1. Introduction
International students or foreign students are those who travel to another country for an educational reason [
1]. According to the United Nations Educational, Scientific and Cultural Organization (UNESCO), over 2.5 million students were enrolled outside their country of citizenship in 2009 and the number of international students might rise to approximately 7 million by the year 2020 [
2]. In recent years, except the main destination countries like the United States, the United Kingdom and Germany, Ireland is gradually becoming a country with rapid growth in the number of international students after New Zealand and the Netherlands [
3]. Based on the results of the 2006 Census in Ireland (23 April 2006), non-nationals made up 10% of the population in Ireland, and this figure was set to increase further in the coming years [
4].
Despite several advantages of studying abroad (i.e., advanced knowledge and multicultural horizons) [
5], dietary changes and health care problems are challenging and disturbing to international students. Dietary behavior played a major role in acculturation for international students [
6]. A qualitative study showed that most international students were unsatisfied with the local foods they consumed [
7]. Edwards et al. [
8] found that many international postgraduate students experienced food neophobia (i.e., the phenomenon of rejection to eat unfamiliar or unknown food) [
9] and the food neophobia scores were even increased after a three-month follow-up. The process of acculturation resulted in changes in health behavior, such as diet and drinking behavior, among international students [
7]. As a result, body weight might increase during dietary acculturation, which could potentially impact their health if the weight gain continued [
10]. Thus, it is important to pay attention to the dietary behavior and health of international students.
The concept of a healthy diet has been studied extensively and several methods of dietary assessment and healthy dietary patterns have been well developed, such as Mediterranean diet (MeDi), Dietary Approaches to Stop Hypertension (DASH), Healthy Diet Indicator (HDI), Healthy Eating Index (HEI) and so on [
11]. Furthermore, adolescent dietary guidelines also varied slightly among different regions. For instance, the World Health Organization (WHO) encouraged adolescents and young adults to consume five main food groups (i.e., grains, fruits and vegetables, milk and dairy food, meats, and fishes) [
12]. The American dietary guideline also recommended adolescents to consume limited solid fats, cholesterol, added sugars and refined grains [
13]. The Australian dietary guideline stated that adolescents required a wide variety of nutritious foods [
14]. Therefore, adolescent students or young adults from various regions may share different dietary knowledge due to individuality and a localized health environment. Previous studies showed that individual dietary knowledge affected one’s food choices that are also influenced by their health attitudes [
15]. Thus, in order to understand international students’ dietary acculturation, their dietary knowledge and attitudes should be paid more attention.
The functional foods are a food group that has specific functions related to improving health or preventing disease beyond adequate nutritional effects, such as low-fat milk [
16,
17]. Consumer’s awareness and attitude towards functional foods differed among European countries and America [
18]. Labrecque et al. reported that French awareness of functional foods is lower than that of Americans and Canadians [
19]. Besides, compared to Americans who easily accepted and consumed functional foods [
20], Europeans’ attitudes were more critical and doubtful [
21]. However, awareness and acceptance among international students are still unclear, and whether they take consumption of functional foods as a way to cope with dietary acculturation is worthy of exploration.
A Knowledge, Attitude and Practices (KAP) survey is an effective method that records the declarative opinions or statements of participants using predefined questions formatted in standardized questionnaires to provide access to quantitative and qualitative information [
22], and it is also an effective method of investigation in nutrition and diet research. A KAP survey found that diabetic patients with higher scores for knowledge of dietary control had better practices of controlling blood glucose with positive attitudes [
23]. Although KAP surveys on diet, lifestyle or nutrition among medical students or other subgroups have been conducted [
24,
25], similar studies among international students have not been reported yet. To some extent, knowledge, beliefs and attitudes could affect health-related behaviors [
26]. Students who studied abroad might experience dietary changes and have different food choices with various dietary knowledge and attitudes during acculturation. Furthermore, KAP investigation related to diet and health among them will provide clear information. However, no research data on dietary attitudes and habits of immigrants in Ireland are available. Thus, this study was conducted to evaluate the dietary knowledge and attitudes among international college students and explore how their diets changed after migration to Ireland.
2. Materials and Methods
2.1. Participants and Sampling
This cross-sectional study was conducted among international students from the upper-level English language classes. Inclusion criteria were students who were 18 years or above who were living in Ireland for at least one week and who were registered in the English language school (upper-level) at the time of the study. Students who did not have high English level or who could not understand the questionnaire well were excluded.
