Abstract
Background: Overweight and obesity have become a major public health concern in recent decades, particularly in patients with chronic health conditions like congenital heart disease (CHD). This systematic review elaborates on the prevalence and the longitudinal development of overweight and obesity in children and adults with CHD. Methods: A systematic literature search was conducted in PubMed, Cochrane, and Scopus from January 2010 to December 2020 on overweight and obesity prevalence in children and adults with CHD. Results: Of 30 included studies, 15 studies evaluated 5680 pediatric patients with CHD, 9 studies evaluated 6657 adults with CHD (ACHD) and 6 studies examined 9273 both pediatric patients and ACHD. Fifteen studies received the quality rating “good”, nine studies “fair”, and six studies “poor”. In children with CHD, overweight prevalence was between 9.5–31.5%, and obesity prevalence was between 9.5–26%; in ACHD, overweight prevalence was between 22–53%, and obesity was between 7–26%. The prevalence of overweight and obesity was thereby similar to the general population. Overweight and obesity have been shown to increase with age. Conclusion: The prevalence of overweight and obesity in children and adults with CHD is similar to the general population, demonstrating that the growing obesity pandemic is also affecting the CHD population.
1. Introduction
Overweight and obesity have become major public health concerns in recent decades [1] and are referred to as a global pandemic [2]. The prevalence of childhood obesity has more than doubled in the last three decades [3], which is particularly concerning as childhood obesity tracks into adulthood [4]. Overweight and obesity, in particular, are independent risk factors for cardiovascular diseases and are associated with increased risk of morbidity and mortality in the general population [5]. As the majority of children with congenital heart disease (CHD) nowadays survive into adulthood [6], environmental and behavioral health risk factors are also of concern in this patient cohort [7,8]. As patients with pre-existing heart conditions are prone to cardiovascular events [9] due to underlying anatomic and functional abnormalities [10], overweight and obesity need to be considered here too.
At first glance, one would assume that patients with CHD are at increased risk for overweight and obesity because, as cardiac patients, physical activity may be reduced due to exercise restriction or overprotection, and patients participate less in leisure and competitive sports [11]. On the other hand, surgeries, hospitalization, and rehabilitation early in life affect the development of children with CHD, which can be linked to underweight and malnutrition [12]. Additionally, many CHD patients have a very strong health awareness and maintain a mindful lifestyle, including a healthy body weight [13].
So far, only limited and conflicting data exist on the prevalence of overweight and obesity in the population with CHD [14]. Therefore, this systematic review elaborates on the prevalence and longitudinal development of overweight and obesity in children and adults with CHD.
2. Materials and Methods
2.1. Search Strategy
A systematic literature search was conducted in the electronic databases PubMed, Cochrane, and Scopus that referred to articles from January 2010 to December 2020. Relevant observational studies in the English language were identified by two independent reviewers. A standard protocol with search terms was developed according to the population, intervention, comparison, outcome, and context (PICO–C) [15] method and applied in the following combination:
- “congenital heart disease” OR “congenital heart defect” AND
- “overweight” OR “obesity” OR “adiposity” OR “body constitution”
Medical Subject Headings terms and filters (published in the previous 10 years, humans, preschool child: 2–5 years, child: 6–12 years, adolescent: 13–18 years, adult: 19+ years) were used and appropriately adapted if necessary.
2.2. Data Collection
Two reviewers screened the relevant articles for title and abstract that had to fulfill the basic inclusion criteria: diagnosed CHD and the measurement of overweight and obesity. At least one of the reviewers had to consider a reference eligible; in case of disagreement, a third reviewer was consulted for a majority decision before full-text analysis.
Documenting critical appraisal of the included literature, reviewers used the “Study Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies” of the National Heart, Lung and Blood Institute (NHLBI), consisting of a 14-item list assessing potential risk for bias. Accordingly, included studies were categorized as good, fair, or poor [16].
