Abstract
Altogether, 1588 dietitians were dispatched from the Japan Dietetic Association (JDA) to a disaster area for the first time on a nationwide scale following the 2011 Great East Japan Earthquake. Various studies have been conducted based on the activity reports, but the support that the disaster area requested was not documented. The purpose of this study is to identify the support that was needed in the disaster area. Therefore, we investigated the necessary support desired by dietitians who lived in the disaster areas. Questionnaires were sent to 1911 dietitians who were members of the JDA and lived in 3 affected prefectures in August 2012. In total, 435 dietitians (22.8%) completed the questionnaire. Among the questions on the questionnaire, we analyzed answers to the open-ended question: “Please write freely about the support that you wanted at the time of the disaster” (n = 332). Using qualitative descriptive analysis, we extracted data from the answers and categorized and labeled them into similar groups. These groups were divided into four categories: (1) “goods,” (2) “establishing a system in advance of a large-scale disaster,” (3) “information,” and (4) “human resources.” To provide “goods,” “information,” and “human resources” to the disaster area smoothly, it is important to plan a “system” in advance of large-scale disasters.
1. Introduction
In recent years, natural hazards, such as earthquakes, typhoons, and hurricanes, have occurred around the world. Natural hazards cascade to cause disasters [1]. For example, earthquakes trigger a cascade of disasters such as building collapses, cracks, tsunamis, etc.
After such a cascading disaster, the living environment of those who are affected often deteriorates. Necessities such as electricity, gas, and water cease, and roads may be damaged due to the collapse of buildings and landslides. It is not unexpected that dietary conditions may worsen. Several studies demonstrated that food provided to emergency shelters in Japan consisted mainly of carbohydrate-rich foods, such as rice balls, bread, and instant noodles [2,3,4]. It has also been reported that the worsening of dietary conditions following a disaster induces a deterioration in the health condition of survivors.
The Great East Japan Earthquake hit the Tohoku district of Japan on 11 March 2011. It was reported that 19,689 were killed, 2563 were missing, and 6233 were injured (as of 8 March 2019) [5]. This earthquake is a typical cascading disaster. It triggered building collapses, a tsunami, and a nuclear reactor meltdown. Many survivors were forced to live in emergency shelters where the provision of food consisted mainly of carbohydrate-rich foods and the nutritional balance was poor, similar to the previous disaster [4]. Furthermore, the nutritional balance still did not improve even 1 month after the disaster, and this was expected to continue [6]. Therefore, the Ministry of Health, Labor and Welfare (MHLW) published Nutritional Reference Values for meal provision in emergency shelters [7]. In addition, the MHLW asked the Japan Dietetic Association (JDA) to assist with supplying food and nutrition in the disaster areas on 22 March 2011. The JDA dispatched registered dietitians and general dietitians (RDs) to the disaster areas for the first time on a national scale.
Support activities by dispatched RDs has been documented [8]. The study reported that the frequency of “Meeting” for RDs was the highest to share information with other supporters. Additionally, the frequency of “dietary/nutritional assessment” was high. In the analysis of “What I Thought Today” reported by dispatched RDs, it was recorded that they felt anxiety, tension, and discomfort [9]. On the other hand, the analysis found that dispatched RDs felt needed in the disaster areas. The usefulness of RDs has been proven in emergency shelters. We reported that menu creation by RDs improved the diets in emergency shelters [10]. In addition, the benefits as seen from the viewpoint of RDs in the disaster area have been assessed. The benefits included the usefulness of the RDs’ skills during disasters and the fact that their assistance provided mental support [11]. On the other hand, it was documented that the assistance provided was not necessarily consistent with needs, a problematic point [11]. However, the support that RDs in the disaster area actually needed has not been documented.
In the present study, we document the support that was needed for RDs in the disaster area. The findings of this study can be used to clarify the ways in which we can make the necessary preparations and plan for support activities in future cascading disasters.
