Abstract
Performance in the supine-to-stand (STS) task is an important functional and health marker throughout life, but the evaluation methods and some correlates can impact it. This article aims to examine the studies that assessed the performance of the STS task of young people, adults and the elderly. Evidence of the association between the STS task and body weight status, musculoskeletal fitness and physical activity was investigated, and a general protocol was proposed. MEDLINE/Pubmed and Web of Science databases were accessed for searching studies measuring the STS task directly; identification, objective, design, sample, protocols and results data were extracted; the risk of bias was assessed (PROSPERO CRD42017055693). From 13,155 studies, 37 were included, and all demonstrated a low to moderate risk of bias. The STS task was applied in all world, but the protocols varied across studies, and they lacked detail; robust evidence demonstrating the association between STS task and musculoskeletal fitness was found; there was limited research examining body weight status, physical activity and the STS task performance. In conclusion, the STS task seems to be a universal tool to track motor functional competence and musculoskeletal fitness throughout life for clinical or research purposes.
1. Introduction
The human development lifespan perspective provides a framework for studying the changes that occur throughout life [1,2]. Within this perspective, some motor actions are considered developmental milestones and health indicators as the action “rising from a supine position on the floor to an erect standing position” (supine-to-stand, STS), since it is an indicative of bipedal readiness for upright locomotion in children [3] and functional capacity for independence in the elderly [4].
The STS task performance also uncovers an individual’s level of motor competence (MC), defined as the proficiency in motor actions performed with coordination and control [5,6,7]. The STS task requires complex coordination of large muscle groups of the trunk and extremities, while controlling their center of mass in dynamic balance during elevation and stabilizing body alignment during the erect posture [8].
During the 1980s, Ann Vansant proposed developmental sequences for this righting task [1,3,9]. Studies related it to physical fitness and lifestyle variables [10,11,12] expanding the focus of motor development per se, to the discussion concerning their relationship with health [6,7]. STS has been investigated at different stages of life [4,8,12,13,14], and unlike other motor skills, such as running or jumping, instruction on how to rise from supine is not taught, which reduces the bias of cultural context or structured practice opportunities. Furthermore, the STS task seems to be a useful marker of health and function problems, predicting serious fall-related injuries [15,16,17].
With these characteristics, maybe the STS task is a useful and practical method to monitor functional MC changes throughout human life and an excellent candidate to be a universal screening tool. However, such assumptions need further examination. For example, health variables as physical activity, musculoskeletal fitness, and body status weight should be considered when evaluating the STS task [14].
Assessing the performance of the STS task or other motor action may involve two different measurement approaches: process and product-oriented. A process-oriented measurement aims to express the quality of the movement, in general, by comparing it with the more successfully mechanical form, as described in the checklists. A product-oriented measurement aims to describe the action results, such as the time to complete a task or the scores on a target, using interval or discrete variables (e.g., seconds, points, speed). Both approaches, complementary, expresses human motor performance [18,19]. Studies using a product-oriented approach measured the STS time by chronometers [20], photoelectric cells [4], or a video [8,12,14,21,22,23,24]. STS process-oriented measurements often uses video recordings, to check the postures [23] or motion sequences [9,10]. Such protocols do not always control procedures as verbal instructions or the number of trials. All of these differences lead to non-standardized performance reporting. As far as we know, there are no studies that have established a full protocol for assessment of the STS task for all ages.
According to PICO strategy, the research problem presented in this study asked if, in typical development individuals (P), the assessment of the STS task performance (I) used in different developmental phases (C) can monitor healthy functional MC changes (O). In this context, the main objective was systematically reviewing the supine-to-stand task assessment methods and the health variables related to this task in youth, adults, and older adults. Specifically, it was examined: [1] The methods used to investigate the STS task, including the risk of bias, and the results, [2] the evidence of an association between the performance of the STS task and the health-related variables body weight status, musculoskeletal fitness, and physical activity. Finally, as a by-product of this review, a protocol for STS task measurement, which is testable across the lifespan, was proposed.
2. Materials and Methods
The present review included studies of the several designs (observational, interventional, cross-sectional, longitudinal), so it can be better classified as a mixed-methods review [25]. This study is registered in PROSPERO (#CRD42017055693) and followed protocols for systematic reviews PRISMA-P [26].
