Environmental Foundations of Typhoid Fever in the Fijian Residential Setting



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.1.1. Geography and Demography
2.1.2. Typhoid Epidemiology
2.1.3. Access to Safe Water and Sanitation
2.2. Residential Setting Selection and Evaluation
2.2.1. Selection of Residences
2.2.2. Geographical Position
2.2.3. Living Condition Evaluation
2.3. Collection and Analysis of Water and Soil Samples
2.4. Data Analysis
2.5. Research Ethics
3. Results
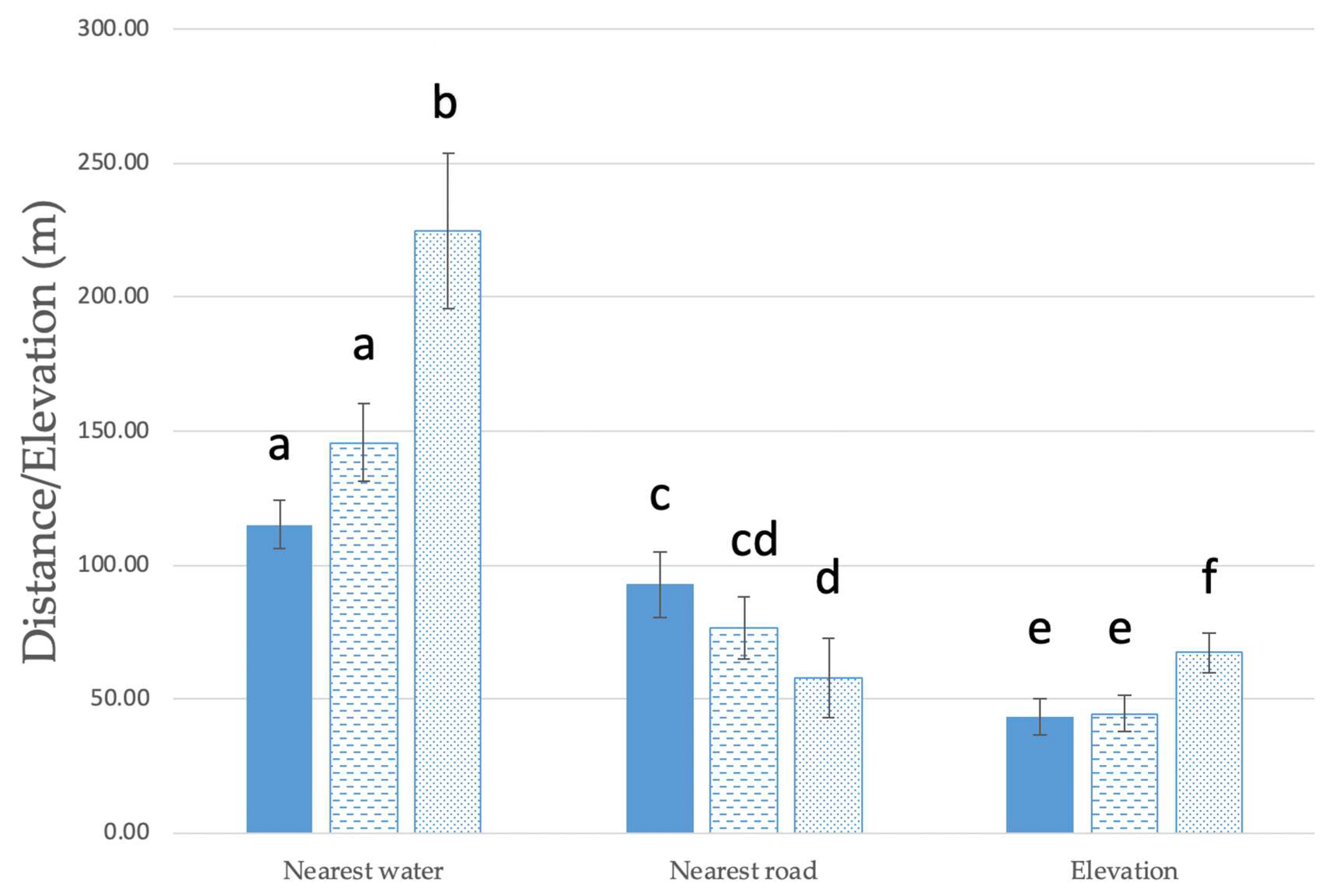
3.1. Proximal Residential Setting
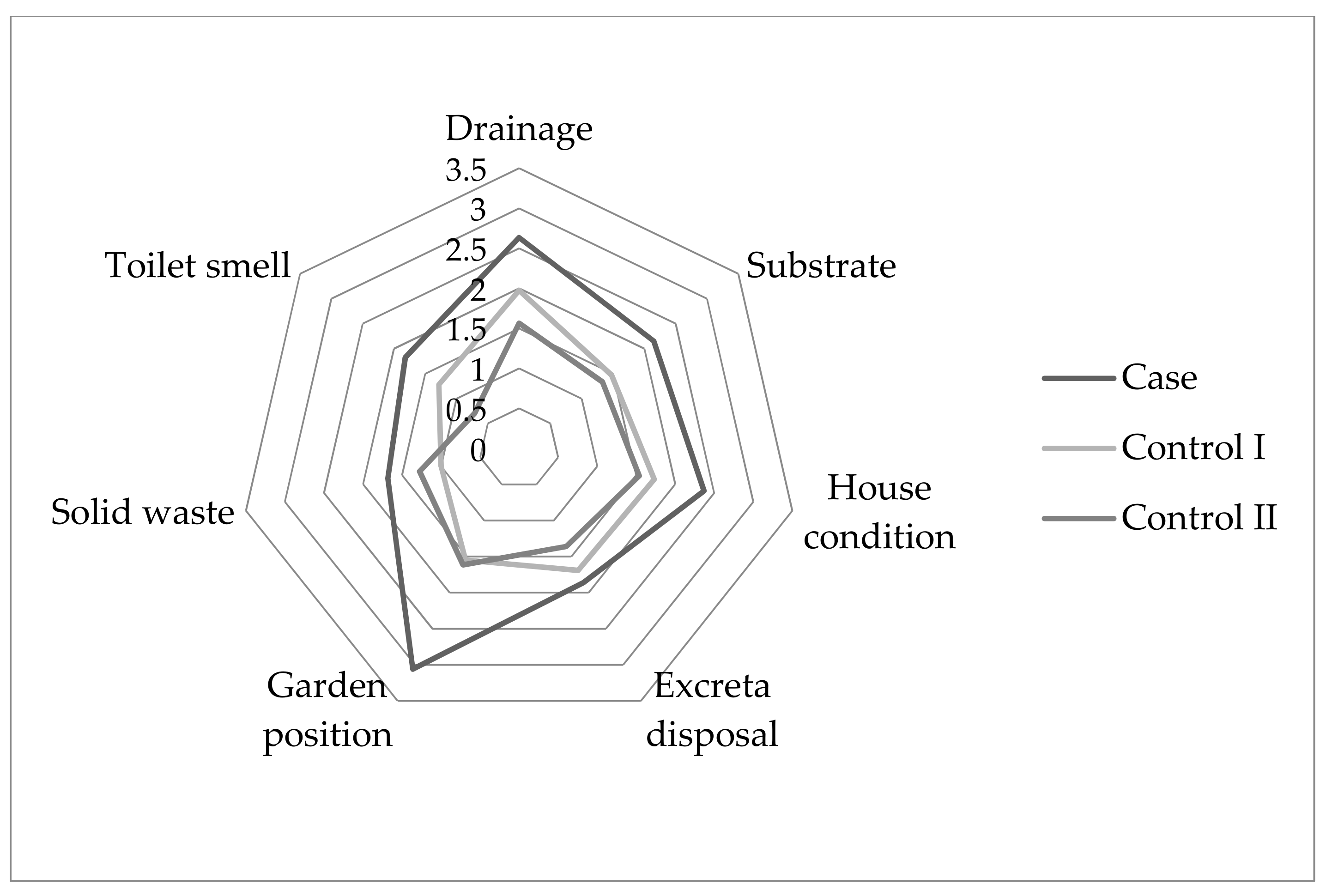
3.2. Household Living Conditions
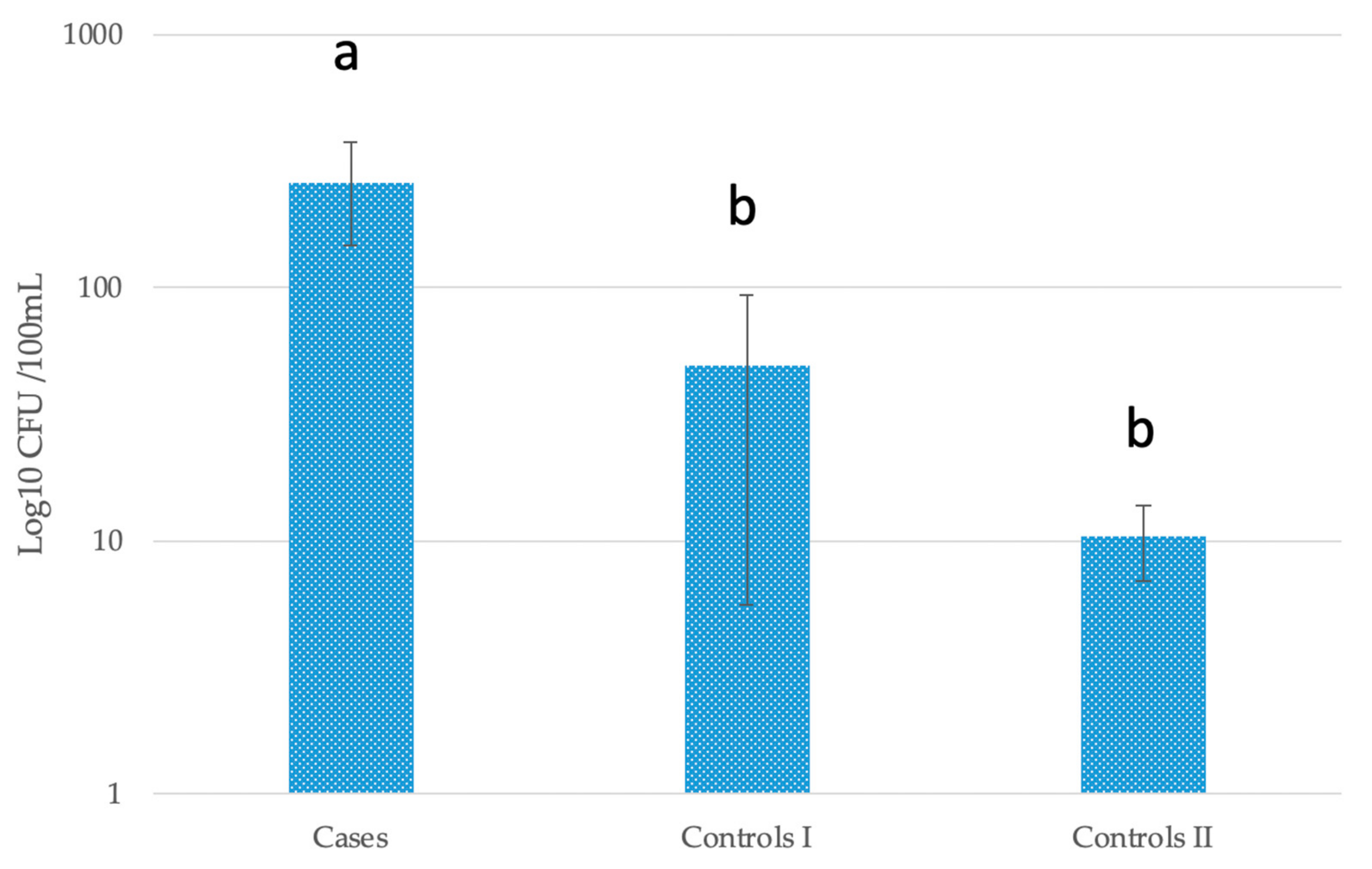
3.3. Biophysical Parameters of Water and Soil (Summary Statistics in Appendix Table A3)
Escherichia coli in Stored Water
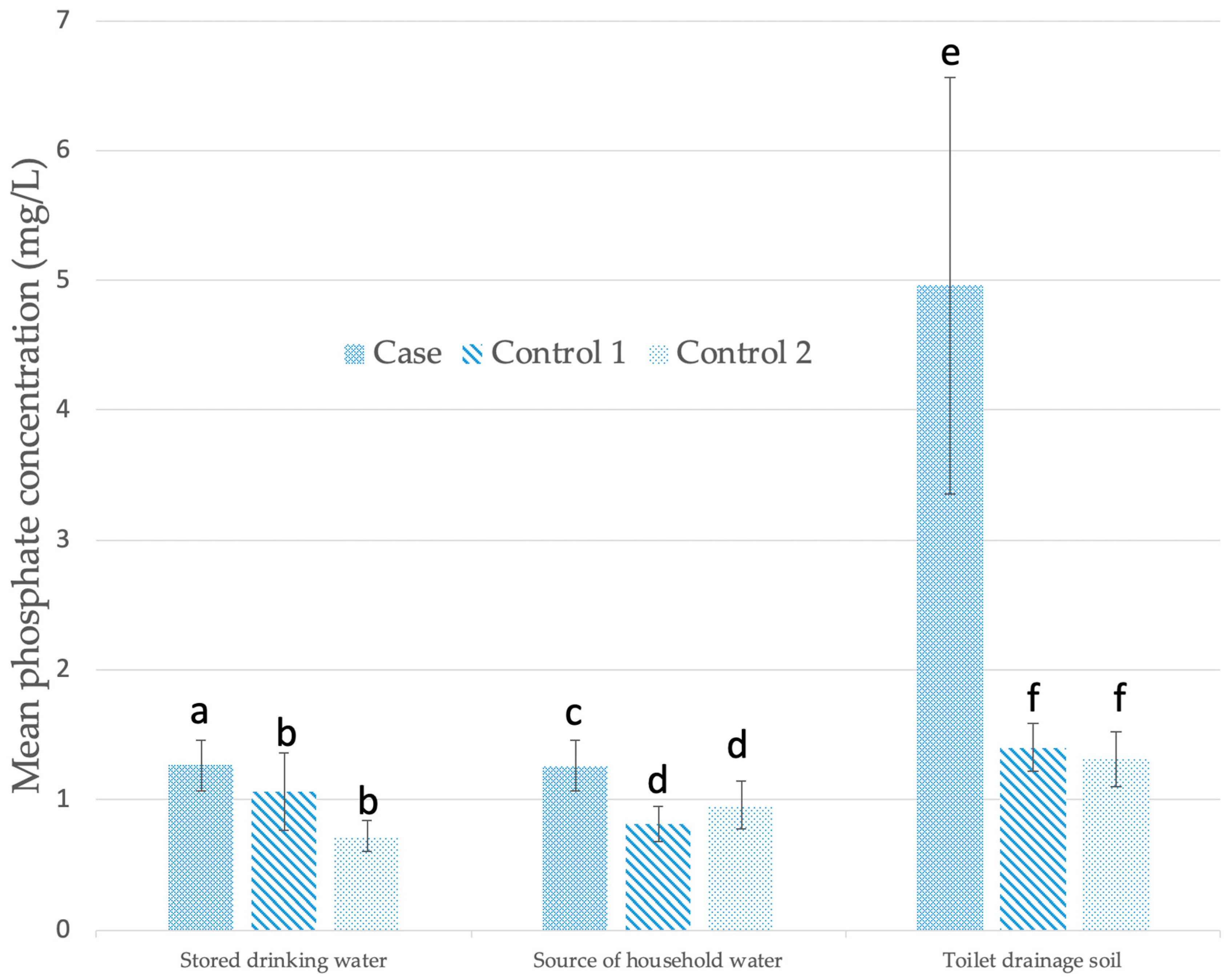
3.4. Physicochemical Parameters
3.5. Factor Analysis
- External Condition = −1.830 + 0.384 (Substrate) + 0.249 (Drainage) + 0.197 (House condition) + 0.146 (Solid waste) +0.055 (Garden position)
- Drinking Water Condition = −0.691 + 0.509 (Drinking water storage) + 0.201 (Phosphate SHW) + 0.002 (Nearest road) + 0.001 (E. coli SHW)
- Sanitary Condition = −0.611 + 2.181 (Ammonia SHW) + 0.404 (Toilet smell)
- Toilet Drainage−Microbial = −1.617 + 0.001 (E. coli TDS)
- Toilet Drainage−Nutrient = −3.72 + 0.140 (Phosphate TDS)
4. Discussion
4.1. External Conditions
4.2. Drinking Water Conditions
4.3. Sanitation Conditions
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Blank | 0 | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|---|
| Bathing environs | Do not know | Inside, piped, treated | Inside, piped, untreated | Outside, piped, treated | Outside, piped or unpiped, untreated | Outside, stream |
| Drainage near house | Do not know | Excellent | Good | Moderate | Minimal | Terrible |
| Drinking water environs | Do not know | Inside, piped, treated | Inside, piped, untreated | Outside, piped, treated | Outside, piped or unpiped, untreated | Outside, stream |
| Drinking Water Storage | Do not know/Not stored | Inside, closed mouth | Inside, open mouth | Outside, closed mouth | Outside, open mouth, sheltered | Outside, open mouth, unsheltered |
| Faecal disposal | Do not know | Flush to sewer line | Flush to intact septic | Flush to damaged septic | Improved Pit latrine | Unimproved pit latrine |
| Garden position | Do not know | Distant and above toilet or septic tank | Distant and level or below toilet or septic tank | Moderate distance from toilet or septic tank | Near and above toilet or septic | Directly below toilet or septic |
| House condition | Do not know | Well maintained | Few repairs needed | Moderate repairs needed | Large repairs needed | Major state of disrepair |
| Housing density | Do not know | Very distant | Distant | Moderately close | Very close | Against another house |
| Smell near toilet | Do not know | None | Slight smell | Moderate smell | Clear smell of faeces or rubbish | Very strong smell of faeces or rubbish |
| Solid waste near house | Do not know | None | Little | Moderate | High | Very High |