2. Materials and Methods
2.1. Setting and Participants
In August 2012, survey questionnaires were sent to 1911 RDs who belonged to the JDA and lived in the 3 most affected prefectures (Iwate, Miyagi, and Fukushima). Letters were sent to the same RDs in October 2012 to remind them to complete the survey. The objective of the study and the confidentiality of the data were described in the letters. Return of the questionnaire implied consent by the RDs (participants) to participate in the study.
The questionnaire was self-administered and included a total of 157 items in maximum. The questionnaire was composed of the following sections: (1) questions about the characteristics of participants, (2) questions about the recognition and usage of some tools provided by the Japanese government, (3) questions about participant’s job in their facility for each period following the disaster, (4) questions about the support activities in emergency shelters for each period following the disaster, (5) questions about the support activities in survivors’ homes for each period following the disaster, and (6) open-ended questions.
2.2. Data Analysis
Data were qualitatively and inductively analyzed through use of the qualitative descriptive analysis method. As an exploration of data organization, this analysis approach uses thematic analysis [12]. The qualitative descriptive analysis eliminates the subjectivity of the analyst and lets the data speak for itself. This analysis also encompasses everything from methods of data collection and organization to problem-solving, extending beyond the simple classification undertaken in thematic analysis.
Specifically, this method involves classifying data while identifying similarities in the dataset. After completing this initial step, the condensed meaning units were then labeled with a code, and the subcategories were created. The code is an attempt to capture the primary content or essence of an extracted segment of data [13]. A main category is a recurrent thread of underlying meaning running through codes and categories.
Participants were included in the analysis if they answered the question with the open-ended question “Please write freely about the support that you wanted at the time of the disaster.” Using qualitative descriptive analysis, we extracted the information on the support they wanted and then categorized and labeled them. Figure 1 shows the qualitative descriptive analysis procedure.
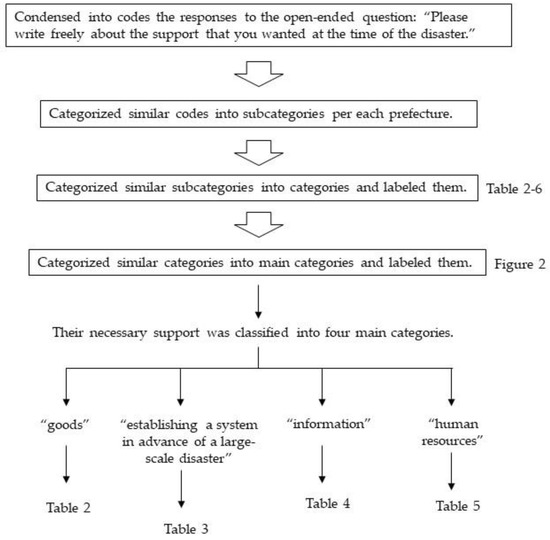
Figure 1.
Procedure for analysis by qualitative descriptive analysis.
2.3. Ethical Considerations
The present study was approved by the institutional ethics committee of the National Institute of Health and Nutrition (Current National Institutes of Biomedical Innovation, Health and Nutrition), Japan (approval number: “20120626-05”).
3. Results
Questionnaires were sent to 1911 RDs; 435 completed the questionnaire (response rate, 22.8%). Three hundred thirty-two participants (76.3%) responded to the open-ended question “Please write freely about the support that you wanted at the time of the disaster.” Table 1 shows that more females responded to the question (89.8%). The age breakdown of the respondents is as follows: 13.0% were 20–29 years, 27.1% were 30–39 years, 25.9% were 40–49 years, 24.4% were 50–59 years, 7.8% were 60–69 years, and 0.9% were 70–79 years. The highest proportion in the occupation category reported was welfare facilities (30.7%), while the second highest was hospitals (28.3%).

Table 1.
Participants’ characteristics and responses (n = 332).
The respondents’ necessary support was classified into four main categories: (1) “goods,” (2) “establishing a system in advance of a large-scale disaster,” (3) “information,” and (4) “human resources.” Figure 2 shows the main categories and categories.
