Abstract
Background and Objectives: Atopic dermatitis is a chronic inflammatory skin disorder with a significant burden on patients’ quality of life. This systematic review aims to evaluate the restoration of skin barrier abnormalities with interleukin-4/interleukin-13 (IL-4/IL-13) inhibitors and Janus kinase (JAK) inhibitors in atopic dermatitis. Materials and Methods: A comprehensive review of the literature was conducted, focusing on studies that assess the use of IL-4/IL-13 inhibitors and JAK inhibitors for atopic dermatitis. We identified eligible studies by searching Medline via PubMed with a special focus on their effect on the restoration of the epidermal barrier. Included studies evaluated the transepidermal water loss (TEWL), the reduction in epidermal thickness (ET), the improvement in ceramide synthesis, and the increase in stratum corneum hydration (SCH) with IL-4/IL-13 inhibitors and JAK inhibitors. The quality of included studies was assessed using the ROBINS-I and the RoB 2.0 tool for assessing the risk of bias. Results: Ten of the included studies concern dupilumab, while two concern JAK inhibitors. Ten were observational studies and two were randomized controlled trials (RCTs). The total number of included participants was 378 concerning dupilumab and 38 concerning JAK inhibitors. Five studies did not include any comparison group, three included healthy volunteers, two were conducted versus placebo, and two compared dupilumab with other treatments. The follow-up period ranged between 29 days and 32 weeks. The results demonstrated a significant decrease in transepidermal water loss (TEWL) and an increase in SCH on eczematous lesions for patients with sustained response to dupilumab treatment and observed improvements in ET and filaggrin (FLG) staining, which further support the efficacy of JAK inhibitors in enhancing skin barrier function. Conclusions: This review underscores the efficacy of IL-4/IL-13 inhibitors in improving skin barrier function. However, the limited number of studies focusing on JAK inhibitors and the overall lack of RCTs highlight the need for further research to establish the definitive role of IL-4/IL-13 inhibitors and JAK inhibitors in the restoration of the skin barrier.
1. Introduction
Atopic dermatitis (AD) is a chronic inflammatory skin disorder characterized by dry, itchy, and inflamed skin. It is often associated with other atopic comorbidities such as allergic rhinitis and asthma.
Atopic dermatitis affects up to 20% of children and 3% of adults worldwide, with a higher prevalence in developed countries [1]. The disorder typically follows a course of episodes with exacerbation and remission. Although AD pathogenesis is complex and multifactorial, it is well established that two key factors are involved in its pathogenesis: epidermal barrier disruption leading to an increase in transepidermal water loss (TEWL), and immune dysregulation mainly consisting of T-helper 2 (Th2) and T-helper 22 (Th22) pathway upregulation. This results in overproduction of type 2 inflammation-related cytokines, such as interleukin-4 (IL-4), interleukin-13 (IL-13), interleukin-5 (IL-5), interleukin-31 (IL-31), and interleukin -22 (IL-22) [2]. However, AD immunological endotypes are characterized by heterogeneity. Recently, four distinct pediatric clusters have been identified: TH2 cell/retinol (dominant), skin-homing (dominant), TH1 cell/TH2 cell/TH17 cell/IL-1 (dominant), and TH1 cell/IL-1/eosinophil (inferior) clusters. These clusters differ from adult clusters previously reported and could potentially be useful as biomarkers of disease severity [3].
More than 90% of AD patients are colonized with Staphylococcus aureus (S. aureus) on both lesional and non-lesional skin compared with <5% of healthy individuals, promoting inflammation and disruption of the barrier [4]. In addition, S. aureus can induce T-cell-independent B cell expansion, upregulate proinflammatory cytokines, such as thymic stromal lymphopoietin (TSLP), IL-4, IL-12, and IL-22, and stimulate mast cell degranulation, which results in Th2 skewing and skin inflammation [5]. It is presumed that the differences and shifts in skin microbiome according to atopic dermatitis status are associated with the production of bacteriocins and antimicrobial peptides (AMPs) from symbiotic bacteria [6].