3. Results
3.1. Study Inclusion
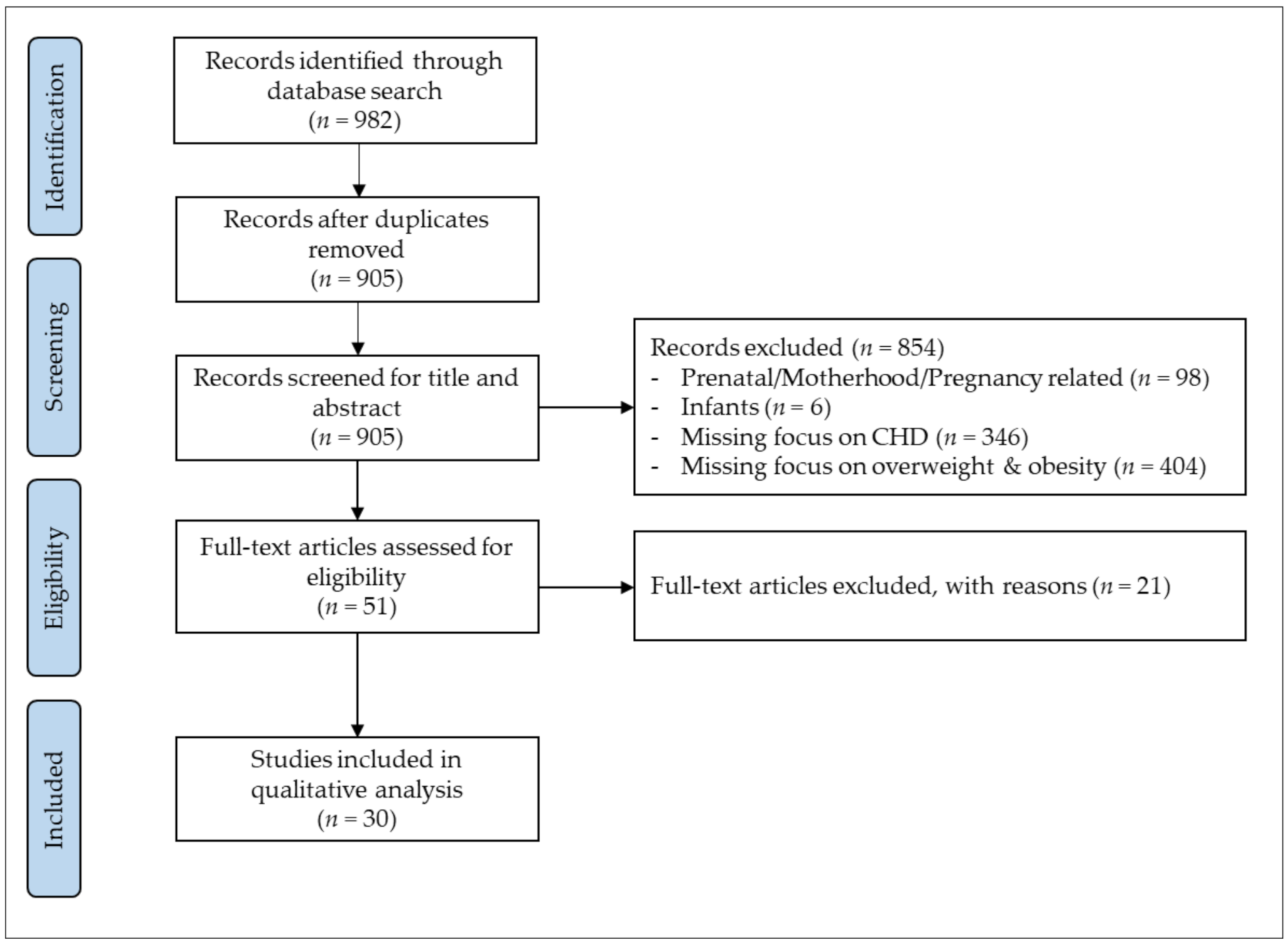
In total, 982 potential studies were identified in the initial search, of which 905 remained after duplicates had been removed. After screening titles and abstracts, 51 potential studies were retrieved for full-text analysis, of which 21 studies were excluded due to: main focus on the impact of overweight and obesity (n = 12), lacking focus on overweight and obesity (n = 5), focus on underweight (n = 1) and not exclusively assessing patients with CHD (n = 3). Finally, 30 studies with a total of 21,610 CHD patients met the inclusion criteria for this systematic review. The search algorithm and selection process is displayed in Figure 1.