| Substrate near house | Do not know | Paved | Fully Vegetated | Moderately vegetated | Minimally vegetated | Bare soil |
| Microbiological/Physicochemical Parameter | Stored Drinking Water | Drinking Water Source | Nearest Stream Water | ||||||
|---|---|---|---|---|---|---|---|---|---|
| C | CI | CII | C | CI | CII | C | CI | CII | |
| Coliforms (CFU/100 mL) | 31 | 25 | 27 | 38 | 36 | 41 | 30 | 25 | 16 |
| E. coli (CFU/100 mL) | 31 | 25 | 27 | 38 | 36 | 41 | 25 | 16 | 15 |
| Turbidity (FTU) | 31 | 22 | 27 | 33 | 32 | 35 | 20 | 13 | 9 |
| Phosphate (mg/L) | 30 | 24 | 26 | 37 | 35 | 39 | 27 | 13 | 14 |
| Nitrate (mg/L) | 30 | 24 | 26 | 36 | 35 | 39 | 25 | 15 | 14 |
| Ammonia (mg/L) | 30 | 24 | 26 | 37 | 36 | 40 | 27 | 17 | 17 |
| Electrical Conductivity (uS/cm) | 30 | 25 | 25 | 37 | 35 | 39 | 25 | 15 | 12 |
| Temperature (°C) | 30 | 25 | 25 | 37 | 35 | 39 | 25 | 14 | 12 |
| Dissolved Oxygen (mg/L) | 28 | 23 | 23 | 36 | 34 | 37 | 23 | 14 | 11 |
| pH | 30 | 25 | 25 | 37 | 35 | 39 | 24 | 15 | 12 |
| # Measurements taken | 301 | 242 | 257 | 366 | 349 | 389 | 251 | 157 | 132 |
| Microbiological/Physicochemical Parameter | Toilet Soil | Toilet Drainage Soil | Household Garden Soil | ||||||
|---|---|---|---|---|---|---|---|---|---|
| C | CI | CII | C | CI | CII | C | CI | CII | |
| Coliforms (CFU/100 mL) | 31 | 16 | 9 | 40 | 37 | 40 | 32 | 28 | 27 |
| E. coli (CFU/100 mL) | 31 | 15 | 9 | 40 | 37 | 49 | 31 | 28 | 27 |
| Phosphate (mg/L) | 30 | 14 | 9 | 37 | 36 | 38 | 27 | 28 | 25 |
| Nitrate (mg/L) | 30 | 15 | 9 | 39 | 38 | 32 | 32 | 29 | 26 |
| Ammonia (mg/L) | 30 | 15 | 9 | 37 | 39 | 34 | 27 | 29 | 27 |
| Electrical Conductivity (uS/cm) | 30 | 14 | 9 | 40 | 36 | 38 | 33 | 28 | 25 |
| Temperature (°C) | 30 | 14 | 9 | 40 | 36 | 38 | 33 | 28 | 25 |
| Dissolved Oxygen (mg/L) | 28 | 13 | 9 | 38 | 34 | 36 | 32 | 28 | 24 |
| pH | 30 | 14 | 9 | 40 | 36 | 38 | 33 | 28 | 25 |
| # Measurements taken | 270 | 130 | 81 | 351 | 329 | 343 | 280 | 254 | 231 |
| Microbiological/Physicochemical Parameter | Stored Drinking Water | Drinking Water Source | Nearest Stream Water | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | R | SD | n | R | SD | n | R | SD | ||||
| Coliforms (CFU/100 mL) | 83 | 274 | 2397 | 639.3 | 115 | 181 | 2397 | 521.8 | 71 | 1495.1 | 2397 | 991.3 |
| E. coli (CFU/100 mL) | 83 | 115.2 | 2397 | 416.6 | 115 | 55.8 | 1097 | 186.2 | 56 | 802.1 | 2397 | 940.2 |
| Turbidity (FTU) | 83 | 2.2 | 27 | 3.6 | 100 | 3.3 | 32 | 5.0 | 42 | 31.4 | 807 | 125.5 |
| Phosphate (mg/L) | 80 | 1.0 | 6.0 | 1.1 | 111 | 1.0 | 6.1 | 1.1 | 54 | 1.3 | 8.3 | 1.5 |
| Nitrate (mg/L) | 80 | 0.02 | 0.31 | 0.05 | 110 | 1.0 | 6.1 | 1.1 | 54 | 0.1 | 2.7 | 0.4 |
| Ammonia (mg/L) | 80 | 0.03 | 0.89 | 0.11 | 113 | 0.04 | 1.1 | 0.14 | 61 | 2.3 | 50 | 9.3 |
| Electrical Conductivity (uS/cm) | 80 | 454.9 | 2046.6 | 451.5 | 111 | 273.9 | 1943.1 | 360 | 52 | 218.5 | 1557.1 | 293.2 |
| Temperature (°C) | 80 | 25.9 | 18.3 | 3.1 | 111 | 26.4 | 10.8 | 2.3 | 51 | 25.8 | 12 | 2.3 |
| Dissolved Oxygen (mg/L) | 74 | 97.9 | 50.7 | 7.5 | 98 | 102 | 54.9 | 7.9 | 47 | 84.1 | 125.4 | 30.2 |
| pH | 80 | 6.8 | 2.3 | 0.5 | 111 | 6.9 | 2.2 | 0.4 | 51 | 6.7 | 4.7 | 0.8 |
