
Prevalence of Prediabetes and Type 2 Diabetes Mellitus in Football Players: A Novel Multi Football Clubs Cross Sectional Study

 , ,
, ,
Abstract
:1. Introduction
2. Subjects and Methods
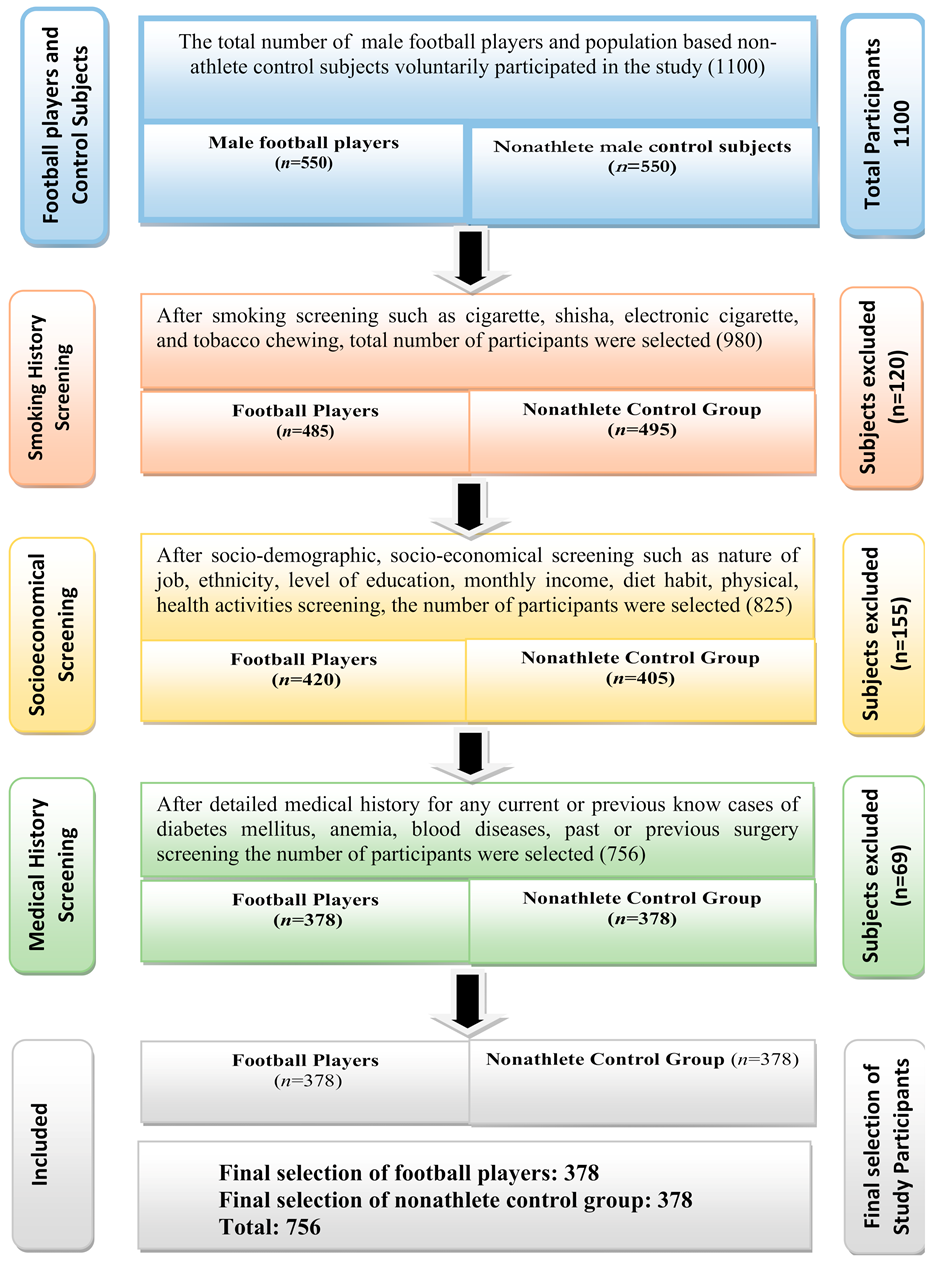
2.1. Study Participants
2.2. Clinical History and Socio Demographic Characteristics
2.3. Exclusion Criteria
2.4. Measurements of Glycated Hemoglobin (HbA1c)
2.5. Ethics Statement
2.6. Statistical Analysis
3. Results
4. Discussion
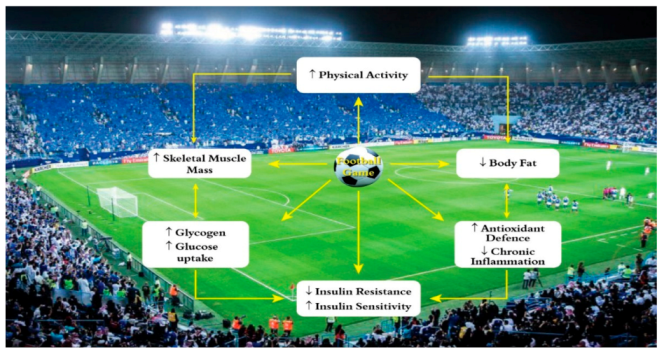
4.1. Possible Mechanism-How Football Reduces Diabetes Mellitus
4.2. Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Skoradal, M.-B.; Weihe, P.; Patursson, P.; Mortensen, J.; Connolly, L.; Krustrup, P.; Mohr, M. Football training improves metabolic and cardiovascular health status in 55- to 70-year-old women and men with prediabetes. Scand. J. Med. Sci. Sports 2018, 28 (Suppl. S1), 42–51. [Google Scholar] [CrossRef] [Green Version]
- Meo, S.A. Diabetes mellitus: Health and wealth threat. Int. J. Diabetes Mellit. 2009, 1, 42. [Google Scholar] [CrossRef] [Green Version]
- Internatinal Diabetes Fedration. Diabetes Atlas, 9th ed. Available online: http://www.diabetesatlas.org/key-messages.html (accessed on 15 November 2019).
- Wang, Q.; Zhang, X.; Fang, L.; Guan, Q.; Guan, L.; Li, Q. Prevalence, awareness, treatment and control of diabetes mellitus among middle-aged and elderly people in a rural Chinese population: A cross-sectional study. PLoS ONE 2018, 13, e0198343. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Protecting Workers’ Health. Available online: https://www.who.int/news-room/fact-sheets/detail/protecting-workers%27-health (accessed on 2 November 2019).
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Faude, O.; Kerper, O.; Multhaupt, M.; Winter, C.; Beziel, K.; Junge, A.; Meyer, T. Football to tackle overweight in children. Scand. J. Med. Sci. Sports 2010, 20, 103–110. [Google Scholar] [CrossRef]
