Abstract
A systematic review and meta-analysis were employed to address the associated factors of gender-based violence (GBV) in sub-Saharan African (SSA) countries. The Preferred Reporting Items for Systematic reviews and Meta-Analysis guidelines were followed. Ovid Medline, CINAHL, Cochrane Central, Embase, Scopus and Web of Science were used to source articles with stringent eligibility criteria. A total of 4931 studies were found and 50 studies met the inclusion criteria. Pooled meta-analyses revealed that low educational attainment, higher alcohol consumption, substance use, history of child and family abuse, limited decision-making skills, experiencing depression, males having multiple sexual partners, and younger age were found to be individual- and family-associated factors that increase the experiences of GBV. Community tolerant attitudes to violence, women’s unemployment, being Muslim, lower socioeconomic class, food and social insecurity were found to be community- and societal-associated factors of GBV. Alcohol consumption, low educational attainment, experiencing depression, being younger, a history of child and family abuse, tolerant attitudes to violence, and low socioeconomic status were poignant factors associated with GBV amongst women in SSA countries. The need to develop a multipronged approach of intervention is a top priority in SSA to reach the Sustainable Development Goals’ (SDGs) target of 2030 to eliminate all forms of violence. Socio-behavioural change communication interventions at individual and community levels need to be introduced, and interventions need to address the prevention of child and family abuse and increase women’s feelings of empowerment in order to prevent GBV in SSA.
1. Introduction
Globally, GBV is an important public health problem and human right violation challenge, worsening in developing countries including SSA [1,2]. The experience of GBV threatens the lives of many women and limits the autonomy of women to address health as a primary concern for themselves and their children [3]. According to the United Nations (UN), GBV is defined as “any act of gender based violence that results in, or is likely to result in, physical, sexual, or mental harm or suffering to women, including threats of such acts, coercion or arbitrary deprivation of liberty, whether occurring in public or in private life” [1,3]. GBV encompasses physical, sexual and psychological abuse from intimate and non-intimate partners [1,3].
Worldwide, it is estimated that one in three women will experience at least one form of GBV during their lifetime experience, from as young as 15 years of age [1]. The prevalence of GBV is intensified in developing countries, such as SSA countries, where socioeconomic status is low and access to education is limited [4]. According to a systematic review and meta-analysis study conducted in SSA in 2020, the prevalence of IPV is as high as 44% and 14% for non-IPV [5], and is one of the worst regions for reporting GBV in comparison to global dimensions [4]. Researchers further explained that the prevalence rate might be higher if there were no barriers to reporting these cases. The barriers include: fear of stigma, revenge, women considering the matter as a private issue, fear of financial barriers and lack of law enforcement, just to mention a few [4].
This study only focused on SSA countries due to evidence showing GBV prevalence is high this region [5] and most available studies are limited to developed countries [1,3,4]. Moreover, researchers reported that factors related to GBV are complex and most available studies are restricted to developed countries, with limited evidence focused on SSA countries [1,2]. Some factors are protective against GBV and other factors may increase the likelihood of GBV [6]. Hence, understanding the factors related to GBV aims to contribute to the field of GBV and complement the existing evidence in order to design comprehensive interventions and inform policy makers.
Various theoretical approaches, views and frameworks have been adopted to explain the potential associated factors that might increase the chance of GBV including gender perspectives or feminist theories and sociological and ecological theories [7]. The ecological framework is the most widely used framework in public health research on GBV [3,7]. The ecological model considers the complex interplay between individual, relationship, community and societal factors that may lead to GBV [7]. This review applied the ecological framework as an exploratory tool to systematically explore associated factors of GBV.
2. Methods
The Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) guidelines were followed [8]. PRISMA is an evidence-based minimum set of items for reporting in systematic reviews and meta-analyses. PRISMA focuses on the reporting of reviews, evaluating studies, and is used as a basis for reporting systematic reviews of various types of research, particularly evaluations of interventions. Ovid Medline, CINAHL, Cochrane Central, Embase, Scopus and Web of Science were used to source articles with stringent eligibility criteria. The search also included grey literature. CASP is a set of critical appraisal tools designed to be used when evaluating research. CASP has appraisal checklists designed for use with systematic reviews, randomised controlled trials, cohort studies, case–control studies, economic evaluations, diagnostic studies, qualitative studies and clinical prediction rules [9]. The quality of included studies was appraised using Critical Appraisal Skills Program (CASP) for cross-sectional studies [9]. The overall quality of each paper was rated on a ten-point scale that was scored from zero (none of the quality measures were met) to ten (all of the quality measures were met). The quality of the paper was based on the sum of points awarded, representing the overall quality score of the study. Studies were rated as poor quality (score ≤ 6), medium quality (7–8), and high quality (≥9) (Table S1). There were no studies excluded due to poor quality. Data were extracted from studies using a specially developed Excel tool for data extraction.