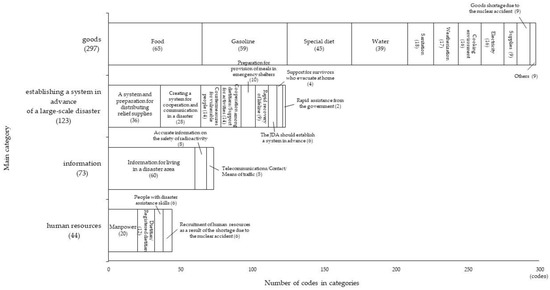
Figure 2.
Number of main categories and categories. (): Number of codes.
3.1. The Main Category: “Goods”
Table 2 shows categories delineated by the qualitative descriptive analysis within the main “goods” category, along with specific code examples and the number of codes supporting each category. Eleven categories were identified within the main category “goods”: “food” (65 codes), “gasoline” (59 codes), “special diet” (45 codes), “water” (39 codes), “sanitation” (18 codes), “weatherization” (17 codes), “cooking environment” (16 codes), “electricity” (16 codes), “supplies” (9 codes), “goods shortage due to the nuclear accident” (9 codes), and “others” (4 codes).
Table 2.
Category, subcategory, and specific code examples included in the main category “goods” (Codes total: n = 297).
The largest category was “food” (65 codes). Because the survey’s participants were RDs, many answers indicated that they desired nutrient-rich supplements difficult to acquire in emergency shelters. Code examples include “vegetables” (10 codes), “food to supplement nutrients” (5 codes), “protein source” (5 codes), etc. In addition, they requested food that could be provided in emergency shelters that did not have cooking facilities: “mass feeding for survivors” (4 codes), “cookless food” (4 codes), “canned food” (2 codes), etc.
The second largest category was “gasoline” (59 codes). Survey answers mentioned a shortage of goods due to a shortage of gasoline. Specific code examples include “Even if there were relief supplies, I had no way to go there (gasoline)” and “In order to procure foods or relief goods, it was helpful if their arrangement to get gasoline was a priority.”
The third largest category was “special diet” (45 codes). The following responses specifically touched upon this: “It was difficult to deal with forms of food other than regular meals (soft, mixed, or minced) because the machine could not be used due to blackout” and “Enteral nutrition (concentrated liquid diet) was in short supply about 1 month after the earthquake, but there was no support for it.” Additionally, there were many responses relating to survivors with special dietary needs, for example, “My 1-year old daughter has an egg allergy, so I was at a loss for her diet. I was afraid to eat the meal to be distributed and was avoiding it” and “There were few supplies that could be provided as fortified food to people with kidney disease, heart disease, liver disease, and diabetes.”
In addition, there were 17 answers regarding weather-related support because the disaster occurred in a relatively cold area and season.
3.2. The Main Category: “Establishing a System in Advance of a Large-Scale Disaster”
Table 3 shows categories delineated by the qualitative descriptive analysis within the main “establishing a system in advance of a large-scale disaster” category, along with specific code examples and the number of codes supporting each category. The nine categories delineated within the main category “establishing a system in advance of a large-scale disaster” include “A system and preparation for distributing relief supplies” (36 codes), “Creating a system for cooperation and communication in a disaster” (28 codes), “Countermeasures for vulnerable people” (14 codes), “Cooperation among dietitians/Support for activities” (14 codes), “Preparation for provision of meals in emergency shelters” (10 codes), “Rapid recovery of lifeline” (9 codes), “The JDA should establish a system in advance” (6 codes), “Support for survivors who evacuate at home” (4 codes), and “Rapid assistance from the government.”.
Table 3.
Category, subcategory, and specific code examples included in the main category “establishing a system in advance of a large-scale disaster” (Codes total: n = 123).
