Abstract
Climate change mitigation policies can either facilitate or hinder progress towards health equity, and can have particular implications for Indigenous health. We sought to summarize current knowledge about the potential impacts (co-benefits and co-harms) of climate mitigation policies and interventions on Indigenous health. Using a Kaupapa Māori theoretical positioning, we adapted a validated search strategy to identify studies for this scoping review. Our review included empirical and modeling studies that examined a range of climate change mitigation measures, with health-related outcomes analyzed by ethnicity or socioeconomic status. Data were extracted from published reports and summarized. We identified 36 studies that examined a diverse set of policy instruments, with the majority located in high-income countries. Most studies employed conventional Western research methodologies, and few examined potential impacts of particular relevance to Indigenous peoples. The existing body of knowledge is limited in the extent to which it can provide definitive evidence about co-benefits and co-harms for Indigenous health, with impacts highly dependent on individual policy characteristics and contextual factors. Improving the quality of evidence will require research partnerships with Indigenous communities and study designs that centralize Indigenous knowledges, values, realities and priorities.
1. Introduction
Climate change is a powerful determinant of current and future health for all human populations [1,2]. The nature and magnitude of health impacts and the distribution of those impacts will be determined by the effectiveness of measures to limit the extent of climate change and protect against the adverse health consequences [2]. However, it is clear that the impacts of climate change are inequitable and, without substantial corrective action, will exacerbate existing health inequities between and within countries [3,4]. Disproportionate adverse impacts will be borne by people in low-income countries, and by disadvantaged populations within all countries [5,6].
Indigenous peoples are among those who will be hardest hit by the health impacts of climate change [7,8]. Although there is no universal definition of Indigenous peoples, key features include self-identification, historical continuity with pre-colonial and/or pre-settler societies, and strong links to territories and associated natural resources. Indigenous peoples currently form non-dominant sectors of society with distinct social, economic or political systems, and distinct languages, cultures and beliefs [9,10]. While there is considerable heterogeneity among Indigenous peoples, including in relation to geographical contexts, cultural backgrounds and sociopolitical circumstances, there are common features that confer greater vulnerability to climate change impacts. For many Indigenous populations, these factors are associated with the legacy and ongoing impacts of colonization.
The health and equity impacts of climate change make mitigation efforts critical. In particular, protecting Indigenous health now and into the future requires rapid, effective action to limit global warming to 1.5 degrees Celsius [11,12]. The choice and design of climate policies are also important for Indigenous health and health equity: actions to reduce greenhouse gas (GHG) emissions can have co-benefits and/or co-harms for health, and can either facilitate or hinder progress towards health equity [13,14]. Without explicit attention to Indigenous health and equity, mitigation actions threaten to exacerbate existing inequities [15].
It is therefore imperative that climate mitigation policies and actions are designed to maximize positive impacts and minimize adverse outcomes for Indigenous health. However, evidence on which to base these decisions is limited. Further, the range of possible climate mitigation policy instruments and their multidimensional impacts, including differential impacts on different populations, make this a complex field of study [16]. Co-impacts of climate change mitigation on health can be mediated through a multitude of pathways [17]. Health co-benefits occur through mechanisms such as reduced air pollution from changes in energy generation and transport mode shift, higher levels of physical activity and social contact as a result of increased active transport, reduced intake of foods from animal sources, and healthier indoor environmental conditions due to improved household insulation [18,19]. Adverse health impacts may occur as a result of increased indoor pollution due to reduced household ventilation, increased fuel poverty due to higher energy costs, greater exposure to danger as a result of increased active transport, and affected childhood growth and development from lower animal product consumption [19,20].
Very little has been published on this topic previously. In a recent review of the literature, Markkanen and Anger-Kraavi synthesized evidence about the social co-benefits and co-harms of climate change mitigation policy, including impacts on equity, with a focus on socioeconomic inequities [21]. Their analysis shows that most policies have the potential to produce both co-benefits and co-harms, and can either exacerbate or reduce inequities depending on contextual factors, policy design and policy implementation.
Over and above a more general analysis of climate policy and health equity (related to differential impacts by socioeconomic status and ethnicity), there is also an imperative for an explicit focus on the implications for Indigenous populations. While general understandings of health equity are relevant, the causal pathways leading to inequities for Indigenous peoples have distinctive features as a result of the historical, social and political contexts within which they are situated [22]. These include greater dependence on environmental resources for basic needs, living on marginal land with poorer infrastructure, socioeconomic deprivation, employment inequities, a greater existing burden of disease, poorer access to and quality of health care, and political marginalization [15,23]. Factors such as poverty and racism are clearly important determinants of Indigenous health, but are only intermediate causes. They are fundamentally driven by the ongoing processes and effects of colonization, which in turn determine how these factors confer differential exposure to health risks and benefits [24]. Colonization also constrains the design and diversity of potential climate and health responses, in particular through the systematic suppression of Indigenous knowledge systems and ways of being [25]. Colonization is itself just one manifestation of an exploitative Enlightenment philosophy that has resulted in catastrophic effects on Indigenous peoples and nature [26,27].
Climate change and societal responses to climate change are experienced in qualitatively and quantitatively different ways by Indigenous peoples in comparison with other population groups. Whyte [28] characterizes anthropogenic climate change as an intensification of environmental changes due to colonialism that have disrupted Indigenous peoples’ ways of living for centuries. The specific considerations in relation to the right to health for Indigenous peoples imply a need for an Indigenous-focused approach to this area of research, grounded in Indigenous worldviews and explicitly centering Indigenous lived experiences and realities [29]. Social policy in settler colonial contexts universally fails to adequately consider social determinants of Indigenous health and Indigenous rights [30], which means that generic equity analyses miss important outcomes for Indigenous populations.
This article summarizes current knowledge about the potential impacts (co-benefits and co-harms) of climate mitigation policy and interventions on Indigenous peoples’ health, and factors influencing the direction and magnitude of those impacts, with a view to informing national, regional and local decision making to uphold Indigenous rights including the right to health. In conceptualizing impacts, we use a multidimensional definition of health that draws on Indigenous understandings of well-being. We consider impacts on both health outcomes and the key determinants of health including modifiable social, economic and environmental conditions. Such an approach aligns with understandings of health inequity that include not only differences in health status, but also in important influences on health that are amenable to change, e.g., through social policy [31]. Health equity can be defined as “the absence of systematic disparities in health (or its social determinants) between more and less advantaged social groups” [32] (p. 256) and health inequities as “differences which are unnecessary and avoidable, but in addition are considered unfair and unjust” [33] (p. 431).
2. Materials and Methods
2.1. Methodology
For this research, we adopted a Kaupapa Māori theoretical positioning. Kaupapa Māori theory arises from Māori (the Indigenous peoples of Aotearoa New Zealand) ontology, epistemology and axiology [34,35], and centralizes Māori worldviews, philosophies and principles [36]. It does not make claims to universal truth or superiority as a research paradigm, but instead seeks to challenge the primacy of ‘conventional’ research methodologies in order to centralize Māori ways of knowing and being [37].
