The Effects of Family Financial Stress and Primary Caregivers’ Levels of Acculturation on Children’s Emotional and Behavioral Problems among Humanitarian Refugees in Australia


Abstract
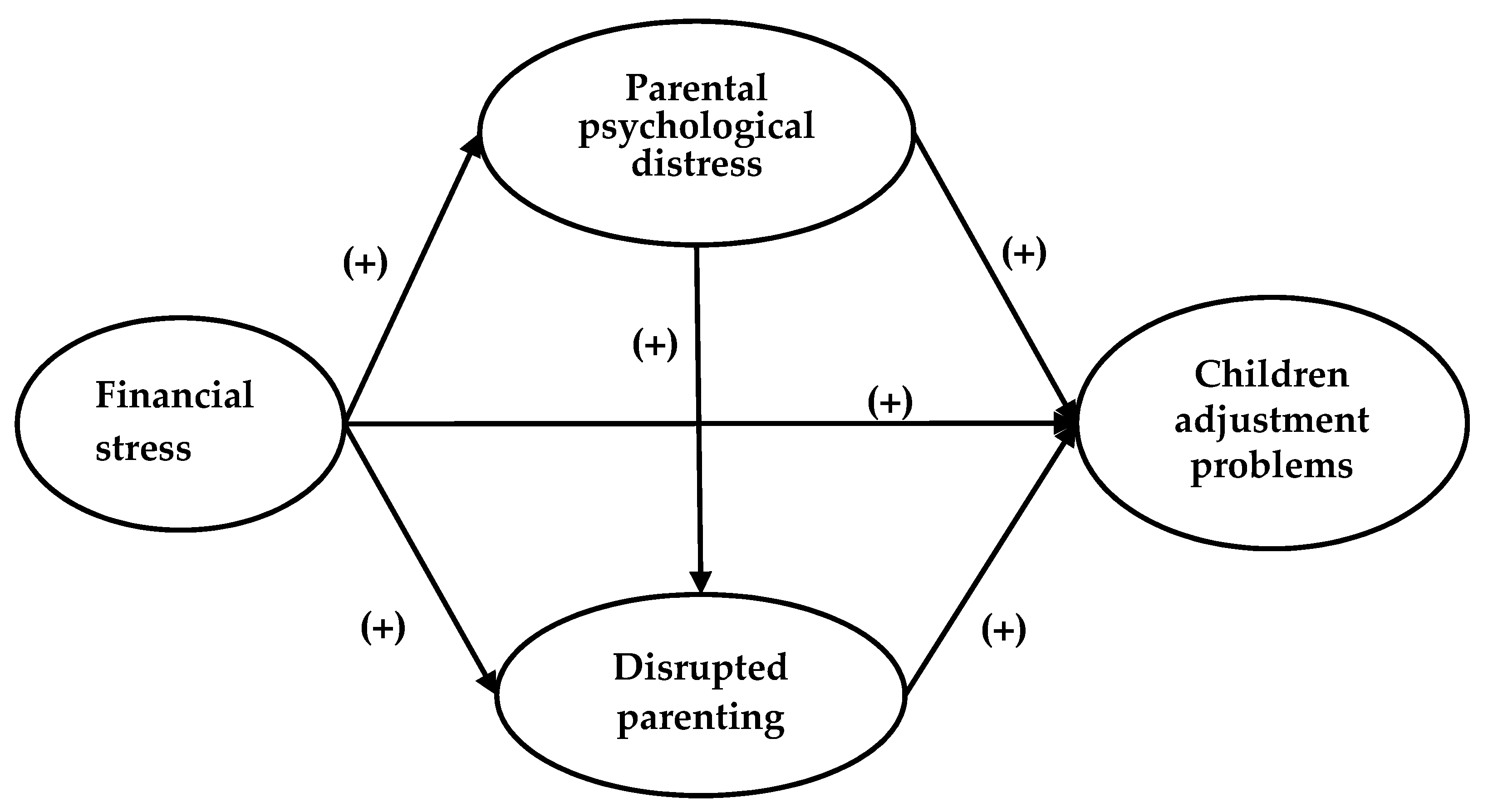
1. Introduction
2. Methods
2.1. Data Sources
2.2. Sampling and Study Participants
2.3. Measures
2.3.1. Children’s Emotional and Behavioral Problems
2.3.2. Family Financial Stress
2.3.3. Primary Caregivers’ Acculturation Level
2.3.4. Primary Caregivers’ Psychological Distress
2.3.5. Parenting Style
2.3.6. Covariates
2.4. Statistical Analyses
2.5. Ethics
3. Results
3.1. Descriptives
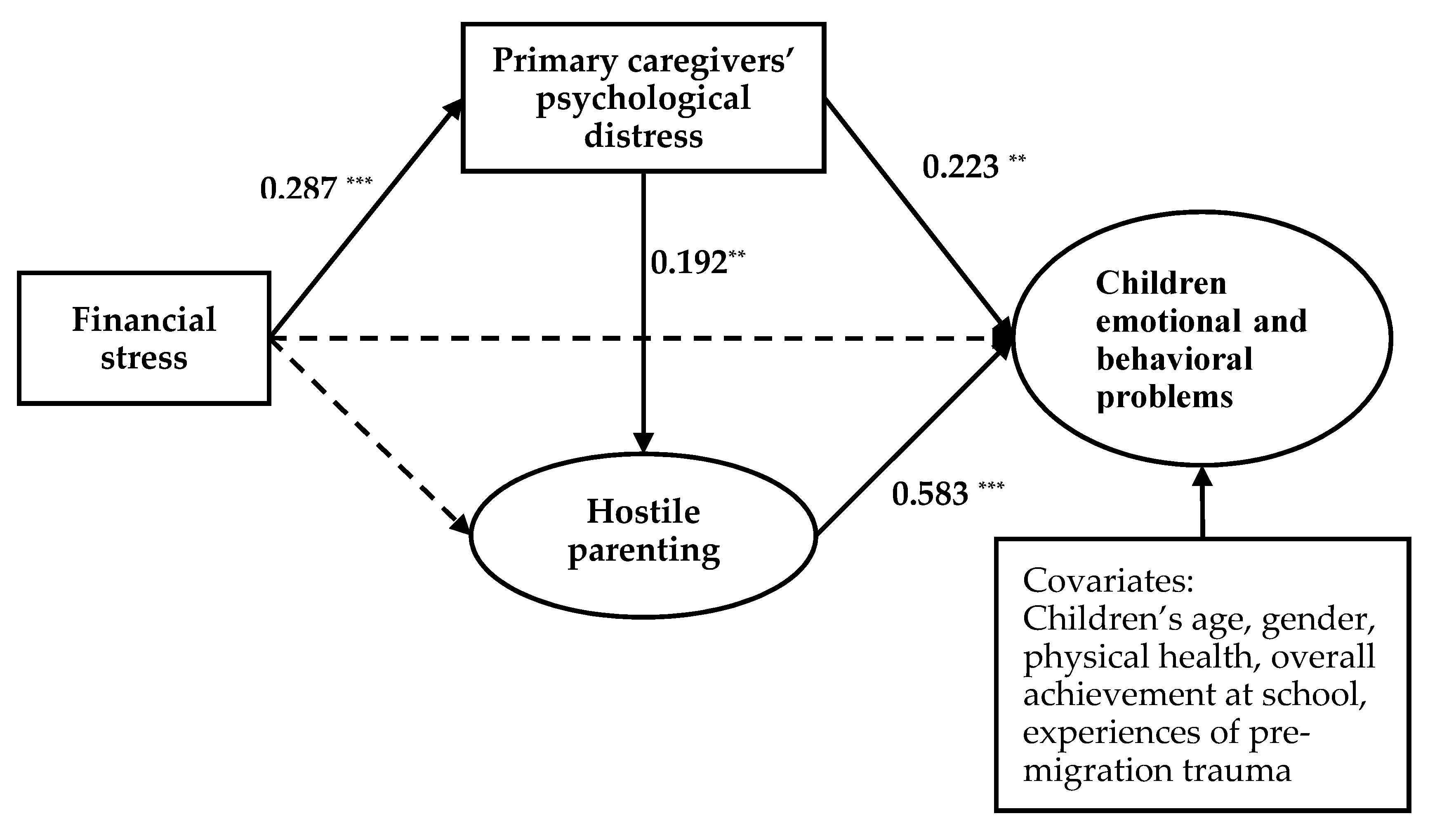
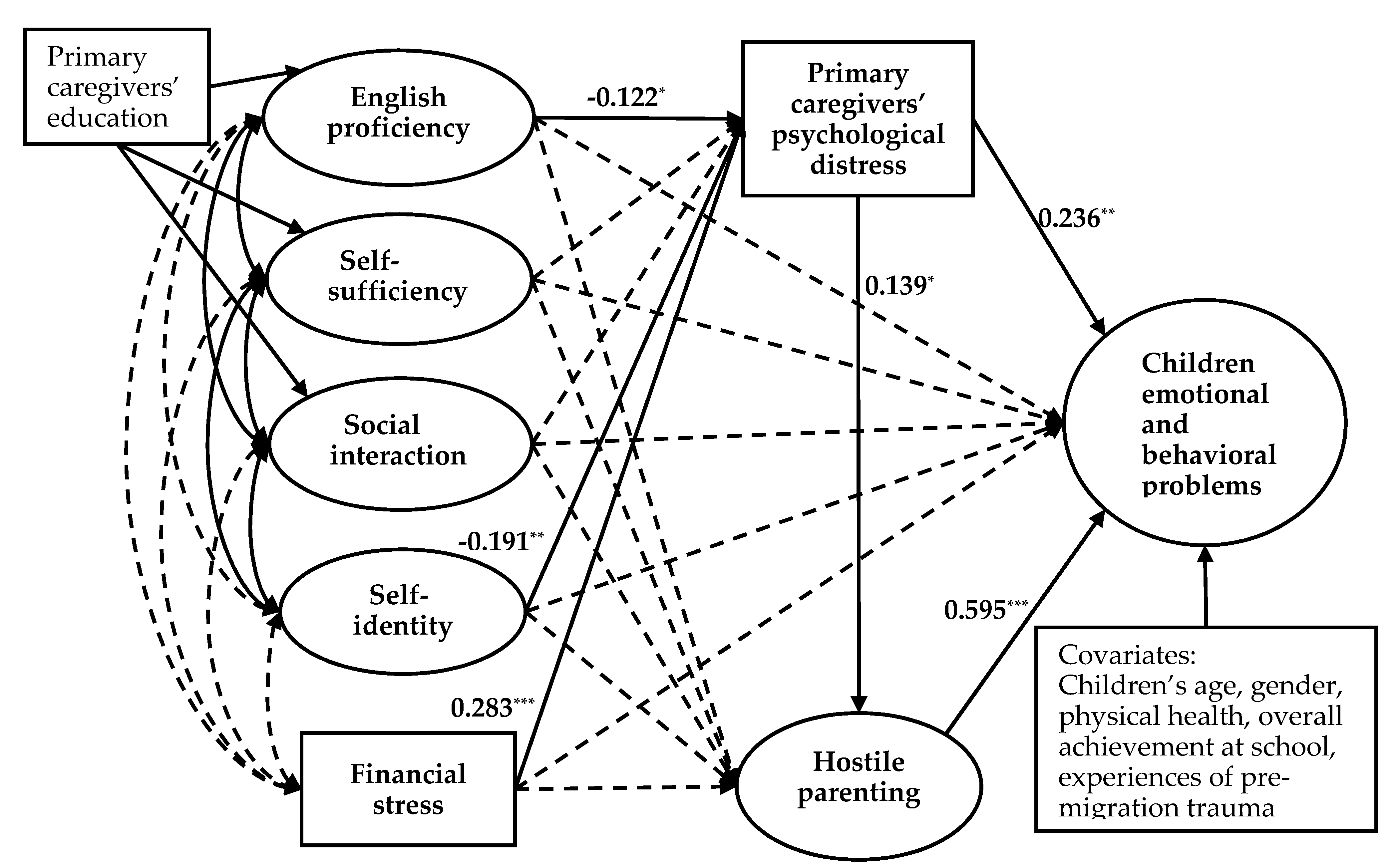
3.2. Multilevel Structural Equation Modeling Analysis
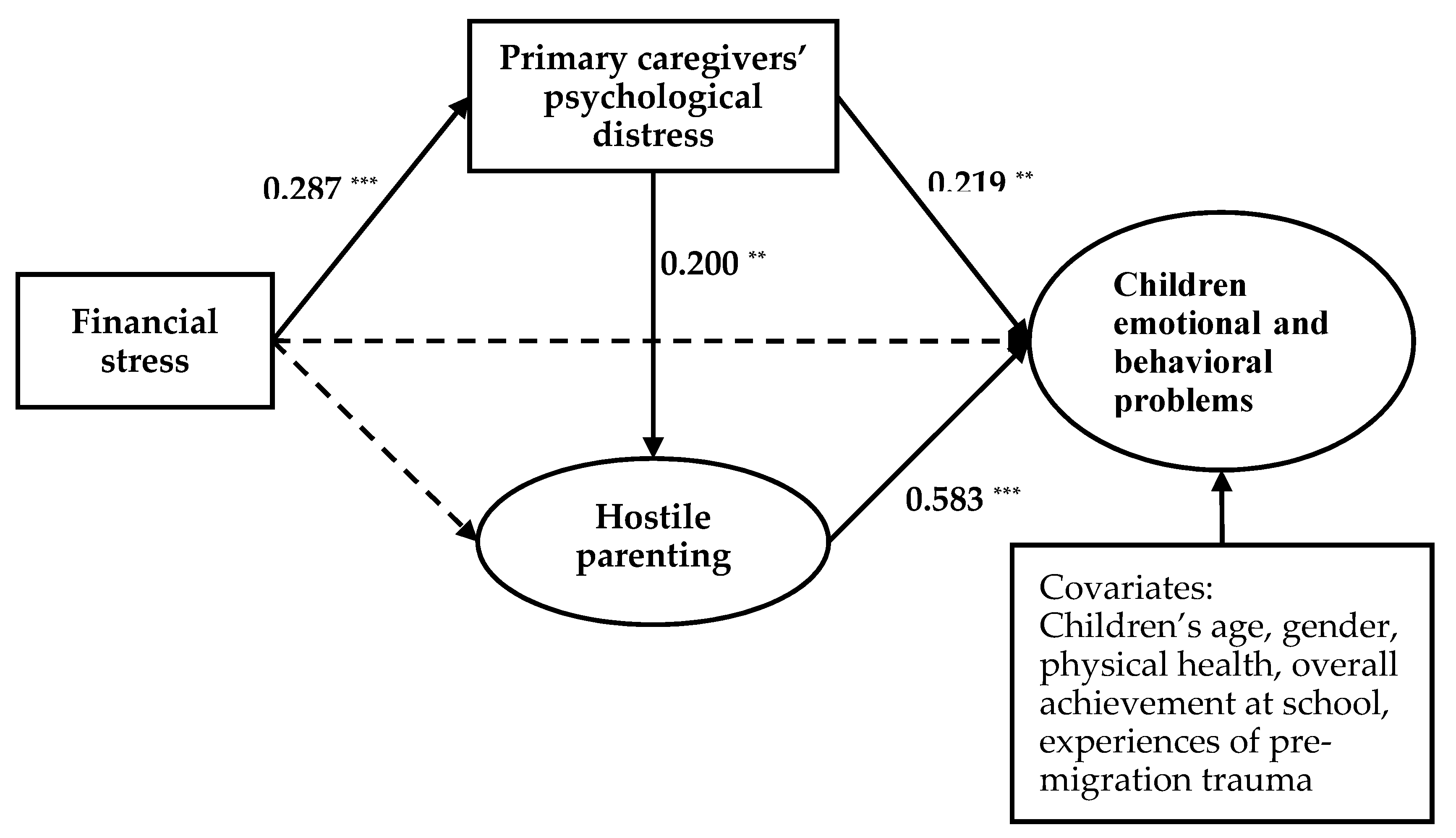
3.3. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primary Caregivers | Refugee Children | t | p | |
|---|---|---|---|---|
| Aged 11–17 (n = 482) | ||||
| Total difficulties score | 8.85 (5.49) | 8.97 (5.31) | 0.329 | 0.742 |
| Emotional symptoms score | 2.25 (2.24) | 2.62 (2.20) | 2.453 | 0.014 |