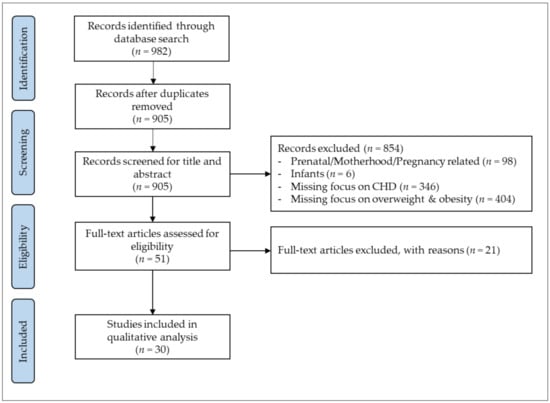
Figure 1.
Search and selection process for systematic review according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISAM). Congenital heart disease (CHD).
3.2. Study Characteristics
Of the included studies, 15 studies evaluated 5680 pediatric patients with CHD (range 32–1080 patients) aged 2–18 years, 9 studies evaluated 6657 ACHD (range 54–2424 patients) aged 18–71 years, and 6 studies examined 9273 both pediatric and ACHD (range 50–4496 patients) aged 2–48 years.
Twenty-six of the included studies were cross-sectional studies that examined the prevalence of overweight and obesity in patients with CHD [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42], and four were cohort studies that investigated the longitudinal change of the prevalence across the lifespan [10,43,44,45]. The body composition of patients with CHD was compared to a healthy reference cohort in 13 of the included studies [20,21,22,23,24,28,29,30,33,35,40,41,45], whereas 9 studies merely investigated the prevalence of overweight and obesity in patients with CHD [10,17,18,19,24,32,36,38,39]. Table 1 provides further information on the study characteristics and outcomes of the included studies.

Table 1.
Study characteristics and outcomes.
3.3. Measuring Overweight & Obesity
All included studies assessed overweight and obesity with the body mass index (BMI), while two studies additionally performed dual x-ray absorptiometry [18,20], one study performed impedance measurement [35], and one study assessed waist circumference [20]. Based on the BMI, patients were classified as underweight (<18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2), obese (≥30 kg/m2) and severe obese (≥35 kg/m2). BMI values were converted into age and gender-specific z-Scores in a subset of studies [10,17,18,38,40]. Fourteen studies converted the BMI into percentiles based on various growth charts, classifying patients with BMI ≥85th–<95th percentile as overweight and those with BMI ≥ 95th percentile as obese [10,19,23,24,32,33,34,36,38,39,40,41,43,45].
3.4. Study Quality
According to the NHLBI study quality assessment tool [16], 15 studies received the quality rating “good”, while 9 studies were rated as “fair”. Six studies showed a substantial risk of bias and were rated as “poor”. Various contributing factors have an impact on weight status and should therefore be considered when investigating the prevalence of overweight and obesity. The included studies in this review controlled for age [21,24,35,37,39], age and lesion severity [27], age and sex [10,17,18,20,23,28,31,33,36,38,40,41,43,44], race/ethnicity [29,45], family history, parent’s nutritional status [19], marital status, educational level, and geographic region [34]. Six studies did not take confounders into account and were therefore rated as “poor” [8,22,25,26,37,42]. Comprehensive information on the quality rating can be found in Table 2.
Table 2.
Quality assessment according to the NHLBI Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies.
3.5. Overweight and Obesity in Children with CHD
In children with CHD, the prevalence of overweight ranged from 9.5% [36] to 31.5% [39] and the prevalence of obesity ranged from 9.5% [19] to 26.2% [36]. Studies comparing children with CHD to healthy controls reported similar overweight and obesity prevalence in both groups [18,20,21,24,33,35,40,41,45], whereby controls were age-matched [21,35], age and sex matched [20], and age, sex and race/ethnicity matched [45].
One study reported decreased BMI in CHD children [23], whereas another study reported increased obesity rates in CHD children compared to healthy controls [33]. CHD participants had a significantly greater waist circumference than controls when controlling for sex, birth weight, physical activity score, and total lean mass [20].
