
Heat or Cold: Which One Exerts Greater Deleterious Effects on Health in a Basin Climate City? Impact of Ambient Temperature on Mortality in Chengdu, China

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Analysis of Temperature-Mortality Relationship
2.2.1. DLNM
2.2.2. Attributable Risk from DLNMs
2.2.3. Separating Attributable Components
2.2.4. Computing Uncertainty Intervals
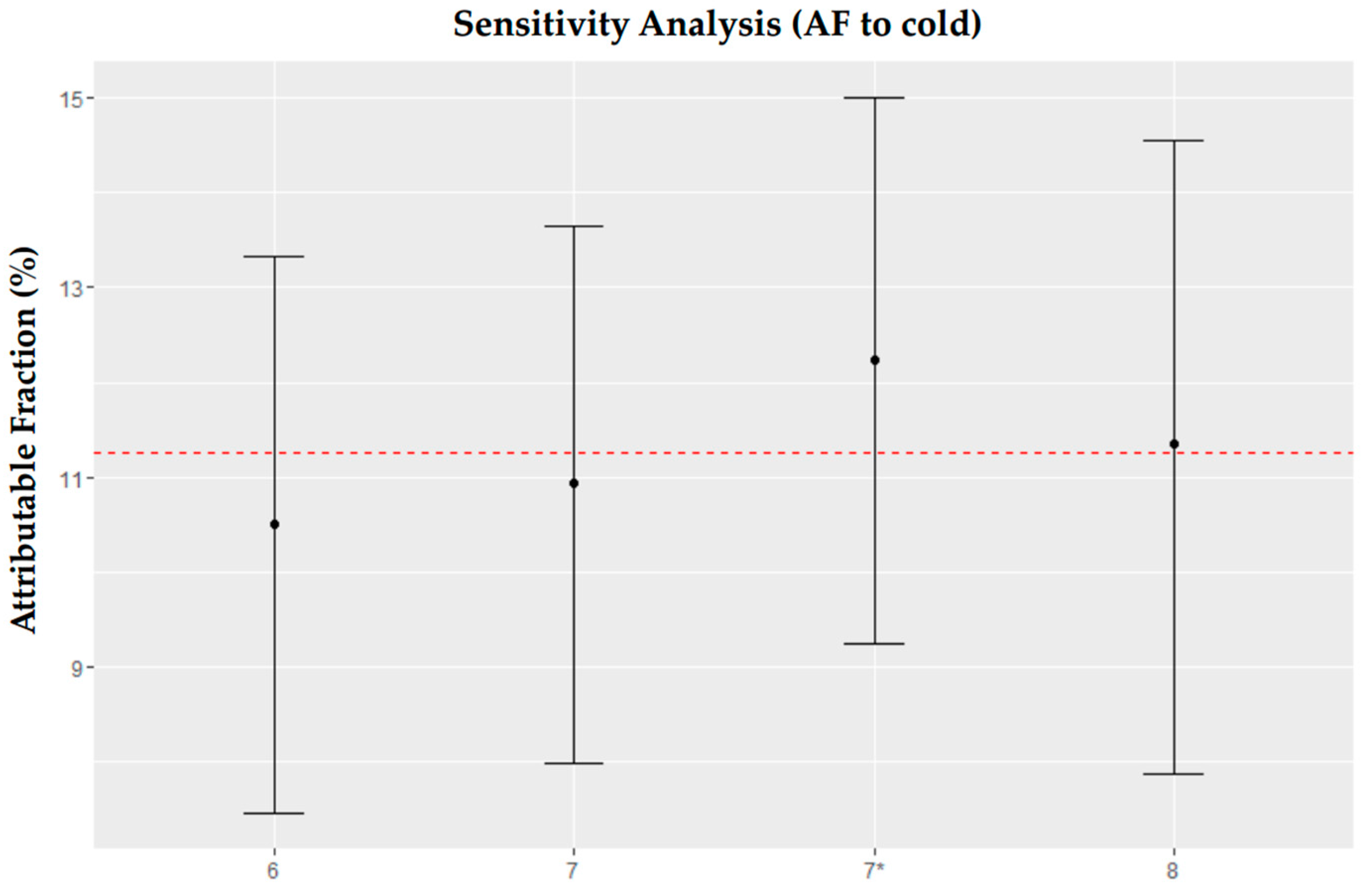
2.3. Sensitivity Analysis
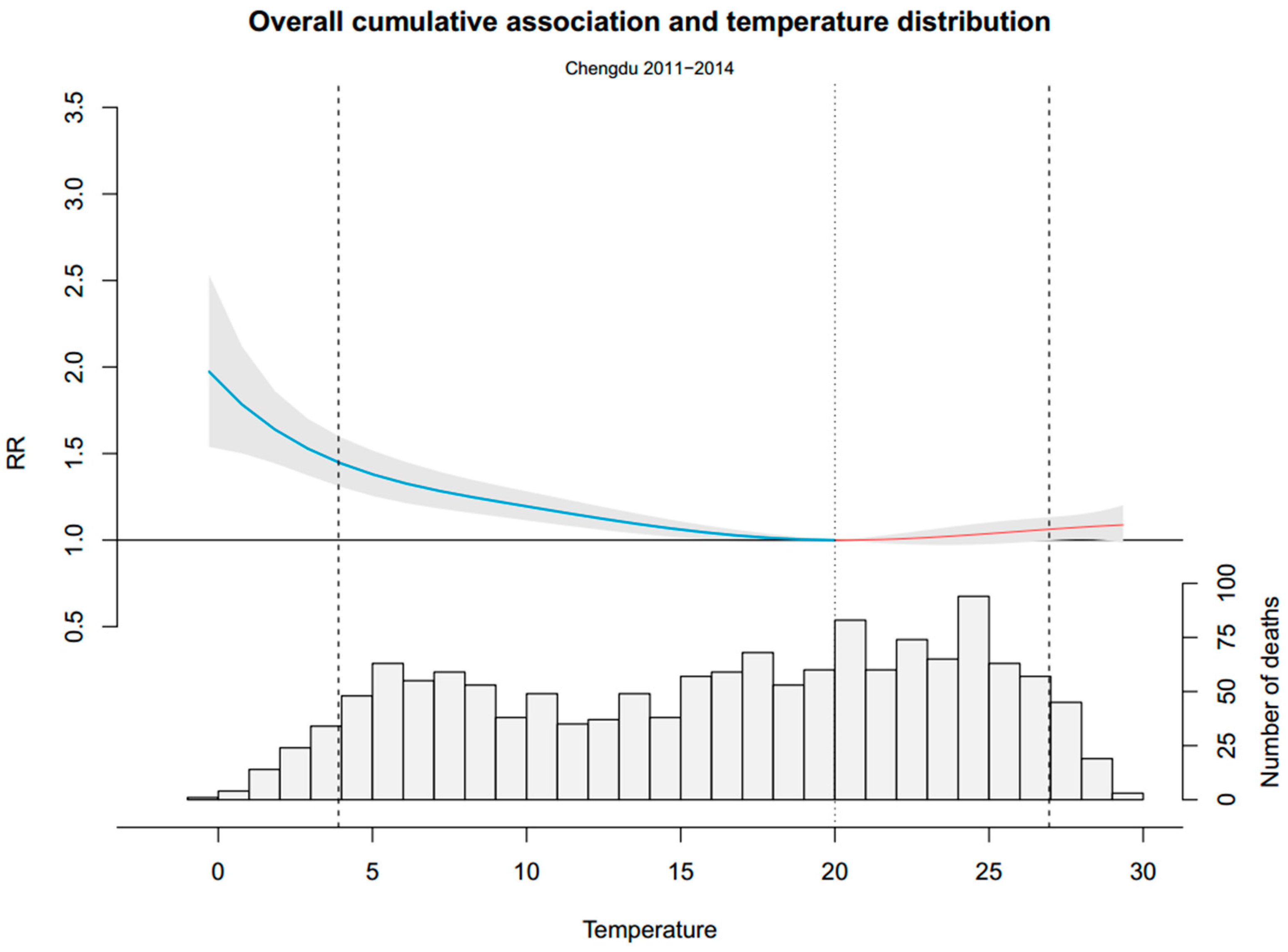
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Air Pollutant | Mean ± SD | Min | P25 | P50 | P75 | Max |
|---|---|---|---|---|---|---|
| PM10 | 122.7 ± 76.3 | 16.0 | 72.0 | 104.0 | 150.0 | 862.0 |
| SO2 | 28.4 ± 14.6 | 5.0 | 18.0 | 25.0 | 35.0 | 96.0 |
| NO2 | 55.7 ± 19.2 | 15.0 | 42.0 | 52.0 | 66.0 | 144.0 |

References
- Barnett, A.G.; Hajat, S.; Gasparrini, A.; Rocklov, J. Cold and heat waves in the United States. Environ. Res. 2012, 112, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Perkins, S.E.; Alexander, L.V.; Nairn, J.R. Increasing frequency, intensity and duration of observed global heatwaves and warm spells. Geophys. Res. Lett. 2012. [Google Scholar] [CrossRef]
- Wang, Y.; Shi, L.; Zanobetti, A.; Schwartz, J.D. Estimating and projecting the effect of cold waves on mortality in 209 US cities. Environ. Int. 2016, 94, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Baccini, M.; Biggeri, A.; Accetta, G.; Kosatsky, T.; Katsouyanni, K.; Analitis, A.; Anderson, H.R.; Bisanti, L.; D′Ippoliti, D.; Danova, J.; et al. Heat effects on mortality in 15 European cities. Epidemiology 2008, 19, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Keatinge, W.R.; Donaldson, G.C.; Cordioli, E.A.; Martinelli, M.; Kunst, A.E.; Mackenbach, J.P.; Nayha, S.; Vuori, I. Heat related mortality in warm and cold regions of Europe: Observational study. Br. Med. J. 2000, 321, 670–673. [Google Scholar] [CrossRef]
- Curriero, F.C.; Heiner, K.S.; Samet, J.M.; Zeger, S.L.; Strug, L.; Patz, J.A. Temperature and mortality in 11 cities of the eastern United States. Am. J. Epidemiol. 2002, 155, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Sun, Y.; Liu, Q.; Zhou, M.; Lu, Y.; Li, L. Impact of extreme high temperature on mortality and regional level definition of heat wave: A multi-city study in China. Sci. Total Environ. 