Kaupapa Māori promotes action that is transformative, empowering and liberatory [38]. It seeks to critically examine and expose systems of power that have created and perpetuate social inequities [37]. Kaupapa Māori research methodology does not prescribe or prohibit any particular study designs, methods or tools, but rather can utilize whatever methods are best suited to answer the research question(s). Decisions about methods are informed by Kaupapa Māori principles, including that research should be transformative; promote social justice; be informed by Māori knowledge; focus on critiquing power and privilege; reject cultural-deficit theories; accept diverse Māori realities; and be emancipatory and supportive of decolonization [39].
This research is Indigenous led and two of the authors (R.J. and P.R.) are senior Māori academics, while the third (A.M.) is Pākehā (New Zealand settler of European descent) and tangata Tiriti (people in NZ by virtue of te Tiriti o Waitangi, the founding treaty between Māori and the British Crown, with a te Tiriti-mandated responsibility for good governance). Collectively, our positionality explicitly acknowledges the central role of colonization in shaping the social, political and economic realities of Indigenous peoples. We assert that it is not possible to understand the implications of climate policy for Indigenous health without situating our review of the evidence within this context. Colonial values and systems also underpin Western academic practice and have powerfully shaped the body of existing research, as well as determining which forms of knowledge are deemed legitimate. While this body of literature has theoretical limitations, there is value in elucidating the issues that are foregrounded within it. We therefore applied a Kaupapa Māori lens in order to review literature with a particular focus on understanding its potential to advance Indigenous health and health equity.
2.2. Research Methods
We utilized standard scoping review methods on this Kaupapa Māori theoretical base and report them below according to the relevant sections of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)-ScR guidelines [40].
2.2.1. Scoping Review Questions
The review sought to answer the following questions:
- What does the current evidence suggest are important potential impacts (co-benefits and co-harms) of climate change mitigation policies and interventions on Indigenous health?
- What factors influence the direction and magnitude of these impacts?
- What are the strengths and limitations of existing research to examine the impacts of climate change mitigation measures on Indigenous health?
2.2.2. Eligibility Criteria
Eligibility of studies was determined according to the criteria detailed below. The review included qualitative, quantitative and mixed methods studies of all study designs. It was limited to English language articles where the full text was available, with no time limit on publication dates. We expected the body of eligible studies specifically relating to Indigenous peoples to be small, and therefore took an inclusive view in how we identified Indigenous populations, as well as including other dimensions of equity. In particular, studies examining the distribution of co-benefits and/or co-harms by ethnicity and socioeconomic status (SES) were included, as they capture dynamics relevant to the etiology of Indigenous/non-Indigenous health inequities. Identifying potentially racist outcomes of policies or interventions (by including studies examining ethnic inequities) is relevant as these racist outcomes are likely to contribute to differential impacts for Indigenous populations. Similarly, in most contexts SES is an important factor mediating Indigenous/non-Indigenous health inequities [41], so actions that have differential impacts by SES are likely to have particular impacts for Indigenous peoples. Studies examining only gender inequities were not included, as there was not considered to be a plausible and consistent mechanism linking gender differences and differences by Indigeneity.
‘Climate Citigation’ Criteria
Inclusion criteria:
- Studies of climate mitigation interventions (policies or interventions designed, at least in part, to reduce net greenhouse gas emissions) were eligible.
- Studies that modeled scenarios associated with climate change mitigation policies or interventions were eligible.
- Eligible outcome measures included all measures of human health and determinants of health.
- Quantitative studies were eligible, including both empirical and modeling studies. Under the ‘empirical’ category, randomized controlled trials, non-randomized controlled trials, controlled before–after studies and interrupted time series studies were eligible. In addition, modeling studies that estimated the impact of climate mitigation interventions on health outcomes were eligible.
- Qualitative studies were eligible.
Exclusion criteria:
- Studies that only described climate mitigation policies or interventions, and did not assess impacts on one or more health outcomes or determinants of health, were not eligible.
- Studies that examined only the health impacts of climate change or of climate-related exposures (e.g., air pollution), and not the health impacts of climate mitigation policy or interventions, were not eligible.
- Studies with an exclusive focus on climate change adaptation, with no mitigation component, were not eligible.
‘Equity-Focused’ Criteria
Inclusion criteria:
- To be eligible, studies must have assessed whether the impacts of climate mitigation measures differ by ethnicity/indigeneity and/or socioeconomic status (SES), or they must have assessed the specific impacts of climate mitigation measures for Indigenous and/or other marginalized populations. The following types of study were eligible:
- ⚬
- Studies that reported effect estimates stratified by ethnicity/indigeneity or SES;
- ⚬
- Studies that reported population-specific effect estimates for Indigenous and/or other marginalized populations;
- ⚬
- Studies that reported whether or not there was an interaction effect between intervention and the ethnicity/SES variable were eligible.
- Indigenous populations were defined according to the approach used by Anderson et al. [42], based on criteria specified by the UNPFII [10].
- Income, education, employment and housing tenure were eligible measures at individual level. Neighborhood deprivation was an eligible area level measure of SES, and also eligible as a proxy for individual SES.
Exclusion criteria:
- Studies that assessed only whether there was confounding by ethnicity/indigeneity/SES (rather than whether intervention effects differed by ethnicity/indigeneity/SES) were not eligible.
2.2.3. Search Strategy
We searched MEDLINE, EMBASE, Web of Science and Scopus from 5 to 8 August 2019. An initial limited search of these databases was conducted, followed by an analysis of text words contained in the title and abstract of identified articles, and of the index terms used. We used these keywords and index terms to develop customized search strategies for each of the databases, based on a validated search strategy for equity-focused reviews [43]. A sample search strategy is provided in Appendix A. In addition, we identified possible evidence sources from the WHO and IPCC websites.
2.2.4. Study Selection
One reviewer (R.J.) screened the titles and abstracts of identified studies to exclude publications that clearly did not meet the inclusion criteria. For each of the remaining articles, the full-text article was retrieved for review and assessed against the inclusion and exclusion criteria. A 10% sample of the full-text articles was assessed by a second reviewer (A.M.).
2.2.5. Data Charting
Data were entered in Microsoft Excel. Given the broad scope of included studies, data charting was an iterative process throughout the review and minor amendments were made to the data variables as required. One reviewer (R.J.) undertook data charting of all included studies, with independent charting of ten randomly selected studies undertaken by a second reviewer (A.M.).
The following data items were collected during the data charting process:
- Publication characteristics: title, year of publication, study design, country of origin, study setting.
- Type of study, e.g., modeling, intervention study, qualitative or quantitative methods.
- Characteristics of mitigation policy or intervention
- Context (governmental jurisdiction(s), target population(s));
- Typology (by IPCC categories) [20]: (i) Policy instrument (e.g., economic instruments, regulatory, government provision of public goods or services); and (ii) Sector (e.g., Energy, Transport, Buildings);
- Detailed description of the policy measure(s) or intervention(s).