2.1. Data Sources and Searches Descriptors
In this review, studies with healthy individuals in the phases of childhood, adolescence, adulthood, and senescence whose performance on the STS task had been assessed through objective measures, but not questionnaires, were searched. The databases were directedly accessed (MEDLINE, Scielo, EMBASE, Scopus, ERIC/ProQuest), and also it was used some search device (PubMed, Web of Science—Main Collection, Science Direct, EBSCO, Cochrane). Subsequently, the search involved gray literature, through the review of the reference lists (only of the included articles, see below) and consultation with specialists in the area. Intragroup descriptors were combined using the Boolean expression OR, whereas between-group descriptors were combined using AND (Figure 1). Inclusion criteria were: (1) Original studies (articles, theses, dissertations) assessing the STS task by using objective measures, (2) English language, (3) healthy/typical development individuals. Exclusion criteria were: (1) Duplicates, (2) not match with the background of this review, (3) not typical individuals, (4) articles not available in full text. There were no restrictions on the year of publication.
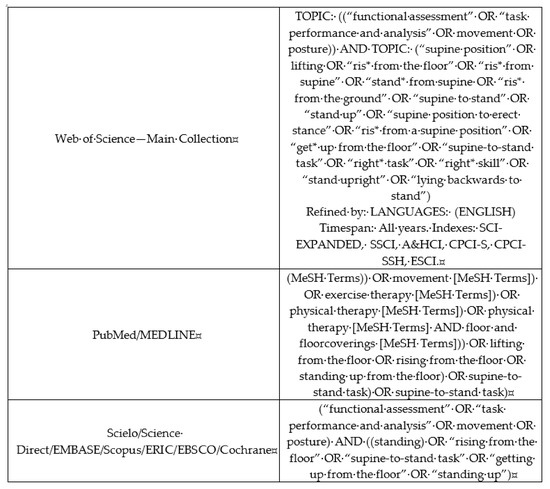
Figure 1.
Descriptors used in the systematic review about the supine-to-stand (STS) task performance, according to research tools in the databases. The figure was originally created by the authors.
2.2. Study Selection
One author (MTC) conducted the identification of the studies, and added it to Rayyan QCRI, a web application for systematic reviews [27]. In this environment, the duplicates were removed by MTC. Before initiating the screening process, MTC and FSS performed an exhaustive training to include articles until they reached a concordance of the 92%; then, these two authors reviewed the list of titles for applying the inclusion criteria. So, the authors compared the results and discussed the discrepancies until they reach a consensus. If there was no consensus about a title, a third researcher resolved the disagreement (MPS). Such a process was repeated, reviewing abstracts and full texts, again applying the inclusion criteria. The identification of articles in the list of references and consultation with specialists supplemented the search strategy, added to the Rayyan application.
2.3. Data Extraction and Methodological Quality Assessment (Risk of Bias)
There was the extraction of the following data: Identification (author, year, and country of publication); objective, design, sample characteristics; STS outcome (process or product-oriented); results/conclusion strictly related to the STS task (Table 1). The number of trials, instruction for performance pace, participant’s caring, and motivational strategies from the protocols’ studies were also extracted (Table 2).

Table 1.
Methodological characteristics, main results, and conclusions from studies on STS task (ordered by developmental phase and year of publication). The table was originally created by the authors.
Table 2.
Absolute and relative frequencies of the protocols’ characteristics of studies reviewed about the Supine-to-Stand (STS) task (n = 37).
The quality of each article (risk of bias) was examined by 15 questions adapted from Law [28], and the scoring was as follows: 0 = does not meet criteria; 1 = satisfies the criteria; ? = not clearly described; NA = not applicable. In the classification, a study with score ≤ 7 = high risk of bias/low quality; studies that reached 8 to 11 points = moderate risk of bias/medium quality; scores ≥ 12 = low risk of bias/high quality (Supplementary material Table S1). Two researchers conducted these data extraction (MTC and FSS), and when there was no consensus, another researcher (ABD) resolved the disagreement.
The data were summarized in tables, and a narrative synthesis was done. Lastly, a full protocol was developed from the critical knowledge generated here. Some authors in this review worked in the clinical setting, and others are specialists in movement analysis, both in children and in the elderly. Then, the theoretical background and practical experience contributed to the presentation of this final protocol (Appendix A, Box A1).
3. Results
In this review, from of 13,155 studies found, 37 articles were included (Figure 2) [8,11,12,14,15,16,17,20,21,22,23,24,29,30,31,32,33,34,35]. The studies investigated subjects ranging in age from 1 to 94 years; the largest proportion of studies investigated up to 100 subjects [11,14,17,31,36,37,38,39,40], and one of them [41] examined a very large sample with 2368 subjects; more than a third of them used both process and product-oriented measurements (Table 1); only one study combined these two approaches creating a full score (MOD score) [40].