2015, 505, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Van Bavel, J.J.; Mende-Siedlecki, P.; Brady, W.J.; Reinero, D.A. Contextual sensitivity in scientific reproducibility. Proc. Natl. Acad. Sci. USA 2016, 113, 6454–6459. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.; Yao, Z.; Zhang, Y.; Xu, Y.; Xu, X.; Liu, T.; Lin, H.; Lao, X.; Rutherford, S.; Chu, C.; et al. Short-Term Effects of the 2008 Cold spell on mortality in three subtropical cities in Guangdong Province, China. Environ. Health Perspect. 2013, 121, 210–216. [Google Scholar] [PubMed]
- Gasparrini, A.; Armstrong, B. The Impact of Heat Waves on Mortality. Epidemiology 2011, 22, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Kysely, J.; Pokorna, L.; Kyncl, J.; Kriz, B. Excess cardiovascular mortality associated with cold spells in the Czech Republic. BMC Public Health 2009. [Google Scholar] [CrossRef] [PubMed]
- Mercer, J.B. Cold—An underrated risk factor for health. Environ. Res. 2003, 92, 8–13. [Google Scholar] [CrossRef]
- Ryti, N.R.I.; Guo, Y.; Jaakkola, J.J. Global Association of Cold Spells and Adverse Health Effects: A Systematic Review and Meta-Analysis. Environ. Health Perspect. 2016, 124, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Acebo, I.; Llorca, J.; Dierssen, T. Cold-related mortality due to cardiovascular diseases, respiratory diseases and cancer: A case-crossover study. Public Health 2013, 127, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Robine, J. Seasonality in human mortality: A demographic approach. Eur. J. Popul. 2006, 24, 125–127. [Google Scholar] [CrossRef]
- Vasconcelos, J.; Freire, E.; Almendra, R.; Silva, G.L.; Santana, P. The impact of winter cold weather on acute myocardial infarctions in Portugal. Environ. Pollut. 2013, 183, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.G.; Wang, L.J.; Liu, T.; Zhang, Y.H.; Lin, H.L.; Luo, Y.; Xiao, J.P.; Zeng, W.L.; Zhang, Y.W.; Wang, X.F.; et al. Health impact of the 2008 cold spell on mortality in subtropical China: The climate and health impact national assessment study (Chinas). Environ. Health 2014. [Google Scholar] [CrossRef] [PubMed]