Overweight and obesity occurred more frequently in CHD boys than in girls [19,23]. There was no association between overweight and obesity prevalence and CHD severity or surgical status in CHD children [26,40]. Children with cyanotic CHD had a lower prevalence of overweight and obesity than those with non-cyanotic CHD [19,23]. Significantly lower BMI values were found in children with tetralogy of Fallot five years after surgery compared to age-matched controls [21]. Patients with Transposition of the Great Arteries and Coarctation of the Aorta showed significantly higher BMI compared with norm data and other cardiac diagnoses [38,44]. Studies on Fontan children reported a lower prevalence of overweight and obesity at the time of Fontan procedure, which increased to 30% five years post-surgery [10], but showed no significant difference to healthy controls [35].
3.6. Overweight and Obesity in Adults with CHD
In adults with CHD, overweight prevalence was found in a range from 22% [24] to 53% [30], while obesity was reported in a range between 7% [22] and 26% [29]. Studies comparing overweight and obesity prevalence with healthy controls found either similar overweight and obesity rates [22,29,43] or lower prevalence compared to the reference cohort [31,42]. However, ACHD showed a decreased prevalence of morbid obesity compared to matched controls [29].
Two studies found no association between CHD severity and prevalence of overweight and obesity [26,29], whereas two other studies reported a reduced prevalence in the more complex classes like total cavopulmonary connection compared to the reference population [31,42]. One study on ACHD reported men being more overweight than women [31], while another study found no sex differences [34]. Hispanic patients were more likely to be obese than white ACHD after adjusting for age and gender [29]. Non-Hispanic Blacks with CHD had a 58% increased risk of obesity in young adulthood and 33% in late adulthood compared to white CHD [28].
BMI was positively associated with impaired NYHA class and cardiovascular medication intake [42]. Metabolic syndrome was more common in ACHD patients than in controls, and obese ACHD patients were more likely to have metabolic syndrome than obese controls [43].
3.7. Longitudinal Development of Overweight and Obesity
The number of overweight and obese children increased during adolescence [27,44]. Also, in adults with CHD, age correlated with increased BMI [29,31,34,42], with similar results found in the general population [29,31]. Generally, adults had significantly higher BMI scores and were more likely to be overweight or obese compared with younger samples [26]. The odds of being overweight or obese as an adult were found to be three times higher if their childhood BMI was already above the 85th percentile [24].
4. Discussion
This systematic review shows that the overall distribution of overweight and obesity is consistent with the prevalence in the general population, in which overweight and obesity rates have increased dramatically in recent decades [37]. Particularly, CHD patients with increasing age, male gender, and Hispanic origin are at risk for overweight and adiposity. These findings are worrisome, as the CHD population is at higher risk of developing metabolic syndrome and premature morbidity and mortality compared to their healthy peers [43]. Obesity is associated with an increased risk of cardiovascular diseases, like heart failure and coronary artery disease [46]. Excessive body adipose tissue impacts the vessel wall by changes in blood pressure, glucose level, lipid metabolism, and systemic inflammation [47]. In children and adults with CHD, overweight and obesity were shown to be associated with cardiac comorbidities, increased cardiac medication intake, and higher systolic and diastolic blood pressure compared to normal-weight patients. According to this recently published study, the elevated risk of morbidity and mortality in the CHD population is exacerbated by obesity [27]. Obesity has been associated with adverse perioperative outcomes [48] as well as adverse short-term outcomes after cardiothoracic surgery in patients with CHD [49]. In contrast, another study on ACHD reported that overweight and moderate obesity were associated with reduced mortality rates, especially in symptomatic ACHD patients and those with complex underlying cardiac defects, replicating the so-called “obesity paradox” in the general population [14]. It was also shown that overweight and obesity are associated with lower heart failure rates in ACHD [24]. In the elderly, this may indeed be true, as a slightly elevated weight above normal BMI can be a resource to build upon when facing surgical procedures or beginning aggressive drug therapy. However, overweight and obesity are among the most significant contributors to illness and adverse health outcomes and should be prevented or reduced at all costs, at least in younger patients with CHD.
