Abstract
Background and Objectives: To assess pregnancy and delivery complications in obese women with gestational diabetes mellitus (GDM) and neonatal weight and condition after birth. Materials and Methods: A retrospective tertiary referral centre study included all cases of GDM in the Department of Obstetrics and Gynaecology of the Lithuanian University of Health Sciences (LUHS) Birth Registry from 1 January 2019 to 31 December 2019. We included 583 women with GDM and singleton pregnancies. Women were divided into two groups according to their pre-pregnancy weight: 202 were obese (BMI ≥ 30 kg/m2), and 381 were weight (BMI 18.5–24.9 kg/m2). Survey data were analysed using IBM SPSS Statistics 26.0 and MS Excel 2016 software. A value of p < 0.05 was considered significant. Results: Fasting glycaemia was significantly higher in obese women with GDM than in normal-weight women with GDM (p < 0.001). In addition, fasting glycaemia was higher in obese women with GDM requiring insulin correction than in normal-weight women (p = 0.006). OGTT 0-min glycaemia was higher in obese than in non-obese women with gestational diabetes (p < 0.001). Women with pre-pregnancy obesity had a higher incidence of primary hypertension (p < 0.001), hypertensive disorders in pregnancy (p < 0.001), gestational cholestasis (p = 0.002), polyhydramnios (p < 0.001), induced labour (p < 0.001), and caesarean section (p = 0.015), with emergency caesarean sections being more frequent than planned caesarean sections (p = 0.011) compared to normal-weight women with GDM. Labour dystocia (p = 0.003) and foetal distress (p = 0,019) were more common during labour in obese women. Neonates of these women more often had macrosomia (p < 0.001) and lower Apgar scores at 1 min (p = 0.024) and at 5 min (p = 0.024) compared to neonates of normal-weight women. Conclusions: Obese women with GDM experience more pregnancy complications than normal-weight women with GDM.
1. Introduction
Gestational diabetes (GD) is a disorder of carbohydrate metabolism characterised by hyperglycaemia of variable severity that is first diagnosed during pregnancy [1,2]. The screening of GD during pregnancy is performed between 24 and 28 weeks of gestation if it is not detected by fasting glycaemia at the beginning of pregnancy [3,4,5]. GD is one of the most common metabolic disorders detected in pregnancy [6]. Many reports indicated that the increasing number of patients with GD worldwide may be related to the growing epidemic of obesity [2,7,8].
The standard definition of obesity in the pregnant population is not easy to adapt because pregnant women gain weight in a relatively short period of time, and most of this is associated with weight gain that is lost during childbirth (consisting of the foetus, amniotic fluid, and blood). In the absence of a standard pregnancy-specific definition of obesity, pregnant women are classified as obese or non-obese based on their pre-pregnancy body mass index (BMI) [9].
Obesity is an important risk factor for the development of GD [2]. Obese pregnant women are at increased risk of various complications during pregnancy and labour. The risk increases with increasing body mass index [10]. Pregnancy in obese women diagnosed with GD is associated with worse pregnancy and delivery outcomes than either GD or obesity alone [11]. In addition, pre-pregnancy overweight and obesity are associated with an increased risk of pregnancy-induced hypertension, pre-eclampsia, an increased risk of emergency caesarean section (CS), and preterm birth [12].
Increased insulin resistance in obese pregnant women affects fetal metabolism: fetal blood glucose, ketones, free fatty acids and amino acids increase [13,14]. As a result, obese women are 1.4 to 1.8 times more likely to give birth to large-for-gestational-age newborns than women of normal weight [14]. Children born to obese women are also at higher risk of becoming obese in childhood and adulthood, as well as developing type 2 diabetes mellitus (DM) and cardiovascular disease [15].
Data from the “Health Behavior in the Lithuanian Adult Population” study showed that the rate of obese women of reproductive age is 24.1% [16]. We do not have data on the prevalence of obese pregnant women in our country. Obesity during pregnancy is a risk factor for complications in pregnancy and childbirth. Obesity and gestational diabetes are likely to have an even greater impact on complications for the women and the foetus. The aim of this study was to compare obstetric outcomes between obese and non-obese women with GDM delivering at a tertiary referral centre.