- Muggeo, V.M.; Hajat, S. Modelling the non-linear multiple-lag effects of ambient temperature on mortality in Santiago and Palermo: A constrained segmented distributed lag approach. Occup. Environ. Med. 2009, 66, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Morabito, M.; Crisci, A.; Moriondo, M.; Profili, F.; Francesconi, P.; Trombi, G.; Bindi, M.; Gensini, G.F.; Orlandini, S. Air temperature-related human health outcomes: Current impact and estimations of future risks in Central Italy. Sci. Total Environ. 2012, 441, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Iniguez, C.; Ballester, F.; Ferrandiz, J.; Perez-Hoyos, S.; Saez, M.; Lopez, A. Relation between Temperature and Mortality in Thirteen Spanish Cities. Int. J. Environ. Res. Public Health 2010, 7, 3196–3210. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhou, H. Characteristics of the wind and temperature field in PBL in Sichuan Basin. J. Sichuan Meteorol. 1999, 3, 39–45. [Google Scholar]
- Li, J.; Zhang, J.; Deng, M. Analysis of aviation climatology features on clouds in Sichuan Basin. J. Sichuan Meteorol. 2003, 1, 45–47. [Google Scholar]
- Hu, Y.; Zhu, K.; Li, Y. Climatic features and changes in the middle and western Chengdu Plain during past 40 years. J. Chengdu Univ. Inf. Technol. 2004, 2, 223–231. [Google Scholar]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Lavigne, E.; Zanobetti, A.; Schwartz, J.; Tobias, A.; Tong, S.; Rocklov, J.; Forsberg, B.; et al. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef]
- Gasparrini, A.; Leone, M. Attributable risk from distributed lag models. BMC Med. Res. Methodol. 2014. [Google Scholar] [CrossRef] [PubMed]
- Zeka, A.; Zanobetti, A.; Schwartz, J. Individual-level modifiers of the effects of particulate matter on daily mortality. Am. J. Epidemiol. 2006, 163, 849–859. [Google Scholar] [CrossRef] [PubMed]
- Willink, R. On using the Monte Carlo method to calculate uncertainty intervals. Metrologia 2006, 43, L39–L42. [Google Scholar] [CrossRef]
- McMichael, A.J.; Woodruff, R.E.; Hales, S. Climate change and human health: Present and future risks. Lancet 2006, 367, 859–869. [Google Scholar] [CrossRef]
- Keatinge, W.R.; Donaldson, G.C. The impact of global warming on health and mortality. South Med. J. 2004, 97, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Diaz, J.; Carmona, R.; Mirón, I.J.; Ortiz, C.; Linares, C. Comparison of the effects of extreme temperatures on daily mortality in Madrid (Spain), by age group: The need for a cold wave prevention plan. Environ. Res. 2015, 143, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Breitner, S.; Pan, X.; Franck, U.; Leitte, A.; von Klot, S.; Wichmann, E.; Peters, A.; Schneider, A. Associations of Cardiovascular and Respiratory Mortality with Air Temperature in the Urban Area of Beijing, China. Epidemiology 2011, 22S, S15–S16. [Google Scholar] [CrossRef]