Genetic variants of filaggrin (FLG) are found in 15–40% of atopic dermatitis patients, and decreased levels of filaggrin and filaggrin-like proteins (hornerin and filaggrin family member 2) are found in lesional and non-lesional skin of atopic dermatitis patients [2]. Underlying inflammation can alter the expression of genes such as FLG that are involved in epidermal-barrier function, allowing increased transepidermal penetration of environmental allergens and, in collaboration with pruritus, further inflammation and sensitization [7].
The ceramide ratio and ceramide/cholesterol ratio have been reported to be reduced in atopic dermatitis skin. Hyperactivity of kallikrein (KLK) along with increased levels of interferon α (IFN-a) produce structural changes in free fatty acid and ceramide chains through an augmented degradation of very long chain fatty acid proteins (ELOV) and impair the barrier [2].
Tight junctions (TJs) between keratinocytes act as a selective second physical barrier, controlling cellular permeability. Decreased levels of the transmembrane protein claudin-1 (CLDN1), a major component of TJs, are strongly associated with atopic dermatitis, leading to barrier function impairment and increased inflammation [2,8]. It has also been stated that abnormalities in TJs unfavorably affect epidermal lipids and metabolic processes associated with FLG [9].
A potential role of DNA methylation in allergic diseases and AD has been under research recently. DNA methylation controls the expression of genes in B cells, T cells, and mast cells. This could potentially modify immunological responses and inflammation pathways in AD. Atmospheric pollutants, smoking, climate factors, microbiota, and parasites have been reported to affect DNA methylation [10].
Interleukin-4 (IL-4) decreases the expression of multiple genes in the epidermal differentiation complex that regulate epidermal barrier function. Keratinocytes differentiated in the presence of IL-4 and IL-13 exhibited significantly reduced FLG gene expression, even in patients without filaggrin mutations. Aside from filaggrin, loricrin and involucrin are also downregulated by IL-4 and IL-13 in lesional and non-lesional atopic dermatitis skin, contributing to a defective skin barrier that allows penetration of bacteria and allergens into the skin, leading to infections and allergen sensitization [11]. Th2 polarization facilitates S. aureus binding and colonization, and IL-4 and IL-13 inhibit skin production of AMPs, predisposing atopic dermatitis skin to S. aureus infections, which, in turn, further exacerbates skin inflammation and barrier defects. Mechanistically, it has been shown that IL-4 and IL-13 inhibit tumor necrosis factor-α (TNF-α) and interferon-γ (IFN-γ induced human β-defensin 3 via activation of signal transducer and activator of transcription-6 (STAT-6) production in keratinocytes), as well as TNF-α-induced cathelicidin production. T-helper 2 (Th2) and T-helper 22 (Th22) responses are intensified in chronic atopic dermatitis lesions, with parallel activation of the Th1 axis, rather than a “switch” to a Th1-only signature, and IL-22 has also been identified as a key mediator of epidermal hyperplasia [12].
Keratinocytes in atopic dermatitis skin also express high levels of thymic stromal lymphopoietin (TSLP), a member of the cytokine family. Thymic stromal lymphopoietin induces the maturation of dendritic cells to express OX40L, which in turn differentiates naive CD4+ T cells into Th2 cells to produce Th2 cytokines such as IL-4, IL-5, and IL-13, leading to the secretion of IgE from B cells. Together with the activation of innate lymphoid 2 cells (ILC2s), TSLP initiates the innate and adaptive immune responses of atopic dermatitis [11]. Dieckol and phloxine O reduce atopic dermatitis-like inflammatory symptoms by inhibiting TSLP production [9].
Consequently, the interaction between the immunological component and the epidermal dysfunction component of AD pathogenesis is highly interwoven. The objective of this review was to evaluate the efficacy of IL-4/IL-13 inhibitors and JAK inhibitors concerning the restoration of skin barrier abnormalities in atopic dermatitis.