The subcategory “A system for distributing relief supplies in a fair and appropriate quantity and timing” received the greatest number of responses (34 codes). The category “Countermeasures for vulnerable people” included “Appropriate response to vulnerable people” (8 codes) and “A system for delivering special diet to people who need it” (6 codes). “Nursing stations or nursing room (in emergency shelters)” and “A system support survivors unable to raise their voices,” which corresponds to vulnerable people, were also mentioned under the main category “goods.” The category “Cooperation among dietitians/Support for activities” featured the following answer: “It is necessary for dietitians to create a system that is positioned similarly to other occupations.” Due to the dispatch of dietitians to the disaster area for the first time, there were also many inquiries about creating a system in which dietitians could perform as dietitians.
3.3. The Main Category: “Information”
Table 4 shows categories delineated by the qualitative descriptive analysis within the main “information” category, along with specific code examples and the number of codes supporting each category. The three categories delineated within the main category “information” are: “Information for living in a disaster area” (60 codes), “Accurate information on the safety of radioactivity” (8 codes), and “Telecommunications/Contact/Means of traffic” (5 codes).
Table 4.
Category, subcategory, and specific code examples included in the main category “information” (Codes total: n = 73).
The category “Information for living in a disaster area” offered multiple answers suggesting that people wanted the necessary information to live in a disaster area and to receive support, for example, “I was worried that information on the damage situation would not come” and “Information on the neighborhood. Opening hours of gas stations and stores. Information on the water station (I got the upper limit per person after arriving).”
3.4. The Main Category: “Human Resources”
Table 5 shows categories delineated by the qualitative descriptive analysis within the main “human resources” category, along with specific code examples and the number of codes supporting each category. Four categories were delineated within the main category “human resources”: “Manpower” (20 codes), “Dietitian/Registered dietitian” (12 codes), “People with disaster assistance skills” (6 codes), and “Recruitment of human resources as a result of shortage due to the nuclear accident” (6 codes).
Table 5.
Category, subcategory, and specific code examples included in the main category “human resources” (Codes total: n = 44).
The category “Manpower” received the most responses, with the next most frequently given being “Dietitian/Registered dietitian.” In addition, some participants responded that dietitians who were in a position to assist survivors needed a support person.
3.5. The Main Category: “Others”
Answers that could not be classified into the above four main categories were classified as “others.” Table 6 shows the specific code examples included in “others.”
Table 6.
Category, subcategory, and specific code examples included in the main category “others” (Codes total: n = 30).
4. Discussion
In order to document the necessary support for RDs in the areas affected by the earthquake, this study analyzed the written responses of dietitians to the open-ended question “Please write freely about the support that you wanted at the time of the disaster.” The responses were classified into four main categories: (1) “goods,” (2) “establishing a system in advance of a large-scale disaster,” (3) “information,” and (4) “human resources.”
4.1. The Main Category: “Goods”
Most of this category was essential to life, including “food,” “special diet,” and “water.” In the category “special diet,” many responses referred to “food for persons having difficulty in chewing/swallowing” and “concentrated liquid diet.” Oral health issues were often related to “difficulty swallowing” and “difficulty chewing” in the areas affected by the Great East Japan Earthquake [14]. One of the reasons behind these is that governments have few special food stockpiles reserved for such disasters. In the national survey of local governments, only 33.7% stated that special food stockpiles were included in their regional disaster prevention plans, guidelines, manuals, etc. [15]. The actual stockpiling rate of the local governments is even lower. Their rate was only 4.5% for the stockpiling of “food for persons having difficulty in chewing/swallowing.” This result reveals that only 19 local governments (1.5%) stockpile “food for persons having difficulty in chewing/swallowing” among all of the local governments that responded (n = 1272). It can therefore be concluded that vulnerable people should stockpile a sufficient quantity of special diet in order to protect themselves in the face of a disaster. In addition, it has been reported that prefectures that had previously been affected by disasters were likely to have food supply damage reporting systems [16]; therefore, establishing such a system might be a useful tool.