Underlying causes and effects of the high overweight and obesity prevalence in the CHD population are multifactorial. Heart failure-associated reasons such as medication intake were identified along with the already mentioned behavioral factors. Two major factors influencing the CHD population are physical inactivity due to restrictions or overprotection by physicians and parents, as well as weight gain interventions in infancy, which can develop into excess weight later in life [17]. Part of the included studies examined the association between overweight and obesity and contributing factors. Yang et al. reported an association between sedentary behavior and increased overweight and obesity prevalence in CHD children [41]. BMI has been shown to be negatively associated with exercise duration [32] and exercise capacity in the CHD population [42].
Continuous monitoring of weight status and interventions to reduce the prevalence of overweight and obesity are required in this patient cohort at high risk for acquired cardiovascular disease [37]. Interventions such as lifestyle and nutritional counseling to reduce risk factors for obesity should begin in early childhood and include parental education.
Limitations and Further Research
The classification of overweight and obesity in the majority of included studies refers to the BMI, which, however, does not analyze fat distribution and body composition. Abdominal fat, in particular, has been associated with various pathologies [45]. Therefore, further studies should specifically address abdominal fat in order to quantify the visceral component of adipose tissue [31]. Moreover, BMI is based on both fat mass and lean mass and therefore carries the risk of classifying muscular patients as overweight [37]. The majority of included studies have not considered race and ethnicity as potential confounders, even though their influence on weight status is well established [44].
5. Conclusions
The prevalence of overweight and obesity in children and adults with CHD reflects that of the general population, demonstrating that the growing obesity pandemic is also affecting the CHD population. Such a high prevalence of overweight and obesity is particularly worrying in the context of CHD. We hope that these results will raise awareness of this issue and encourage appropriate health-promoting interventions and individual consultations.
Author Contributions
Conceptualization, J.M.; methodology, J.M., L.W., L.B. and M.M.; validation, L.W. and L.B.; formal analysis, J.M.; investigation, L.W., M.M. and L.B.; resources, J.M. and P.E.; data curation, L.W. and M.M.; writing—original draft preparation, L.W.; writing—review and editing, J.M., L.W., L.B., M.M., P.E. and R.O.-F.; supervision, J.M.; project administration, J.M.; funding acquisition, J.M. and P.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by an unrestricted grant from the “Fördergemeinschaft Deutsche Kinderherzzentren e.V.”.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of over-weight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Ogden, C.L.; Carroll, M.D.; Lawman, H.G.; Fryar, C.D.; Kruszon-Moran, D.; Kit, B.K.; Flegal, K.M. Trends in obesity prevalence among chil-dren and adolescents in the United States, 1988–1994 through 2013–2014. JAMA 2016, 315, 2292–2299. [Google Scholar] [CrossRef] [PubMed]