| Conduct problems score | 1.32 (1.54) | 1.45 (1.53) | 1.258 | 0.209 |
| Hyperactivity score | 2.85 (2.15) | 2.55 (1.71) | −2.342 | 0.019 |
| Peer problems score | 2.42 (1.50) | 2.36 (1.67) | −0.558 | 0.577 |
| Variables | 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. |
|---|---|---|---|---|---|---|---|---|---|
| 1. Financial stress | 1.000 | ||||||||
| 2. English proficiency | −0.002 | 1.000 | |||||||
| 3. Self-sufficiency | 0.019 | 0.490 *** | 1.000 | ||||||
| 4. Social interaction | 0.072 | 0.323 *** | 0.538 *** | 1.000 | |||||
| 5. Self-identity | −0.035 | 0.037 | 0.180 ** | 0.273 *** | 1.000 | ||||
| 6. Psychological distress | 0.290 *** | −0.139 ** | −0.070 | −0.133 * | −0.206 ** | 1.000 | |||
| 7. Warm parenting | −0.061 | 0.215 ** | 0.223 ** | 0.255 ** | 0.244 ** | −0.056 | 1.000 | ||
| 8. Hostile parenting | 0.084 | −0.071 | −0.103 | −0.176 * | −0.226 ** | 0.185 ** | −0.198 | 1.000 | |
| 9. Emotional and behavioral problems | 0.148 * | −0.138 * | −0.116 | −0.178 ** | −0.092 | 0.355 *** | −0.152 | 0.565 *** | 1.000 |
| Pathways | β | 95% CI | |
|---|---|---|---|
| Lower | Upper | ||
| Extended FSM | |||