- Outcomes analyzed
- Climate outcomes (e.g., emissions reductions);
- Social co-benefits and/or co-harms (e.g., air pollution, household costs/savings, employment, food security);
- Health outcomes (e.g., mortality, morbidity, risk factors).
- Equity and/or subgroup analyses
- Detail of any equity analysis (e.g., by gender, ethnicity, SES);
- Were Indigenous-specific outcomes reported?
- Key findings
- General findings;
- Equity findings;
- Indigenous-specific findings (if applicable).
- Implications for mitigation policy design and implementation
- Factors influencing direction and magnitude of co-benefits/co-harms;
- Recommendations for promoting pro-equity outcomes.
- Validity assessment
- Internal validity (‘quality’ assessment);
- External validity (Kaupapa Māori) assessment.
We reported the setting of the policy or intervention according to the relevant policy making or governmental jurisdiction(s), e.g., USA, China, New Zealand. This approach reflects the importance of identifying the national contexts within which climate policy making occurs and is consistent with an emphasis on critiquing systems of power.
2.2.6. Data Synthesis
The data were summarized numerically using descriptive statistical methods, and qualitatively using thematic analysis. The study findings were grouped into different categories of mitigation policy measures, and within each category we summarized the type of settings, populations and study designs, along with the measures used and broad findings. Where we identified a systematic review, we counted the number of studies included in the review that potentially met our inclusion criteria and noted how many studies had been missed by our search.
2.2.7. Validity Assessment
Because of the very heterogeneous and sparse nature of the literature, a detailed assessment of study quality was not undertaken. Internal validity was assessed informally using criteria adapted from CASP checklists [44] for different study types. A greater emphasis was placed on external validity, for which we focused on the potential contribution of studies in relation to Indigenous health and equity, using a set of Kaupapa Māori criteria. This assessment addressed: (i) theoretical/methodological issues (e.g., consistency with Indigenous theoretical positioning and/or critical/decolonial theory); (ii) validity of process (e.g., involvement of Indigenous communities and contribution of Indigenous knowledges and values); and (iii) validity of outcomes (e.g., the extent to which potential impacts of particular relevance to Indigenous peoples were included in the analysis).
3. Results
From an initial 3539 citations, we identified 36 published articles, each from separate studies. Thirteen of the initial citations were identified from systematic reviews having been missed by our search; from these citations, one study met the scoping review inclusion criteria and was added. Figure 1 provides details of the study selection process.
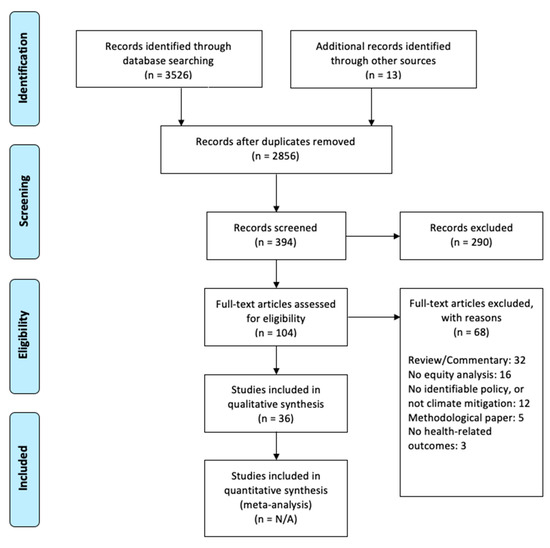
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram for study inclusion.
Table 1 provides details of the included studies, including governmental jurisdiction, type of study, summary of any Indigenous participation or methodology, policy instrument and sector, a brief description of the policy or intervention, and an indication of positive and/or negative implications for Indigenous health.

Table 1.
Details of included studies.
Eight studies were carried out in the USA [48,52,53,56,58,70,72,74], seven in the UK [60,68,73,75,77,78,80], three in New Zealand [57,66,67], and two each in China [47,62], India [49,61] and Mexico [50,59]. Other jurisdictions represented were Canada [69], the Dominican Republic [71], Ecuador [64], France [55], Finland [45], Greece [46], Malaysia [65], South Africa [79], Tanzania [63] and Venezuela [51]. Two studies examined policies across multiple jurisdictions [54,76].
The most common study type was modeling (n = 18), which included a range of environmental modeling methods and general equilibrium economic modeling [45,48,52,55,59,60,61,62,65,66,67,68,72,73,77,78,79,80]. Two studies used health impact assessment methods [46,70] and the remainder (n = 16) were empirical studies, including surveys, before/after comparisons, randomized controlled trials and case studies [47,49,50,51,53,54,56,57,58,63,64,69,71,74,75,76].
Table 2 shows how the studies were distributed according to the type of policy instrument and sector.
Table 2.
Distribution of studies according to policy instrument and sector.
3.1. Indigenous Data
Twelve studies included an identifiable Indigenous population, either as a central focus of the research or as an identifiable subgroup in the analysis [49,50,51,54,56,64,66,67,69,71,74,76]. These studies were carried out in Canada [69], the Dominican Republic [71], Ecuador [64], India [49], Mexico [59], New Zealand [66,67], the USA [56,74], and Venezuela [51], with one study covering Australia and British Columbia, Canada [54] and one examining multiple countries (Brazil, Peru, Cameroon, Tanzania, Indonesia and Vietnam) [76]. Of these studies, nine had an explicit focus on Indigenous communities and/or the policy or intervention was predominantly based in Indigenous communities [50,51,54,56,64,69,71,74,76].
3.2. Validity Assessment
The most common type of study involved modeling the impacts of proposed or existing climate policy, with many using general equilibrium macroeconomic modeling. Such models have been subjected to significant and fundamental critiques, including that their foundational assumptions are widely accepted to be wrong (including that the economy tends towards equilibrium, that actors make homogenous rational choices—with an extremely limited understanding of “rational”, and that actors are individualistic and selfish) [81,82], that important differences that determine inequities must be ignored [82] and that large and vital parts of the real economy (e.g., unpaid work and the commons) are absent [81]. These critiques are particularly important to the understanding of impacts on Indigenous health (not just because inequities are missing, but also because of the missing roles of unpaid work, collective ownership and decisions based on collective well-being).
Other studies varied in terms of quality, ranging from well-designed before–after comparison studies to uncontrolled case studies. Almost all employed conventional Western research methodologies and did not incorporate Indigenous theoretical positioning or engage with critical or decolonial theory. Few studies examined potential impacts of particular relevance to Indigenous peoples, such as revitalization of Indigenous languages and knowledge systems, protection of sites of cultural significance or sovereignty.