- Krustrup, P.; Krustrup, B.R. Football is medicine: It is time for patients to play! Br. J. Sports Med. 2018, 52, 1412–1414. [Google Scholar] [CrossRef] [Green Version]
- Oja, P.; Titze, S.; Kokko, S.; Kujala, U.M.; Heinonen, A.; Kelly, P.; Koski, P.; Foster, C. Health benefits of different sport disciplines for adults: Systematic review of observational and intervention studies with meta-analysis. Br. J. Sports Med. 2015, 49, 434–440. [Google Scholar] [CrossRef] [Green Version]
- Meo, S.A.; Almutairi, F.J.; Alasbali, M.M.; Alqahtani, T.B.; Almutairi, S.S.; Albuhayjan, R.A.; Al Rouq, F.; Ahmed, N. Men’s Health in Industries: Plastic Plant Pollution and Prevalence of Pre-diabetes and Type 2 Diabetes Mellitus. Am. J. Men’s Health 2018, 12, 2167–2172. [Google Scholar] [CrossRef] [Green Version]
- Meo, S.A.; Bin Muneif, Y.A.; BenOmran, N.A.; Alsadhan, M.A.; Hashem, R.F.; Alobaisi, A.S. Prevalence of Prediabetes and Type 2 Diabetes Mellitus among cement industry workers. Pak. J. Med. Sci. 2020, 36, 32–36. [Google Scholar]
- Kim, J.-H.; Noh, J.; Choi, J.W.; Park, E.-C. Association of Education and Smoking Status on Risk of Diabetes Mellitus: A Population-Based Nationwide Cross-Sectional Study. Int. J. Environ. Res. Public Health 2017, 14, 655. [Google Scholar] [CrossRef] [Green Version]
- Majbauddin, A.; Tanimura, C.; Aoto, H.; Otani, S.; Parrenas, M.C.E.; Kobayashi, N.; Morita, T.; Inoue, K.; Masumoto, T.; Kurozawa, Y. Association between dental caries indicators and serum glycated hemoglobin-levels among patients with type 2 diabetes mellitus. J. Oral Sci. 2019, 61, 335–342. [Google Scholar] [CrossRef]
- American Diabetes Association. Classification and diagnosis of diabetes: Standards of medical care in diabetes. Diabetes Care 2018, 41, S13–S27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherwani, S.I.; Khan, H.A.; Ekhzaimy, A.; Masood, A.; Sakharkar, M.K. Significance of HbA1c Test in Diagnosis and Prognosis of Diabetic Patients. Biomark. Insights 2016, 11, 95–104. [Google Scholar] [CrossRef]