| Microbiological/Physicochemical Parameter | Toilet Soil | Toilet Drainage Soil | Household Garden Soil | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | R | SD | n | R | SD | n | R | SD | ||||
| Coliforms (CFU/100 mL) | 42 | 1832.6 | 2397 | 946.1 | 117 | 1944.7 | 2397 | 862.9 | 87 | 2023.9 | 2397 | 819.6 |
| E. coli (CFU/100 mL) | 42 | 1579.2 | 2397 | 1032.2 | 117 | 1647.6 | 2397 | 997.9 | 86 | 1673.2 | 2397 | 1011.2 |
| Phosphate (mg/L) | 40 | 1.5 | 12.5 | 2.21 | 114 | 2.7 | 45 | 6.3 | 86 | 1.7 | 12.1 | 2.2 |
| Nitrate (mg/L) | 40 | 1.0 | 26.4 | 4.2 | 114 | 1.5 | 32.5 | 4.6 | 87 | 0.3 | 7.2 | 1.0 |
| Ammonia (mg/L) | 41 | 1.9 | 50 | 8.5 | 116 | 2.2 | 50 | 9.1 | 86 | 0.5 | 22 | 2.5 |
| Electrical Conductivity (uS/cm) | 41 | 196.9 | 1949.3 | 342.3 | 114 | 123.8 | 1172.3 | 178.2 | 88 | 97.8 | 1682.9 | 218.4 |
| Temperature (°C) | 40 | 26.3 | 9.2 | 2.1 | 114 | 26.3 | 9.8 | 2.1 | 88 | 26.4 | 10 | 2.1 |
| Dissolved Oxygen (mg/L) | 39 | 85.2 | 97.1 | 25.1 | 108 | 83.4 | 104.3 | 27.4 | 84 | 83.8 | 104.7 | 29.5 |
| pH | 40 | 6.6 | 4.0 | 0.9 | 114 | 6.6 | 4.7 | 0.9 | 88 | 6.6 | 4.1 | 0.7 |
| Variable |
|---|
| 1. Nearest road (m) |
| 2. Elevation (m) |
| 3. Drainage (0–4) |
| 4. Substrate (0–4) |
| 5. House condition (0–4) |
| 6. Excreta disposal (0–4) |
| 7. Garden position (0–4) |
| 8. Bathing environs (0–4) |
| 9. Drinking water environs (0–4) |
| 10. Drinking water storage (0–4) |
| 11. Housing density (0–4) |
| 12. Solid Waste (0–4) |
| 13. Toilet smell (0–4) |
| 14. Coliforms_SHW (CFU/100 mL) |
| 15. E. coli_SHW (CFU/100 mL) |
| 16. Phosphate_SHW (mg/L) |
| 17. Nitrate_SHW (mg/L) |
| 18. Ammonia_SHW (mg/L) |
| 19. Turbidity_SHW (FTU) |
| 20. Temperature_SHW (oC) |
| 21. Conductivity_SHW (μS) |
| 22. DO_SHW (mg/L) |
| 23. pH_SHW |
| 24. Coliforms_TDS (CFU/100 mL) |
| 25. E. coli_TDS (CFU/100 mL) |
| 26. Phosphate_TDS (mg/L) |
| 27. Nitrate_TDS (mg/L) |
| 28. Ammonia_TDS (mg/L) |
| 29. Temperature_TDS (oC) |
| 30. Conductivity_TDS (μS) |
| 31. DO_TDS (mg/L) |
| 32. pH_TDS |
References
- Watson, C.H.; Edmunds, W.J. A review of typhoid fever transmission dynamic models and economic evaluations of vaccination. Vaccine 2015, 33, 42–54. [Google Scholar] [CrossRef] [PubMed]
- Velema, J.P.; Wijne, G.; Bult, B.; Naerssen, T. Typhoid fever in Ujung Pandang, Indonesia— high-risk groups and high-risk behaviors. Trop. Med. Int. Health 1997, 2, 1088–1094. [Google Scholar] [CrossRef] [PubMed]
- Hennekens, C.H.; Buring, J.E. Case-control Studies. In Epidemiology in Medicine; Mayrent, S.L., Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 1987; pp. 132–152. ISBN1 0316356360. ISBN2 9780316356367. [Google Scholar]
- Baker, S.; Holt, K.E.; Clements, A.C.A.; Karkey, A.; Arjyal, A.; Boni, M.F.; Dongol, S.; Hammond, N.; Koirala, S.; Duy, P.T.; et al. Combined high-resolution genotyping and geospatial analysis reveals modes of endemic urban typhoid fever transmission. Open Biol. 2011, 1, 110008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Alwis, R.; Watson, C.; Nikolay, B.; Lowry, J.H.; Thieu, N.T.; Van, T.T.; Ngoc, D.T.; Rawalai, K.; Taufa, M.; Coriakula, J.; et al. Role of environmental factors in shaping spatial distribution of Salmonella enterica serovar Typhi, Fiji. Emerg. Infect. Dis. 2018, 24, 284. [Google Scholar] [CrossRef] [PubMed]