Only three studies reported being conceived, designed or conducted in partnership with Indigenous communities or informed by Indigenous knowledges and values [56,69,74]. Richards et al. [69] reported on three projects among Inuit peoples in Canada that involved supporting Indigenous communities to conduct their own research. These projects contributed to building community capacity, with significant value placed on Indigenous ways of knowing, doing and being in order to create positive change for their communities. The study by Champion et al. [56] followed key concepts in Navajo philosophy relating to partnership, community consensus, education and critical thinking to develop a culturally-specific framework to evaluate household heating alternatives in the Navajo nation. Sikka et al. [74] examined the outcomes of developing a sustainable biomass energy industry in Alaska Native communities with an explicit emphasis on how the initiative aligned with core cultural values.
3.3. Impact by Policy Type
Analysis of economic instruments such as carbon taxes and emissions trading schemes predominantly examined co-impacts mediated through socioeconomic inequities. These instruments were generally shown to be financially regressive, at least in high-income countries and in the absence of mitigating actions [48,54,60,72]. Carbon pricing can lead to improvements in other determinants of health such as air quality [48]. However, these effects can be inequitable, as was observed in California’s cap-and-trade program that resulted in a paradoxical increase in GHG and co-pollutant emissions in disadvantaged neighborhoods [58]. One study examined different methods of revenue recycling as a way to mitigate the regressive impacts of emissions pricing, and found that the most progressive approach was direct household rebates [48]. Revenue can also be recycled in ways which address other aspects of equity, for example programs to reduce energy poverty such as electrification, sustainable housing and rooftop solar for low-income households [79].
One study explicitly considered the impact of carbon pricing policies on Indigenous populations, and identified some important principles for promoting equity [54]. For example, procedural fairness was shown to be a key consideration, including the ability for Indigenous peoples to participate in the process of selecting and designing the policy. Such participation could help to avoid disproportionate impacts from the increased cost of goods and services, and improve access to the measures introduced to mitigate the cost increases. The authors noted the importance of considering the equity implications of the entire policy package, not only in relation to income but also by cultural, ethnic, gender, region and other demographic factors.
Policies based on government provision of public goods or services were most commonly in the buildings sector, with four studies examining housing renovation to improve insulation and/or heating [53,57,73,75]. Three of these studies reported largely positive effects for low income households, including reduced energy use and fuel poverty, increased indoor temperatures and improved health outcomes [53,57,75]. Some adverse impacts on health equity were noted, with one study reporting an increase in general practitioner visits post-intervention [57] and an analysis of the Warm Front program in England identifying a number of challenges including targeting of assistance and increased fuel consumption in some low-income households [75]. The fourth study identified negative impacts on indoor air quality based on modeling of a full retrofit of the UK housing stock, with elevated health risks primarily due to reduced building permeability [73]. This was the only study in this category to explicitly consider equity implications, with generally higher estimated indoor PM2.5 concentrations in low-income households in the retrofitted scenario.
Four studies examined regulatory approaches, all of which were situated in the forestry sector and predominantly focused on aspects of REDD (Reducing Emissions from Deforestation and forest Degradation in developing countries) and REDD+ programs (REDD plus sustainable forest management, as well as enhancement of forest carbon stocks) [59,63,64,76]. These tended to have mixed results, with apparently inevitable trade-offs between effectiveness, efficiency and equity [59]. While there were some benefits identified, for example, better governance and potential employment opportunities, two studies demonstrated inequities in relation to knowledge, participation and benefit sharing [63,64]. A further study found no significant contribution of REDD+ to improving well-being or perceived income sufficiency among most communities [76]. Recommendations from these studies examining regulatory approaches included the need to avoid a one-size-fits-all approach, to strengthen participation and ensure greater community involvement throughout the program, and to respect the self-determination of Indigenous communities.
Five studies examined a combination of different types of policy or intervention [45,46,47,56,61] and a further seven were based on scenario modeling rather than a specific policy or policies [52,62,66,68,77,78,80].
The three studies that had documented Indigenous participation and/or incorporation of Indigenous methodologies in the research process contributed distinctive insights [56,69,74]. They examined aspects of interventions and outcome measures that differed in important ways from other studies included in this review. For example, in the study examining climate adaptation and mitigation initiatives in Inuit communities, intergenerational knowledge transmission was identified as a key factor in strengthening community resiliency and promoting the sustainability of these initiatives over time [69]. In relation to home heating in the Navajo nation, as a result of explicitly incorporating community perceptions and cultural values in the analysis, the study arrived at different conclusions than would have been the case if the model had included only the ‘standard’ environmental, health and economic indicators [56]. Among the merits of using wood pellets rather than oil for Alaska Native communities, affirmation of core Indigenous cultural values around preservation of resources for future generations was identified as a key social benefit [74].
3.4. Implications for Indigenous Health
Potential co-benefits for Indigenous health identified in the studies arise through a number of different mechanisms, including reduced air pollution; warmer, drier homes; lower energy costs; increased physical activity; improved diets, validation of Indigenous knowledges; and revitalizing and supporting the use of traditional practices. The actual benefits and impacts on Indigenous/non-Indigenous inequities in health depend on a variety of factors relating to policy or intervention design and implementation.
The most important co-harms to Indigenous health identified in this review were due to economically regressive impacts (especially carbon taxes and emissions trading schemes); job losses that disproportionately affect low income and/or Indigenous populations; fuel poverty; and negative impacts on diet (Indigenous dietary systems and traditional food sources were not considered).
4. Discussion
This scoping review sought to summarize the current state of knowledge about the co-impacts of climate change mitigation policy and interventions on Indigenous health. In relation to Indigenous peoples and climate change, research attention has tended to focus on adaptation rather than mitigation [23]. Nonetheless, there are examples in the published literature of local-level mitigation initiatives that have been evaluated with regard to outcomes for Indigenous populations [51,63,71]. However, to our knowledge this is the first systematic review of climate change mitigation policy with respect to Indigenous health.
This scoping review was inclusive of a broad range of policy instruments, interventions and study designs. We adapted a search strategy that had been developed and validated for reviews investigating whether the effects of interventions differ by ethnicity or socioeconomic status. In keeping with a Kaupapa Māori methodological approach, we explicitly analyzed how well studies addressed issues of importance to Indigenous peoples. However, given the wide scope of the review and the heterogeneity of terminology used in article titles, abstracts and keywords, our search is likely to have missed relevant studies. The review also had an emphasis on publications in the peer-reviewed literature, which may have led to the exclusion of potentially eligible studies, for example those disseminated as unpublished evaluations and reports. The search may also have missed studies reported in non-indexed journals. These factors may explain the dearth of Indigenous-centered research identified by our search strategy. However, there is utility in examining the published literature as this is likely to be an important source of information for policy makers.
The heterogeneity of evidence sources, including the range of study designs, contexts, policy and intervention types, and approaches to equity analysis make it difficult to draw specific conclusions about the relative merits of particular interventions. Climate mitigation draws on numerous different policy instruments across many different sectors [20], with myriad possible co-impacts on health and on the determinants of health [17]. Indeed, our analysis indicates a range of possible impacts on Indigenous health, both positive and negative. There does not appear to be a clear pattern based on policy or intervention type, with specific features and contextual factors likely to be important in determining impacts. Rather than specifically guiding policy selection or design, the breadth of sources considered in this study allow the identification of general principles that can inform climate mitigation efforts in order to contribute to Indigenous health equity.