- Suchindran, C.; North, K.E.; Popkin, B.M.; Gordon-Larsen, P. Association of Adolescent Obesity With Risk of Severe Obesity in Adulthood. JAMA 2010, 304, 2042–2047. [Google Scholar]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G. A comparative risk assessment of burden of dis-ease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- Khairy, P.; Ionescu-Ittu, R.; Mackie, A.; Abrahamowicz, M.; Pilote, L.; Marelli, A.J. Changing Mortality in Congenital Heart Disease. J. Am. Coll. Cardiol. 2010, 56, 1149–1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- St-Pierre, J.; Poirier, P. What Nature Used to Allow to Die, Don’t Let Modern Habits Damage After Repair: Preventable Obe-sity Risk in Congenital Heart Disease. Can. J. Cardiol. 2015, 31, 109–111. [Google Scholar] [CrossRef]
- Lui, G.K.; Fernandes, S.; McElhinney, D.B. Management of Cardiovascular Risk Factors in Adults With Congenital Heart Disease. J. Am. Hear. Assoc. 2014, 3, e001076. [Google Scholar] [CrossRef] [Green Version]
- Verheugt, C.L.; Uiterwaal, C.S.P.M.; Van Der Velde, E.T.; Meijboom, F.J.; Pieper, P.G.; van Dijk, A.; Vliegen, H.W.; Grobbee, D.E.; Mulder, B.J. Mortality in adult congenital heart disease. Eur. Hear. J. 2010, 31, 1220–1229. [Google Scholar] [CrossRef] [Green Version]
- Wellnitz, K.; Harris, I.S.; Sapru, A.; Fineman, J.R.; Radman, M. Longitudinal development of obesity in the post-Fontan population. Eur. J. Clin. Nutr. 2015, 69, 1105–1108. [Google Scholar] [CrossRef] [Green Version]
- Diller, G.-P.; Kempny, A.; Alonso-Gonzalez, R.; Swan, L.; Uebing, A.; Li, W.; Babu-Narayan, S.; Wort, S.J.; Dimopoulos, K.; Gatzoulis, M.A. Survival Prospects and Circumstances of Death in Contemporary Adult Congenital Heart Disease Patients Under Follow-Up at a Large Tertiary Centre. Circulation 2015, 132, 2118–2125. [Google Scholar] [CrossRef] [Green Version]
- Costello, C.L.; Gellatly, M.; Daniel, J.; Justo, R.N.; Weir, K. Growth Restriction in Infants and Young Children with Congenital Heart Disease. Congenit. Hear. Dis. 2015, 10, 447–456. [Google Scholar] [CrossRef]
- Zomer, A.C.; Vaartjes, I.; Uiterwaal, C.S.; van der Velde, E.T.; Sieswerda, G.-J.T.; Wajon, E.M.; Plomp, K.; van Bergen, P.F.; Verheugt, C.L.; Krivka, E.; et al. Social Burden and Lifestyle in Adults With Congenital Heart Disease. Am. J. Cardiol. 2012, 109, 1657–1663. [Google Scholar] [CrossRef]
- Brida, M.; Dimopoulos, K.; Kempny, A.; Liodakis, E.; Alonso-Gonzalez, R.; Swan, L.; Uebing, A.; Baumgartner, H.; Gatzoulis, M.A.; Diller, G.-P. Body mass index in adult congenital heart disease. Heart 2017, 103, 1250–1257. [Google Scholar] [CrossRef] [PubMed]
- Uman, L.S. Systematic reviews and meta-analyses. J. Can. Acad. Child. Adolesc. Psychiatry 2011, 20, 57. [Google Scholar]
- National Heart, Lung, and Blood Institute. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies 2014. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 1 June 2021).
- Aguilar, D.C.; Raff, G.W.; Tancredi, D.; Griffin, I.J. Childhood growth patterns following congenital heart disease. Cardiol. Young 2015, 25, 1044–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avitabile, C.M.; Leonard, M.B.; Zemel, B.S.; Brodsky, J.L.; Lee, D.; Dodds, K.; Hayden-Rush, C.; Whitehead, K.K.; Goldmuntz, E.; Paridon, S.M.; et al. Lean mass deficits, vitamin D status and exercise capacity in children and young adults after Fontan palliation. Heart 2014, 100, 1702–1707. [Google Scholar] [CrossRef] [Green Version]
- Barbiero, S.M.; D’Azevedo Sica, C.; Schuh, D.S.; Cesa, C.C.; de Oliveira Petkowicz, R.; Pellanda, L.C. Overweight and obesity in children with congenital heart disease: Combination of risks for the future? BMC Pediatrics 2014, 14, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbour-Tuck, E.; Boyes, N.G.; Tomczak, C.R.; Lahti, D.S.; Baril, C.L.; Pockett, C.; Runalls, S.; Kakadekar, A.; Pharis, S.; Bradley, T.J.; et al. A cardiovascular disease risk factor in chil-dren with congenital heart disease: Unmasking elevated waist circumference-a CHAMPS* study *CHAMPS: Children’s Healthy-Heart Activity Monitoring Program in Saskatchewan. BMC Cardiovasc. Disord. 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Briston, D.A.; Sabanayagam, A.; Zaidi, A.N. Observations on obesity patterns in tetralogy of Fallot patients from childhood to adulthood. Cardiol. Young 2017, 27, 890–894. [Google Scholar] [CrossRef]