- Akullian, A.; Ng’eno, E.; Matheson, A.I.; Cosmas, L.; Macharia, D.; Fields, B.; Bigogo, G.; Mugoh, M.; John-Stewart, G.; Walson, J.L.; et al. Environmental transmission of typhoid fever in an urban slum. PLoS Negl. Trop. Dis. 2015, 12, e0004212. [Google Scholar] [CrossRef]
- Jenkins, A.P.; Jupiter, S.; Mueller, U.; Jenney, A.; Vosaki, G.; Rosa, V.; Naucukidi, A.; Mulholland, K.; Strugnell, R.; Kama, M.; et al. Health at the sub-catchment scale: Typhoid and its environmental determinants in Central Division, Fiji. EcoHealth 2016, 13, 633–651. [Google Scholar] [CrossRef] [PubMed]
- Mermin, J.H.; Villar, R.; Carpenter, J.; Roberts, L.; Samaridden, A.; Gasanova, L.; Lomakina, S.; Bopp, C.; Hutwagner, L.; Mead, P.; et al. A massive epidemic of multidrug-resistant typhoid fever in Tajikistan associated with consumption of municipal water. J. Infect. Dis 1999, 179, 1416–1422. [Google Scholar] [CrossRef]
- Kelly-Hope, L.A.; Alonso, W.J.; Thiem, V.D.; Anh, D.D.; Do Gia, C.A.N.H.; Lee, H.; Smith, D.L.; Miller, M.A. Geographical distribution and risk factors associated with enteric diseases in Vietnam. Am. J. Trop Med. Hyg. 2007, 76, 706–712. [Google Scholar] [CrossRef]
- Wang, J.F.; Wang, Y.; Zhang, J.; Christakos, G.; Sun, J.L.; Liu, X.; Lu, L.; Fu, X.Q.; Shi, Y.Q.; Li, X.M. Spatiotemporal transmission and determinants of typhoid and paratyphoid fever in Hongta District, Yunnan Province, China. PLoS Negl. Trop Dis. 2013, 7, e2112. [Google Scholar] [CrossRef]
- Tran, H.H.; Bjune, G.; Nguyen, B.M.; Rottingen, J.A.; Grais, R.F.; Guerin, P.J. Risk factors associated with typhoid fever in Son La province, northern Vietnam. Trans. R. Soc. Trop. Med. Hyg. 2005, 99, 819–826. [Google Scholar] [CrossRef]
- Prasad, N.; Jenkins, A.P.; Naucukidi, L.; Rosa, V.; Sahu-Khan, A.; Kama, M.; Jenkins, K.M.; Jenney, A.W.; Jack, S.J.; Saha, D.; et al. Epidemiology and risk factors for typhoid fever in Central Division, Fiji, 2014–2017: A case-control study. PLoS Negl. Trop. Dis. 2018, 12, e0006571. [Google Scholar] [CrossRef] [PubMed]
- Hoque, B.A.; Chakraborty, J.; Chowdhury, J.T.A.; Chowdhury, U.K.; Ali, M.; El Arifeen, S.; Sack, R.B. Effects of environmental factors on child survival in Bangladesh: A case control study. Public Health 1999, 113, 57–64. [Google Scholar] [CrossRef]
- Sharma, P.K.; Ramakrishnan, R.; Hutin, Y.; Manickam, P.; Gupte, M.D. Risk factors for typhoid in Darjeeling, West Bengal, India: Evidence for practical action. Trop. Med. Int. Health 2009, 14, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Gasem, M.H.; Dolmans, W.M.V.; Keuter, M.M.; Djokomoeljanto, R.R. Poor food hygiene and housing as risk factors for typhoid fever in Semarang, Indonesia. Trop. Med. Int. Health 2001, 6, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Vollaard, A.M.; Ali, S.; van Asten, H.A.; Widjaja, S.; Visser, L.G.; Surjadi, C.; van Dissel, J.T. Risk factors for typhoid and paratyphoid fever in Jakarta, Indonesia. JAMA 2004, 291, 2607–2615. [Google Scholar] [CrossRef] [PubMed]