2. Materials and Methods
A retrospective study at a tertiary referral centre was conducted to review the obstetric records of women with GD who gave birth at 22 to 41 weeks of gestation at the Department of Obstetrics and Gynaecology, Lithuanian University of Health Sciences (LUHS) Hospital, from 1 January 2019 to 31 December 2019. The data were approved by the Kaunas Regional Bioethics Committee, Kaunas, Lithuania, under registration number BE-2-41. Data collected included maternal pre-pregnancy height and weight (BMI—weight in kilograms divided by height in metres squared (kg/m2) [17]), socio-demographic information (age, place of residence), number of previous pregnancies and births, duration of the current pregnancy, fasting venous plasma glucose (in the first trimester), and oral glucose tolerance test (OGTT) parameters at three glycaemic time points (0 min—fasting glycaemia, 60 min and 120 min glycaemia after ingestion of 75 g of glucose solution). This study also analysed the course of pregnancy and labour complications, including hypertensive disorders in pregnancy (pregnancy-induced hypertension, pre-eclampsia), anaemia, cholestasis, changes in the amount of amniotic fluid (polyhydramnios, oligohydramnios), methods of induction of labour, cephalopelvic disproportion (type of dystocia), other dystocia (prolonged labour related to the birth process), abnormal fetal position (breech presentation, transverse position), preterm birth (22 + 0 weeks to 36 + 6 weeks), mode of delivery (vaginal delivery or caesarean section, with indications for caesarean section analysed), bleeding due to uterine atony (data collected and analysed but not reported due to a small number of cases), chorioamnionitis, duration of labour and stage of delivery (in minutes), neonatal weight (in grams), assessed by sex and gestational age, and neonatal Apgar scores at 1 and 5 min.
The height and weight of the pregnant women were obtained from their medical records, and the first antenatal visit was made within the first 14 weeks of pregnancy. Obesity was diagnosed if the BMI was ≥30 kg/m2. The data collected in the study were compared between normal-weight women (18.5–24.9 kg/m2) and obese women with GD. Gestational diabetes is classified according to White: primarily diet-controlled GDM (class A1GDM) or GDM requiring pharmacological treatment (insulin therapy) of hyperglycaemia (class A2GDM) [18].
Hypertensive disorders in pregnancy are defined when arterial blood pressure (ABP) rises above 140/90 mmHg without proteinuria (pregnancy-induced hypertension) or with proteinuria (pre-eclampsia). Chronic (primary) hypertension and chronic (primary) hypertension complicated by pregnancy are diagnosed when elevated ABP and/or proteinuria are observed up to 20 weeks of gestation. Polyhydramnios is diagnosed in the presence of excess amniotic fluid as determined by ultrasound when the amniotic fluid index is greater than 240 mm or the deepest amniotic pocket is greater than 80 mm.
Foetal macrosomia was observed if the birth weight was greater than 4000 g. Excessive foetal or neonatal weight for gestational age is defined as greater than the 90th percentile for sex and gestational age.
The survey data were analysed using IBM SPSS Statistics 26.0 and MS Excel 2016 software. Descriptive data statistics—absolute (n) and percentage frequencies (%)—were used to assess the distribution of the analysed characteristics in the selected sample. The mean (m) and standard deviation (SD) used to describe the interval scale variables are given as the median (Me), minimum (min), and maximum (max) values of the variable. Distributions of two independent samples and unsatisfactory assumptions of normality were compared using the Mann–Whitney U test, while distributions of more than two independent samples were analysed using the Kruskal–Wallis test. The means of the quantitative variables of the two independent samples, for which the normality assumption was satisfied, were compared using the Student’s t-test. Tables of related variables, the chi-square (χ2) criterion for determining the homogeneity of variables, and the number of degrees of freedom (NDF) were calculated to assess the relationships between variables. Pairwise comparisons were performed using the z-test with Bonferroni correction. A value of p < 0.05 was considered significant.
We considered the relationship between variables to be statistically significant if the p-value was less than 0.05 (p < 0.05) and the statistical power of the 1-β test was 0.95 (1-β = 0.95). If these conditions are met, the effect size w = 0.25, and the number of degrees of freedom Df = 1–4 are chosen, the total sample size is 208–298. The survey data were analysed using IBM SPSS Statistics 26.0 and MS Excel 2016 software, G*Power V.3.1.9.4 University of Düsseldorf, Germany.
3. Results
According to data from the maternity register of the Department of Obstetrics and Gynaecology at LUHS Kauno klinikos, 3010 women gave birth at the maternity unit in 2019. Of our sample, 784 had gestational diabetes and gave birth between 22 and 41 weeks of gestation. In total, 583 women were selected for this study: 381 (65.3%) were of normal weight and 202 (34.7%) were obese. The BMI of 108 obese pregnant women was between 30 and 34.9 kg/m2 (53.5%), the BMI of 63 women was between 35 and 39.9 kg/m2 (31.2%), and the BMI of 31 women was ≥40 kg/m2 (15.3%).
Obese mothers were statistically significantly older than normal weight pregnant women (p = 0.012). Type A2 GD was significantly more common in obese women than in women of normal weight. Type A1 GD was diagnosed more often in normal-weight women than in obese women. Obese women were more likely to live in rural areas than normal-weight women. The median gestational age was 39 weeks in both groups and was not statistically significantly different (Table 1).