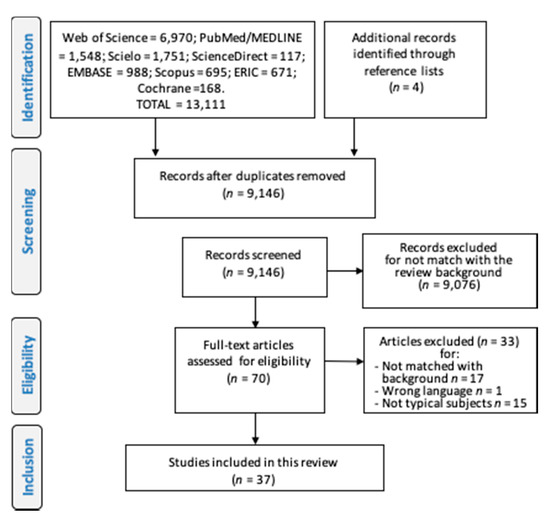
Figure 2.
Flowchart describing the process to include studies in the systematic review according to the PRISMA-P protocol. The figure was originally created by the authors.
Just four studies reported the verbal instructions on starting position, which included legs extended and arms extended to the side of the trunk [14,31,36,40] five studies reported the final position as stable standing upright with both feet on the ground [23,24,31,38,40]. Nesbitt et al. [8] used final position goal combined with touching a designated point on the wall; Alexander et al. [4] asked the subjects to press a switch placed on a tripod when assuming the standing position, marking the end of the task. Other protocols’ characteristics were summarized in Table 2.
None of the studies that investigated the STS task were classified as high risk of bias. However, the item most frequently absent in assessing the risk of bias was “Was the justification for the sample size?”, with only 18.9% of studies presenting such a justification (for detailed information, see Supplementary Material Table S1).
The STS Task Performance and Body Weight Status, Musculoskeletal Fitness and Physical Activity
By investigating young children, Ng et al. [31] and Nesbit et al. [12] did not find an association between STS time and BMI; by investigating older children, Duncan et al. [11] found a moderate inverse correlation (r = −0.508). Naugle et al. [37] investigated older adults and found that each unit of BMI was associated with an increase in the severity of compensatory strategies to rise; also investigating older people, Manckoundia et al. [38] found that being overweight was associated with fails to perform STS (not able to rise); Henwood and Taaffe [47] investigated the effect of a fitness program in seniors and found a positive effect on STS time. Belt et al. [42] investigated people from ages 7 to 36 years with Prader-Willi syndrome and typical controls, and regardless of diagnosis, they found a very poor correlation between STS task process measurement and BMI, but there were not confirmed relationships between BMI and any of the three body region scores. However, some cautions are need because BMI at different ages is related to various components of body composition.
Four studies investigated the relationship between STS task performance and musculoskeletal fitness, which showed a direct relationship [23,32,33,39]. One investigated children by testing grip and trunk muscle strength [32]; lower limb power of the older people were investigated [23,33,37,39], as well as flexibility [23] and upper limb strength [39]. One study [20] investigated a musculoskeletal training intervention on STS time performance in seniors that showed a positive effect.
Two studies examined the association between STS task performance with physical activity [14,39]. Green and Williams [14] investigated 72 middle-age adults and noted that the most active adults used more advanced STS task patterns than those who were rarely active, but they did not perform an inferential test. Klima et al. [39] investigated older adults and found an inverse correlation between STS task time and physical activity level (rho = −0.29).
4. Discussion
In this present review, the methods used in the STS assessment were summarized and critically examined. Furthermore, this review verified the association of STS task performance with select health variables. The results showed that the STS task performance was investigated throughout the life cycle, in various countries, and several studies used large samples [3,12,15,16,17,31,36,37,38]. In general, these results suggest the STS task can be considered a functional health assessment, from youth to old age.
However, the measurement type can be a critical issue. For example, by using a dichotomous variable (to be able or not gets up from the floor), Bergland et al. [15,16,17] investigated seniors (over 75 years) and concluded that the STS task is a valid marker of health and function problems, as well as a significant predictor of falls-related severe injuries in this life phase. One’s ability to stand up is a validated measure; however [15], it does not reveal the phenomenon of functional MC throughout life, since it seems to have been very suitable for use in the sample of older subjects, but it must have a ceiling effect at younger ones.
Both process and product-oriented measurements were used in a similar proportion in the literature. Process-oriented measurement identifies the difficulties in the task but demands much time to code and seems to be more valuable to propose intervention, mainly in older adults. Alternatively, product-oriented measurement, as movement time, maybe more related to functional outcomes. Facing a challenge, such as standing up as fast as possible, and relating this outcome to functional capabilities, like muscular strength and endurance, speaks to the ability to solve a functional motor task in various ways and at various speeds. This task speaks to the importance of being able to vary the execution of STS based on specific task demands. Thus, STS time is a resourceful way to operationalize functional MC, mainly with large samples or studies with many variables, as it requires limited technological resources and provides better discrimination and sensitivity in measurement than process-oriented assessments.