2. Materials and Methods
A systematic search was undertaken to identify all relevant studies. Studies were identified using an online search of Medline via PubMed. Literature search strategies were developed using both free text words and medical subject headings (MeSH). More specifically, the review was designed using the search algorithm (atopic dermatitis[MeSH Terms]) AND ((janus kinase inhibitors[MeSH Terms]) OR (interleukins[MeSH Terms])) and also (dupilumab) AND (skin barrier) and (janus kinase inhibitors) AND (skin barrier). The last search was performed on 18 April 2024. The reference lists of included studies or relevant reviews identified through the search were scanned and a bibliography of the included articles was additionally checked. The inclusion/exclusion criteria were studies with patients with AD treated with dupilumab or JAKs and also evaluating skin barrier function. Articles written in any language other than English were excluded as well as case series, case reports, and conference abstracts. Only one researcher (IC) reviewed the titles and the abstracts of the studies obtained in the first search in order to include relevant studies. Subsequently, the full texts of all articles meeting the inclusion criteria were reviewed as well as their bibliographic references for additional studies. The variables assessed were the number of all included participants, number of patients treated with dupilumab or Janus kinase inhibitors, age, sex (male/female ratio), comparator, weeks of follow-up, parameters used to evaluate skin barrier function (TEWL or any other parameter), and the measurement location.
3. Results
3.1. Study Selection Process and Study Characteristics
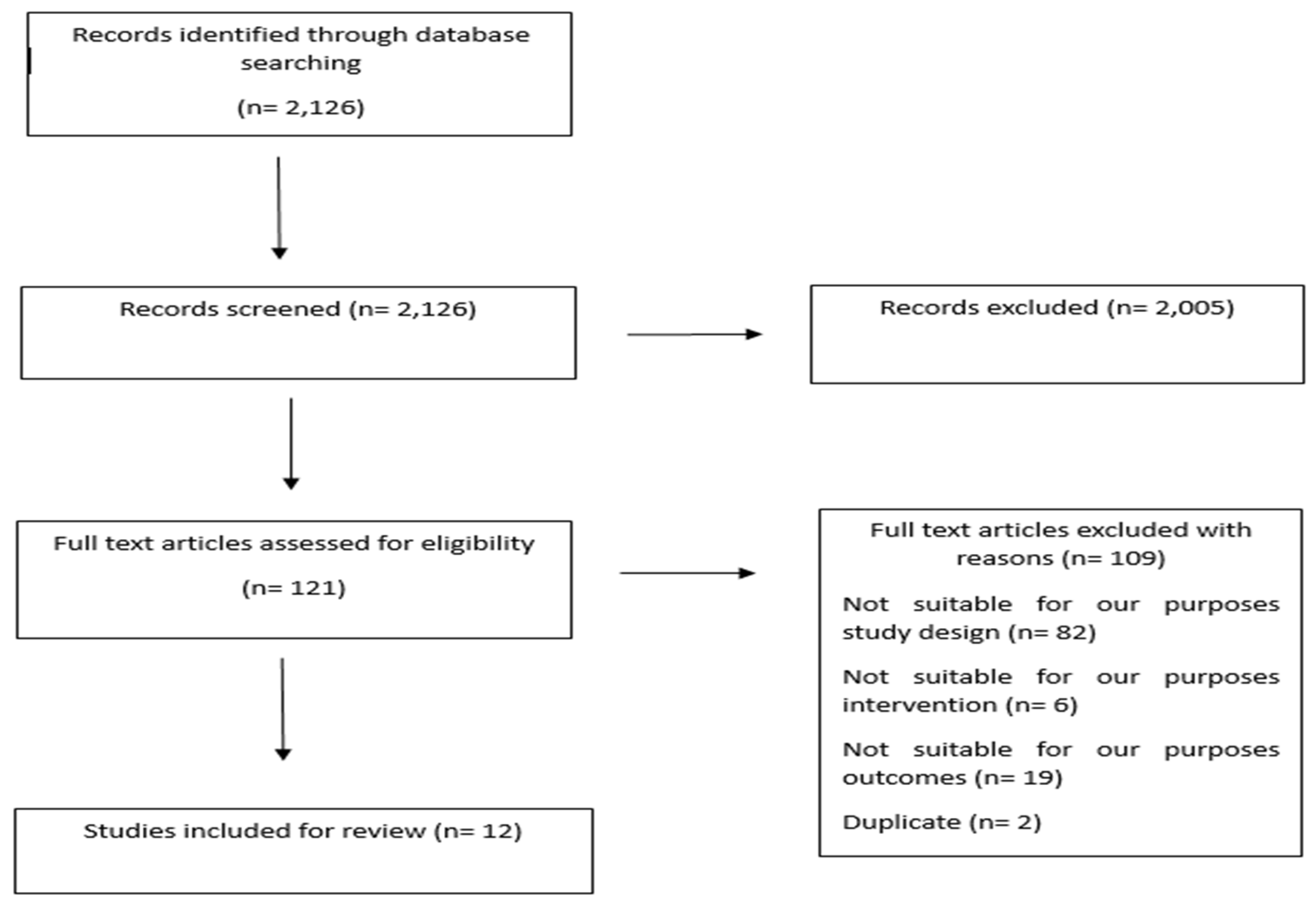