Table 1.
Socio-demographic factor (N = 583).
Obese women with gestational diabetes had a statistically significant increase in the number of pregnancies and births compared to non-obese women (p < 0.001). Obese pregnant women with type A2 GD were statistically significantly more likely to become pregnant and give birth three or more times than normal-weight women. The latter, normal-weight women, were more likely to give birth for the first time (Table 2).
Table 2.
The number of pregnancies and deliveries (N = 583).
In the first trimester of pregnancy, GD was detected in 224 women. Venous plasma glucose concentration was statistically significantly higher in obese women compared with normal-weight women. By type of gestational diabetes, fasting venous plasma glucose was statistically significantly higher in obese women with type A2 diabetes than in women of normal weight.
In the second and third trimesters of pregnancy, 359 women were diagnosed with gestational diabetes after OGTT. Fasting venous glucose (I OGTT point) was statistically significantly higher in obese than in normal-weight women. A significant difference was also found when comparing fasting glycaemia according to GD types A1 and A2 in obese and normal-weight women. The results of the second OGTT point (glycaemia 60 min after glucose ingestion) did not differ significantly. OGTT point III glycaemia (120 min after glucose ingestion) was significantly higher in normal-weight women with type A1 diabetes than in obese women with type A1 GD. The data are shown in Table 3.
Table 3.
Comparison of mean venous plasma glucose level and mean venous plasma glucose level at exact OGTT points in normal-weight vs. obese pregnant women with GD (isolating type A1 and A2 according to White) diagnosed in the first third of pregnancy (N = 583).
Primary arterial hypertension was statistically significantly more common in obese pregnant women compared to normal-weight women (p < 0.001). Obese women with both GD A1 and GD A2 were statistically significantly more likely to develop primary arterial hypertension than normal-weight women. Hypertensive disorders in pregnancy (p < 0.001) and gestational cholestasis (p = 0.002) were diagnosed statistically significantly more often in obese pregnant women with GD than in those with normal body weight (type A1—p = 0.006, type A2—no significant difference; pre-eclampsia in obese women—6 (3.4%) and in normal-weight women—4 (3.2%)). The incidence of anaemia was not significantly different between the groups. The data are shown in Table 4.
Table 4.
Distribution of pregnant obese and normal-body-weight women with GD (isolating A1 and A2 types according to White) according to pregnancy complications (N = 299).
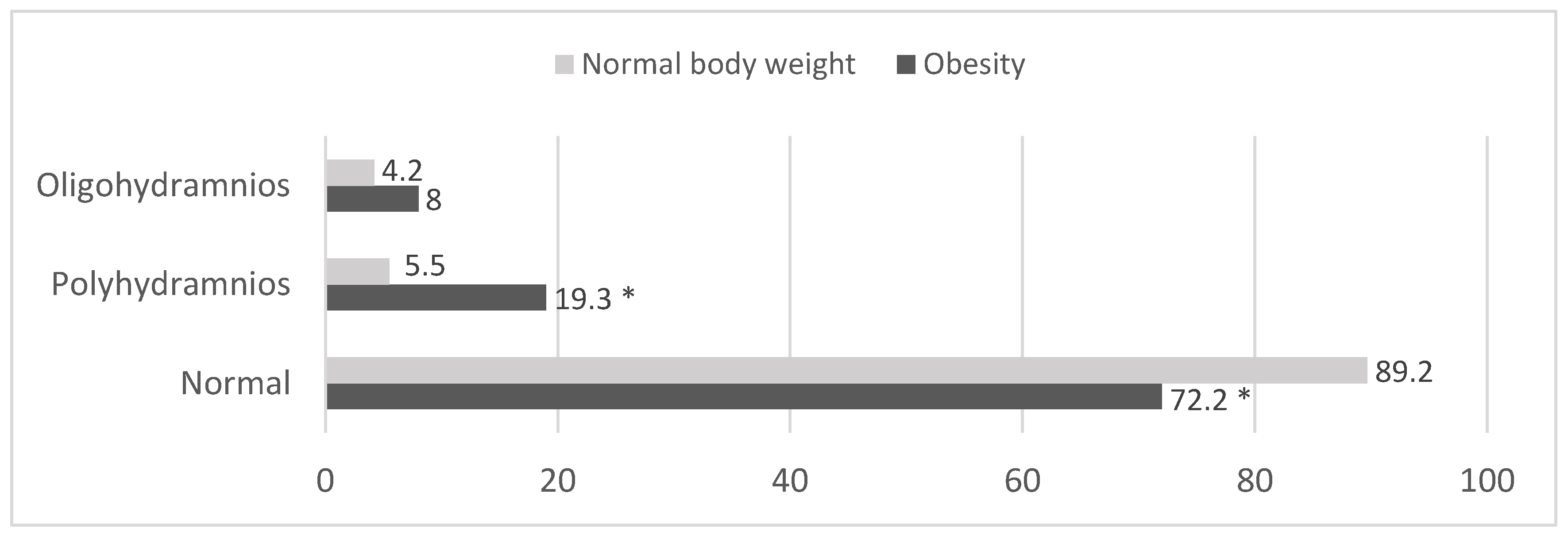
Normal amniotic fluid volume was statistically significantly more common in women of normal body weight than in women with GD (n = 340) and obese women (n = 146) (p < 0.001). Polyhydramnios was statistically significantly more frequent in the group of obese pregnant women (p < 0.001) (n = 39) compared to normal-weight women (n = 21) (Figure 1).