- Meo, S.A.; Usmani, A.M.; Qalbani, E. Prevalence of type 2 diabetes in the Arab world: Impact of GDP and energy consumption. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 1303–1312. [Google Scholar]
- Meo, S.A. Prevalence and future prediction of type 2 diabetes mellitus in the Kingdom of Saudi Arabia: A systematic review of published studies. J. Pak. Med. Assoc. 2016, 66, 722–725. [Google Scholar]
- International Diabetes Fedration (IDF). Available online: https://idf.org/our-network/regions-members/middle-east-and-north-africa/members/46-saudi-arabia.html (accessed on 12 December 2019).
- World Health Organization. Saudi Arabia. Available online: https://www.who.int/diabetes/country-profiles/sau_en.pdf (accessed on 12 December 2019).
- Feito, Y.; Patel, P.; Redondo, A.S.; Heinrich, K.M. Effects of Eight Weeks of High Intensity Functional Training on Glucose Control and Body Composition among Overweight and Obese Adults. Sports 2019, 7, 51. [Google Scholar] [CrossRef] [Green Version]
- Nieuwoudt, S.; Fealy, C.E.; Foucher, J.A.; Scelsi, A.R.; Malin, S.K.; Pagadala, M.; Rocco, M.; Burguera, B.; Kirwan, J.P. Functional high-intensity training improves pancreatic beta-cell function in adults with type 2 diabetes. Am. J. Physiol. Endocrinol. 2017, 313, E314–E320. [Google Scholar] [CrossRef] [PubMed]
- Fealy, C.E.; Nieuwoudt, S.; Foucher, J.A.; Scelsi, A.R.; Malin, S.K.; Pagadala, M.; Cruz, L.A.; Li, M.; Rocco, M.; Burguera, B.; et al. Functional high-intensity exercise training ameliorates insulin resistance and cardiometabolic risk factors in type 2 diabetes. Exp. Physiol. 2018, 103, 985–994. [Google Scholar] [CrossRef] [PubMed]
- De Sousa, M.V.; Fukui, R.; Krustrup, P.; Pereira, R.M.R.; Silva, P.R.S.; Rodrigues, A.C.; De Andrade, J.L.; Hernandez, A.J.; Da Silva, M.E.R. Positive effects of football on fitness, lipid profile, and insulin resistance in Brazilian patients with type 2 diabetes. Scand. J. Med. Sci. Sports 2014, 24 (Suppl. S1), 57–65. [Google Scholar] [CrossRef] [PubMed]