| Family financial stress | |||
| a. Financial stress → Psychological distress → Hostile parenting → Children’s emotional and behavioral problems | 0.023 | 0.002 | 0.054 |
| b. Financial stress → Psychological distress → Children’s emotional and behavioral problems | 0.060 | 0.016 | 0.119 |
| c. Financial stress → Hostile parenting → Children’s emotional and behavioral problems | 0.033 | -0.040 | 0.117 |
| English proficiency | |||
| a. English proficiency → Psychological distress → Hostile parenting → Children’s emotional and behavioral problems | −0.025 | −0.071 | 0.001 |
| b. English proficiency → Psychological distress → Children’s emotional and behavioral problems | −0.065 | −0.165 | −0.0001 |
| c. English proficiency → Hostile parenting → Children’s emotional and behavioral problems | −0.020 | −0.218 | 0.179 |
| Self-sufficiency | |||
| a. Self-sufficiency → Psychological distress → Hostile parenting → Children’s emotional and behavioral problems | 0.015 | −0.020 | 0.066 |
| b. Self-sufficiency → Psychological distress → Children’s emotional and behavioral problems | 0.039 | −0.052 | 0.153 |
| c. Self-sufficiency → Hostile parenting → Children’s emotional and behavioral problems | 0.061 | −0.181 | 0.325 |
| Social interaction | |||
| a. Social interaction → Psychological distress → Hostile parenting → Children’s emotional and behavioral problems | −0.025 | −0.099 | 0.026 |
| b. Social interaction → Psychological distress → Children’s emotional and behavioral problems | −0.065 | −0.237 | 0.068 |
| c. Social interaction → Hostile parenting → Children’s emotional and behavioral problems | −0.216 | −0.592 | 0.105 |
| Self-identity | |||
| a. Self-identity → Psychological distress → Hostile parenting → Children’s emotional and behavioral problems | −0.052 | −0.136 | −0.004 |
| b. Self-identity → Psychological distress → Children’s emotional and behavioral problems | −0.139 | −0.311 | −0.023 |
| c. Self-identity → Hostile parenting → Children’s emotional and behavioral problems | −0.276 | −0.653 | 0.034 |
References
- United Nations High Commissioner for Refugees. Global trends: Forced displacement in 2018. Available online: https://www.unhcr.org/globaltrends2018/ (accessed on 20 June 2019).