- Watson, C.H.; Baker, S.; Lau, C.L.; Rawalai, K.; Taufa, M.; Coriakula, J.; Thieu, N.T.V.; Van, T.T.; Ngoc, D.T.T.; Hens, N.; et al. A cross-sectional seroepidemiological survey of typhoid fever in Fiji. PLoS Negl. Trop Dis. 2017, 11, e0005786. [Google Scholar] [CrossRef] [PubMed]
- Hosoglu, S.; Celen, M.K.; Geyik, M.F.; Akalin, S.; Ayaz, C.; Acemoglu, H.; Loeb, M. Risk factors for typhoid fever among adult patients in Diyarbakir, Turkey. Epidemiol. Infec. 2006, 134, 612–616. [Google Scholar] [CrossRef]
- Corner, R.J.; Dewan, A.M.; Hashizume, M. Modelling typhoid risk in Dhaka Metropolitan Area of Bangladesh: The role of socio-economic and environmental factors. Int. J. Health Geogr. 2013, 12, 13. [Google Scholar] [CrossRef]
- Cairncross, S.; Blumenthal, U.; Kolsky, P.; Moraes, L.; Tayeh, A. The public and domestic domains in the transmission of disease. Trop. Med. Int. Health 1996, 1, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Moraes, L.R.S.; Cancio, J.A.; Cairncross, S.; Huttly, S. Impact of drainage and sewerage on diarrhoea in poor urban areas in Salvador, Brazil. Trans. R. Soc. Trop. Med. Hyg. 2003, 97, 153–158. [Google Scholar] [CrossRef]
- Lall, C.; Kumar, K.V.; Raj, R.V.; Vedhagiri, K.; Vijayachari, P. Prevalence and diversity of leptospires in different ecological niches of urban and rural areas of South Andaman Island. Microbes Environ. 2016, 31, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Karkey, A.; Jombart, T.; Walker, A.W.; Thompson, C.N.; Torres, A.; Dongol, S.; Thieu, N.T.V.; Thanh, D.P.; Ngoc, D.T.T.; Vinh, P.V.; et al. The ecological dynamics of fecal contamination and Salmonella Typhi and Salmonella Paratyphi A in municipal Kathmandu drinking water. PLoS Negl. Trop Dis. 2016, 10, e0004346. [Google Scholar] [CrossRef] [PubMed]
- Neall, V.E.; Trewick, S.A. The age and origin of the Pacific islands: A geological overview. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2008, 363, 3293–3308. [Google Scholar] [CrossRef] [PubMed]
- Barker, G.M.; Price, R.J.; McGree, S. Climate Surfaces for Fiji; LandCare Research: Hamilton, New Zealand, 2016. [Google Scholar]
- World Health Organization. Meeting Report: Expert Consultation on Typhoid Fever Vaccination in Fiji; Ministry of Health: Suva, Fiji, 2010. [Google Scholar]
- Scobie, H.M.; Nilles, E.; Kama, M.; Kool, J.L.; Mintz, E.; Wannemuehler, K.A.; Hyde, T.B.; Dawainavesi, A.; Singh, S.; Korovou, S.; et al. Impact of a targeted typhoid vaccination campaign following cyclone Tomas, Republic of Fiji, 2010. Am. J. Trop. Med. Hyg. 2014, 90, 1031–1038. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.N.; Kama, M.; Acharya, S.; Bera, U.; Clemens, J.; Crump, J.A.; Dawainavesi, A.; Dougan, G.; Edmunds, W.J.; Fox, K.; et al. Typhoid fever in Fiji: A reversible plague? Trop. Med. Int. Health 2014, 19, 1284–1292. [Google Scholar] [CrossRef] [PubMed]
- Singh, S. Epidemiology of Laboratory Confirmed Typhoid Fever Cases from Year 2000 to July 2010 in the Central Eastern Division in Fiji; Department of Microbiology, College of Medicine, Nursing and Health Sciences, Fiji National University: Suva, Fiji, 2010. [Google Scholar]