- Lao, X.Q.; Deng, H.-B.; Liu, X.; Chan, T.-C.; Zhang, Z.; Chang, L.-Y.; Yeoh, E.-K.; Tam, T.; Wong, M.C.S.; Thomas, G.N. Increased leisure-time physical activity associated with lower onset of diabetes in 44 828 adults with impaired fasting glucose: A population-based prospective cohort study. Br. J. Sports Med. 2018, 53, 895–900. [Google Scholar] [CrossRef]
- Sarmento, H.; Clemente, F.M.; Marques, A.; Milanović, Z.; Harper, L.D.; Figueiredo, A. Recreational football is medicine against non-communicable diseases: A systematic review. Scand. J. Med. Sci. Sports 2020, 30, 618–637. [Google Scholar] [CrossRef] [PubMed]
- Krustrup, P.; Helge, E.W.; Hansen, T.W.; Aagaard, P.; Hagman, M.; Randers, M.B.; De Sousa, M.; Mohr, M. Effects of recreational football on women’s fitness and health: Adaptations and mechanisms. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 118, 11–32. [Google Scholar] [CrossRef] [PubMed]
- Andersen, T.R.; Schmidt, J.F.; Thomassen, M.; Hornstrup, T.; Frandsen, U.; Randers, M.B.; Hansen, P.R.; Krustrup, P.; Bangsbo, J. A preliminary study: Effects of football training on glucose control, body composition, and performance in men with type 2 diabetes. Scand. J. Med. Sci. Sports 2014, 24 (Suppl. S1), 43–56. [Google Scholar] [CrossRef]
- Busquets-Cortés, C.; Capó, X.; Martorell, M.; Tur, J.A.; Sureda, A.; Pons, A. Training and acute exercise modulates mitochondrial dynamics in football players’ blood mononuclear cells. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 117, 1977–1987. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Parameters | Football Players (n = 378) | Control Group (n = 378) | p-Value |
|---|---|---|---|
| Age (years) | 31.80 ± 5.46 | 32.32 ± 4.37 | 0.148 |
| Height (m) | 1.72 ± 0.07 | 1.69 ± 0.07 | 0.088 |
| Weight (kg) | 77.81 ± 6.88 | 76.85 ± 6.99 | 0.060 |