With its particular emphasis, our review complements existing reviews and adds novel insights. For example, the recent synthesis of evidence by Markkanen and Anger-Kraavi [21] included only one of the studies in our sample [63]. Like our review, it showed that most climate change mitigation policies can produce both co-benefits and co-harms, and can be either pro- or anti-equity depending on a range of factors. It also found that the adverse equity impacts of climate policies can be mitigated, but noted that this requires a deliberate, carefully planned approach with community engagement. Our review had a greater focus on critically examining the literature with respect to its implications for Indigenous health.
Most studies in our review did not explicitly consider Indigenous health equity. Existing evidence therefore comes from research that is generally not designed to centralize Indigenous considerations. Drawing conclusions about potential impacts on Indigenous health requires a degree of inference based on factors such as differences by socioeconomic status, which leave out a range of specific considerations for Indigenous peoples. The outcome of this information gap will be climate mitigation actions that fail to fully account for the unique realities of Indigenous peoples or address the specific determinants of inequity, especially those resulting from ongoing colonization. Policies and interventions are therefore likely to drive further inequity, which is a breach of Indigenous rights [83].
Further, the vast majority of the evidence identified in this review relates to climate mitigation that operates within existing social, political and economic systems. This is problematic from a Kaupapa Māori perspective given the integral role these systems play in perpetuating not only climate change [3] but processes of colonization, marginalization and exploitation that drive Indigenous health inequities. Genuine climate solutions must seek to disinvest from institutions and systems that are complicit in fueling the climate crisis, and instead must be grounded in different ways of knowing, doing and being that reflect Indigenous values [84].
These gaps in existing research and policy mean that there is insufficient evidence to inform climate mitigation action that can uphold Indigenous rights and contribute to health equity. In order to address these gaps, research must centralize Indigenous worldviews, methodologies, realities and priorities. As underlined by our analysis of the three studies in this review that adopted Indigenous methodologies, such research examines the issues through a distinctive lens that generates unique and important insights. These studies highlighted issues not considered in other studies, including aspects of interventions such as intergenerational knowledge transmission and incorporation of cultural values, as well as critical contextual factors related to ongoing experiences of colonization. Brugnach et al. [85] provide a conceptual framework to support the participation of Indigenous communities in climate mitigation policy and decision making, emphasizing the recognition of Indigenous knowledges and the need for power-sharing. As the impacts of climate mitigation measures on Indigenous health equity are highly dependent on the specific characteristics of the intervention and relevant contextual factors, these generic principles of engagement are critical in ensuring that Indigenous realities and priorities are addressed and that equity issues are centered.
5. Conclusions
There is a dearth of information about the co-benefits and co-harms of climate mitigation policy for Indigenous health. Much of the evidence that currently exists is from generic equity analyses and limited Western perspectives on relevant outcomes, which has serious limitations in relation to informing future climate policy. Very few studies have used Indigenous or decolonial research methodologies, which influences the philosophical basis of the research, the questions asked, methods used, type of outcomes examined, interpretation of findings and translation of knowledge into action.
Despite the complexity of this field of research, it is possible to improve the quality of evidence about co-impacts on Indigenous health in order to inform pro-equity climate mitigation. This will require partnership with Indigenous communities, recognition and privileging of Indigenous knowledges and study design that fully embeds Indigenous values, realities and priorities. Fundamentally, sharing of power, both in the research process and in the conception, design and implementation of climate policy and interventions, will be essential for Indigenous rights and health equity.
Author Contributions
R.J., A.M. and P.R., conceived the study and contributed to development of the research methods. R.J. conducted the literature searches, screening and selection of studies, data charting and analysis, and prepared the first draft of the manuscript. A.M. undertook the independent review of study selection and data charting. A.M. and P.R. advised on the literature search strategy, data analysis and interpretation of findings. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
We declare no other competing interests.
Appendix A. Sample Search Strategy (MEDLINE)
- (equit* or inequit* or inequalit* or disparit* or equality).tw.
- (ethnic* or race or racial* or racis*).tw.
- (indigen* or Maori or Aborigin* or native or tribal or First Nations).tw.
- ((social* or socio-economic or socioeconomic or economic or structural or material) adj3 (advantage* or disadvantage* or exclude* or exclusion or include* or inclusion or status or position or gradient* or hierarch* or class* or determinant*)).tw.
- (health adj3 (gap* or gradient* or hierarch*)).tw.
- Vulnerable populations/ or socioeconomic factors/ or poverty/ or social class/ or Healthcare Disparities/ or Health Status Disparities/ or Poverty areas/ or Urban population/
- (SES or SEP or sociodemographic* or socio-demographic* or income or wealth* or poverty or educational level or level of education or educational attainment or well educated or better educated or unemploy* or home owner* or tenure or affluen* or well off or better off or worse off).tw.
- 1 or 2 or 3 or 4 or 5 or 6 or 7
- (climate change or global warming or greenhouse gas or GHG or carbon or CO2 or methane or emissions).tw. or Climate Change/ or Greenhouse Effect/pc
- (mitigat* or cut or low or lower or limit or curb or reduce or abate* or sequestr* or Paris Agreement or energy justice or just transition or energy transition* or renewable energy or polic* or plan or plans or planning or intervention or strategy or strategies or experiment or trial or program* or tax* or cap-and-trade or initiative* or pric* or subsid* or promot* or campaign* or evaluation or evaluating or implementation or implementing or modelling or modeling or impact assessment or cost-benefit analysis or comparative risk assessment).tw. or health impact assessment/
- (health or wellbeing or well-being or wellness).tw.
