Scholar] [CrossRef]
- Jacka, F.N.; O’Neil, A.; Opie, R.; Itsiopoulos, C.; Cotton, S.; Mohebbi, M.; Castle, D.; Dash, S.; Mihalopoulos, C.; Chatterton, M.L.; et al. A randomised controlled trial of dietary improvement for adults with major depression (the ‘SMILES’ trial). BMC Med. 2017, 15, 23. [Google Scholar] [CrossRef] [PubMed]
- Flor-Alemany, M.; Baena-Garcia, L.; Migueles, J.H.; Henriksson, P.; Lof, M.; Aparicio, V.A. Associations of Mediterranean diet with psychological ill-being and well-being throughout the pregnancy course: The GESTAFIT project. Qual. Life Res. 2022, 31, 2705–2716. [Google Scholar] [CrossRef]
- Bosdriesz, J.R.; Stel, V.S.; van Diepen, M.; Meuleman, Y.; Dekker, F.W.; Zoccali, C.; Jager, K.J. Evidence-based medicine-When observational studies are better than randomized controlled trials. Nephrology 2020, 25, 737–743. [Google Scholar] [CrossRef]
- Shafiei, F.; Salari-Moghaddam, A.; Larijani, B.; Esmaillzadeh, A. Adherence to the Mediterranean diet and risk of depression: A systematic review and updated meta-analysis of observational studies. Nutr. Rev. 2019, 77, 230–239. [Google Scholar] [CrossRef]
- Pribisalić, A.; Popović, R.; Salvatore, F.P.; Vatavuk, M.; Mašanović, M.; Hayward, C.; Polašek, O.; Kolčić, I. The Role of Socioeconomic Status in Adherence to the Mediterranean Diet and Body Mass Index Change: A Follow-Up Study in the General Population of Southern Croatia. Nutrients 2021, 13, 3802. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; Burns, J.K.; Dhingra, M.; Tarver, L.; Kohrt, B.A.; Lund, C. Income inequality and depression: A systematic review and meta-analysis of the association and a scoping review of mechanisms. World Psychiatry 2018, 17, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, Y.; Shobugawa, Y.; Nozaki, I.; Takagi, D.; Nagamine, Y.; Funato, M.; Chihara, Y.; Shirakura, Y.; Lwin, K.T.; Zin, P.E.; et al. Association between depressive symptoms and objective/subjective socioeconomic status among older adults of two regions in Myanmar. PLoS ONE 2021, 16, e0245489. [Google Scholar] [CrossRef] [PubMed]
- AlOmar, R.S.; Parslow, R.C.; Law, G.R. Development of two socioeconomic indices for Saudi Arabia. BMC Public Health 2018, 18, 791. [Google Scholar] [CrossRef] [PubMed]
- García-Conesa, M.T.; Philippou, E.; Pafilas, C.; Massaro, M.; Quarta, S.; Andrade, V.; Jorge, R.; Chervenkov, M.; Ivanova, T.; Dimitrova, D.; et al. Exploring the Validity of the 14-Item Mediterranean Diet Adherence Screener (MEDAS): A Cross-National Study in Seven European Countries around the Mediterranean Region. Nutrients 2020, 12, 2960. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Feart, C.; Samieri, C.; Rondeau, V. Adherence to a Mediterranean diet, cognitive decline, and risk of dementia. JAMA 2009, 302, 638–648. [Google Scholar] [CrossRef] [PubMed]
- Chrysohoou, C.; Tsitsinakis, G.; Siassos, G. Fish Consumption Moderates Depressive Symptomatology in Elderly Men and Women from the IKARIA Study. Cardiol. Res. Pract. 2010, 2011, 219578. [Google Scholar] [CrossRef]
- Luciano, M.; Mottus, R.; Starr, J.M. Depressive symptoms and diet: Their effects on prospective inflammation levels in the elderly. Brain Behav. Immun. 2012, 26, 717–720. [Google Scholar] [CrossRef]