Search algorithm (atopic dermatitis[MeSH Terms]) AND ((janus kinase inhibitors[MeSH Terms]) OR (interleukins[MeSH Terms])) identified 1973 references, search algorithm (dupilumab) AND (skin barrier) and search algorithm (janus kinase inhibitors) AND (skin barrier) identified 102 and 51 references respectively. In total, the literature search identified 2126 references. After title and abstract review, 121 records underwent full-text screening. A total of 12 studies met the eligibility criteria and were included in the review, while 109 studies were excluded (Figure 1).
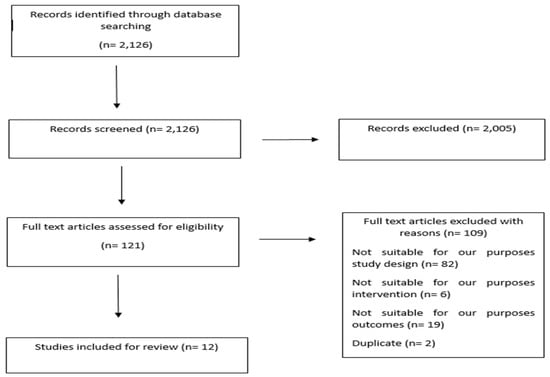
Figure 1.
Study selection flow diagram.
Table 1 summarizes the characteristics of all included studies. Ten of the included studies concern IL4/13 inhibitors (dupilumab), while two of the included studies concern JAK inhibitors. The total number of included participants was 378 concerning dupilumab and 38 patients concerning JAK inhibitors. In so far as dupilumab is concerned, all the studies included adult patients, except one study, which included both adults and adolescents. One of the two studies concerning JAK inhibitors was conducted in a pediatric population (11–12 years), while the second one did not specify the age group of the participants. Ten of the included studies were observational studies, and two were randomized controlled trials (RCTs). Five researchers did not include any comparison group, three included healthy volunteers as a comparator group, two studies were conducted versus placebo, and two studies compared dupilumab with other treatments (cyclosporine, topical corticosteroids, topical calcineurin inhibitors, and ultraviolet phototherapy). The follow-up period ranged between 29 days and 32 weeks. Table 2 summarizes the changes in skin barrier function.

Table 1.
Characteristics of included studies (TCs: topical corticosteroids; TCI: topical calcineurin inhibitor).
Table 2.
Changes in skin barrier function.