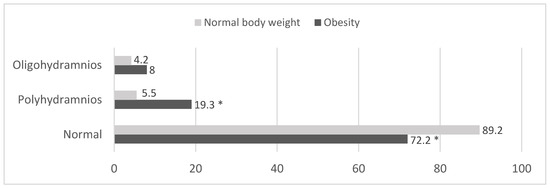
Figure 1.
Distribution of normal-body-weight and obese pregnant women by amount of amniotic fluid (%) (N = 583). * p < 0.001 compared to women with normal body weight (z test with Bonferroni correction).
Comparing obese and normal-weight pregnant women by type of GD, both poly- and oligohydramnios were statistically significantly more common in obese pregnant women with type A1 GD compared to normal-weight women with type A1 GD (p = 0.003). Normal-weight women with type A2 gestational diabetes were statistically significantly more likely to have normal amniotic fluid levels compared to obese pregnant women with type A2 GD. In addition, in this group, polyhydramnios was statistically significantly more common in obese women compared to women with normal BMI. The data are shown in Table 5.
Table 5.
Distribution of normal-body-weight and obese pregnant women with A1 and A2 types of gestational diabetes by amount of amniotic fluid (N = 583).
Labour was induced statistically significantly more often in obese women than in normal-weight women, regardless of the type of GD. Labour was induced in a total of 286 women. The most common method used was amniotomy, followed by medication (cervical ripening with misoprostol) and the least common by mechanical means (Foley catheter and other mechanical dilators). The analysis showed no statistically significant differences between the study groups regarding the choice of induction method. It is noteworthy that the number of cases of labour induction (177 in the normal weight group and 169 in the obese group) did not correspond to the number of births (151 in the normal weight group and 135 in the obese group) due to the use of multiple methods of labour induction for a single woman (Table 6).
Table 6.
Labour of normal-body-weight and obese women with GD (A1 and A2 types). (N = 519).
Obese women with GD had a statistically significantly higher rate of caesarean section (p = 0.015) than in normal-weight women. Emergency caesarean section was also more frequent in the obese group (p = 0. 011). The data are shown in Table 7.
Table 7.
Type of delivery of normal-body-weight and obese pregnant women.
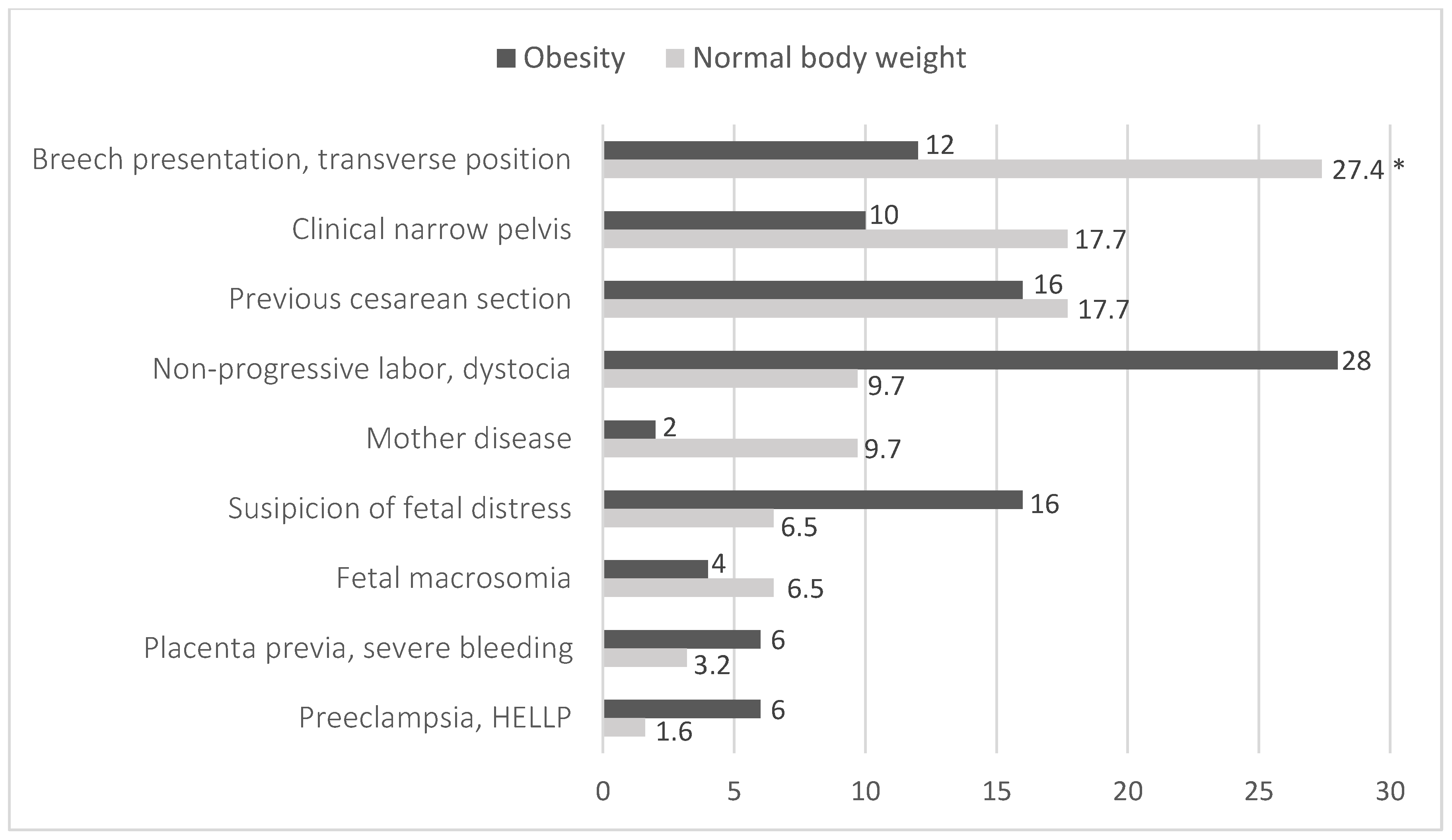
Caesarean section was performed statistically significantly more often in obese pregnant women with GD than in normal-weight women for suspected foetal distress—16% (n = 8), dystocia and non-progressive labour—28% (n = 14) compared to the frequency of these indications in normal-weight women—6.5% (n = 4) and 9.7% (n = 6), respectively (p = 0.032). Irregular position of the foetus in the uterus, i.e., breech presentation and transverse position, was statistically significantly more common as an indication for caesarean section in normal-weight pregnant women compared to the obese group (Figure 2).