- 8 and 9 and 10 and 11
- limit 12 to humans
References
- Costello, A.; Abbas, M.; Allen, A.; Ball, S.; Bell, S.; Bellamy, R.; Friel, S.; Groce, N.; Johnson, A.; Kett, M.; et al. Managing the health effects of climate change: Lancet and University College London Institute for Global Health Commission. Lancet 2009, 373, 1693–1733. [Google Scholar] [CrossRef]
- Smith, K.R.; Woodward, A.; Campbell-Lendrum, D.; Chadee, D.; Honda, Y.; Liu, Q.; Olwoch, J.M.; Revich, B.; Sauerborn, R. Human Health: Impacts, Adaptation, and Co-benefits. In Climate Change 2014: Impacts, Adaptation and Vulnerability. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Field, C.B., Barros, V.R., Dokken, D.J., Mach, K.J., Mastrandrea, M.D., Bilir, T.E., Chatterjee, M., Ebi, K.L., Estrada, Y.O., Genova, R.C., et al., Eds.; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014; pp. 709–754. [Google Scholar]
- Friel, S.; Marmot, M.; McMichael, A.J.; Kjellstrom, T.; Vagero, D. Global health equity and climate stabilisation: A common agenda. Lancet 2008, 372, 1677–1683. [Google Scholar] [CrossRef]
- World Health Organization. Quantitative Risk Assessment of the Effects of Climate Change on Selected Causes of Death, 2030s and 2050s; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Patz, J.A.; Gibbs, H.K.; Foley, J.A.; Rogers, J.V.; Smith, K.R. Climate Change and Global Health: Quantifying a Growing Ethical Crisis. Ecohealth 2007, 4, 397–405. [Google Scholar] [CrossRef]
- World Health Organization; World Meteorological Association. Atlas of Health and Climate; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Ford, J.D. Indigenous health and climate change. Am. J. Public Health 2012, 102, 1260–1266. [Google Scholar] [CrossRef]
- Green, D.; King, U.; Morrison, J. Disproportionate burdens: The multidimensional impacts of climate change on the health of Indigenous Australians. Med. J. Aust. 2009, 190, 4–5. [Google Scholar] [CrossRef]
- United Nations. State of the World’s Indigenous Peoples, Introduction; United Nations: New York, NY, USA, 2009; pp. 1–11. [Google Scholar]
- United Nations Permanent Forum on Indigenous Issues. Who Are Indigenous Peoples? Available online: http://www.un.org/esa/socdev/unpfii/documents/5session_factsheet1.pdf (accessed on 2 November 2020).
- Intergovernmental Panel on Climate Change. Global Warming of 1.5 °C. An IPCC Special Report on the Impacts of Global Warming of 1.5 °C above Pre-Industrial Levels and Related Global Greenhouse Gas Emission Pathways, in the Context of Strengthening the Global Response to the Threat of Climate Change, Sustainable Development, and Efforts to Eradicate Poverty; IPCC: Geneva, Switzerland, 2018. [Google Scholar]
- Sealey-Huggins, L. ‘1.5 °C to stay alive’: Climate change, imperialism and justice for the Caribbean. Third World Q. 2017, 38, 2444–2463. [Google Scholar] [CrossRef]
- Walpole, S.C.; Rasanathan, K.; Campbell-Lendrum, D. Natural and unnatural synergies: Climate change policy and health equity. Bull. World Health Organ. 2009, 87, 799–801. [Google Scholar] [CrossRef]
- Watts, N.; Adger, W.N.; Agnolucci, P.; Blackstock, J.; Byass, P.; Cai, W.; Chaytor, S.; Colbourn, T.; Collins, M.; Cooper, A.; et al. Health and climate change: Policy responses to protect public health. Lancet 2015, 386, 1861–1914. [Google Scholar] [CrossRef]
- Jones, R. Climate change and Indigenous Health Promotion. Glob. Health Promot. 2019, 26, 73–81. [Google Scholar] [CrossRef]
- Klinsky, S.; Winkler, H. Building equity in: Strategies for integrating equity into modelling for a 1.5 °C world. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2018, 376, 20160461. [Google Scholar] [CrossRef]
- Ürge-Vorsatz, D.; Herrero, S.T.; Dubash, N.K.; Lecocq, F. Measuring the Co-Benefits of Climate Change Mitigation. Annu. Rev. Environ. Resour. 2014, 39, 549–582. [Google Scholar] [CrossRef]
- Gao, J.; Kovats, S.; Vardoulakis, S.; Wilkinson, P.; Woodward, A.; Li, J.; Gu, S.; Liu, X.; Wu, H.; Wang, J.; et al. Public health co-benefits of greenhouse gas emissions reduction: A systematic review. Sci. Total Environ. 2018, 627, 388–402. [Google Scholar] [CrossRef]
- Haines, A.; McMichael, A.J.; Smith, K.R.; Roberts, I.; Woodcock, J.; Markandya, A.; Armstrong, B.G.; Campbell-Lendrum, D.; Dangour, A.D.; Davies, M.; et al. Public health benefits of strategies to reduce greenhouse-gas emissions: Overview and implications for policy makers. Lancet 2009, 374, 2104–2114. [Google Scholar] [CrossRef]
- Intergovernmental Panel on Climate Change. Climate Change 2014: Mitigation of Climate Change: Working Group III Contribution to the IPCC Fifth Assessment Report; Cambridge University Press: Cambridge, UK, 2015. [Google Scholar]
- Markkanen, S.; Anger-Kraavi, A. Social impacts of climate change mitigation policies and their implications for inequality. Clim. Policy 2019. [Google Scholar] [CrossRef]
- Reid, P.; Robson, B. Understanding Health Inequities. In Hauora: Māori Standards of Health IV. A Study of the Years 2000–2005; Robson, B., Harris, R., Eds.; Te Rōpū Rangahau Hauora a Eru Pōmare: Wellington, New Zealand, 2007; pp. 3–10. [Google Scholar]
- Ramos-Castillo, A.; Castellanos, E.J.; Galloway McLean, K. Indigenous peoples, local communities and climate change mitigation. Clim. Chang. 2017, 140, 1–4. [Google Scholar] [CrossRef]
- Paradies, Y. Colonisation, racism and indigenous health. J. Popul. Res. 2016, 33, 83–96. [Google Scholar] [CrossRef]
- Reid, P.; Cormack, D.; Paine, S.J. Colonial histories, racism and health-The experience of Maori and Indigenous peoples. Public Health 2019, 172, 119–124. [Google Scholar] [CrossRef]
- Lindgren, T. Ecocide, genocide and the disregard of alternative life-systems. Int. J. Hum. Rights 2018, 22, 525–549. [Google Scholar] [CrossRef]
- Moewaka Barnes, H.; McCreanor, T. Colonisation, hauora and whenua in Aotearoa. J. R. Soc. N. Z. 2019, 49, 19–33. [Google Scholar] [CrossRef]
- Whyte, K.P. Indigenous Climate Change Studies: Indigenizing Futures, Decolonizing the Anthropocene. Engl. Lang. Notes 2017, 55, 153–162. [Google Scholar] [CrossRef]