3.2. Quality of Included Studies
The ROBINS-I tool was used to evaluate the risk of bias of the included observational studies (Table 3) and the RoB 2.0 tool was used to assess the risk of bias of the included RCTs (Table 4). Nine out of ten included observational studies were assessed as having a moderate overall risk of bias and one as having a serious overall risk of bias. Berdyshev et al. [13] was assessed as having a moderate to serious overall risk of bias in several domains, particularly due to a lack of randomization and potential confounding factors. Rohner et al. [14] was also assessed as having a moderate to serious overall risk of bias. The primary concerns resulted from confounding, selection of participants, missing data, and potential selective reporting. Concerning Lee et al. [16], the small sample size, the potential handling of missing data, and the lack of detailed confounder control contributed to a moderate risk of bias. Ferruci et al. [2] was assessed as having a moderate overall risk of bias. Key areas of concern included confounding factors (environmental influences on TEWL) and selection bias (restricting the study to patients with severe atopic dermatitis). Montero-Vilchez et al. (2022) [17], considering all the domains, demonstrated a generally low to moderate risk of bias, primarily due to potential issues in the blinding of outcome assessment and possible missing data not explicitly addressed. The study’s design and reporting adhered to many of the criteria needed to ensure reliable findings. Thereinafter, Cristaudo et al. [18] was rated as having a moderate to serious risk of bias, particularly due to potential confounding factors and lack of detailed adherence and blinding information. Furuhashi et al. [19] was assessed as having a moderate overall risk of bias. Key concerns included potential confounding factors, selection bias (non-random participant selection), and measurement bias. Despite these concerns, the study had clear reporting and standardized measurement tools that helped mitigate some biases. Dini et al.’s [20] study design had clear intervention groups and objective outcome measures. However, the lack of detailed information on confounder control, adherence monitoring, missing data handling, and blinding introduced some risk of bias, and for these reasons, the study was judged as having a moderate overall risk of bias. Subsequently, the overall risk of bias for Montero-Vilchez et al. (2023) [21], using the ROBINS-I tool, was judged to be moderate. The main concerns arose from deviations from intended interventions and the selection of reported results. Lastly, the overall risk of bias for Horimukai et al. [23] was assessed as serious. The primary concerns included the small sample size, the retrospective design, potential confounding factors, and selection bias. Both RCTs included in the review were evaluated as having a low overall risk of bias.
Table 3.
Risk of bias assessment of included observational studies using the ROBINS-I tool.
Table 4.
Risk of bias assessment of included RCTs using the RoB 2.0 tool.
3.3. Results of Individual Studies
The results of individual studies are described in detail in the Supplementary Materials section.
4. Discussion
This review mainly summarizes the beneficial effects of IL-4/IL-13 inhibitors, and comparatively less of JAK inhibitors, on skin barrier function in atopic dermatitis. As patients with atopic dermatitis have high TEWL values, reflecting skin barrier dysfunction, the majority of studies used TEWL as a measurement tool to evaluate skin barrier both on eczematous lesions and non-lesional skin. Some studies also evaluated SCH, which is also decreased in patients with atopic dermatitis, ET, expression of FLG, ceramide composition, PH, and temperature. As shown, dupilumab decreased TEWL on lesional and non-lesional skin and improved skin barrier function parameters such as SCH, ET, ceramide composition, FLG expression, PH, and temperature. Only two studies regarding JAK inhibitors and restoration of skin barrier emerged from our search; however, given the small sample size, and despite the positive results regarding TEWL and ET, further research is needed.
Improvement of skin barrier dysfunction by inhibiting IL4/IL-13 confirms the interwoven impact in AD pathogenesis of the immunological component and the expression of barrier proteins as well as ceramides and tight junction quality. The impact of this holistic effect on clinical practice is multifactorial. Guidelines suggest a stepwise therapeutic algorithm with emollients as baseline therapy, regardless of the severity of AD, topical steroids and calcineurin inhibitor treatment added to the emollients in mild AD, UV treatment added to topicals and emollients in moderate AD, and systemic therapy added in severe AD. Furthermore, systemic therapy is also encouraged in patients not responding adequately to topicals or with impaired social or functional quality of life. Systemic therapy with biologics or JAKs is also approved by both the FDA and EMA for moderate AD based on the results of the respective pivotal studies [24].
The improvement of the novel agents on skin barrier properties does not make the use of emollients obsolete or encourage early intervention with biologicals or JAKs. Emollients, especially emollient-plus, have a well-documented effect on improving skin barrier qualities and decreasing inflammation. A much-discussed debate regards whether initiation of emollient-plus at a presymptomatic stage in infants at risk of AD could modify the disease. Current literature suggests that emollients have a synergistic effect with topical and systemic agents, and this is reflected in the recommendation of all guidelines. In the same perspective, the use of systemics should be encouraged only for those patients in need of systemic therapy [25].