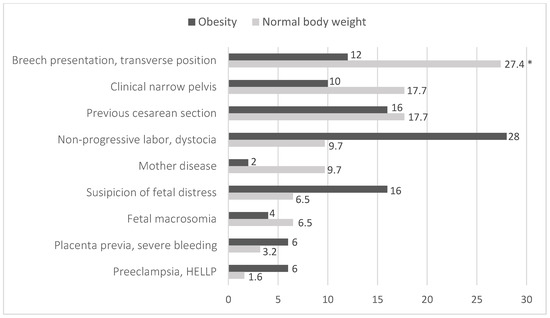
Figure 2.
Distribution of normal-body-weight and obese pregnant women according to the causes for a C-section (N = 112). p = 0.032; *—p < 0.05, compared to women with normal body weight (z test with Bonferroni correction).
The most common birth complications were chosen for the calculations. Only a few were statistically significant: foetal distress was more common in the obese group (p = 0.019) compared to the normal weight group. By type of GD, this complication was found to be statistically significantly more common in the A1 group of obese individuals. Dystocia was significantly more common in the obese group and in obese women with type A2 GD compared to normal weight mothers. Complications such as clinical pelvic obliquity, abnormal foetal position, chorioamnionitis and preterm delivery were similarly distributed in both groups with no statistically significant differences. The data are shown in Table 8.
Table 8.
Distribution of pregnant obese and normal-body-weight women with GD (isolating A1 and A2 types according to White) according to delivery complications (N = 583).
The calculation and comparison of the median and mean duration of labour showed that the second stage of labour was statistically significantly longer in normal-weight women compared to obese pregnant women (Table 9).
Table 9.
Comparison labour duration in normal-body-weight and obese pregnant women with A1 and A2 gestational diabetes (m ± SN).
No significant differences were found when comparing neonatal weights were compared without distinguishing between women by GD type, but neonates of normal-weight women with type A1 GD were statistically significantly heavier than those of obese women (p = 0.002). In contrast, in the A2 group, neonates of obese women were heavier than those of women of normal-weight women (p = 0.002). Apgar scores at 1 and 5 min were statistically significantly lower in neonates of obese women compared to neonates of normal-weight women. Foetal macrosomia was found to be statistically significantly more common in neonates in the obese women group than in neonates of normal-weight women. Obese pregnant women with both GD A1 and A2 were more likely to deliver macrosomic neonates than normal-weight women (Table 10).