The Advisory Council for English Language Schools (ACELS) website was accessed and the database of recognized schools in Dublin was used as the sampling frame. Schools belonging to the ACELS were qualified and approved by the Education sector to deliver English language education. Students who attended these schools were mainly international students (i.e., students who moved from their mother country to Ireland) whose first language was not English. From a list of 60 recognized schools, 10 schools were randomly selected. Managers of these schools were invited to take part in this study via telephone calls. All schools contacted agreed to participate. Then the teachers of upper-level classes invited all the students who met the inclusion and exclusion criteria to participate in this study.
2.2. Ethical Statement
This study was approved by the Research Ethics Committee of Dublin Institute of Technology. Permission to conduct the study was also sought from ten selected language schools. Confidentiality and anonymity were explained to each participant, and oral consent was obtained from all participants.
2.3. Data Collection
The questionnaires and an instruction letter for the teachers of each class were sent to the participating schools. The researchers QZ and PA went to each school informed and explained the detailed procedure of the study to the teachers before the study. At the end of the class, the teachers distributed questionnaires to the students who agreed to participate and made a clear explanation of the purpose and requirement of this study. These participants completed the questionnaire and returned it to the teachers. Then the filled questionnaires were gathered and delivered to researchers by the managers of each school.
2.4. Questionnaires
The questionnaire used in this study was self-reported with closed-ended and open-ended questions and could be broadly divided into two parts. One was socio-demographics information, including age, gender, marital status, education level, nationality and length of current stay in Ireland. Nationalities were further grouped into four categories by geographic region, including Asia, Europe, Africa, and South and Central America. The other was healthy diet and functional food knowledge, self-perceived health status, the degree of “Health Locus of Control” (HLC) (i.e., an area-specific measure of locus of control expectancies developed to predict health-related behavior) [
27], dietary change practices and consumption of functional food.
In the functional food section, participants were asked to choose the best explanation of the functional food from four choices (i.e., healthy food; artificial food; food with a specific benefit above the nutrients it naturally contains; and genetically modified food). The statement “food with a specific benefit above the nutrients it naturally contains” is the most accurate. For questions about attitudes and behaviors towards the functional food, the meaning and examples of functional foods were explained, which ensured that the participants understood the questions correctly.
Participants were asked to report their subjective health status and to express their opinions to three health-related attitudinal statements (HLC), based on a 4-point Likert scale (1 = strongly disagree; 2 = tend to disagree; 3 = tend to agree; 4 = strongly agree). The statement was tailored to meet our study aims, including “good health is mainly determined by chance, and there is not much that I can do to influence my long term health” (HLC-1), “my health is mainly controlled by outside influences over which I have little or no control” (HLC-2), and “my health is under my own control, and I can improve my long term health by adopting a healthy lifestyle” (HLC-3) [
27]. Responses to HLCs were further divided into “agree” or “disagree” with the statements.
Questions concerning knowledge of healthy diet, main dietary changes (i.e., Compared to the diet you had in your home country, what are the major differences of your current diet in Ireland?) were open-ended. Furthermore, responses to these questions were grouped into approximately ten broad categories. Besides, functional food consumers were classified as those who reported consuming any food or drinks with added ingredients that claimed to improve their health.
The questionnaire took approximately 15 min to complete. It was reviewed for content validity and reliability by a panel of nutritionists and food scientists. The final questionnaire was pilot tested on 20 international undergraduate students studying in the Dublin Institute of Technology, to assess clarity, literacy and redundancy.
2.5. Statistical Analysis
Data analyses were performed using the SPSS v.15 software (IBM Corp. Armonk, NY, USA). Results were mainly presented as frequencies and percentages. Cross-tabulations and Pearson Chi-square analyses were conducted to explore differences of participants’ perception of health status, dietary changes and HLCs across demographic characteristics. If the cross-tabulation was a 2 × 2, Yates continuity correction was performed when interpreting p values. Furthermore, the level of 5% significance was used throughout the statistical analyses. Content analyses were performed by QZ and PA for open-ended questions. The researchers read all the answers and grouped them into categories individually. They then reviewed the groupings together and discussed to reach an agreement when inconsistency in the groupings existed.
4. Discussion
The current study explored international students’ dietary knowledge, attitude and practices after immigrating to Ireland. This study included 473 participants with a relatively balanced gender ratio. Our major findings were as follows: (1) less than half of the participants had a broad concept of healthy diet and even fewer knew the specific meaning; (2) more than two thirds of the participants could explain the term functional foods, and Asian students had the highest usage and daily usage rate of functional foods; (3) participants who perceived their health better were more likely to think that their health status was controlled by themselves; (4) participants who were younger, single, from African and South and Central American countries or who were in Ireland for less than one year were more likely to report dietary change after immigration.