- Kien, C.; Sommer, I.; Faustmann, A.; Gibson, L.; Schneider, M.; Krczal, E.; Jank, R.; Klerings, I.; Szelag, M.; Kerschner, B.; et al. Prevalence of mental disorders in young refugees and asylum seekers in European Countries: A systematic review. Eur. Child Adolesc. Psychiatry 2019, 28, 1295–1310. [Google Scholar] [CrossRef] [PubMed]
- Stolk, Y.; Kaplan, I.; Szwarc, J. Review of the strengths and difficulties questionnaire translated into languages spoken by children and adolescents of refugee background. Int. J. Methods Psychiatr. Res. 2017, 26. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, A.; Flouri, E.; Ten Brinke, J. Emotional and behavioural problems in childhood and distress in adult life: Risk and protective factors. Aust. N. Z. J. Psychiatry 2002, 36, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Narusyte, J.; Ropponen, A.; Alexanderson, K.; Svedberg, P. Internalizing and externalizing problems in childhood and adolescence as predictors of work incapacity in young adulthood. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Letourneau, N.; Duffett-Leger, L.; Levac, L.; Watson, B.; Young, C. Socioeconomic Status and Child Development A Meta-Analysis. J. Emot. Behav. Disord. 2013, 21, 211–224. [Google Scholar] [CrossRef]
- Cobham, V.E.; McDermott, B.; Haslam, D.; Sanders, M.R. The Role of Parents, Parenting and the Family Environment in Children’s Post-Disaster Mental Health. Curr. Psychiatry Rep. 2016, 18, 53. [Google Scholar] [CrossRef]
- Repetti, R.L.; Taylor, S.E.; Seeman, T.E. Risky families: Family social environments and the mental and physical health of offspring. Psychol. Bull. 2002, 128, 330–366. [Google Scholar] [CrossRef]
- Bryant, R.A.; Edwards, B.; Creamer, M.; O’Donnell, M.; Forbes, D.; Felmingham, K.L.; Silove, D.; Steel, Z.; Nickerson, A.; McFarlane, A.C.; et al. The effect of post-traumatic stress disorder on refugees’ parenting and their children’s mental health: A cohort study. Lancet Public Health 2018, 3, e249–e258. [Google Scholar] [CrossRef]
- Eruyar, S.; Maltby, J.; Vostanis, P. Mental health problems of Syrian refugee children: The role of parental factors. Eur. Child Adolesc. Psychiatry 2018, 27, 401–409. [Google Scholar] [CrossRef]
- Conger, R.D.; Ge, X.; Elder, G.H.; Lorenz, F.O.; Simons, R.L. Economic stress, coercive family process, and developmental problems of adolescents. Child Dev. 1994, 65, 541–561. [Google Scholar] [CrossRef]
- Mistry, R.S.; Vandewater, E.A.; Huston, A.C.; McLoyd, V.C. Economic well-being and children’s social adjustment: The role of family process in an ethnically diverse low-income sample. Child Dev. 2002, 73, 935–951. [Google Scholar] [CrossRef] [PubMed]
- Barajas-Gonzalez, R.G.; Brooks-Gunn, J. Income, neighborhood stressors, and harsh parenting: Test of moderation by ethnicity, age, and gender. J. Fam. Psychol. 2014, 28, 855–866. [Google Scholar] [CrossRef] [PubMed]
- Betancourt, T.S.; Abdi, S.; Ito, B.S.; Lilienthal, G.M.; Agalab, N.; Ellis, H. We left one war and came to another: Resource loss, acculturative stress, and caregiver-child relationships in Somali refugee families. Cult. Divers. Ethnic Minor. Psychol. 2015, 21, 114–125. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Wu, S.; Ling, L.; Renzaho, A.M.N. Impacts of social integration and loneliness on mental health of humanitarian migrants in Australia: Evidence from a longitudinal study. Aust. N. Z. J. Public Health 2019, 43, 46–55. [Google Scholar] [CrossRef]
- Gibson, M.A. Immigrant Adaptation and Patterns of. Hum. Dev. 2001, 44, 19–23. [Google Scholar] [CrossRef]
- Ho, G.W. Acculturation and its implications on parenting for Chinese immigrants: A systematic review. J. Transcult. Nurs. 2014, 25, 145–158. [Google Scholar] [CrossRef]
- Nguyen, P.V. Perceptions of Vietnamese fathers’ acculturation levels, parenting styles, and mental health outcomes in Vietnamese American adolescent immigrants. Soc. Work 2008, 53, 337–346. [Google Scholar] [CrossRef]
- Rogler, L.H.; Cortes, D.E.; Malgady, R.G. Acculturation and mental health status among Hispanics. Convergence and new directions for research. Am. Psychol. 1991, 46, 585–597. [Google Scholar] [CrossRef]
- Gorden, M.M. Assimilation in American life. New York: Oxford University Press. Greenleaf, RK (1991). The servant as leader. Indianapolis: The Robert K. Greenleaf Center. Griffith, J.(2000). School climate as group evaluation and group consensus: Student and parent perceptions of the elementary school environment. Elem. Sch. J. 1964, 101, 35–61. [Google Scholar]
- Berry, J.W. Immigration, Acculturation, and Adaptation. Appl. Psychol. 1997, 46, 5–34. [Google Scholar] [CrossRef]
- Shin, C.N.; Todd, M.; An, K.; Kim, W.S. Unidimensional and Bidimensional Approaches to Measuring Acculturation. J. Nurs. Meas. 2017, 25, 370–384. [Google Scholar] [CrossRef] [PubMed]
- Matsudaira, T. Measures of psychological acculturation: A review. Transcult. Psychiatry 2006, 43, 462–487. [Google Scholar] [CrossRef] [PubMed]
- Kartal, D.; Alkemade, N.; Eisenbruch, M.; Kissane, D. Traumatic exposure, acculturative stress and cultural orientation: The influence on PTSD, depressive and anxiety symptoms among refugees. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 931–941. [Google Scholar] [CrossRef] [PubMed]
- Australian Department of Social Services. Building a New Life in Australia (BNLA): The Longitudinal Study of Humanitarian Migrants. Available online: https://www.dss.gov.au/about-the-department/national-centre-for-longitudinal-data/building-a-new-life-in-australia-the-longitudinal-study-of-humanitarian-migrants (accessed on 14 April 2020).