Many RDs responded concerning a need for “gasoline” (n = 59). Because the disaster areas were areas where cars were usually essential for transportation, it is thought that this shortage of “gasoline” impeded the distribution of supplies, contributing to the shortage of goods such as “food.” According to a previous report, “the large logistics companies or cooperatives often have in-tanks (small gas stations on their site), but their stockpiles are limited. They had an amount for only 2 or 3 days, and there were many cases of lack of supply. As for businesses that transport emergency relief supplies, although fuel was supplied preferentially, many businesses had difficulty securing it” [17]. In this analysis, there are also responses that “it was helpful if there were arrangements to make getting gasoline a priority,” and it was demonstrated that there was a shortage of fuel including gasoline. A previous review paper indicated that to deal with the challenges of large-scale disasters, we need to change many basic assumptions that we usually use in traditional business logistics [18]. It is necessary to make rebuilding the system that supplies the fuel a priority, especially in places where a lot of survivors depend on suppliers of goods, emergency shelters, and facilities for the elderly.
4.2. The Main Category: “Establishing a System in Advance of a Large-Scale Disaster”
This main category included “A system and preparation for distributing relief supplies” and “Creating a system for cooperation and communication in a disaster.” In fact, we reported that “simulation and system maintenance both in the dispatch of RDs and in disaster areas is essential” [11]. It is possible to perform more appropriate support activities by making an assumption at the time of the disaster and preparing the system before the disaster occurs. In this analysis, one answer suggested that “training needs to be quick-witted.” In regard to this point, the JDA established “The Japan Dietetic Association-Disaster Assistance Team (JDA-DAT)” [7]. The JDA-DAT is a nutrition assistance team that received training in the specialty of nutrition care activities in disaster areas. The purpose of this team is to promote and foster RDs equipped with the necessary technical knowledge and techniques required in order to provide swift emergency dietary assistance for a disaster-stricken region in cooperation with medical, welfare, and government nutrition specialists, etc., when a large-scale natural disaster, such as a major earthquake or typhoon, occurs.
In this main category, one affected prefecture differed from the others. Many RDs who lived in Fukushima responded concerning a need for “creating a system for cooperation and communication in a disaster.” Compared to other prefectures, Fukushima was affected by a cascading disaster that the earthquake and tsunami triggered the meltdown of the Fukushima Daiichi nuclear reactor. The suffering of the survivors was not limited to the increased physical health problems directly attributable to radiation exposure but also included psychological and social effects [19]. The prevalence of mental disorders was high overall in Fukushima survivors [20]. Many residents were also subjected to home evacuation, displacement, relocation, work/school changes, and family separation [19,21]. In addition, they had raised concerns about the safety of food and water [22]. In areas affected by large-scale cascading disasters such as Fukushima, “creating a system for cooperation and communication in a disaster” is important for solving these problems. Effective dispatch of disaster dietitians (such as the JDA-DAT) is expected.
4.3. The Main Category: “Information”
Almost all answers in this main category mentioned “information for living in a disaster area” (n = 60). It is assumed that even “information about the neighborhood” was difficult to obtain, as the blackout limited communication and the lack of gasoline made transportation difficult. It has also been reported that “communication was difficult because means of sharing information could not be secured” and “accurate information could not be transmitted fairly and managed even as time passed from the occurrence of the disaster” [17]. Facilities that were reachable by landline, mobile phone, fax, or email had favorable dietary conditions [23]. Therefore, it is important to identify successful ways to obtain information at the time of disaster before disasters happen and to have communication devices that can be used in times of disaster.
4.4. The Main Category: “Human Resources”
In this main category, the need for human resources to assist with activities such as cooking, carrying water, etc., was the highest. In fact, the number of survivors dedicated to mass feeding assistance was higher as compared to the Self-Defense Forces and volunteers during the disaster [24]. It is essential to create a quick and effective system involving the assistance of an outside team, such as the Self-Defense Forces, volunteers, and dietitians.