- Cameron, J. Confronting social policy challenges in Fiji. In Confronting Fiji Futures; Akram-Lodhi, H., Ed.; ANU Press: Canberra, Australia, 2016; p. 133. ISBN 9781921934292. [Google Scholar]
- WHO/FMOH/UNDP. Protecting Human Health from Climate Change: Working Paper—Climate-Sensitive Infectious Diseases in Fiji; World Health Organization, Fiji Ministry of Health, United Nations Development Program: Suva, Fiji, 2011. [Google Scholar]
- Jenkins, K. Post Cyclone Tomas Support to Typhoid fever control in Fiji March 2010; Fiji Health Sector Improvement Program: Suva, Fiji, 2010. [Google Scholar]
- World Health Organization. Sanitation, Drinking Water and Health in Pacific Island Countries: 2015 Update and Future Outlook; World Health Organization, Regional Office for the Western Pacific: Manila, Philippines, 2016; pp. 1–108. ISBN 9789290617471. [Google Scholar]
- Bain, R.; Cronk, R.; Hossain, R.; Bonjour, S.; Onda, K.; Wright, J.; Yang, H.; Slaymaker, T.; Hunter, P.; Prüss-Ustün, A.; et al. Global assessment of exposure to faecal contamination through drinking water based on a systematic review. Trop. Med. Int. Health 2014, 19, 917–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Government of Fiji. Fiji National Liquid Waste Management Strategy and Action Plan; International Waters of the Pacific Islands: Suva, Fiji, 2006; pp. 1–72. [Google Scholar]
- WHO/UNICEF Joint Monitoring Program on Water and Sanitation (JMP). Progress on Drinking Water, Sanitation and Hygiene 2017 Update and SDG Baselines; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 159–174. [Google Scholar] [CrossRef]
- McCrady, M.H. Tables for rapid interpretation of fermentation-tube results. J. Public Health 1918, 9, 201–220. [Google Scholar]
- Osborne, J.W.; Costello, A.B.; Kellow, J.T. Best practices in exploratory factor analysis. In Best Practices in Quantitative Methods; Osborne, J., Ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2008; pp. 86–99. [Google Scholar] [CrossRef]
- Dempster, A.P.; Laird, N.M.; Rubin, D.B. Maximum likelihood from incomplete data via the EM algorithm. J. R. Stat. Soc. Ser. B 1977, 39, 1–38. [Google Scholar] [CrossRef]
- Ngugi, H.N.; Home, P.G.; Mutwiwa, U.N. Impacts of water and sanitation activities on the environment in the Upper Mara Basin. Civ. Env. Res. 2017, 6, 9–16. [Google Scholar]
- Craun, G.F. A summary of waterborne illness transmitted through contaminated groundwater. J. Environ. Health 1985, 48, 122–127. [Google Scholar]
- Dewan, A.M.; Corner, R.; Hashizume, M.; Ongee, E.T. Typhoid Fever and its association with environmental factors in the Dhaka Metropolitan Area of Bangladesh: A spatial and time-series approach. PLoS Negl. Trop. Dis. 2013, 7, e1998. [Google Scholar] [CrossRef] [PubMed]
- Gaffield, S.J.; Goo, R.L.; Richards, L.A.; Jackson, R.J. Public health effects of inadequately managed stormwater runoff. Am. J. Public Health 2003, 93, 1527–1533. [Google Scholar] [CrossRef] [PubMed]