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Renzaho, A.; Mellor, D.; McCabe, M.; Powell, M. Family Functioning, Parental Psychological Distress and Child Behaviours: Evidence from the Victorian Child Health and Wellbeing Study. Aust. Psychol. 2013, 48, 217–225. [Google Scholar] [CrossRef][Green Version]
- Renzaho, A.M.; Karantzas, G. Effects of parental perception of neighbourhood deprivation and family environment characteristics on pro-social behaviours among 4–12 year old children. Aust. N. Z. J. Public Health 2010, 34, 405–411. [Google Scholar] [CrossRef]
- Chen, W.; Ling, L.; Renzaho, A.M. Building a new life in Australia: An analysis of the first wave of the longitudinal study of humanitarian migrants in Australia to assess the association between social integration and self-rated health. BMJ Open 2017, 7, e014313. [Google Scholar] [CrossRef]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Kessler, R.C.; Slade, T.; Andrews, G. The performance of the K6 and K10 screening scales for psychological distress in the Australian National Survey of Mental Health and Well-Being. Psychol. Med. 2003, 33, 357–362. [Google Scholar] [CrossRef]
- Paterson, G.; Sanson, A. The Association of Behavioural Adjustment to Temperament, Parenting and Family Characteristics among 5-Year-Old Children. Soc. Dev. 1999, 8, 293–309. [Google Scholar] [CrossRef]
- US Department of Education. US Childhood Longitudinal Study, Birth Cohort; National Center for Education Statistics: Washington, DC, USA, 2001.
- MacKinnon, D.P.; Valente, M.J. Mediation from multilevel to structural equation modeling. Ann. Nutr. Metab. 2014, 65, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F.; Preacher, K.J.; Myers, T.A. Mediation and the estimation of indirect effects in political communication research. Sourceb. Political Commun. Res. Methods Meas. Anal. Tech. 2011, 23, 434–465. [Google Scholar]
- Amrock, S.M.; Weitzman, M. Parental psychological distress and children’s mental health: Results of a national survey. Acad. Pediatr. 2014, 14, 375–381. [Google Scholar] [CrossRef]
- Wickham, S.; Whitehead, M.; Taylor-Robinson, D.; Barr, B. The effect of a transition into poverty on child and maternal mental health: A longitudinal analysis of the UK Millennium Cohort Study. Lancet Public Health 2017, 2, e141–e148. [Google Scholar] [CrossRef]
- Yeung, W.J.; Linver, M.R.; Brooks-Gunn, J. How money matters for young children’s development: Parental investment and family processes. Child Dev. 2002, 73, 1861–1879. [Google Scholar] [CrossRef] [PubMed]
- Duncan, G.J.; Magnuson, K.; Votruba-Drzal, E. Boosting family income to promote child development. Future Child. 2014, 24, 99–120. [Google Scholar] [CrossRef] [PubMed]
- Masarik, A.S.; Conger, R.D. Stress and child development: A review of the Family Stress Model. Curr. Opin. Psychol. 2017, 13, 85–90. [Google Scholar] [CrossRef]
- Liu, L.L.; Lau, A.S.; Chen, A.C.; Dinh, K.T.; Kim, S.Y. The influence of maternal acculturation, neighborhood disadvantage, and parenting on Chinese American adolescents’ conduct problems: Testing the segmented assimilation hypothesis. J. Youth Adolesc. 2009, 38, 691–702. [Google Scholar] [CrossRef]
- De Vroome, T.; Coenders, M.; Van Tubergen, F.; Verkuyten, M. Economic participation and national self-identification of refugees in the Netherlands. Int. Migr. Rev. 2011, 45, 615–638. [Google Scholar] [CrossRef]
- Lopez-Class, M.; Castro, F.G.; Ramirez, A.G. Conceptions of acculturation: A review and statement of critical issues. Soc. Sci. Med. 2011, 72, 1555–1562. [Google Scholar] [CrossRef]
- White, R.M.; Roosa, M.W.; Weaver, S.R.; Nair, R.L. Cultural and Contextual Influences on Parenting in Mexican American Families. J. Marriage Fam. 2009, 71, 61. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.H.; Hua, M.; Zhou, Q.; Tao, A.; Lee, E.H.; Ly, J.; Main, A. Parent-child cultural orientations and child adjustment in Chinese American immigrant families. Dev. Psychol. 2014, 50, 189–201. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.L.; Benner, A.D.; Lau, A.S.; Kim, S.Y. Mother-adolescent language proficiency and adolescent academic and emotional adjustment among Chinese American families. J. Youth Adolesc. 2009, 38, 572–586. [Google Scholar] [CrossRef] [PubMed]
- Ying, Y.W.; Han, M. Parental acculturation, parental involvement, intergenerational relationship and adolescent outcomes in immigrant Filipino American families. J. Immigr. Refug. Stud. 2008, 6, 112–131. [Google Scholar] [CrossRef]
- Zhang, W.; Hong, S.; Takeuchi, D.T.; Mossakowski, K.N. Limited English proficiency and psychological distress among Latinos and Asian Americans. Soc. Sci. Med. 2012, 75, 1006–1014. [Google Scholar] [CrossRef]
- Kim, G.; Aguado Loi, C.X.; Chiriboga, D.A.; Jang, Y.; Parmelee, P.; Allen, R.S. Limited English proficiency as a barrier to mental health service use: A study of Latino and Asian immigrants with psychiatric disorders. J. Psychiatr. Res. 2011, 45, 104–110. [Google Scholar] [CrossRef]
- Australian Department of Social Services. Beginning a Life in Australia. Available online: https://immi.homeaffairs.gov.au/settlement-services-subsite/files/beginning-a-life-in-australia-english.pdf (accessed on 14 April 2020).