- Keatinge, W.R.; Donaldson, G.C. Winter mortality in elderly people in Britain—Action on outdoor cold stress is needed to reduce winter mortality. Br. Med. J. 2004. [Google Scholar] [CrossRef] [PubMed]
- Koskela, H.O. Cold air-provoked respiratory symptoms: The mechanisms and management. Int. J. Circumpolar Health 2007, 66, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Liener, K.; Leiacker, R.; Lindemann, J.; Rettinger, G.; Keck, T. Nasal mucosal temperature after exposure to cold, dry air and hot, humid air. Acta Oto-Laryngol. 2003, 123, 851–856. [Google Scholar]
- Bennett, C.M.; Dear, K.B.; McMichael, A.J. Shifts in the seasonal distribution of deaths in Australia, 1968–2007. Int. J. Biometeorol. 2014, 58, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Gasparrini, A.; Armstrong, B.G.; Tawatsupa, B.; Tobias, A.; Lavigne, E.; Coelho, M.D.S.Z.S.; Pan, X.; Kim, H.; Hashizume, M.; et al. Temperature Variability and Mortality: A Multi-Country Study. Environ. Health Perspect. 2016, 124, 1554–1559. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Gasparrini, A.; Armstrong, B.; Li, S.; Tawatsupa, B.; Tobias, A.; Lavigne, E.; Coelho, M.D.S.Z.S.; Leone, M.; Pan, X.; et al. Global variation in the effects of ambient temperature on mortality a systematic evaluation. Epidemiology 2014, 25, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Kinney, P.L.; Schwartz, J.; Pascal, M.; Petkova, E.; Le Tertre, A.; Medina, S.; Vautard, R. Winter season mortality: Will climate warming bring benefits? Environ. Res. Lett. 2015. [Google Scholar] [CrossRef] [PubMed]





| Variables | Mean ± SD | Min | P25 | P50 | P75 | Max |
|---|---|---|---|---|---|---|
| Meteorological Factors | ||||||
| Temperature (°C) | 16.2 ± 7.6 | −0.3 | 9.3 | 17.3 | 22.8 | 29.4 |
| Relative humidity (%) | 74.8 ± 8.9 | 33.5 | 69.0 | 76.0 | 81.1 | 92.5 |
| Pressure (hpa) | 942.5 ± 7.2 | 925.2 | 936.4 | 942.7 | 948.2 | 963.8 |
| Wind speed (m/s) | 1.1 ± 0.4 | 0.2 | 0.8 | 1.0 | 1.3 | 3.0 |
| NAD | 188.9 ± 34.8 | 110.0 | 165.0 | 183.0 | 209.0 | 318.0 |
| Cardiovascular | 58.24 ± 13.7 | 21.0 | 49.0 | 56.0 | 67.0 | 118.0 |
| Respiratory | 48.6 ± 16.2 | 16.0 | 37.0 | 44.0 | 58.0 | 109.0 |
| Sex | ||||||
| Male | 110.7 ± 21.1 | 61.0 | 96.0 | 107.0 | 123.0 | 191.0 |