- Jones, R.; Bennett, H.; Keating, G.; Blaiklock, A. Climate change and the right to health for Maori in Aotearoa/New Zealand. Health Hum. Rights 2014, 16, 54–68. [Google Scholar] [PubMed]
- George, E.; Mackean, T.; Baum, F.; Fisher, M. Social Determinants of Indigenous Health and Indigenous Rights in Policy: A Scoping Review and Analysis of Problem Representation. Int. Indig. Policy J. 2019, 10. [Google Scholar] [CrossRef]
- Braveman, P. Health disparities and health equity: Concepts and measurement. Annu. Rev. Public Health 2006, 27, 167–194. [Google Scholar] [CrossRef] [PubMed]
- Braveman, P.; Gruskin, S. Defining equity in health. J. Epidemiol. Commun. Health 2003, 57, 254–258. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, M. The concepts and principles of equity and health. Int. J. Health Serv. 1992, 22, 429–445. [Google Scholar] [CrossRef]
- Pihama, L. Kaupapa Māori Theory: Transforming Theory in Aotearoa. He Pukenga Kōrero 2010, 9, 5–14. [Google Scholar]
- Smith, L. Decolonising Methodologies: Research and Indigenous Peoples, 2nd ed.; Zed Books Ltd.: London, UK, 2012. [Google Scholar]
- Smith, G.H. The Development of Kaupapa Māori: Theory and Praxis. Ph.D. Thesis, The University of Auckland, Auckland, New Zealand, 1997, unpublished. [Google Scholar]
- Mahuika, M. Kaupapa Māori Theory is critical and anti-colonial. MAI Rev. 2008, 3, 1–16. [Google Scholar]
- Walker, S.; Eketone, A.; Gibbs, A. An exploration of kaupapa Māori research, its principles, processes and applications. Int. J. Soc. Res. Methodol. 2006, 9, 331–344. [Google Scholar] [CrossRef]
- Curtis, E. Indigenous positioning in health research: The importance of Kaupapa Māori theory informed practice. Altern. Int. J. Indig. Peoples 2016, 12, 396. [Google Scholar] [CrossRef]
- Tricco, A.; Lillie, E.; Zarin, W.; O’Brien, K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation.(Research And Reporting Methods)(Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews)(Report)(Author abstract). Ann. Intern. Med. 2018, 169, 467. [Google Scholar] [CrossRef]
- Gracey, M.; King, M. Indigenous health part 1: Determinants and disease patterns. Lancet 2009, 374, 66–75. [Google Scholar] [CrossRef]
- Anderson, I.; Robson, B.; Connolly, M.; Al-Yaman, F.; Bjertness, E.; King, A.; Tynan, M.; Madden, R.; Bang, A.; Coimbra, C.; et al. Indigenous and tribal peoples’ health (The Lancet–Lowitja Institute Global Collaboration): A population study. Lancet 2016, 388, 131–157. [Google Scholar] [CrossRef]
- Hosking, J.; Macmillan, A.; Jones, R.; Ameratunga, S.; Woodward, A. Searching for health equity: Validation of a search filter for ethnic and socioeconomic inequalities in transport. Syst. Rev. 2019, 8, 94. [Google Scholar] [CrossRef]
- Critical Skills Appraisal Programme. CASP Checklists; Critical Appraisal Skills Programme: Oxford, UK, 2020. [Google Scholar]
- Asikainen, A.; Parjala, E.; Jantunen, M.; Tuomisto, J.T.; Sabel, C.E. Effects of Local Greenhouse Gas Abatement Strategies on Air Pollutant Emissions and on Health in Kuopio, Finland. Climate 2017, 5, 43. [Google Scholar] [CrossRef]
- Bailey, J.; Gerasopoulos, E.; Rojas-Rueda, D.; Benmarhnia, T. Potential health and equity co-benefits related to the mitigation policies reducing air pollution from residential wood burning in Athens, Greece. J. Environ. Sci. Health Part A Toxic/Hazard. Subst. Environ. Eng. 2019. [Google Scholar] [CrossRef]
- Barrington-Leig, C.; Baumgartner, J.; Carter, E.; Robinson, B.E.; Tao, S.; Zhang, Y. An evaluation of air quality, home heating and well-being under Beijing’s programme to eliminate household coal use. Nat. Energy 2019, 4, 416–423. [Google Scholar] [CrossRef]
- Barron, A.R.; Fawcett, A.A.; Hafstead, M.A.C.; McFarland, J.R.; Morris, A.C. Policy insights from the emf 32 study on u.s. carbon tax scenarios. Clim. Chang. Econ. 2018, 9. [Google Scholar] [CrossRef]
- Basu, J.P. Agroforestry, climate change mitigation and livelihood security in India. N. Z. J. For. Sci. 2014, 44. [Google Scholar] [CrossRef]
- Berrueta, V.M.; Serrano-Medrano, M.; Garcia-Bustamante, C.; Astier, M.; Masera, O.R. Promoting sustainable local development of rural communities and mitigating climate change: The case of Mexico’s Patsari improved cookstove project. Clim. Chang. 2017, 140, 63–77. [Google Scholar] [CrossRef]
- Bilbao, B.A.; Leal, A.V.; Mendez, C.L. Indigenous Use of Fire and Forest Loss in Canaima National Park, Venezuela. Assessment of and Tools for Alternative Strategies of Fire Management in Pemn Indigenous Lands. Hum. Ecol. 2010, 38, 663–673. [Google Scholar] [CrossRef]
- Boyce, J.K.; Pastor, M. Clearing the air: Incorporating air quality and environmental justice into climate policy. Clim. Chang. 2013, 120, 801–814. [Google Scholar] [CrossRef]
- Breysse, J.; Jacobs, D.E.; Weber, W.; Dixon, S.; Kawecki, C.; Aceti, S.; Lopez, J. Health outcomes and green renovation of affordable housing. Public Health Rep. 2011, 126, 64–75. [Google Scholar] [CrossRef] [PubMed]
- Bubna-Litic, K.; Chalifour, N.J. Are climate change policies fair to vulnerable communities? The impact of British Columbia’s carbon tax and Australia’s carbon pricing policy on indigenous communities. Dalhous. Law J. 2012, 35, 127–178. [Google Scholar]
- Caillavet, F.; Fadhuile, A.; Nichele, V. Taxing animal-based foods for sustainability: Environmental, nutritional and social perspectives in France. Eur. Rev. Agric. Econ. 2016, 43, 537–560. [Google Scholar] [CrossRef]
- Champion, W.M.; Charley, P.H.; Klein, B.; Stewart, K.; Solomon, P.A.; Montoya, L.D. Perception, culture, and science: A framework to identify in-home heating options to improve indoor air quality in the Navajo Nation. Sci. Total Environ. 2017, 580, 297–306. [Google Scholar] [CrossRef]
- Chapman, R.; Howden-Chapman, P.; Viggers, H.; O’Dea, D.; Kennedy, M. Retrofitting houses with insulation: A cost-benefit analysis of a randomised community trial. J. Epidemiol. Community Health 2009, 63, 271–277. [Google Scholar] [CrossRef]
- Cushing, L.; Blaustein-Rejto, D.; Wander, M.; Pastor, M.; Sadd, J.; Zhu, A.; Morello-Frosch, R. Carbon trading, co-pollutants, and environmental equity: Evidence from California’s cap-and-trade program (2011–2015). PLoS Med. 2018, 15. [Google Scholar] [CrossRef]