- Leslie, D. A Reference Manual for Utilizing and Managing the Soil Resources of Fiji; Secretariat of the Pacific Community, Land Resources Publication Unit: Nabua, Fiji, 2016. [Google Scholar]
- Ling, T.Y.; Achberger, E.C.; Drapcho, C.M.; Bengtson, R.L. Quantifying adsorption of an indicator bacteria in a soil–water system. Trans. ASAE 2002, 45, 669. [Google Scholar]
- Mitscherlich, E.; Marth, E.H. Microbial Survival in the Environment: Bacteria and Rickettsiae Important in Human and Animal Health; Springer Science & Business Media: New York, NY, USA, 2012; ISBN 9783642699764. [Google Scholar]
- Smith, S.J. Health status and the housing system. Soc. Sci. Med. 1990, 31, 753–762. [Google Scholar] [CrossRef]
- Siwatibau, S. Traditional Environmental Practices in the South Pacific: A case study of Fiji. Ambio 1984, 1, 365–368. [Google Scholar]
- Sears, S.D.; Ferreccio, C.; Levine, M.M.; Cordano, A.M.; Monreal, J.; Black, R.E.; D’Ottone, K.; Rowe, B.; Chilean Typhoid Committee. The use of Moore swabs for isolation of Salmonella typhi from irrigation water in Santiago, Chile. J. Infect. Dis. 1984, 149, 640–642. [Google Scholar] [CrossRef]
- Golterman, H.L. The Chemistry of Phosphate and Nitrogen Compounds in Sediments; Springer Science & Business Media: New York, NY, USA, 2007; ISBN 978-1-4020-2516-7. [Google Scholar]
- World Health Organization. Guidelines for Drinking-Water Quality, 4th ed.; World Health Organization: Geneva, Switzerland, 2011; ISBN 9787313123671. [Google Scholar]
- Luby, S.P.; Faizan, M.K.; Fisher-Hoch, S.P.; Syed, A.; Mintz, E.D.; Bhutta, Z.A.; McCormick, J.B. Risk factors for typhoid fever in an endemic setting, Karachi, Pakistan. Epidemiol. Infect. 1998, 120, 129–138. [Google Scholar] [CrossRef]
- Fujioka, R.; Sian-Denton, C.; Borja, M.; Castro, J.; Morphew, K. Soil: The environmental source of Escherichia coli and enterococci in Guam’s streams. J. Appl. Microbiol. 1998, 85, 83S–89S. [Google Scholar] [CrossRef]
- Jenkins, M.W.; Cairncross, S. Modelling latrine diffusion in Benin: Towards a community typology of demand for improved sanitation in developing countries. J. Water Health 2010, 8, 166–183. [Google Scholar] [CrossRef] [PubMed]
- Bishop, P.K.; Misstear, B.D.; White, M.; Harding, N.J. Impacts of sewers on groundwater quality. Water Environ. J. 1998, 12, 216–223. [Google Scholar] [CrossRef]
- Song, J.W.; Chung, K.C. Observational studies: cohort and case-control studies. Plast. Reconstr. Surg. 2010, 126, 2234. [Google Scholar] [CrossRef] [PubMed]





| Base Layer | Source | Dataset Details | Processing Details * |
|---|---|---|---|
| Viti Levu coastline | Fiji Department of Lands, National Government (NG) | NA | None |
| Central Division boundary | iTaukei Lands and Fisheries Commission, NG | NA | Removed small islands off Viti Levu |
| Road network | Fiji Roads Authority, NG | 2015 update (sealed and unsealed) | None |
| River network | Fiji Department of Lands, NG | Primary network with 2nd order streams | None |
| Creek network | Fiji Department of Lands, NG | 3rd order and higher creeks | Merged creek and river layers to create hydrology network layer |