- Antonogeorgos, G.; Panagiotakos, D.B.; Pitsavos, C. Understanding the role of depression and anxiety on cardiovascular disease risk, using structural equation modeling; the mediating effect of the Mediterranean diet and physical activity: The ATTICA study. Ann. Epidemiol. 2012, 22, 630–637. [Google Scholar] [CrossRef]
- Rienks, J.; Dobson, A.J.; Mishra, G.D. Mediterranean dietary pattern and prevalence and incidence of depressive symptoms in mid-aged women: Results from a large community-based prospective study. Eur. J. Clin. Nutr. 2013, 67, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Crichton, G.E.; Bryan, J.; Hodgson, J.M.; Murphy, K.J. Mediterranean diet adherence and self-reported psychological functioning in an Australian sample. Appetite 2013, 70, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Hansson, M.; Chotai, J.; Nordstom, A.; Bodlund, O. Comparison of two self-rating scales to detect depression: HADS and PHQ-9. Br. J. Gen. Pract. 2009, 59, e283–e288. [Google Scholar] [CrossRef] [PubMed]
- Milette, K.; Hudson, M.; Baron, M.; Thombs, B.D.; Canadian Scleroderma Research Group. Comparison of the PHQ-9 and CES-D depression scales in systemic sclerosis: Internal consistency reliability, convergent validity and clinical correlates. Rheumatology 2010, 49, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Wang, S.; Wang, L.; Yi, X.; Jia, X.; Jia, C. Comparison of the Geriatric Depression Scale-15 and the Patient Health Questionnaire-9 for screening depression in older adults. Geriatr. Gerontol. Int. 2020, 20, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Hadjimbei, E.; Botsaris, G.; Gekas, V.; Panayiotou, A.G. Adherence to the Mediterranean Diet and Lifestyle Characteristics of University Students in Cyprus: A Cross-Sectional Survey. J. Nutr. Metab. 2016, 2016, 2742841. [Google Scholar] [CrossRef] [PubMed]
- Marventano, S.; Godos, J.; Platania, A.; Galvano, F.; Mistretta, A.; Grosso, G. Mediterranean diet adherence in the Mediterranean healthy eating, aging and lifestyle (MEAL) study cohort. Int. J. Food Sci. Nutr. 2018, 69, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Lotfi, K.; Saneei, P.; Hajhashemy, Z.; Esmaillzadeh, A. Adherence to the Mediterranean Diet, Five-Year Weight Change, and Risk of Overweight and Obesity: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. Adv. Nutr. 2022, 13, 152–166. [Google Scholar] [CrossRef]
- Ubago-Jimenez, J.L.; Zurita-Ortega, F.; San Roman-Mata, S.; Puertas-Molero, P.; Gonzalez-Valero, G. Impact of Physical Activity Practice and Adherence to the Mediterranean Diet in Relation to Multiple Intelligences among University Students. Nutrients 2020, 12, 2630. [Google Scholar] [CrossRef]
- Survey of Access & Usage Households & Individuals to ICT. 2021. Available online: https://www.stats.gov.sa/sites/default/files/ICT%202021%20-%20kp%20-%20E.pdf (accessed on 27 December 2023).


{kind=link}
| Variables | Overall n (%) | Adherent n (%) | Non-Adherent n (%) | Test | p |
|---|---|---|---|---|---|
| Overall | 467 (100) | 98 (21) | 369 (79) | ||
| Sex | |||||
| Male | 105 (22.5) | 19 (19.4) | 86 (23.3) | 0.68 | 0.41 |
| Female | 362 (77.5) | 79 (80.6) | 283 (76.7) | ||