- Dyer, G.A.; Matthews, R.; Meyfroidt, P. Is There an Ideal REDD plus Program? An Analysis of Policy Trade-Offs at the Local Level. PLoS ONE 2012, 7. [Google Scholar] [CrossRef]
- Feng, K.; Hubacek, K.; Guan, D.; Contestabile, M.; Minx, J.; Barrett, J. Distributional Effects of Climate Change Taxation: The Case of the UK. Environ. Sci. Technol. 2010, 44, 3670–3676. [Google Scholar] [CrossRef]
- Garg, A. Pro-equity Effects of Ancillary Benefits of Climate Change Policies: A Case Study of Human Health Impacts of Outdoor Air Pollution in New Delhi. World Dev. 2011, 39, 1002–1025. [Google Scholar] [CrossRef]
- Ji, S.; Cherry, C.R.; Zhou, W.; Sawhney, R.; Wu, Y.; Cai, S.; Wang, S.; Marshall, J.D. Environmental Justice Aspects of Exposure to PM2.5 Emissions from Electric Vehicle Use in China. Environ. Sci. Technol. 2015, 49, 13912–13920. [Google Scholar] [CrossRef]
- Khatun, K.; Gross-Camp, N.; Corbera, E.; Martin, A.; Ball, S.; Massao, G. When Participatory Forest Management makes money: Insights from Tanzania on governance, benefit sharing, and implications for REDD+. Environ. Plan. A Econ. Space 2015, 47, 2097–2112. [Google Scholar] [CrossRef]
- Krause, T.; Collen, W.; Nicholas, K.A. Evaluating Safeguards in a Conservation Incentive Program: Participation, Consent, and Benefit Sharing in Indigenous Communities of the Ecuadorian Amazon. Ecol. Soc. 2013, 18. [Google Scholar] [CrossRef]
- Li, Y.; Shi, X.; Su, B. Economic, social and environmental impacts of fuel subsidies: A revisit of Malaysia. Energy Policy 2017, 110, 51–61. [Google Scholar] [CrossRef]
- Lindsay, G.; Macmillan, A.; Woodward, A. Moving urban trips from cars to bicycles: Impact on health and emissions. Aust. N. Z. J. Public Health 2011, 35, 54–60. [Google Scholar] [CrossRef]
- Ni Mhurchu, C.; Eyles, H.; Genc, M.; Scarborough, P.; Rayner, M.; Mizdrak, A.; Nnoaham, K.; Blakely, T. Effects of Health-Related Food Taxes and Subsidies on Mortality from Diet-Related Disease in New Zealand: An Econometric-Epidemiologic Modelling Study. PLoS ONE 2015, 10, e0128477. [Google Scholar] [CrossRef]
- Reynolds, C.J.; Horgan, G.W.; Whybrow, S.; Macdiarmid, J.I. Healthy and sustainable diets that meet greenhouse gas emission reduction targets and are affordable for different income groups in the UK. Public Health Nutr. 2019, 22, 1503–1517. [Google Scholar] [CrossRef]
- Richards, G.; Frehs, J.; Myers, E.; Van Bibber, M. The Climate Change and Health Adaptation Program: Indigenous climate leaders’ championing adaptation efforts. Health Promot. Chronic Dis. Prev. Can. Res. Policy Pract. 2019, 39, 127–130. [Google Scholar] [CrossRef]
- Richardson, M.J.; English, P.; Rudolph, L. A health impact assessment of California’s proposed cap-and-trade regulations. Am. J. Public Health 2012, 102, e52–e58. [Google Scholar] [CrossRef]
- Sanchez, A.; Izzo, M. Micro hydropower: An alternative for climate change mitigation, adaptation, and development of marginalized local communities in Hispaniola Island. Clim. Chang. 2017, 140, 79–87. [Google Scholar] [CrossRef]
- Shammin, M.R.; Bullard, C.W. Impact of cap-and-trade policies for reducing greenhouse gas emissions on US households. Ecol. Econ. 2009, 68, 2432–2438. [Google Scholar] [CrossRef]
- Shrubsole, C.; Taylor, J.; Das, P.; Hamilton, I.G.; Oikonomou, E.; Davies, M. Impacts of energy efficiency retrofitting measures on indoor PM2.5 concentrations across different income groups in England: A modelling study. Adv. Build. Energy Res. 2016, 10, 69–83. [Google Scholar] [CrossRef]
- Sikka, M.; Thornton, T.F.; Worl, R. Sustainable Biomass Energy and Indigenous Cultural Models of Wellbeing in an Alaska Forest Ecosystem. Ecol. Soc. 2013, 18. [Google Scholar] [CrossRef]
- Sovacool, B.K. Fuel poverty, affordability, and energy justice in England: Policy insights from the Warm Front Program. Energy 2015, 93, 361–371. [Google Scholar] [CrossRef]
- Sunderlin, W.D.; de Sassi, C.; Ekaputri, A.D.; Light, M.; Pratama, C.D. REDD plus Contribution to Well-Being and Income Is Marginal: The Perspective of Local Stakeholders. Forests 2017, 8, 125. [Google Scholar] [CrossRef]
- Tainio, M.; Monsivais, P.; Jones, N.R.V.; Brand, C.; Woodcock, J. Mortality, greenhouse gas emissions and consumer cost impacts of combined diet and physical activity scenarios: A health impact assessment study. BMJ Open 2017, 7. [Google Scholar] [CrossRef]
- Williams, M.L.; Lott, M.C.; Kitwiroon, N.; Dajnak, D.; Walton, H.; Holland, M.; Pye, S.; Fecht, D.; Toledano, M.B.; Beevers, S.D. The Lancet Countdown on health benefits from the UK Climate Change Act: A modelling study for Great Britain. Lancet Planet. Health 2018, 2, e202–e213. [Google Scholar] [CrossRef]
- Winkler, H. Reducing energy poverty through carbon tax revenues in South Africa. J. Energy S. Afr. 2017, 28, 12–26. [Google Scholar] [CrossRef]
- Woodcock, J.; Abbas, A.; Ullrich, A.; Tainio, M.; Lovelace, R.; Sa, T.H.; Westgate, K.; Goodman, A. Development of the Impacts of Cycling Tool (ICT): A modelling study and web tool for evaluating health and environmental impacts of cycling uptake. PLoS Med. 2018, 15. [Google Scholar] [CrossRef]
- Raworth, K. Doughnut Economics: Seven Ways to Think Like a 21st-Century Economist; Random House Business Books: London, UK, 2017. [Google Scholar]
- Stiglitz, J.E. Where modern macroeconomics went wrong. Oxf. Rev. Econ. Policy 2018, 34, 70–106. [Google Scholar] [CrossRef]
- United Nations. United Nations Declaration on the Rights of Indigenous Peoples; United Nations, Ed.; United Nations: Geneva, Switzerland, 2008. [Google Scholar]
- Stein, S. The Ethical and Ecological Limits of Sustainability: A Decolonial Approach to Climate Change in Higher Education. Aust. J. Environ. Educ. 2019, 35, 198–212. [Google Scholar] [CrossRef]
- Brugnach, M.; Craps, M.; Dewulf, A. Including indigenous peoples in climate change mitigation: Addressing issues of scale, knowledge and power. Clim. Chang. 2017, 140, 19–32. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).