In our study, almost half of the international students had a broad concept about healthy diet (i.e., “balanced/various/nutritious diet”). However, the number of participants who related a healthy diet to “reduce fat” or “less sugar and salt” was less than those who related a healthy diet to “more fruit and vegetables". Participants who knew that a healthy diet is associated with “less red meat, more white meat and fish” and “more fiber” were fewer. Dietary knowledge survey results in this study indicated that dietary knowledge was not comprehensive among international students in Ireland. Previous research concluded that the awareness of a healthy diet was generally insufficient among international students, especially those studying nonhealth sciences [
28]. Therefore, it is necessary to provide international students with essential knowledge of a healthy diet. The knowledge could be spread via English language schools by integrating dietary knowledge with other core subjects, such as language [
29].
Functional foods that claim to improve health and wellbeing generally have special functions such as protecting the cardiovascular system, preventing cancers and so on [
30,
31,
32]. Functional food is gradually being accepted by consumers, especially elderly adults [
33]. However, whether international students take functional food as a way to keep healthy is worth exploring. Besides, the perception, acceptability or consumption of functional food among international students remains unclear. In the current study, functional food was found to be used by some international students, with differences among students from different regions. Our results showed that although the percentage was not high among participants who knew functional food, their perception was largely correct. The previous study suggested that increased knowledge was an important factor promoting functional food consumption [
33]. Thus, it is suggested that the information of functional food could be incorporated into nutrition education for international students.
For the attitude of international students towards their health status and health locus of control (HLC), our results showed that participants who evaluated their health better were more likely to believe that their health status was determined by their own control (e.g., the European participants). By contrast, Asian participants who were least likely to deem their health status as very good or excellent showed no strong tendency to either agree or disagree with all attitudinal statements. Marques et al. also found that 20% of the total variance in people’s subjective health status was due to country differences [
34]. Intriguingly, the consumption percentage and daily use of functional food among Asian students were high. Thus, it can be seen that whether international students adopted functional food or not was not determined by their own attitude towards health status. Furthermore, Herath et al. also came to similar conclusions [
35]. The differences in subjective health status, attitudes towards health control and functional food consumption among different countries might be attributed to the distinctness of personality traits across countries. The Five-Factor Model (FFM) is used to describe human personality psychologically, which consists of five trait factors: Neuroticism (N); Extraversion (E); Openness (O); Agreeableness (A); and Conscientiousness (C) [