The next most common answer was “dietitian/registered dietitian.” The usefulness of RDs at emergency shelters has been reported [10]. Additionally, there were some answers that requested “people with disaster assistance skills.” The JDA-DAT includes human resources who have both of these skills. Although the JDA-DAT has already been dispatched in response to some disasters in Japan, it is recommended that programs continue to prepare and foster disaster dietitians in preparation for future disasters.
4.5. Limitations
One limitation of this study was that only 22.8% of the distributed questionnaires were returned. The disaster damage did not occur in the entire prefecture and affected only parts of it. Therefore, it is possible that dietitians who did not assist in the disaster area did not answer the questionnaire. However, the sample is considered to have possibly represented the Japanese RDs population because the results of previous studies targeting RDs all over Japan were similar in terms of sex ratio and occupation category to those in this study [25].
5. Conclusions
The findings suggest that a “system” is needed to ensure that “goods,” “information,” and “human resources” can easily and quickly enter a disaster area to facilitate nutritional support, specifically, (1) goods: creating a system to stock emergency supplies and deliver them where needed (a shift in assumptions that we usually use in traditional business logistics is also necessary [18]); (2) information: establishing a plan or system to obtain information at the time of disaster prior to a disaster occurring; and (3) human resources: establishing a system for dispatching volunteers and disaster dietitians (such as the JDA-DAT) in the appropriate places based on their specialties (the usefulness of RDs at emergency shelters has been reported [10]).
It is expected that each country will successfully implement the 2015 Sendai Framework for Disaster Risk Reduction (SFDRR). Our suggested systems are the result of a scientific analysis of the support actually needed in the disaster area. Therefore, establishing these systems is considered helpful for policy making to achieve disaster risk reduction in each country. In addition, it is essential to run a practical simulation prior to a disaster, making the best use of those “systems” in order to provide the support that is really needed in a large-scale disaster. Training on and practicing this system might also lead to disaster risk management. Indeed, the SFDRR have reported the following four renewed priorities: “It is important to promote regular disaster preparedness, response, and recovery exercises with a view to ensuring rapid and effective response to disasters and related displacement essential food and non-food relief supplies” [26]. Further, a systematic review reported that all four priorities for action are relevant to Disaster Risk Management [27].
It is necessary to establish a “system” to provide “goods,” “information,” and “human resources” to a disaster area in order to align practice and policy making based on the circumstances of each country in addition to scientific evidence.
Author Contributions
Conceptualization, K.I.-T. and N.T.-K.; methodology, N.T.-K.; software, M.H.; validation, N.T.-K.; formal analysis, M.H.; investigation, N.T.-K.; resources, N.T.-K.; data curation, N.T.-K.; writing—original draft preparation, M.H.; writing—review and editing, N.T.-K.; visualization, M.H.; supervision, K.I.-T. and N.T.-K.; project administration, N.T.-K.; and funding acquisition, N.T.-K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by JSPS KAKENHI “Grant Number JP15K00868” and by The Japanese Society of Nutrition and Dietetics Research Grant: Research on support of nutrition improvement activities after the Great East Japan Earthquake.
Acknowledgments
We wish to thank all respondents for their participation as well as the Japan Dietetic Association (JDA). We are indebted to Jun Oka and Akana Motomura from Tokyo Kasei University for their support regarding data analysis.
Conflicts of Interest
The authors declare no conflict of interest.