- Buys, R.; Budts, W.; Delecluse, C.; Vanhees, L. Exercise Capacity, Physical Activity, and Obesity in Adults With Repaired Aortic Coarctation. J. Cardiovasc. Nurs. 2013, 28, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-A.; Wang, J.-K.; Lue, H.-C.; Hua, Y.-C.; Chang, M.-H.; Wu, M.-H. A Shift from Underweight to Overweight and Obesity in Asian Children and Adolescents with Congenital Heart Disease. Paediatr. Périnat. Epidemiol. 2012, 26, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.T.; Hong, B.; Patterson, L.; Petit, C.J.; Ham, J.N. High Overweight and Obesity in Fontan Patients: A 20-Year History. Pediatr. Cardiol. 2016, 37, 192–200. [Google Scholar] [CrossRef]
- Fedchenko, M.; Mandalenakis, Z.; Dellborg, H.; Hultsberg-Olsson, G.; Björk, A.; Eriksson, P.; Dellborg, M. Cardiovascular risk factors in adults with coarctation of the aorta. Congenit. Hear. Dis. 2019, 14, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Harris, K.C.; Voss, C.; Rankin, K.; Aminzadah, B.; Gardner, R.; Mackie, A.S. Modifiable cardiovascular risk factors in adolescents and adults with congenital heart disease. Congenit. Hear. Dis. 2018, 13, 563–570. [Google Scholar] [CrossRef]
- Jackson, J.L.; Fox, K.R.; Cotto, J.; Harrison, T.M.; Tran, A.H.; Keim, S.A. Obesity across the lifespan in congenital heart disease survi-vors: Prevalence and correlates. Heart Lung 2020, 49, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Jackson, J.L.; Harrison, T.; Keim, S. Differences in Obesity Among Black and White Children, Adolescents, and Adults With Congenital Heart Disease. J. Cardiovasc. Nurs. 2019, 34, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Lerman, J.B.; Parness, I.A.; Shenoy, R.U. Body Weights in Adults With Congenital Heart Disease and the Obesity Frequency. Am. J. Cardiol. 2017, 119, 638–642. [Google Scholar] [CrossRef]
- Lui, G.K.; Rogers, I.S.; Ding, V.Y.; Hedlin, H.K.; MacMillen, K.; Maron, D.J.; Sillman, C.; Romfh, A.; Dade, T.C.; Haeffele, C.; et al. Risk Estimates for Atherosclerotic Cardiovascular Disease in Adults With Congenital Heart Disease. Am. J. Cardiol. 2017, 119, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Malavazos, A.; Capitanio, G.; Chessa, M.; Matelloni, I.A.; Milani, V.; Stella, E.; Al Kassem, L.; Sironi, F.; Boveri, S.; Giamberti, A.; et al. Body mass index stratification in hospitalized Italian adults with congenital heart disease in relation to complexity, diagnosis, sex and age. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 367–377. [Google Scholar] [CrossRef]
- O’Byrne, M.L.; McBride, M.G.; Paridon, S.; Goldmuntz, E. Association of Habitual Activity and Body Mass Index in Survivors of Congenital Heart Surgery: A Study of Children and Adolescents With Tetralogy of Fallot, Transposition of the Great Arteries, and Fontan Palliation. World J. Pediatr. Congenit. Hear. Surg. 2018, 9, 177–184. [Google Scholar] [CrossRef]
- Perin, F.; Blesa, C.C.; Cobo, I.; Maldonado, J. Overweight and obesity in children treated for congenital heart disease. An. de Pediatría 2018, 90, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Pike, N.A.; Evangelista, L.; Doering, L.V.; Eastwood, J.-A.; Lewis, A.B.; Child, J.S. Sex and Age Differences in Body-Image, Self-Esteem, and Body Mass Index in Adolescents and Adults After Single-Ventricle Palliation. Pediatr. Cardiol. 2012, 33, 705–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powell, A.W.; Wittekind, S.G.; Alsaied, T.; Lubert, A.M.; Chin, C.; Veldtman, G.R.; Cordina, R.; Katz, D.A.; Mays, W.A.; Knecht, S.K.; et al. Body Composition and Exercise Performance in Youth With a Fontan Circulation: A Bio-Impedance Based Study. J. Am. Hear. Assoc. 2020, 9, e018345. [Google Scholar]