| Female | 78.23 ± 16.8 | 36.0 | 66.0 | 76.0 | 88.0 | 150.0 |
| Age | ||||||
| Age (0–64) | 89.9 ± 14.3 | 51.0 | 80.0 | 89.0 | 98.0 | 139.0 |
| Age (65+) | 99.0 ± 24.1 | 47.0 | 82.0 | 95.0 | 113.0 | 198.0 |
| Group | Minimum Mortality Percentile | Total | Cold | Heat |
|---|---|---|---|---|
| NAD | 62nd | 10.93% (7.99%–13.65%) | 9.96% (6.90%–12.81%) | 0.97% (−0.45%–2.35%) |
| Cir. | 72nd | 12.09% (7.12%–16.48%) | 11.40% (6.29%–16.01%) | 0.69% (−1.69%–2.89%) |
| Res. | 58th | 19.69% (14.45%–24.24%) | 16.17% (10.65%–21.02%) | 3.53% (1.29%–5.59%) |
| Male | 72nd | 10.29% (6.56%–13.70%) | 10.07% (6.22%–13.65%) | 0.22% (−1.65%–1.99%) |
| Female | 58th | 11.78% (7.45%–15.69%) | 9.77% (5.25%–13.80%) | 2.02% (−0.01%–3.92%) |
| Age 0–64 | 100th | 8.21% (4.14%–11.89%) | 7.66% (3.45%–11.52%) | 0.56% (−1.48%–2.47%) |
| Age 65+ | 68th | 13.50% (9.69%–16.99%) | 12.13% (8.10%–15.82%) | 1.37% (−0.43%–3.09%) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, Y.; Yin, F.; Deng, Y.; Volinn, E.; Chen, F.; Ji, K.; Zeng, J.; Zhao, X.; Li, X. Heat or Cold: Which One Exerts Greater Deleterious Effects on Health in a Basin Climate City? Impact of Ambient Temperature on Mortality in Chengdu, China. Int. J. Environ. Res. Public Health 2016, 13, 1225. https://doi.org/10.3390/ijerph13121225
Cui Y, Yin F, Deng Y, Volinn E, Chen F, Ji K, Zeng J, Zhao X, Li X. Heat or Cold: Which One Exerts Greater Deleterious Effects on Health in a Basin Climate City? Impact of Ambient Temperature on Mortality in Chengdu, China. International Journal of Environmental Research and Public Health. 2016; 13(12):1225. https://doi.org/10.3390/ijerph13121225
Chicago/Turabian StyleCui, Yan, Fei Yin, Ying Deng, Ernest Volinn, Fei Chen, Kui Ji, Jing Zeng, Xing Zhao, and Xiaosong Li. 2016. "Heat or Cold: Which One Exerts Greater Deleterious Effects on Health in a Basin Climate City? Impact of Ambient Temperature on Mortality in Chengdu, China" International Journal of Environmental Research and Public Health 13, no. 12: 1225. https://doi.org/10.3390/ijerph13121225
APA StyleCui, Y., Yin, F., Deng, Y., Volinn, E., Chen, F., Ji, K., Zeng, J., Zhao, X., & Li, X. (2016). Heat or Cold: Which One Exerts Greater Deleterious Effects on Health in a Basin Climate City? Impact of Ambient Temperature on Mortality in Chengdu, China. International Journal of Environmental Research and Public Health, 13(12), 1225. https://doi.org/10.3390/ijerph13121225