- Silove, D.; Ventevogel, P.; Rees, S. The contemporary refugee crisis: An overview of mental health challenges. World Psychiatry 2017, 16, 130–139. [Google Scholar] [CrossRef]
- Martinez, C.R.; Eddy, J.M. Effects of culturally adapted parent management training on Latino youth behavioral health outcomes. J. Consult. Clin. Psychol. 2005, 73, 841–851. [Google Scholar] [CrossRef]
- Schwartz, S.J.; Unger, J.B.; Zamboanga, B.L.; Szapocznik, J. Rethinking the concept of acculturation: Implications for theory and research. Am. Psychol. 2010, 65, 237–251. [Google Scholar] [CrossRef]



| Variables | Mean (SD)/n (%) | Cronbach’s | Range/Valuation | Missing Value/n |
|---|---|---|---|---|
| Level-1 (n = 658) | ||||
| Children’s emotional and behavioral problems | 0.71 | |||
| SDQ total difficulties score | 9.03 (5.60) | 0–29 | 0 | |
| SDQ emotional symptoms score | 2.24 (2.25) | 0–10 | 0 | |
| SDQ conduct problems score | 1.38 (1.57) | 0–10 | 0 | |
| SDQ hyperactivity score | 3.02 (2.19) | 0–10 | 0 | |
| SDQ peer problems score | 2.40 (1.55) | 0–8 | 0 | |
| Parenting style | ||||
| Warm parenting | 0.75 | |||
| Has warm close times with child | 4.34 (0.88) | 1 = never/almost never; 2 = rarely; 3 = sometimes; 4 = often; 5 = always/almost always. | 17 | |
| Enjoys doing things with and listening to child | 4.33 (0.86) | 22 | ||
| Talk about what is going on in their life | 3.56 (1.30) | 34 | ||
| Is good at getting child to do what is told | 3.75 (1.20) | 33 | ||
| Feels close to child when child is happy and upset | 4.21 (1.07) | 30 | ||
| Hostile parenting | 0.73 | |||
| Has been angry with child | 2.05 (1.06) | 1 = never/almost never; 2 = rarely; 3 = sometimes; 4 = often; 5 = always/almost always. | 28 | |
| Has raised voice or shouted at child | 1.98 (0.97) | 28 | ||
| Gets on my nerves when child cries | 2.28 (1.35) | 38 | ||
| Has lost temper with child | 1.58 (0.93) | 27 | ||
| Has left child alone in bedroom when upset | 1.44 (0.92) | 29 | ||
| Level-2 (n = 410) | ||||
| Primary caregivers’ acculturation level | 0.91 | |||
| English proficiency | 0.94 | |||
| Understand spoken English | 2.20 (0.71) | 1 = not at all; 2 = not well; 3 = well; 4 = very well. | 11 | |
| Speak English | 2.04 (0.74) | 6 | ||
| Read English | 2.15 (0.82) | 7 | ||
| Write English | 2.07 (0.77) | 8 | ||
| Self-sufficiency to participate in the life in Australia | 0.92 | |||
| Look for a job | 1.76 (0.92) | 1 = would not know at all; 2 = would know a little; 3 = would know fairly well; 4 = would know very well. | 4 | |
| Find a school or childcare for children | 2.31 (1.04) | 22 | ||
| Use public transport | 2.93 (1.04) | 4 | ||
| Get help in an emergency | 2.68 (1.06) | 3 | ||
| Use bank services | 2.23 (1.08) | 4 | ||
| Find out what government services and benefits are available | 2.30 (1.04) | 4 | ||
| Find out about your rights | 2.24 (1.05) | 4 | ||
| Get help from the police | 2.59 (1.09) | 3 | ||
| Social interaction | 0.80 | |||
| Make friends in Australia | 2.51 (0.76) | 1 = very hard; 2 = hard; 3 = easy; 4 = very easy. | 23 | |
| Understand Australian ways/culture | 2.53 (0.76) | 20 | ||
| Talk to Australian neighbors | 2.30 (0.81) | 27 | ||
| Self-identity | 0.54 | |||
| Feel welcome in Australia | 3.57 (0.67) | 1 = hardly ever; 2 = some of the time; 3 = most of the time; 4 = always. | 3 | |
| Feel part of the Australian community | 3.38 (0.86) | 2 | ||
| Experience discrimination in Australia n (%) | 2 | |||
| Yes | 24 (5.85) | |||
| No | 384 (93.66) | |||
| Financial stress | 1.22 (1.51) | 0–6 | 5 | |
| Psychological distress | 14.31 (6.01) | 0.90 | 6–30 | 8 |
| Characteristics | n (%) | Mean (SD) |
|---|---|---|
| Primary caregivers’ characteristics (n = 410) | ||
| Age (years) | 40.1 (8.8) | |
| Gender | ||
| Male | 98 (23.9) | |
| Female | 312 (76.1) | |
| Years of education | ||
| Never attended school | 93 (22.7) | |
| ≤6 years of schooling | 80 (19.8) | |
| ≥7 years of schooling | 175 (43.2) | |
| Trade or technical qualification beyond school | 21 (5.2) | |
| University degree | 36 (8.9) | |
| Household structure | ||
| Single parent family | 103 (25.1) | |
| Couple family | 301 (73.4) | |
| Children’s characteristics (n = 658) | ||
| Age (years) | 12.0 (3.5) | |
| Gender | ||
| Male | 354 (53.8) | |