- Ray, T.D.; Green, A.; Henry, K. Physical activity and obesity in children with congenital cardiac disease. Cardiol. Young 2011, 21, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Sandberg, C.; Rinnström, D.; Dellborg, M.; Thilén, U.; Sörensson, P.; Nielsen, N.E.; Christersson, C.; Wadell, K.; Johansson, B. Height, weight and body mass index in adults with congenital heart disease. Int. J. Cardiol. 2015, 187, 219–226. [Google Scholar] [CrossRef]
- Smith-Parrish, M.; Yu, S.; Rocchini, A. Obesity and Elevated Blood Pressure following Repair of Coarctation of the Aorta. J. Pediatr. 2014, 164, 1074–1078.e1. [Google Scholar] [CrossRef]
- Steele, J.M.; Preminger, T.J.; Erenberg, F.G.; Wang, L.; Dell, K.; Alsaied, T.; Zahka, K.G. Obesity trends in children, adolescents, and young adults with congenital heart disease. Congenit. Hear. Dis. 2019, 14, 517–524. [Google Scholar] [CrossRef]
- Welisch, E.; Rauch, R.; Seabrook, J.A.; Filler, M.G.; Norozi, K. Are the children and adolescents with congenital heart disease living in Southwestern Ontario really overweight and obese? Cardiol. Young 2013, 24, 848–853. [Google Scholar] [CrossRef]
- Yang, F.-L.; Gau, B.-S.; Yang, H.-L.; Lin, M.-T.; Moons, P. Energy Balance-Related Behaviors and Body Mass Index in Asian School-Aged Children With Congenital Heart Disease. J. Cardiovasc. Nurs. 2020, 35, 291–299. [Google Scholar] [CrossRef]
- Zaqout, M.; Vandekerckhove, K.; Michels, N.; Demulier, L.; Bove, T.; François, K.; de Backer, J.; de Henauw, S.; de Wolf, D. Body mass index in adults with congenital heart disease. Congenit. Hear. Dis. 2019, 14, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Deen, J.F.; Krieger, E.; Slee, A.E.; Arslan, A.; Arterburn, D.; Stout, K.K.; Portman, M.A. Metabolic Syndrome in Adults With Congenital Heart Disease. J. Am. Hear. Assoc. 2016, 5, e001132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamayo, C.; Manlhiot, C.; Patterson, K.; Lalani, S.; McCrindle, B.W. Longitudinal evaluation of the prevalence of over-weight/obesity in children with congenital heart disease. Can. J. Cardiol. 2015, 31, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Weinreb, S.J.; Pianelli, A.J.; Tanga, S.R.; Parness, I.A.; Shenoy, R.U. Risk factors for development of obesity in an ethnically diverse CHD population. Cardiol. Young 2019, 29, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Sen, A.; Norat, T.; Janszky, I.; Romundstad, P.; Tonstad, S.; Vatten, L.J. Body mass index, abdominal fatness, and heart failure incidence and mortality: A systematic review and dose-response meta-analysis of prospective studies. Circulation 2016, 133, 639–649. [Google Scholar] [CrossRef]
- Fantuzzi, G.; Mazzone, T. Adipose tissue and atherosclerosis: Exploring the connection. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 996–1003. [Google Scholar] [CrossRef]
- O’Byrne, M.L.; Kim, S.; Hornik, C.P.; Yerokun, B.A.; Matsouaka, R.A.; Jacobs, J.P.; Jacobs, M.L.; Jonas, R.A. Effect of obesity and underweight status on perioperative outcomes of congenital heart operations in children, adolescents, and young adults: An analysis of data from the society of thoracic surgeons database. Circulation 2017, 136, 704–718. [Google Scholar] [CrossRef]
- Garcia, R.U.; Balakrishnan, P.L.; Aggarwal, S. Does obesity affect the short-term outcomes after cardiothoracic surgery in adoles-cents with congenital heart disease? Cardiol. Young 2020, 30, 372–376. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).