References
- AghaKouchak, A.; Huning, L.S.; Chiang, F.; Sadegh, M.; Vahedifard, F.; Mazdiyasni, O.; Moftakhari, H.; Mallakpour, I. How do natural hazards cascade to cause disasters? Nature 2018, 561, 458–460. [Google Scholar] [CrossRef] [PubMed]
- Hirai, K.; Okuda, T.; Masuda, T.; Yamaguchi, H.; Tsuzukida, Y.; Takao, F. Food Intake and Diet Considerations among Victims Living in Evacuation Centers after the Great Hanshin-Awaji Earthquake. J. Integr. Study Diet. Habits 1998, 9, 28–35. (In Japanese) [Google Scholar] [CrossRef]
- Tsuchida, N.; Isobe, S.; Watanabe, S.; Ishigami, K.; Yoshita, K.; Yoshiike, N.; Murayama, N. Changes in Access to Food and the Frequency of Food Consumption before and after the Niigata Chuetsu Earthquake: Comparison between Households in Temporary Housing and Disaster-stricken Housing. J. Jpn. Diet. Assoc. 2010, 53, 340–348. (In Japanese) [Google Scholar]
- Tsuboyama-Kasaoka, N.; Hoshi, Y.; Onodera, K.; Mizuno, S.; Sako, K. What factors were important for dietary improvement in emergency shelters after the Great East Japan Earthquake? Asia Pac. J. Clin. Nutr. 2014, 23, 159–166. [Google Scholar]
- Fire and Disaster Management Agency. Available online: https://www.fdma.go.jp/disaster/higashinihon/items/159.pdf (accessed on 24 March 2020). (In Japanese).
- Harada, M.; Tsuboyama-Kasaoka, N.; Takizawa, A.; Hidemi, T.; Oka, J. Improving Nutrient Balance by Providing Main and Side Dishes in Emergency Shelters after the Great East Japan Earthquake. J. J. Disast. Med. 2017, 22, 17–23. (In Japanese) [Google Scholar]
- Tsuboyama-Kasaoka, N.; Purba, M.B. Nutrition and earthquakes: Experience and recommendations. Asia Pac. J. Clin. Nutr. 2014, 23, 505–513. [Google Scholar]
- Ito, S.; Sudo, N.; Tsuboyama-Kasaoka, N.; Okazaki, N.; Nabeshima, K.; Kanatani, Y.; Okumura, T.; Shimoura, Y. An Analysis of Support Activities by Registered Dietitians and Dietitians Dispatched by the Japan Dietetic Association after the Great East Japan Earthquake. J. Jpn. Diet. Assoc. 2015, 58, 111–120. (In Japanese) [Google Scholar]
- Hamaguchi, H.; Sudo, N.; Tsuboyama-Kasaoka, N.; Kanatani, Y.; Shimoura, Y. Analysis of “what I thought today” reported by dietitians dispatched by the Japan Dietetic Association to the affected areas by the Great East Japan Earthquake. J. Jpn. Diet. Assoc. 2015, 58, 35–44. (In Japanese) [Google Scholar]
- Harada, M.; Takizawa, A.; Oka, J.; Tsuboyama-Kasaoka, N. The effects of changes in the meal providing system on emergency shelter menus following the Great East Japan Earthquake. Nihon Koshu Eisei Zasshi 2017, 64, 547–555. (In Japanese) [Google Scholar]
- Tsuboyama-Kasaoka, N.; Hirono, R.; Ishikawa-Takata, K.; Takizawa, A.; Sudo, N.; Shimoura, Y.; Sako, K. Analysis of the Effective or Problematic Points of Nutrition Support Activities by Dietitians Dispatched to Areas Affected by the Great East Japan Earthquake. J. Jpn. Disaster Food Soc. 2016, 3, 19–24. (In Japanese) [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Saldana, J. The Coding Manual for Qualitative Researchers, 2nd ed.; SAGE Publications: London, UK, 2014; pp. 4–16. [Google Scholar]
- Tsuboyama-Kasaoka, N.; Kondo, A.; Harada, M.; Ueda, S.; Sudo, N.; Kanatani, Y.; Shimoura, Y.; Nakakuki, K. Analysis of an Oral Health Report from Dietitians Dispatched to the Areas Affected by the Great East Japan Earthquake. Jpn. J. Dysphagia. Rehabil. 2017, 21, 191–199. (In Japanese) [Google Scholar]