| BMI (kg/m2) | 26.40 ± 2.08 | 26.66 ± 1.87 | 0.068 |
| Parameters | Football Players (n = 378) | Control Group (n = 378) | p-Value |
|---|---|---|---|
| Non-diabetic (HbA1c < 5.7%) | 342 (90.48%) | 218 (57.67%) | 0.001 |
| Prediabetic (HbA1c 5.7–6.4%) | 30 (7.96%) | 71 (18.78%) | 0.001 |
| Diabetic (HbA1c > 6.4%) | 6 (1.59%) | 89 (23.54%) | 0.001 |
| Parameters | HBA1C | |
|---|---|---|
| Pearson Correlation Coefficient | p-Value | |
| Age (years) | 0.026 | 0.479 |
| BMI (kg/m2) | −0.008 | 0.817 |
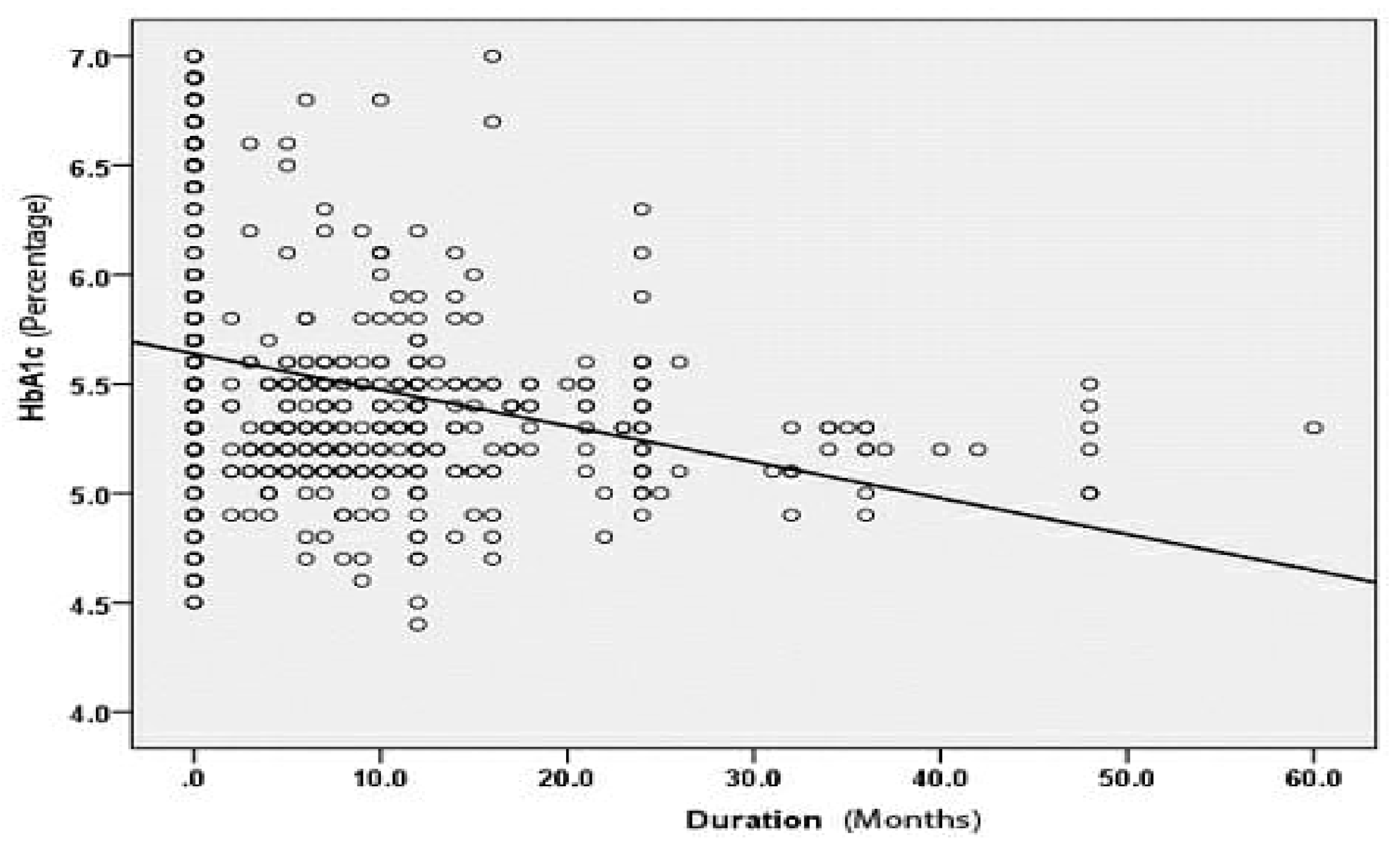
| Duration (months) | −0.278 ** | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meo, S.A.; Abukhalaf, A.A.; Alomar, A.A.; Alessa, O.M.; Sumaya, O.Y.; Meo, A.S. Prevalence of Prediabetes and Type 2 Diabetes Mellitus in Football Players: A Novel Multi Football Clubs Cross Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 1763. https://doi.org/10.3390/ijerph18041763
Meo SA, Abukhalaf AA, Alomar AA, Alessa OM, Sumaya OY, Meo AS. Prevalence of Prediabetes and Type 2 Diabetes Mellitus in Football Players: A Novel Multi Football Clubs Cross Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(4):1763. https://doi.org/10.3390/ijerph18041763
Chicago/Turabian StyleMeo, Sultan Ayoub, Abdulelah Adnan Abukhalaf, Ali Abdullah Alomar, Omar Mohammed Alessa, Omar Yassin Sumaya, and Anusha Sultan Meo. 2021. "Prevalence of Prediabetes and Type 2 Diabetes Mellitus in Football Players: A Novel Multi Football Clubs Cross Sectional Study" International Journal of Environmental Research and Public Health 18, no. 4: 1763. https://doi.org/10.3390/ijerph18041763
APA StyleMeo, S. A., Abukhalaf, A. A., Alomar, A. A., Alessa, O. M., Sumaya, O. Y., & Meo, A. S. (2021). Prevalence of Prediabetes and Type 2 Diabetes Mellitus in Football Players: A Novel Multi Football Clubs Cross Sectional Study. International Journal of Environmental Research and Public Health, 18(4), 1763. https://doi.org/10.3390/ijerph18041763