Table 10.
Comparison of the data of neonates of normal-body-weight and obese pregnant women (N = 583).
4. Discussion
This study aimed to evaluate maternal, foetal, and neonatal outcomes during pregnancy and delivery in obese and normal-weight women with gestational diabetes. This study showed that adverse pregnancy outcomes—foetal macrosomia, emergency caesarean delivery, and low post-delivery Apgar scores—were more common in obese pregnant women with GD than in normal-weight women with GD.
Obesity and gestational diabetes are conditions that significantly affect both the woman and the foetus before, during, and after pregnancy. It is, therefore, important to assess the pregnancy and birth complications associated with these metabolic disorders and to identify and treat them in time to minimise the consequences for the woman and the foetus.
In our study, a quarter of pregnant women with gestational diabetes were obese, just over a fifth were overweight, and almost half had a normal BMI. Similar data were obtained in a study by C. Machado et al., which included 3013 women diagnosed with GD, of whom 56.9% were overweight or obese [19]. In our study, gestational diabetes type A2 was diagnosed more often in obese women than in pregnant women with normal body weight, whereas GD type A1 was diagnosed more often in women who had a normal BMI before pregnancy. Based on these results, we can say that the carbohydrate metabolism of obese women is more altered, leading to a higher incidence of gestational diabetes requiring more intensive treatment, including diet, lifestyle changes, and insulin treatment.
In our study, fasting plasma venous glucose in women diagnosed with GD in the first trimester of pregnancy was found to be statistically significantly higher in obese women than in women with normal pre-pregnancy weight. In addition, the first sample point (0 min, fasting) of the 2-hour 75 g OGTT was statistically significantly higher in obese pregnant women than in those with normal BMI diagnosed with GD in the second and third trimesters. Similar data were reported in the 2012 study by Baliutavičienė et al., who found that fasting glucose was higher in obese women (5.2 ± 1.1 mmol/L) than in normal-weight women (4.5 ± 0.8 mmol/L) [20]. It is important to note that in a recent study, gestational diabetes was diagnosed according to the guidelines for two glycaemic points. According to this OGTT methodology, GD was diagnosed but untreated if the fasting glycaemia was greater than 5.1 mmol/L. The same result is shown in a study by Sugiyama and co-authors, who found that the fasting point of the 2-hour 75 g OGTT was statistically significantly lower in the control group (normal-weight women) and higher in obese pregnant women. The second and third OGTT results were not statistically significantly different in our study; however, in the study by Sugiyama et al. study, both of these results were higher in the obese group compared to normal weight pregnant women [21]. Thus, these data again suggest that carbohydrate metabolism is altered obese women. Physiological changes in a woman’s body during pregnancy can affect metabolism, especially carbohydrate metabolism, leading to excessive glycaemia and an increased risk of complications during pregnancy and labour associated with hyperglycaemia.
In the studies by Sugiyama et al. and Baliutavičienė et al., as in our study, primary arterial hypertension was more common in obese pregnant women [20,21]. Hypertensive disorders in pregnancy, regardless of the type of GD, were statistically significantly more frequent in the obese group than in the normal weight group. The same data—hypertensive disorders in pregnancy statistically significantly more common in pregnant women—are published in many other studies describing the complications of pregnancy and labour in obese pregnant women with GD [20,21,22,23].
Polyhydramnios was more frequent in the group of obese pregnant women than in the group of normal-weight women. Similar data were found in the study by Baliutavičienė et al. [20].
Obese women were statistically significantly more likely to have induced labour than women with a normal BMI, and their second stage of labour was shorter than that of women of normal weight. This may be due to higher birth rates and epidural analgesia, but we did not analyse these associations. Similar data were reported in other studies showing that obese women were more likely to have induced labour than a group of normal-weight women [21,24]. Our study found that obese pregnant women were more likely to deliver by CS than normal-weight mothers. The same data are described in the studies by Lithuanian and foreign authors [11,19,20,22,23]. In many studies, obesity and gestational diabetes are independent risk factors for CS, but both may increase the risk of foetal macrosomia and influence the higher number of CS [19]. According to our study, dystocia as a complication of labour was more frequent in obese pregnant women. The largest sample (n = 1,057,647) in the study by Whiteman et al. describes that there was no statistically significant difference in the incidence of dystocia between obese and normal weight pregnant women [11]. The difference in results may be due to the different types of dystocia included in the study data.
One of the most commonly described complications of obesity, especially gestational diabetes, is overweight foetuses. In our study, neonatal birth weight was not statistically significantly different between groups, but macrosomia was several times more common in the obese group than in the normal weight group. Authors in many other countries have also found that macrosomia is more common in obese mothers with GD than in normal-weight women with gestational diabetes [6,17,22,25,26,27].