4.1. Risk of Bias and Procedure Protocols
Since all studies showed a moderate or low risk of bias, the internal validity was considered satisfactory. The more comprehensive analysis of the STS protocols showed a wide variety of procedures, which can be a severe problem if one proposes to have one protocol to be used for all the developmental levels. The instruction on the mechanics of the movement can facilitate performance [34,35] so for an understanding of how people typically get off the ground, controlling the instructions is critical to STS assessment. All studies instructed subjects individually, and most of them relied on verbal information rather than demonstration; some researchers even explicitly prevented any visual demonstration or explanation of the STS mechanics [11]. In summary, it was clear that researchers avoided any modeling or verbal instruction bias to examine the movement patterns typically used by participants.
Also, the time constraint instruction needs to be highlighted, since maximum speed instruction can affect the automaticity of the movements (i.e., minimizing the conscious analysis of the motor action) [53]. An external focus of attention (i.e., time restriction) organizes the motor system according to individual constraints and choice, rather than when the focus of attention is internal (i.e., on a movement pattern), which can interfere with the automatic process control as explained by the “constrained-action hypothesis” [35,53]. Depending on the measurement intents, a researcher can choose whether to impose a time constraint. For instance, to examine a general STS movement process that individuals would use in everyday life, a time constraint would not be necessary. Alternatively, to examine functional capacity as it relates to a “best” or “maximal” performance, a time constraint may be the most appropriate option. The time factor may be a more salient choice to predict health outcomes as the ability to produce power has strong implications for all-cause mortality and functional independence in older adults [54], as well as fitness, physical activity, and weight status in youth and young adults [5,55,56].
The final position of the task is another critical element related to the instructions. Two studies combined the goal of postural alignment with an external target [4,12]. This seems to be an efficient methodological strategy, since the performer has a simple and easy-to-execute external goal (touching the point in front of him/her), and in turn, the evaluators’ job is facilitated to stop the chronometer or video frame. However, understanding whether providing a final position with an additional reaching task might alter how an individual stand needs to be addressed.
Regarding feedback and rewards, three studies detailed the procedures given to motivate children by using verbal reinforcement during or after the task execution, using praise or words highlighting their efforts [3,12,24]. Motivational feedback was used only with early childhood children, since the motivational climate can dramatically affect preschoolers’ performance [55]. Encouraging may be highly beneficial if the time task constraint is “maximum” (i.e., shortest time) [40].
The number of repetitions varied widely among the studies. This lack of uniformity weakens the findings as a high number of repetitions without adequate rest can cause fatigue, adversely affecting motor performance. It seems to be the case with older or frail individuals that demonstrate limited physical function and fitness. Conversely, only one trial may not represent typical behavior. When addressing the movement process, two to five trials would be necessary to gain insight into an individual’s most probable movement process.
4.2. STS Performance and Body Weight Status, Musculoskeletal Fitness, and Physical Activity
Seven studies examined the body weight status and the STS task performance, and three of them demonstrating significant associations. It seems reasonable to expect that weight status, specifically with increased adipose tissue, is associated with STS performance. In overweight or obese individuals, the motor system has to overcome higher inertia to accelerate the body mass against the force of gravity to attain an upright position. Individuals can accomplish these using variable body actions that may not require high power outputs. Rather, maximizing postural alignments that minimize the demand for high muscle activity levels (i.e., manipulation of multiple degrees of freedom with minimum energy expenditure) would be a favorable strategy for individuals who demonstrate low muscular power/strength and endurance. However, while these strategies may be useful for minimizing energy expenditure, they may increase the time to stand. This potential trade-off may also speak to the variability in individuals’ MC. If individuals demonstrate higher MC levels, they may be able to stand using different coordination patterns regardless of energy used (i.e., level of neuromuscular demand or segmental coordination patterns), as demonstrated in Didier’s study [43]. However, individuals with low levels of overall MC may be more restricted in their movement patterns, due to a lack of muscular strength or coordinative capabilities across multiple joints. It is possible to think that the bodyweight status is a good candidate to be a moderator variable to the STS task performance, playing a role integrated with other fitness variables. More scientific pieces of evidence are necessary on this topic.
This review has confirmed there is a positive association between the STS task performance and musculoskeletal fitness for all ages, confirming previous literature results [5,6,55]. Therefore, it seems the STS is a good candidate to be a musculoskeletal health indicator in all cycle life.