| Age group | |||||
| 18–25 | 197 (42.2) | 40 (40.8) | 157 (42.5) | 5.57 | 0.14 |
| 26–35 | 93 (19.9) | 24 (24.5) | 69 (18.7) | ||
| 36–45 | 85 (18.2) | 11 (11.2) | 74 (20.1) | ||
| ≥46 | 92 (19.7) | 23 (23.5) | 69 (18.7) | ||
| Education | |||||
| None | 4 (0.9) | 3 (3.1) | 1 (0.3) | 12.57 | 0.014 * |
| High school | 131 (28.1) | 23 (23.5) | 108 (29.3) | ||
| Graduate | 251 (53.7) | 52 (53.1) | 199 (53.9) | ||
| Diploma | 39 (8.4) | 6 (6.1) | 33 (8.9) | ||
| Postgraduate | 42 (9) | 14 (14.3) | 28 (7.6) | ||
| Employment/occupation status | |||||
| Unemployed | 3 (0.6) | 1 (1) | 2 (0.5) | 6.51 | 0.58 |
| Employed | 167 (35.8) | 39 (39.8) | 128 (34.7) | ||
| Student | 166 (35.5) | 36 (36.7) | 130 (35.2) | ||
| Intern | 2 (0.4) | 0 (0) | 2 (0.5) | ||
| Housewife | 84 (18) | 11 (11.2) | 73 (19.8) | ||
| Retired | 35 (7.5) | 9 (9.2) | 26 (7) | ||
| Searching for work | 7 (1.5) | 1 (1) | 6 (1.6) | ||
| Graduated | 1 (0.2) | 0 (0) | 1 (0.3) | ||
| Private Work | 2 (0.4) | 1 (1) | 1 (0.3) | ||
| Marital status | |||||
| Single | 209 (44.8) | 42 (42.9) | 167 (45.3) | 1.04 | 0.79 |
| Married | 237 (50.7) | 52 (53.1) | 185 (50.1) | ||
| Widowed | 3 (0.6) | 0 (0) | 3 (0.8) | ||
| Divorced | 18 (3.9) | 4 (4.1) | 14 (3.8) | ||
| Nationality | |||||
| Saudi | 429 (91.9) | 89 (90.8) | 340 (92.1) | 0.18 | 0.67 |
| Non-Saudi | 38 (8.1) | 9 (9.2) | 29 (7.9) | ||
| Province | |||||
| Southern | 63 (13.5) | 21 (21.4) | 42 (11.4) | 8.46 | 0.08 |
| Northern | 35 (7.5) | 4 (4.1) | 31 (8.4) | ||
| Central | 25 (5.4) | 4 (4.1) | 21 (5.7) | ||
| Western | 252 (54) | 52 (53.1) | 200 (54.2) | ||
| Eastern | 92 (19.7) | 17 (17.3) | 75 (20.3) | ||
| Smoking | 102 (21.8) | 24 (24.5) | 78 (21.1) | 0.51 | 0.47 |
| Exercise | |||||
| Do not exercise | 234 (50.1) | 34 (34.7) | 200 (54.2) | 12.08 | 0.007 * |
| Once per week | 86 (18.4) | 22 (22.4) | 64 (17.3) | ||
| Twice per week | 66 (14.1) | 19 (19.4) | 47 (12.7) | ||
| ≥3 times per week | 81 (17.3) | 23 (23.5) | 58 (15.7) | ||
| BMI (kg/m2), mean ± SD | 25.56 ± 0.27 | 25.49 ± 0.53 | 25.57 ± 0.32 | 0.12 | 0.90 |
| Variables | Overall n (%) | Adherent n (%) | Non-Adherent n (%) | Test | p |
|---|---|---|---|---|---|
| Home type | |||||
| Villa | 152 (32.5) | 30 (30.6) | 122 (33.1) | 9.10 | 0.11 |
| Apartment | 168 (36) | 30 (30.6) | 138 (37.4) | ||
| Traditional House | 105 (22.5) | 30 (30.6) | 75 (20.3) | ||
| Floor in Traditional House | 40 (8.6) | 7 (7.1) | 33 (8.9) | ||
| Duplex | 1 (0.2) | 1 (1) | 0 (0) | ||
| Rented Apartment | 1 (0.2) | 0 (0) | 1 (0.3) | ||
| Tenure of housing | |||||
| Owned | 342 (73.2) | 73 (74.5) | 269 (72.9) | 3.60 | 0.16 |
| Rented | 112 (24) | 25 (25.5) | 87 (23.6) | ||
| Provided | 13 (2.8) | 0 (0) | 13 (3.5) | ||
| Car ownership | |||||
| No car | 249 (53.3) | 51 (52) | 198 (53.7) | 0.35 | 0.83 |
| One car | 155 (33.2) | 32 (32.7) | 123 (33.3) | ||
| Two or more cars | 63 (13.5) | 15 (15.3) | 48 (13) | ||
| Phone ownership | 447 (95.7) | 93 (94.9) | 354 (95.9) | 0.20 | 0.65 |
| TV ownership | 370 (79.2) | 87 (88.8) | 283 (76.7) | 6.86 | 0.009 * |
| PC ownership | 356 (76.2) | 81 (82.7) | 275 (74.5) | 2.82 | 0.09 |
| Internet | 377 (80.7) | 74 (75.5) | 303 (82.1) | 2.17 | 0.14 |