There are several limitations to this study. The most important is the relatively small sample size of this research. Because of this limitation, amniotic fluid volume (polyhydramnios and oligohydramnios) in women with foetal macrosomy and foetal hypotophy is not compared.
Due to the small sample size, we were not able to analyse the data by obesity class. The next planned direction of research is to assess the complications of pregnancy and childbirth by obesity class.
5. Conclusions
Pregnancy complications were significantly more common in obese pregnant women with gestational diabetes. Obese pregnant women with gestational diabetes had higher glucose levels and were more likely to be diagnosed with primary and hypertensive disorders in pregnancy, cholestasis, polyhydramnios, and foetal macrosomia. They were also more likely to have an emergency caesarean section at birth, to be diagnosed with labour dystocia, and to have lower Apgar scores than normal-weight women with gestational diabetes.
Author Contributions
Conceptualization, E.S.; methodology, G.R., E.S. and L.M. (Laima Maleckiene); software, E.S.; validation, G.R.; investigation, G.R.; resources, G.R.; writing—original draft preparation, G.G.; writing—review and editing, L.M. (Laura Malakauskiene); visualization, L.M. (Laura Malakauskiene) and G.G.; supervision, G.R., L.M. (Laura Malakauskiene), E.S. and L.M. (Laima Maleckiene); project administration, G.R. and G.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Kaunas Regional Biomedical Research Ethics Committee, on 26 July 2023 (protocol number BE-2-41).
Informed Consent Statement
Patient consent was not required as this was a retrospective study, and the data were obtained from patients’ medical histories, which allowed the data to be used for medical research prior to their treatment.
Data Availability Statement
Anonymised data used for the study will be stored on a separate biomedical study data storage computer that was used to conduct the biomedical study. The data will be kept for 15 years after the study and then destroyed.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. Diagnostic Criteria and Classification of Hyperglycemia First Detected in Pregnancy. 2013. Available online: https://apps.who.int/iris/handle/10665/85975 (accessed on 16 November 2020).
- Law, K.P.; Zhang, H. The pathogenesis and pathophysiology of gestational diabetes mellitus: Deductions from a three-part longitudinal metabolomics study in China. Clin. Chim. Acta 2017, 468, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health of the Republic of Lithuania. Guidelines and Protocols of Diagnostics and Treatment in Obstetrics “Nesciuju Diabetas”. 2019. Available online: https://sam.lrv.lt/uploads/sam/documents/files/Akušerinė%20metodika_Nėščiųjų%20diabetas_SAM_2019-07-20.pdf (accessed on 16 December 2020).
- Quintanilla Rodriguez, B.S.; Vadakekut, E.S.; Mahdy, H. Gestational Diabetes. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar] [PubMed]
- Zhang, M.; Zhou, Y.; Zhong, J.; Wang, K.; Ding, Y.; Li, L. Current guidelines on the management of gestational diabetes mellitus: A content analysis and appraisal. BMC Pregnancy Childbirth 2019, 19, 200. [Google Scholar] [CrossRef] [PubMed]
- Macrì, F.; Pitocco, D.; di Pasquo, E.; Salvi, S.; Rizzi, A.; Di Leo, M.; Tartaglione, L.; Di Stasio, E.; Lanzone, A.; De Carolis, S. Gestational weight gain as an independent risk factor for adverse pregnancy outcomes in women with gestational diabetes. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 4403–4410. [Google Scholar] [CrossRef] [PubMed]
- Aaron, B.C.; Erika, F.W.; Vanessa, A.B.; FACOG. Gestational Diabetes Mellitus: Obstetric Issues and Management. UpToDate 2019 October. Available online: https://www-uptodate-com.ezproxy.dbazes.lsmuni.lt/contents/gestational-diabetes-mellitus-obstetric-issues-and-management?search=gestationaldiabetes&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 (accessed on 25 November 2020).