The association between STS task performance and physical activity was examined in only two studies [14,39]. Even though the results had agreed with each other, and both studies have shown a low risk of bias, they have used different approaches, and one of them [14] did not report inferential associations. Thus, it seems too early to state that there is evidence of a direct association between physical activity and STS task performance. A previous study [56] has supported the notion of reciprocal action between the physical activity and MC, and perhaps it was the case of thinking more about how they enhance each other than just the simple relationship between them.
4.3. Clinical Applications
Hofmeyer et al. [20] carried out the only study that tested training for getting off the ground: Their results showed an improvement in the experimental group performance compared to the controls. This study reinforces that the STS task also has interventional value to health professionals. By taking all results of this review, one can generally state that STS is a potentially useful tool to examine functional MC and a general health status marker, as well as a useful approach to clinicians and researchers. It is notable in the present review that the STS task was investigated in the stages of childhood, adulthood, and old age. These results allow us to recognize that this is a task that is appropriate to play at all ages; in particular, a measure of the STS time has shown to have sufficient variability to distinguish individuals in all ages, without having a ceiling or floor effects.
The upright posture enables the subject to dominate his environment, and righting behaviors is an expression of physical independence [1]. Also, achieving such an upright posture in the shortest possible time, challenging individual constraints (e.g., unfavorable weight status), is a clear expression of human motor competence, i.e., the ability to solve motor problems in the face of challenging demands from the environment or of the subject itself. However, more evidence across the lifespan is needed to demonstrate these linkages.
Even the results of this review allow affirming that the STS task has a strong potential to uncover MC at any phase of life, the studies used diversified protocols and methodological strategies along with what prevented comparison and the generalization of findings. So, as a by-product of this review, a unique and universal protocol is proposed (Appendix A). We also understand that we are in agreement with contemporary literature on this subject. A very recent article [52] researched the same task with minor differences, showing its importance for older adults and investigating its clinimetric properties. We reinforce and extend the results of this study because we proposed that this task can be tested for all ages.
4.4. Study Strengths and Limitations
The strength of this study was that it examined all STS literature across the lifespan, and disentangled the various methods used to assess this task in several countries. It is plausible to present STS as a good candidate for a valid and non-culturally biased measure of functional MC across the lifespan. It is also advantageous to have a unique protocol that can be applied across all ages to facilitate tracking motor competence over time. The limitations of this study were that only studies in English were reviewed. Moreover, since the objective of this study was only to review methods, other studies should be carried out to establish typical values and significant cutoff points for the STS task performance.
5. Conclusions
This review showed that the STS task was tested at all ages, in various parts of the world, confirming it as a useful tool to track functional motor competence throughout life, in a universal way. In particular, measuring the time of the STS task is an ingenious way to operationalize functional motor competence mainly in large-scale studies. In addition, as it was found that the STS task has a strong relationship with musculoskeletal fitness over the years, it can help to monitor this health variable throughout life. It is not yet possible to recognize a factual relationship between the performance of the STS task and health variables, such as body weight status and physical activity.
Supplementary Materials
The following are available online at https://www.mdpi.com/1660-4601/17/16/5794/s1, Table S1 Risk of bias within articles included in the review regarding the performance of the supine-to-stand (STS) task.
Author Contributions
Conceptualization, M.T.C., F.S.d.S. and M.P.S.; methodology, M.T.C., F.S.d.S. and M.P.S.; formal analysis, M.T.C. and F.S.d.S.; investigation, M.T.C. and F.S.d.S.; resources, M.P.S., data curation, M.T.C.; writing—original draft preparation, M.T.C. and F.S.d.S.; writing—review and editing M.P.S., A.H.N.R., D.R.N., A.B.D.S., A.H.P.F. and D.F.S.; visualization, A.H.N.R., D.R.N., A.B.D.S., A.H.P.F. and D.F.S.; supervision, D.F.S.; project administration, M.T.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Box A1. Supine-To-Stand (STS) task measure protocol for all ages.
Objective: To get up as fast as possible from the floor.
Place and procedures
1. Quiet room with a clean and flat floor;
2. Floor marks. With a contrasting colored adhesive tape mark on the floor a perpendicular distance equal to the participant’s arm length to the wall; this distance cannot be less than 30 cm, approximately the same distance of the semi-extend arms to the wall, in order to be a comfortable space to the participant rising him/herself.
3. Mark a dot on the wall. The placement of the target on the wall must match with the height of the subject’s gaze.
4. Initial position: Lie flat (dorsal decubitus position) on the ground with hands in a prone position;
5. Final position: Upright orthostatic position touching a fixed target on the wall.
General recommendations
- ✓
- The participant’s feet must be bare, and it is suggested that participants wear light clothes, suitable for exercise;
- ✓
- The subject makes a trail test in order to train before performing valid attempts.