36]. It showed that people from Asian countries were lower in Extraversion and higher in Neuroticism compared to people from European countries [
37]. Besides personality, cultural diversity or climate differences might also be potential reasons; related research should be pursued.
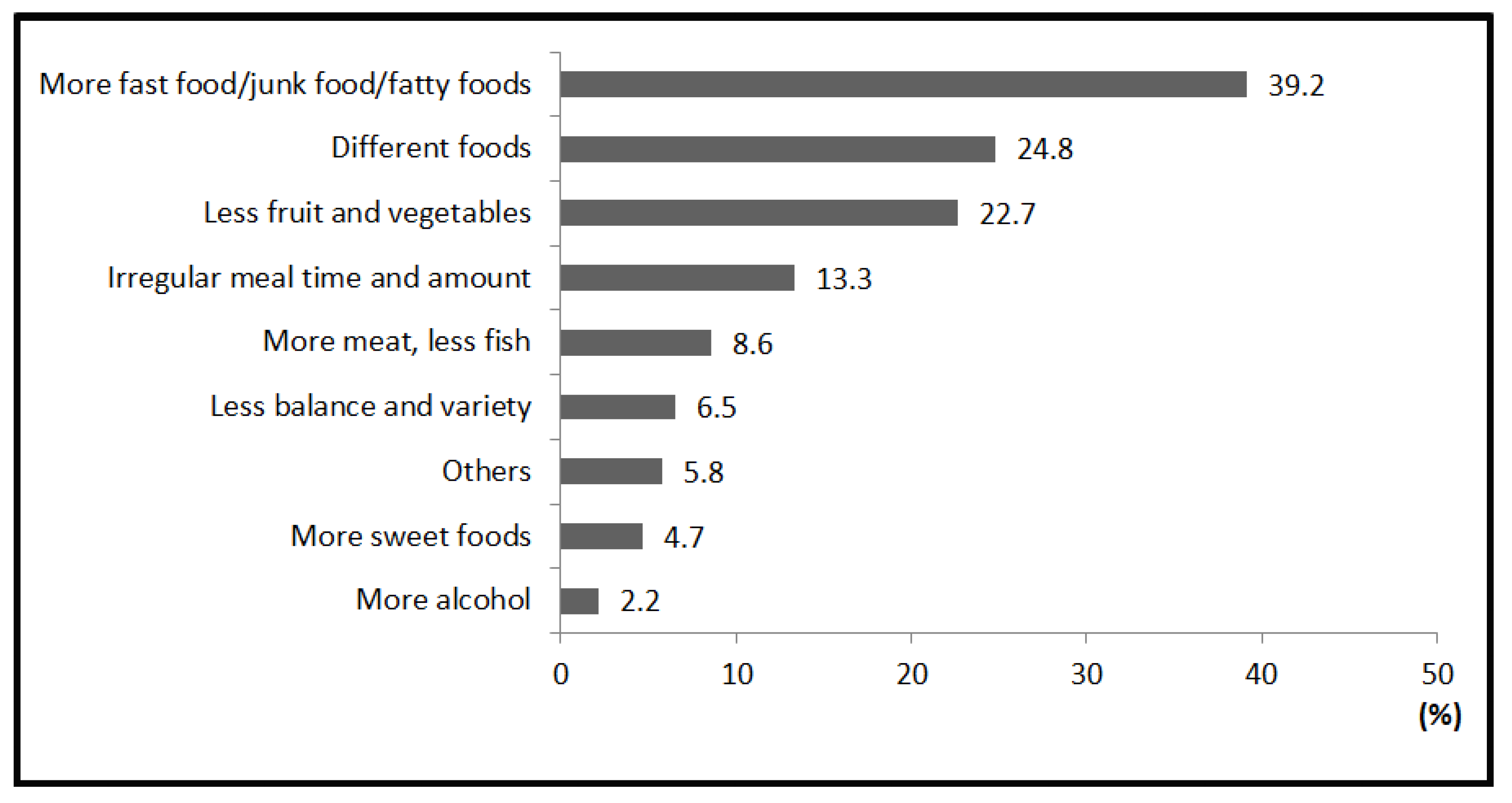
We found that international students may change their dietary practices to adapt to a new life abroad. In the current study, participants who were younger, single, from African and South and Central American countries and who were living in Ireland for less than one year were more likely to perceive overall dietary changes. However, the dietary changes they reported showed that their diet became unhealthier after coming to Ireland. As they reported, “more fast food/junk food/fatty food” was the most common change, and lower intakes of fruit, vegetables, and fish were also frequently reported. This result was consistent with the previous study showing that people from non-Western countries suffered from a worse dietary change after migrating to Western countries [
38,
39]. Furthermore, these dietary changes may be related to the increasing prevalence of diet-related diseases among the immigrants in certain ethnic groups, e.g., South-Asians in the UK [
40]. Besides, Akresh et al. [
41] found that Hispanic immigrants had a greater degree of dietary change with a longer stay in the United States, which is contrary to our results in which being in Ireland for less than one year was more likely to lead to dietary change. It is possible that newcomers were more likely to be influenced by the local Irish dietary culture and environment because of living with a host family, eating outside, etc. The longer they settled down, the more familiar they were with their ethnic food market in Ireland so that they might return to their original diet.
To the authors’ knowledge, literature on the diet of international students was limited. This study is novel in its examination of diet and health among international students who were living in Ireland for study. The current study included not only international students’ dietary knowledge and attitude but also their practices and dietary changes after immigrating. Besides, the participant characteristics of youth, bachelordom and high education level were in accord with the fast facts towards college and university students from the National Center for Education Statistics [
42]. Therefore, the participating international students who came from 36 countries were representative and cross-cultural.
However, this study was limited by its cross-sectional nature and the convenience sample of international students from different countries. Our findings might not apply to students from other countries and immigrants with little English skills or who were working in Ireland. Moreover, no comparative studies on domestic students were conducted. We were unable to differentiate which changes were caused by migration to Ireland and which changes were caused by leaving one’s hometown or parental home for other cities. Future studies among Irish students who left their parental home or hometown for other cities for tertiary education are worth conducting. Besides, there is some variability in the samples as the length of staying in Ireland ranged from one week to 7.4 years. Information on participants’ socioeconomic and health status and religious information that might impact results were not assessed in the survey.

 ,
, 


{kind=link}
{kind=link}
{kind=link}