- Plows, J.F.; Stanley, J.L.; Baker, P.N.; Reynolds, C.M.; Vickers, M.H. The Pathophysiology of Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2018, 19, 3342. [Google Scholar] [CrossRef] [PubMed]
- Catalano, P.M. Management of Obesity in Pregnancy. Obstet. Gynecol. 2007, 109 Pt 1, 419–433. [Google Scholar] [CrossRef]
- Lisonkova, S.; Muraca, G.M.; Potts, J.; Liauw, J.; Chan, W.S.; Skoll, A.; Lim, K.I. Association Between Prepregnancy Body Mass Index and Severe Maternal Morbidity. JAMA 2017, 318, 1777–1786. [Google Scholar] [CrossRef]
- Whiteman, V.E.; Salemi, J.L.; Mejia De Grubb, M.C.; Ashley Cain, M.; Mogos, M.F.; Zoorob, R.J.; Salihu, H.M. Additive effects of pre-pregnancy body mass index and gestational diabetes on health outcomes and costs. Obesity 2015, 23, 2299–2308. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Chen, H.; Hsu, H. Maternal Prepregnancy Body Mass Index, Gestational Weight Gain, and Risk of Adverse Perinatal Outcomes in Taiwan: A Population-Based Birth Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 1221. [Google Scholar] [CrossRef] [PubMed]
- Metzger, B.E.; Buchanan, T.A.; Coustan, D.R.; De Leiva, A.; Dunger, D.B.; Hadden, D.R.; Hod, M.; Kitzmiller, J.L.; Kjos, S.L.; Oats, J.N.; et al. Summary and recommendations of the Fifth International Workshop-Conference on Gestational Diabetes Mellitus. Diabetes Care 2007, 30 (Suppl. S2), S251–S260. [Google Scholar] [CrossRef]
- King, J.C. Maternal Obesity, Metabolism, and Pregnancy Outcomes. Annu. Rev. Nutr. 2006, 26, 271–291. [Google Scholar] [CrossRef]
- Gaillard, R. Maternal obesity during pregnancy and cardiovascular development and disease in the offspring. Eur. J. Epidemiol. 2015, 30, 1141–1152. [Google Scholar] [CrossRef] [PubMed]
- Underweight and Obesity in Lithuania. 2022. Available online: https://ncdrisc.org/downloads/country-pdf/double-burden/NCD-RisC%20country%20factsheet%20Lithuania.pdf (accessed on 12 November 2024).
- Centers for Disease Control and Prevention (CDC). Defining Adult Overweight and Obesity. 2017. Available online: https://www.cdc.gov/nccdphp/dnpao/data-trends-maps/help/npao_dtm/definitions.html (accessed on 25 November 2020).
- ACOG. Practice Bulletin No. 190: Gestational Diabetes Mellitus. Obstet. Gynecol. 2018, 131, e49–e64. [Google Scholar] [CrossRef] [PubMed]
- Machado, C.; Monteiro, S.; Oliveira, M.J. Impact of overweight and obesity on pregnancy outcomes in women with gestational diabetes—Results from a retrospective multicenter study. Arch. Endocrinol. Metab. 2019, 64, 45–51. [Google Scholar] [CrossRef]
- Baliutavičienė, D.; Buinauskienė, J.B.; Petrenko, V.; Danytė, E.; Žalinkevičius, R. Gestational Diabetes, Obesity, and Metabolic Syndrome Diagnosed During Pregnancy. Metab. Syndr. Relat. Disord. 2012, 10, 214–217. [Google Scholar] [CrossRef]
- Sugiyama, T.; Nagao, K.; Metoki, H.; Nishigori, H.; Saito, M.; Tokunaga, H.; Nagase, S.; Sugawara, J.; Watanabe, Y.; Yaegashi, N.; et al. Pregnancy outcomes of gestational diabetes mellitus according to pre-gestational BMI in a retrospective multi-institutional study in Japan. Endocr. J. 2014, 61, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Wahabi, H.A.; Fayed, A.A.; Alzeidan, R.A.; Mandil, A.A. The independent effects of maternal obesity and gestational diabetes on the pregnancy outcomes. BMC Endocr. Disord. 2014, 14, 47. [Google Scholar] [CrossRef] [PubMed]
- Miao, M.; Dai, M.; Zhang, Y.; Sun, F.; Guo, X.; Sun, G. Influence of maternal overweight, obesity and gestational weight gain on the perinatal outcomes in women with gestational diabetes mellitus. Sci. Rep. 2017, 7, 305–308. [Google Scholar] [CrossRef] [PubMed]
- Huet, J.; Beucher, G.; Rod, A.; Morello, R.; Dreyfus, M. Joint impact of gestational diabetes and obesity on perinatal outcomes. J. Gynecol. Obstet. Hum. Reprod. 2018, 47, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Li, F.; Zhang, Y.; Xu, X. Associations of the pre-pregnancy BMI and gestational BMI gain with pregnancy outcomes in Chinese women with gestational diabetes mellitus. Int. J. Clin. Exp. Med. 2014, 7, 5784–5789. [Google Scholar]
- Sabolović Rudman, S.; Djaković, I.; Gall, V.; Djaković, Ž.; Košec, V. Pregnancy outcome in gestational diabetes compared to body mass index. Acta Clin. Croat. 2019, 58, 37–41. [Google Scholar] [CrossRef]
- Dennedy, M.C.; Dunne, F. The maternal and fetal impacts of obesity and gestational diabetes on pregnancy outcome. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 573–589. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).