Data in the literature are more robust for dupilumab’s effect on improving skin barrier dysfunction compared to JAKs. A possible explanation is that dupilumab has been available as a treatment option for several years, making research on this issue more conclusive. Even though the data for JAKs are limited, they are encouraging based on the rationale that the IL4/13 inflammatory pathway is also inhibited by JAKs, along with several others such as TSLP and IL-22. Future publications on JAKs and on novel biologics such as OX-40 and OX-40 ligand blockers’ effects on improving skin barrier properties are expected. The multitude of approved and future treatments and their improvement of all components of AD pathogenesis signifies a new and optimistic future for AD patients.
Limitations
A literature search was carried out by a single researcher and was limited to Medline via PubMed. The overall sample size was relatively small, which limits the general applicability of the findings. The retrospective nature of the majority of the included studies may introduce biases. The scarcity of robust data on JAK inhibitors may be partly due to their relatively more recent use in the treatment of atopic dermatitis. As a result, there is a significant gap in the literature regarding their comparative effectiveness against other established therapies such as IL-4/IL-13 inhibitors, topical corticosteroids, and calcineurin inhibitors in correcting epidermal barrier dysfunction. Additionally, many studies are open-label or involve comparison with placebo rather than existing standard treatments, which further complicates the interpretation of their relative efficacy. The absence of sufficient RCTs in the context of JAK inhibitors and other emerging treatments for AD hinders the ability to perform systematic reviews and meta-analyses that could offer more definitive guidance on treatment protocols. Equally important is the fact that TEWL was not measured using the same method across the different studies, nor at the same anatomical location, raising risks of additional biases.
5. Conclusions
In conclusion, this study underscores the efficacy of IL-4/IL-13 inhibitors and JAK inhibitors in improving skin barrier function in atopic dermatitis patients. The significant reductions in TEWL and increases in SCH on eczematous lesions among sustained responders highlight the potential of these treatments in managing atopic dermatitis. Early identification of treatment response predictors can enhance clinical decision-making, leading to more personalized and effective therapeutic interventions. Further research is warranted to expand on these findings, particularly through large-scale, prospective studies. Such research will be critical in confirming the long-term efficacy and safety of these inhibitors and in developing optimized treatment protocols for atopic dermatitis patients. Additionally, the integration of non-invasive monitoring techniques in routine clinical practice represents a promising avenue for improving patient outcomes and advancing the management of atopic dermatitis.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/medicina60081376/s1, Results of individual studies.
Author Contributions
Conceptualization, I.C. and S.G.; methodology, I.C. and S.G.; software, I.C.; validation, I.C., S.G., E.V. and I.P.; formal analysis, I.C. and S.G.; investigation, I.C.; resources, I.C.; data curation, I.C. and S.G.; writing—original draft preparation, I.C.; writing—review and editing, I.C., S.G., E.V., I.P. and D.K.; visualization, I.C.; supervision, S.G. and E.V.; project administration, S.G. and E.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