| Satellite | 84 (18) | 19 (19.4) | 65 (17.6) | 0.16 | 0.68 |
| Video games | 137 (29.3) | 26 (26.5) | 111 (30.1) | 0.47 | 0.49 |
| Video player | 83 (17.8) | 15 (15.3) | 68 (18.4) | 0.51 | 0.47 |
| Library | 124 (26.6) | 25 (25.5) | 99 (26.9) | 0.08 | 0.78 |
| Total | Adhered | Did Not Adhere | Test | p | |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |||
| MEDAS | 5.74 ± 0.13 | 10.45 ± 0.06 | 4.49 ± 0.07 | 40.43 | <0.001 * |
| PHQ-9 | 7.89 ± 0.29 | 6.16 ± 0.68 | 8.35 ± 0.31 | 3.12 | 0.002 * |
| PHQ-9 Grading | n (%) | n (%) | n (%) | Test | p |
| Non-Minimal (0–4) | 161 (34.5) | 51 (52) | 110 (29.8) | 18.46 | <0.001 * |
| Mild (5–9) | 143 (30.6) | 24 (24.5) | 119 (32.2) | ||
| Moderate (10–14) | 90 (19.3) | 10 (10.2) | 80 (21.7) | ||
| Moderately Severe (15–19) | 48 (10.3) | 8 (8.2) | 40 (10.8) | ||
| Severe (20–27) | 25 (5.4) | 5 (5.1) | 20 (5.4) |
| Variables | Overall n (%) | Adherent n (%) | Non-Adherent n (%) | Test | p |
|---|---|---|---|---|---|
| Presence of Chronic Disease | |||||
| No | 371 (79.4) | 79 (80.6) | 292 (79.1) | 7.20 | 0.10 |
| Yes | 96 (20.6) | 19 (19.4) | 77 (20.9) | ||
| Type of chronic disease | |||||
| Diabetes Mellitus (DM) | 19 (4.1) | 2 (2) | 17 (4.6) | 14.13 | 0.74 |
| Gestational Diabetes | 1 (0.2) | 1 (1) | 0 (0) | ||
| Hypertension (HTN) | 17 (3.6) | 5 (5.1) | 12 (3.3) | ||
| DM, HTN, and Hyperlipidemia | 13 (2.8) | 4 (4.1) | 9 (2.4) | ||
| Chronic Heart Disease | 3 (0.6) | 1 (1) | 2 (0.5) | ||
| Autoimmune Disease | 9 (1.9) | 1 (1) | 8 (2.2) | ||
| G6PD Deficiency | 2 (0.4) | 1 (1) | 1 (0.3) | ||
| Irritable Bowel Syndrome and Polycystic Ovary Syndrome | 2 (0.4) | 0 (0) | 2 (0.5) | ||
| Rheumatoid Arthritis, Knee Affection, Psoriasis, Anemia, and Depression | 1 (0.2) | 0 (0) | 1 (0.3) | ||
| Asthma and Sinusitis | 3 (0.6) | 0 (0) | 3 (0.8) | ||
| Thyroid Disease | 4 (0.9) | 0 (0) | 4 (1.1) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alnabulsi, M.; Imam, A.A.; Alawlaqi, A.A.; Alhawaj, F.H.; Jamjoom, G.F.; Alsaeidi, L.D.; Hassan, F.E.-S.; Ansari, S.A. Adherence to the Mediterranean Diet in Saudi Arabia and Its Association with Socioeconomic Status and Depression. Medicina 2024, 60, 642. https://doi.org/10.3390/medicina60040642
Alnabulsi M, Imam AA, Alawlaqi AA, Alhawaj FH, Jamjoom GF, Alsaeidi LD, Hassan FE-S, Ansari SA. Adherence to the Mediterranean Diet in Saudi Arabia and Its Association with Socioeconomic Status and Depression. Medicina. 2024; 60(4):642. https://doi.org/10.3390/medicina60040642
Chicago/Turabian StyleAlnabulsi, Majed, Ahmad Abdullah Imam, Atheer Ahmed Alawlaqi, Fatimah Hussain Alhawaj, Ghazal Fareed Jamjoom, Lina Dakhil Alsaeidi, Fatma El-Sayed Hassan, and Shakeel Ahmed Ansari. 2024. "Adherence to the Mediterranean Diet in Saudi Arabia and Its Association with Socioeconomic Status and Depression" Medicina 60, no. 4: 642. https://doi.org/10.3390/medicina60040642
APA StyleAlnabulsi, M., Imam, A. A., Alawlaqi, A. A., Alhawaj, F. H., Jamjoom, G. F., Alsaeidi, L. D., Hassan, F. E.-S., & Ansari, S. A. (2024). Adherence to the Mediterranean Diet in Saudi Arabia and Its Association with Socioeconomic Status and Depression. Medicina, 60(4), 642. https://doi.org/10.3390/medicina60040642