- ✓
- All commands given to participants must be communicated with kindness and firmness;
- ✓
- Do not give any feedback to participants between tests;
- ✓
- Do not give any visual instructions;
- ✓
- Repeat a minimum of three times and more if needed to address process-oriented mode sequences; the best performance (lowest movement time) is the primary measure for the analyses;
- ✓
- The interval between trials must last for as long as it takes for the participant to reposition himself/herself on the floor. It is not a problem if the participant takes more time between one attempt and another to return to the initial position: Individual comfort should be maintained;
- ✓
- In the case of elderly participants, at least one assistant must be behind the performer to provide any help during the action of rising from the ground.
References
- VanSant, A.F. Life-span development in functional tasks. Phys. Ther. 1990, 70, 788–798. [Google Scholar] [CrossRef] [PubMed]
- Leversen, J.S.R.; Haga, M.; Sigmundsson, H. From children to adults: Motor performance across the life-span. PLoS ONE 2012, 7, e38830. [Google Scholar] [CrossRef] [PubMed]
- VanSant, A.F. Age Differences in Movement Patterns Used by Children to Rise from a Supine Position to Erect Stance. Phys. Ther. 1988, 68, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Alexander, N.B.; Ulbrich, J.; Raheja, A.; Channer, D. Rising from the floor in older adults. J. Am. Geriatr. Soc. 1997, 45, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Cattuzzo, M.T.; dos Santos Henrique, R.; Ré, A.H.N.; de Oliveira, I.S.; Melo, B.M.; de Sousa Moura, M.; de Araújo, R.C.; Stodden, D. Motor competence and health related physical fitness in youth: A systematic review. J. Sci. Med. Sport 2016, 19, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.E.; Stodden, D.F.; Barnett, L.M.; Lopes, V.P.; Logan, S.W.; Rodrigues, L.P.; D’Hondt, E. Motor Competence and its Effect on Positive Developmental Trajectories of Health. Sport. Med. 2015, 45, 1273–1284. [Google Scholar] [CrossRef]
- Stodden, D.F.; Langendorfer, S.J.; Goodway, J.D.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A developmental perspective on the role of motor skill competence in physical activity: An emergent relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Nesbitt, D.; Molina, S.L.; Sacko, R.; Robinson, L.E.; Brian, A.; Stodden, D. Examining the Feasibility of Supine-to-Stand as a Measure of Functional Motor Competence. J. Mot. Learn. Dev. 2018, 6, 267–286. [Google Scholar] [CrossRef]
- VanSant, A.F. Rising from a supine position to erect stance. Description of adult movement and a developmental hypothesis. Phys. Ther. 1988, 62, 185–192. [Google Scholar]
- Duncan, M.J.; Lawson, C.; Walker, L.J.; Stodden, D.; Eyre, E.L.J. The Utility of the Supine-to-Stand Test as a Measure of Functional Motor Competence in Children Aged 5-9 Years. Sports 2017, 5, 67. [Google Scholar] [CrossRef]
- Nesbitt, D.; Molina, S.L.; Cattuzzo, M.T.; Robinson, L.E.; Phillips, D.; Stodden, D. Assessment of a Supine-to-Stand (STS) Task in Early Childhood: A Measure of Functional Motor Competence. J. Mot. Learn. Dev. 2017, 5, 252–266. [Google Scholar] [CrossRef]
- Marsala, G.; VanSant, A.F. Age-related differences in movement patterns used by toddlers to rise from a suppine position to erect stance. Phys. Ther. 1998, 78, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Green, L.N.; Williams, K. Differences in developmental movement patterns used by active versus sedentary middle-aged adults coming from a supine position to erect stance. Phys. Ther. 1992, 8, 560–568. [Google Scholar] [CrossRef]
- Bergland, A.; Jarnlo, G.B.; Laake, K. Validity of an index of self-reported walking for balance and falls in elderly women. Adv. Physiother. 2002, 4, 65–73. [Google Scholar] [CrossRef]
- Bergland, A.; Wyller, T.B. Risk factors for serious fall related injury in elderly women living at home. Inj. Prev. 2004, 10, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Bergland, A.; Laake, K. Concurrent and predictive validity of “getting up from lying on the floor”. Aging Clin. Exp. Res. 2005, 17, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Hands, B.P.; Hands, B. How Can We Best Measure Fundamental Movement Skills? Paper presented at the Australian Council for Health, Physical Education and Recreation Inc. (ACHPER) 23rd Biennial National/International Conference: Interactive Health & Physical Education, Launceston, TAS, Australia, 3–5 July 2002. [Google Scholar]