We exclude this statement because the study did not require ethical approval.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data presented are original and not inappropriately selected, manipulated, enhanced, or fabricated.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Nutten, S. Atopic dermatitis: Global epidemiology and risk factors. Ann. Nutr. Metab. 2015, 66 (Suppl. 1), 8–16. [Google Scholar] [CrossRef]
- Ferrucci, S.; Romagnuolo, M.; Maronese, C.A.; Germiniasi, F.; Tavecchio, S.; Angileri, L.; Casazza, G.; Marzano, A.V.; Genovese, G. Skin barrier status during dupilumab treatment in patients with severe atopic dermatitis. Ther. Adv. Chronic Dis. 2021, 12, 20406223211058332. [Google Scholar] [CrossRef]
- Bakker, D.S.; de Graaf, M.; Nierkens, S.; Delemarre, E.M.; Knol, E.; van Wijk, F.; de Bruin-Weller, M.S.; Drylewicz, J.; Thijs, J.L. Unraveling heterogeneity in pediatric atopic dermatitis: Identification of serum biomarker-based patient clusters. J. Allergy Clin. Immunol. 2022, 149, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Grice, E.A.; Segre, J.A. The skin microbiome. Nat. Rev. Microbiol. 2011, 9, 244–253. [Google Scholar] [CrossRef]
- Grafanaki, K.; Antonatos, C.; Maniatis, A.; Petropoulou, A.; Vryzaki, E.; Vasilopoulos, Y.; Georgiou, S.; Gregoriou, S. Intrinsic Effects of Exposome in Atopic Dermatitis: Genomics, Epigenomics and Regulatory Layers. J. Clin. Med. 2023, 12, 4000. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, B.E.; Leung, D.Y.M. Pathophysiology of atopic dermatitis: Clinical implications. Allergy Asthma Proc. 2019, 40, 84–92. [Google Scholar] [CrossRef]
- Bieber, T. Atopic dermatitis. N. Engl. J. Med. 2008, 358, 1483–1494. [Google Scholar] [CrossRef] [PubMed]
- Katsarou, S.; Makris, M.; Vakirlis, E.; Gregoriou, S. The Role of Tight Junctions in Atopic Dermatitis: A Systematic Review. J. Clin. Med. 2023, 12, 1538. [Google Scholar] [CrossRef]
- Yang, G.; Seok, J.K.; Kang, H.C.; Cho, Y.Y.; Lee, H.S.; Lee, J.Y. Skin Barrier Abnormalities and Immune Dysfunction in Atopic Dermatitis. Int. J. Mol. Sci. 2020, 21, 2867. [Google Scholar] [CrossRef]
- Han, R.; Zhu, D.; Sha, J.; Zhao, B.; Jin, P.; Meng, C. Decoding the role of DNA methylation in allergic diseases: From pathogenesis to therapy. Cell Biosci. 2024, 14, 89. [Google Scholar] [CrossRef]
- Savva, M.; Papadopoulos, N.G.; Gregoriou, S.; Katsarou, S.; Papapostolou, N.; Makris, M.; Xepapadaki, P. Recent Advancements in the Atopic Dermatitis Mechanism. Front. Biosci. 2024, 29, 84. [Google Scholar] [CrossRef] [PubMed]
- Brunner, P.M.; Guttman-Yassky, E.; Leung, D.Y. The immunology of atopic dermatitis and its reversibility with broad-spectrum and targeted therapies. J. Allergy Clin. Immunol. 2017, 139, S65–S76. [Google Scholar] [CrossRef]
- Berdyshev, E.; Goleva, E.; Bissonnette, R.; Bronova, I.; Bronoff, A.S.; Richers, B.N.; Garcia, S.; Ramirez-Gama, M.; Taylor, P.; Praestgaard, A.; et al. Dupilumab significantly improves skin barrier function in patients with moderate-to-severe atopic dermatitis. Allergy 2022, 77, 3388–3397. [Google Scholar] [CrossRef] [PubMed]
- Rohner, M.H.; Thormann, K.; Cazzaniga, S.; Yousefi, S.; Simon, H.U.; Schlapbach, C.; Simon, D. Dupilumab reduces inflammation and restores the skin barrier in patients with atopic dermatitis. Allergy 2021, 76, 1268–1270. [Google Scholar] [CrossRef] [PubMed]
- Guttman-Yassky, E.; Blauvelt, A.; Eichenfield, L.F.; Paller, A.S.; Armstrong, A.W.; Drew, J.; Gopalan, R.; Simpson, E.L. Efficacy and Safety of Lebrikizumab, a High-Affinity Interleukin 13 Inhibitor, in Adults with Moderate to Severe Atopic Dermatitis: A Phase 2b Randomized Clinical Trial. JAMA Dermatol. 2020, 156, 411–420. [Google Scholar] [CrossRef]