| Female | 304 (46.2) | |
| Physical health | 4.1 (1.0) | |
| Poor | 16 (2.4) | |
| Fair | 31 (4.7) | |
| Good | 125 (19.0) | |
| Very good | 218 (33.1) | |
| Excellent | 266 (40.4) | |
| Overall achievement at school | 3.8 (1.0) | |
| Below average | 39 (5.9) | |
| Average | 252 (38.3) | |
| Above average | 172 (26.1) | |
| Excellent | 186 (28.3) | |
| Experiences of pre-migration trauma | ||
| Yes | 189 (28.7) | |
| No | 457 (69.5) |
| Model | χ2 | d.f. | χ2/d.f. | CFI | TLI | RMSEA | SRMR |
|---|---|---|---|---|---|---|---|
| Basic FSM | 242.442 | 105 | 2.309 | 0.880 | 0.844 | 0.045 | 0.079 |
| Extended FSM | 751.0455 | 437 | 1.720 | 0.939 | 0.928 | 0.034 | 0.062 |
| Pathways | 95% CI | ||
|---|---|---|---|
| Lower | Upper | ||
| Extended FSM | |||
| Family financial stress | |||
| a. Financial stress → Psychological distress → Hostile parenting → Children’s emotional and behavioral problems | 0.021 | 0.001 | 0.053 |
| b. Financial stress → Psychological distress → Children’s emotional and behavioral problems | 0.061 | 0.016 | 0.119 |
| c. Financial stress → Hostile parenting → Children’s emotional and behavioral problems | 0.037 | −0.038 | 0.125 |
| English proficiency | |||
| a. English proficiency → Psychological distress → Hostile parenting → Children’s emotional and behavioral problems | −0.023 | −0.071 | 0.002 |
| b. English proficiency → Psychological distress → Children’s emotional and behavioral problems | −0.067 | −0.165 | −0.001 |
| c. English proficiency → Hostile parenting → Children’s emotional and behavioral problems | −0.034 | −0.238 | 0.165 |
| Self-sufficiency | |||
| a. Self-sufficiency → Psychological distress → Hostile parenting → Children’s emotional and behavioral problems | 0.014 | −0.020 | 0.065 |
| b. Self-sufficiency → Psychological distress → Children’s emotional and behavioral problems | 0.039 | −0.053 | 0.153 |
| c. Self-sufficiency → Hostile parenting → Children’s emotional and behavioral problems | 0.058 | −0.184 | 0.324 |
| Social interaction | |||
| a. Social interaction → Psychological distress → Hostile parenting → Children’s emotional and behavioral problems | −0.023 | −0.097 | 0.026 |
| b. Social interaction → Psychological distress → Children’s emotional and behavioral problems | −0.066 | −0.236 | 0.068 |
| c. Social interaction → Hostile parenting → Children’s emotional and behavioral problems | −0.225 | −0.603 | 0.094 |
| Self-identity | |||
| a. Self-identity → Psychological distress → Hostile parenting → Children’s emotional and behavioral problems | −0.049 | −0.136 | −0.001 |
| b. Self-identity → Psychological distress → Children’s emotional and behavioral problems | −0.141 | −0.312 | −0.023 |
| c. Self-identity → Hostile parenting → Children’s emotional and behavioral problems | −0.284 | −0.675 | 0.035 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, L.; Renzaho, A.M.N.; Shi, L.; Ling, L.; Chen, W. The Effects of Family Financial Stress and Primary Caregivers’ Levels of Acculturation on Children’s Emotional and Behavioral Problems among Humanitarian Refugees in Australia. Int. J. Environ. Res. Public Health 2020, 17, 2716. https://doi.org/10.3390/ijerph17082716
Yu L, Renzaho AMN, Shi L, Ling L, Chen W. The Effects of Family Financial Stress and Primary Caregivers’ Levels of Acculturation on Children’s Emotional and Behavioral Problems among Humanitarian Refugees in Australia. International Journal of Environmental Research and Public Health. 2020; 17(8):2716. https://doi.org/10.3390/ijerph17082716
Chicago/Turabian StyleYu, Linlin, Andre M.N. Renzaho, Lishuo Shi, Li Ling, and Wen Chen. 2020. "The Effects of Family Financial Stress and Primary Caregivers’ Levels of Acculturation on Children’s Emotional and Behavioral Problems among Humanitarian Refugees in Australia" International Journal of Environmental Research and Public Health 17, no. 8: 2716. https://doi.org/10.3390/ijerph17082716
APA StyleYu, L., Renzaho, A. M. N., Shi, L., Ling, L., & Chen, W. (2020). The Effects of Family Financial Stress and Primary Caregivers’ Levels of Acculturation on Children’s Emotional and Behavioral Problems among Humanitarian Refugees in Australia. International Journal of Environmental Research and Public Health, 17(8), 2716. https://doi.org/10.3390/ijerph17082716