- Yamada, K.; Sudo, N.; Tsuboyama-Kasaoka, N.; Yamamura, K.; Yamashita, M.; Yamamoto, M.; Shimoura, Y.; Komatsu, T. Nationwide survey on local governments’ current preparedness for food and nutrition assistance during natural disasters: Regional disaster prevention plan and stockpiles. J. Jpn. Diet. Assoc. 2015, 58, 517–526. (In Japanese) [Google Scholar]
- Sudo, N.; Urakawa, M.; Tsuboyama-Kasaoka, N.; Yamada, K.; Shimoura, Y.; Yoshiike, N. Local Governments’ Disaster Emergency Communication and Information Collection for Nutrition Assistance. Int. J. Environ. Res. Public Health. 2019, 16, 4617. [Google Scholar] [CrossRef] [PubMed]
- Yano, Y. Logistics for Disaster Relief Supply. RKU Logist. Rev. 2011, 56, 11–15. (In Japanese) [Google Scholar]
- Jiang, Y.; Yuan, Y. Emergency Logistics in a Large-Scale Disaster Context: Achievements and Challenges. Int. J. Environ. Res. Public Health. 2019, 16, 779. [Google Scholar] [CrossRef]
- Hasegawa, A.; Tanigawa, K.; Ohtsuru, A.; Yabe, H.; Maeda, M.; Shigemura, J.; Ohira, T.; Tominaga, T.; Akashi, M.; Hirohashi, N.; et al. Health effects of radiation and other health problems in the aftermath of nuclear accidents, with an emphasis on Fukushima. Lancet 2015, 386, 479–488. [Google Scholar] [CrossRef]
- Shigemura, J.; Terayama, T.; Kurosawa, M.; Kobayashi, Y.; Toda, H.; Nagamine, M.; Yoshino, A. Mental health consequences for survivors of the 2011 Fukushima nuclear disaster: A systematic review. Part 1: Psychological Consequences. CNS Spectr. 2020, 20, 1–16. [Google Scholar]
- Yoshioka-Maeda, K.; Kuroda, M.; Togari, T. Difficulties of fathers whose families evacuated voluntarily after the Fukushima nuclear disaster. Nurs. Health. Sci. 2018, 20, 296–303. [Google Scholar] [CrossRef]
- Hamada, N.; Ogino, H. Food safety regulations: What we learned from the Fukushima nuclear accident. J. Environ. Radioact. 2012, 111, 83–99. [Google Scholar] [CrossRef]
- Nozue, M.; Ishikawa-Takata, K.; Sarukura, N.; Sako, K.; Tsuboyama-Kasaoka, N. Stockpiles and food availability in feeding facilities after the Great East Japan Earthquake. Asia Pac. J. Clin. Nutr. 2014, 23, 321–330. [Google Scholar] [PubMed]
- Tsuboyama-Kasaoka, N.; Harada, M. Analysis of Mass Feeding for Evacuees in Emergency Shelters after the Great East Japan Earthquake: Outside Support from Self-defense Forces, Volunteers, and Dietitians. J. Jpn. Disaster Food Soc. 2017, 5, 1–5. (In Japanese) [Google Scholar]
- Toh, N. State of current status and issues for visiting nutritional guidance for home-bound patients: The internet based attitude survey of nutritional counselling for home-bound patient by 450 dieticians and management dieticians. J. Integr. Study Diet. Habits 2017, 28, 159–168. (In Japanese) [Google Scholar] [CrossRef][Green Version]
- UNISDR (United Nations International Strategy for Disaster Reduction). Sendai Framework for Disaster Risk Reduction 2015–2030. 2015. Available online: https://www.preventionweb.net/files/43291_sendaiframeworkfordrren.pdf (accessed on 6 May 2020).
- Surianto, S.; Alim, S.; Nindrea, R.D.; Trisnantoro, L. Regional Policy for Disaster Risk Management in Developing Countries Within the Sendai Framework: A Systematic Review. Open Access Maced. J. Med Sci. 2019, 7, 2213–2219. [Google Scholar] [CrossRef] [PubMed]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).