- Burton, A.W.; Miller, D.E. Movement Skill Assessment; Human Kinectis: Champaign, IL, USA, 1998. [Google Scholar]
- Hofmeyer, M.R.; Alexander, N.B.; Nyquist, L.V.; Medell, J.L.; Koreishi, A. Floor-rise strategy training in older adults. J. Am. Geriatr. Soc. 2002, 50, 1702–1706. [Google Scholar] [CrossRef] [PubMed]
- Hsue, B.J.; Chen, Y.J.; Wang, Y.E. The intra- and inter-rater reliability of component analysis of rise from supine in the children with typical development and developmental delay. Res. Dev. Disabil. 2014, 35, 162–170. [Google Scholar] [CrossRef]
- Hsue, B.J.; Wang, Y.E.; Chen, Y.J. The movement patterns used to rise from a supine position by children with developmental delay and age-related differences in these. Res. Dev. Disabil. 2014, 35, 2205–2214. [Google Scholar] [CrossRef]
- Schwickert, L.; Oberle, C.; Becker, C.; Lindemann, U.; Klenk, J.; Schwenk, M.; Bourke, A.; Zijlstra, W. Model development to study strategies of younger and older adults getting up from the floor. Aging Clin. Exp. Res. 2016, 28, 277–287. [Google Scholar] [CrossRef]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Info. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Stewart, D.; Letts, L.; Pollock, N.; Bosch, J.; Westmorland, M. Guidelines for Critical Review of Qualitative Studies; McMaster University Occupational Therapy Evidence-Based Practice Research Group: Hamilton, ON, Canada, 1998. [Google Scholar]
- Mewasingh, L.D.; Demil, A.; Christiaens, F.J.C.; Missa, A.M.; Cheron, G.; Dan, B. Motor strategies in standing up in leukomalacic spastic diplegia. Brain Dev. 2002, 24, 291–295. [Google Scholar] [CrossRef]
- Mewasingh, L.D.; Sékhara, T.; Pelc, K.; Missa, A.M.; Cheron, G.; Dan, B. Motor strategies in standing up in children with hemiplegia. Pediatr. Neurol. 2004, 30, 257–261. [Google Scholar] [CrossRef]
- Ng, J.; Conaway, M.R.; Rigby, A.S.; Priestman, A.; Baxter, P.S. Methods of standing from supine and percentiles for time to stand and to run 10 m in young children. J. Pediatr. 2013, 162, 552–556. [Google Scholar] [CrossRef]
- Kuwabara, C.; Shiba, Y.; Sakamoto, M.; Sato, H. The Relationship between the Movement Patterns of Rising from a Supine Position to an Erect Stance and Physical Functions in Healthy Children. Adv. Phys. Educ. 2013, 3, 92–97. [Google Scholar] [CrossRef][Green Version]
- Bohannon, R.W.; Lusardi, M.M. Getting up from the floor. Determinants and techniques among healthy older adults. Physiother. Theory Pract. 2004, 20, 233–241. [Google Scholar] [CrossRef]
- James, E.G. Body movement instructions facilitate synergy level motor learning, retention and transfer. Neurosci. Lett. 2012, 522, 162–166. [Google Scholar] [CrossRef]
- Santos De Oliveira, I.; Da, D.; Oliveira, S.; Cattuzzo, M.T. The Effect of Different Instructions in a General Motor Competence and Perceived Competence of Children. J. Phys. Educ. Sport. Manag. 2016, 3, 108–126. [Google Scholar]
- Beenakker, E.A.C.; Maurits, N.M.; Fock, J.M.; Brouwer, O.F.; van der Hoeven, J.H. Functional ability and muscle force in healthy children and ambulant Duchenne muscular dystrophy patients. Eur. J. Paediatr. Neurol. 2005, 9, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Naugle, K.M.; Higgins, T.J.; Manini, T.M. Obesity and use of compensatory strategies to perform common daily activities in pre-clinically disabled older adults. Arch. Gerontol. Geriatr. 2012, 54, e134–e138. [Google Scholar] [CrossRef] [PubMed]
- Manckoundia, P.; Buatois, S.; Gueguen, R.; Perret-Guillaume, C.; Laurain, M.C.; Pfitzenmeyer, P.; Benetos, A. Clinical determinants of failure in balance tests in elderly subjects. Arch. Gerontol. Geriatr. 2008, 47, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Klima, D.W.; Anderson, C.; Samrah, D.; Patel, D.; Chui, K.; Newton, R. Standing from the floor in community-dwelling older adults. J. Aging Phys. Act. 2016, 24, 207–213. [Google Scholar] [CrossRef]
- Manini, T.M.; Cook, S.B.; VanArnam, T.; Marko, M.; Ploutz-Snyder, L. Evaluating task modification as an objective measure of functional limitation: Repeatability and comparability. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 718–725. [Google Scholar] [CrossRef]