| Dense forest cover | Fiji Department of Forestry (DoF), NG | Digitized from 2001 Landsat ETM+ data, verified against DoF vegetation maps of 2010 | None |
| Digital terrain model (DTM) | Secretariat of the Pacific Community, Geoscience Division | 25 m resolution with contour shading | None |
| Typhoid case and control household positions | This study | Digitized from GPS Map80 position, 1 m in front of house. | None |
| FACTORS | ||||||
|---|---|---|---|---|---|---|
| Variables | 1 (External Condition) | 2 (Drinking Water Condition) | 3 (Sanitary Conditions) | 4 (TDS Microbial) | 5 (TDS Nutrient) | Communalities |
| Substrate | 0.827 | 0.000 | −0.008 | 0.035 | −0.037 | 0.648 |
| Drainage | 0.780 | 0.177 | 0.157 | −0.008 | 0.034 | 0.706 |
| House condition | 0.724 | −0.003 | 0.006 | −0.041 | 0.084 | 0.665 |
| Solid Waste | 0.532 | −0.165 | 0.035 | −0.185 | −0.007 | 0.515 |
| Garden position | 0.448 | 0.279 | 0.236 | −0.101 | 0.126 | 0.471 |
| E. coli SHW | 0.078 | 0.665 | −0.138 | −0.070 | −0.110 | 0.487 |
| Drinking water storage | 0.007 | 0.634 | 0.151 | 0.090 | 0.170 | 0.506 |
| Phosphate SHW | −0.049 | 0.472 | −0.087 | −0.145 | 0.047 | 0.408 |
| Nearest road | 0.055 | 0.459 | 0.149 | −0.089 | −0.028 | 0.427 |
| Toilet smell | 0.277 | −0.054 | 0.642 | 0.008 | 0.045 | 0.510 |
| Ammonia SHW | −0.009 | 0.094 | 0.420 | 0.165 | −0.080 | 0.360 |
| E. coli TDS | −0.032 | −0.064 | 0.011 | 0.592 | 0.111 | 0.405 |
| Ammonia TDS | −0.001 | −0.128 | 0.356 | 0.590 | 0.085 | 0.368 |
| Phosphate TDS | 0.080 | 0.113 | −0.077 | 0.171 | 0.899 | 0.452 |
| Eigenvalue | 4.193 | 3.010 | 2.516 | 1.976 | 1.892 | |
| Cumulative % variance | 13.1 | 22.5 | 30.4 | 36.5 | 42.5 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jenkins, A.P.; Jupiter, S.D.; Jenney, A.; Rosa, V.; Naucukidi, A.; Prasad, N.; Vosaki, G.; Mulholland, K.; Strugnell, R.; Kama, M.; et al. Environmental Foundations of Typhoid Fever in the Fijian Residential Setting. Int. J. Environ. Res. Public Health 2019, 16, 2407. https://doi.org/10.3390/ijerph16132407
Jenkins AP, Jupiter SD, Jenney A, Rosa V, Naucukidi A, Prasad N, Vosaki G, Mulholland K, Strugnell R, Kama M, et al. Environmental Foundations of Typhoid Fever in the Fijian Residential Setting. International Journal of Environmental Research and Public Health. 2019; 16(13):2407. https://doi.org/10.3390/ijerph16132407
Chicago/Turabian StyleJenkins, Aaron P., Stacy D. Jupiter, Adam Jenney, Varanisese Rosa, Alanieta Naucukidi, Namrata Prasad, Gandercillar Vosaki, Kim Mulholland, Richard Strugnell, Mike Kama, and et al. 2019. "Environmental Foundations of Typhoid Fever in the Fijian Residential Setting" International Journal of Environmental Research and Public Health 16, no. 13: 2407. https://doi.org/10.3390/ijerph16132407
APA StyleJenkins, A. P., Jupiter, S. D., Jenney, A., Rosa, V., Naucukidi, A., Prasad, N., Vosaki, G., Mulholland, K., Strugnell, R., Kama, M., Crump, J. A., & Horwitz, P. (2019). Environmental Foundations of Typhoid Fever in the Fijian Residential Setting. International Journal of Environmental Research and Public Health, 16(13), 2407. https://doi.org/10.3390/ijerph16132407