- Lee, S.J.; Kim, S.E.; Shin, K.O.; Park, K.; Lee, S.E. Dupilumab Therapy Improves Stratum Corneum Hydration and Skin Dysbiosis in Patients with Atopic Dermatitis. Allergy Asthma Immunol. Res. 2021, 13, 762–775. [Google Scholar] [CrossRef]
- Montero-Vilchez, T.; Rodriguez-Pozo, J.A.; Diaz-Calvillo, P.; Salazar-Nievas, M.; Tercedor-Sanchez, J.; Molina-Leyva, A.; Arias-Santiago, S. Dupilumab Improves Skin Barrier Function in Adults with Atopic Dermatitis: A Prospective Observational Study. J. Clin. Med. 2022, 11, 3341. [Google Scholar] [CrossRef]
- Cristaudo, A.; Pigliacelli, F.; Sperati, F.; Orsini, D.; Cameli, N.; Morrone, A.; Mariano, M. Instrumental evaluation of skin barrier function and clinical outcomes during dupilumab treatment for atopic dermatitis: An observational study. Ski. Res. Technol. 2021, 27, 810–813. [Google Scholar] [CrossRef]
- Furuhashi, T.; Oda, T.; Torii, K.; Nishida, E.; Morita, A. Dupilumab probably reduces transepidermal water loss but does not increase stratum corneum hydration in atopic dermatitis. J. Dermatol. 2021, 48, e74–e75. [Google Scholar] [CrossRef]
- Dini, V.; Iannone, M.; Michelucci, A.; Manzo Margiotta, F.; Granieri, G.; Salvia, G.; Oranges, T.; Janowska, A.; Morganti, R.; Romanelli, M. Ultra-High Frequency UltraSound (UHFUS) Assessment of Barrier Function in Moderate-to-Severe Atopic Dermatitis during Dupilumab Treatment. Diagnostics 2023, 13, 2721. [Google Scholar] [CrossRef]
- Montero-Vilchez, T.; Rodriguez-Pozo, J.A.; Cuenca-Barrales, C.; Sanabria-de-la-Torre, R.; Torres-de-Pinedo, J.M.; Arias-Santiago, S. Stratum Corneum Hydration as a Potential Marker of Response to Dupilumab in Atopic Dermatitis: A Prospective Observational Study. Dermatitis 2023, 35, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Pavel, A.B.; Song, T.; Kim, H.J.; Del Duca, E.; Krueger, J.G.; Dubin, C.; Peng, X.; Xu, H.; Zhang, N.; Estrada, Y.D.; et al. Oral Janus kinase/SYK inhibition (ASN002) suppresses inflammation and improves epidermal barrier markers in patients with atopic dermatitis. J. Allergy Clin. Immunol. 2019, 144, 1011–1024. [Google Scholar] [CrossRef] [PubMed]
- Horimukai, K.; Kinoshita, M.; Takahata, N. Transepidermal Water Loss and T-helper 2 (Th2)-Associated Inflammatory Markers in Two Pediatric Patients During the First Four Weeks of Treatment with the Oral Janus Kinase Inhibitor Upadacitinib. Cureus 2023, 15, e51196. [Google Scholar] [CrossRef] [PubMed]
- Argenziano, G.; Cusano, F.; Corazza, M.; Amato, S.; Amerio, P.; Naldi, L.; Patruno, C.; Pigatto, P.D.; Quaglino, P.; Gisondi, P.; et al. Italian S3-Guideline on the treatment of Atopic Eczema—Part 2: Non-systemic treatments and treatment recommendations for special AE patient populations, adapted from EuroGuiDerm by the Italian Society of Dermatology and STD (SIDEMAST), the Italian Association of Hospital Dermatologists (ADOI) and the Italian Society of Allergological and Occupational Dermatology (SIDAPA). Ital. J. Dermatol. Venerol. 2024, 159, 251–278. [Google Scholar] [CrossRef] [PubMed]
- AAAAI/ACAAI JTF Atopic Dermatitis Guideline Panel; Chu, D.K.; Schneider, L.; Asiniwasis, R.N.; Boguniewicz, M.; De Benedetto, A.; Ellison, K.; Frazier, W.T.; Greenhawt, M.; Huynh, J.; et al. Atopic dermatitis (eczema) guidelines: 2023 American Academy of Allergy, Asthma and Immunology/American College of Allergy, Asthma and Immunology Joint Task Force on Practice Parameters GRADE- and Institute of Medicine-based recommendations. Ann. Allergy Asthma Immunol. 2024, 132, 274–312. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).