- King, L.A.; VanSant, A.F. The effect of solid ankle-foot orthoses on movement patterns used in a supine-to-stand rising task. Phys. Ther. 1995, 75, 952–964. [Google Scholar] [CrossRef]
- Belt, A.B.; Hertel, T.A.; Mante, J.R.; Marks, T.; Rockett, V.L.; Wade, C.; Clayton-Krasinski, D. Movement Characteristics of Persons with Prader-Willi Syndrome Rising from Supine. Pediatr. Phys. Ther. 2001, 13, 110–121. [Google Scholar] [CrossRef]
- Didier, J.P.; Mourey, F.; Brondel, L.; Marcer, I.; Milan, C.; Casillas, J.M.; Verges, B.; Winsland, J.K.D. The energetic cost of some daily activities: A comparison in a young and old population. Age Ageing 1993, 22, 90–96. [Google Scholar] [CrossRef]
- Ulbrich, J.; Raheja, A.; Alexander, N.B. Body positions used by healthy and frail older adults to rise from the floor. J. Am. Geriatr. Soc. 2000, 48, 1626–1632. [Google Scholar] [CrossRef]
- Schwickert, L.; Boos, R.; Klenk, J.; Bourke, A.; Becker, C.; Zijlstra, W. Inertial sensor based analysis of lie-to-stand transfers in younger and older adults. Sensors (Switz.) 2016, 16, 1277. [Google Scholar] [CrossRef]
- Schenkman, M.; Morey, M.; Kuchibhatla, M. Spinal flexibility and balance control among community-dwelling adults with and without Parkinson’s disease. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2000, 55, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Henwood, T.R.; Taaffe, D.R. Improved physical performance in older adults undertaking a short-term programme of high-velocity resistance training. Gerontology 2005, 51, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Manckoundia, P.; Gerbault, N.; Mourey, F.; d’Athis, P.; Nourdin, C.; Monin, M.P.; Camus, A.; Pfitzenmeyer, P. Multidisciplinary management in geriatric day-hospital is beneficial for elderly fallers: A prospective study of 28 cases. Arch. Gerontol. Geriatr. 2007, 44, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Geraldes, A.A.R.; Albuquerque, R.B.; Soares, R.M.; Carvalho, J.; Farinatti, P.T.V. Association between flexibility of the glenohumeral and hip joints and functional performance in active elderly women. Rev. Bras. Fisioter. 2008, 12, 274–282. [Google Scholar]
- Raso, V.; Greve, J.M.D. Aerobic or resistance exercise improves performance in activities of daily living in elderly women. Rev. Bras. Med. Esporte 2012, 18, 87–90. [Google Scholar] [CrossRef]
- Manckoundia, P.; Barthélémy, E.; Bonnot, R.; d’Athis, P. Impact of an ambulatory physical activity program on balance and motor abilities of retirees: A prospective study. Int. J. Clin. Pract. 2020, e13474. [Google Scholar]
- Moffett, M.A.; Avers, D.; Bohannon, R.W.; Shaw, K.L.; Merlo, A.R. Performance and Clinimetric Properties of the Timed Up From Floor Test Completed by Apparently Healthy Community-Dwelling Older Women. J. Geriatr. Phys. Ther. 2020. [Google Scholar] [CrossRef]
- Wulf, G.; McNevin, N.; Shea, C.H. The automaticity of complex motor skill learning as a function of attentional focus. Q. J. Exp. Psychol. A 2001, 54, 1143–1154. [Google Scholar] [CrossRef]
- Reid, K.F.; Fielding, R.A. Skeletal Muscle Power: A Critical Determinant of Physical. Exerc. Sport Sci. Rev. 2012, 40, 4–12. [Google Scholar] [CrossRef]
- Stodden, D.F.; True, L.K.; Langendorfer, S.J.; Gao, Z. Associations among selected motor skills and health-related fitness: Indirect evidence for Seefeldt’s proficiency barrier in young adults? Res. Q. Exerc. Sport 2013, 84, 397–403. [Google Scholar] [CrossRef]
- Utesch, T.; Bardid, F.; Strauss, B. The relationship between motor competence and physical fitness from early childhood to early adulthood: A meta-analysis. Sport. Med. 2019, 49, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.E.; Goodway, J.D. Instructional climates in preschool children who are at-risk. Part I: Object-control skill development. Res. Q. Exerc. Sport 2009, 80, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Barnett, L.M.; Morgan, P.J.; Van Beurden, E.; Ball, K.; Lubans, D.R. A reverse pathway? Actual and perceived skill proficiency and physical activity. Med. Sci. Sports Exerc. 2011, 43, 898–904. [Google Scholar] [CrossRef] [PubMed]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).