Two reviewers independently extracted and assessed the quality of the articles. Studies published in SSA countries between 2008 and 2019 were included. The year 2008 was used as a baseline as a year of a greater global commitment to addressing violence against women; there has been a rapid expansion in the number of population studies examining GBV [10] since that time. Gender-based violence, intimate partner violence, domestic violence, physical abuse, emotional violence, reproductive coercion, sexual assault, sub-Saharan countries, women aged 15–49 years, determinants predictors and associated factors were the search terms and words used when performing the review search (Table S1).
Studies were included if they (i) focused on the associated factors of GBV; (ii) included females in the age range of 15–49 years; (iii) were studies conducted in SSA countries [11] including Benin, Burkina Faso, Cape Verde, Gambia, Ghana, Guinea, Guinea-Bissau, Ivory Coast, Liberia, Mali, Mauritania, Niger, Nigeria, Senegal, Sierra Leone, Togo, Cameroon, Central African Republic, Chad, Congo Republic-Brazzaville, Democratic Republic of Congo, Equatorial Guinea, Gabon, Sao Tome and Principe, Angola, Botswana, Lesotho, Mozambique, Namibia, South Africa, Swaziland, Zambia, Zimbabwe, Burundi, Comoros, Djibouti, Eritrea, Ethiopia, Kenya, Madagascar, Malawi, Mauritius, Rwanda, Seychelles, Somalia, Somaliland, Tanzania and Uganda; (iv) were published in English from 2008 to 2019; and (v) were quantitative studies
Gender-based violence was measured using the Demographic and Health survey (DHS) tool. The following key questions focused on experiences within women’s relationships, perpetrated by their husband/partner. Women were asked about physical violence experiences including push you, shake you, or throw something at you, slap you; twist arm or pull, punch you with his/her fist or with something that could hurt you; choke you or burn you on purpose; threaten or attack you with a knife and gun. Sexual violence experiences included: physically force to have sexual intercourse, physically force to perform any other sexual acts without need, and force you with threats or in any other way to perform sexual acts. Emotional violence experiences include say or do something to humiliate; threaten to hurt or harm you or someone close to you; and insult you or make you feel bad.
The metan command provides methods for the meta-analysis of studies with two groups. The effect measure with binary data is the difference between the ratio of two proportions (risk ratio), or the odds ratio. The syntax “metan” in Stata version 16.0 [12] was used to generate forest plots for each of the pooled effects. In a forest plot, the contribution of each study to the meta-analysis (its weight) is represented by the area of a box whose centre represents the size of the treatment effect estimated from that study (point estimate). A test of heterogeneity of each of the study datasets was obtained for the different authors and showed levels of inconsistency (I2 > 50%), thereby warranting the use of a random effects model in all the meta-analyses. The I2 statistic describes the percentage of variation across studies that is due to heterogeneity rather than chance. The metabias command performs the tests for funnel plot asymmetry proposed by Egger [13]. Sensitivity analyses were attended to examine the effect of outliers [13]. Egger’s test was used for publication bias. Publication bias is usually defined as the tendency for authors to publish studies with significant results. This bias might be for various reasons; for instance, selective publication of studies based on the direction and magnitude of their results, and studies without statistical significance (negative studies) being less likely to be published. Biased results from pooling the results from published studies alone are some of the examples.
3. Results
3.1. Description of Included Studies
A total of 4931 articles, citations and 6 grey literature articles were included. After removing duplicates, 3275 titles and abstracts were screened. Of these, 245 full-text articles were retrieved. Fifty studies met the inclusion criteria about the associated factors of GBV (Figure 1).
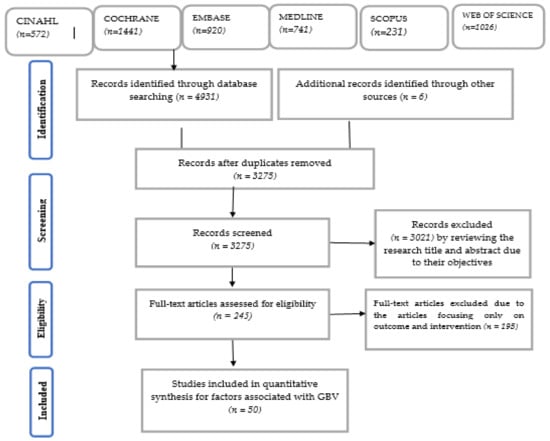
Figure 1.
PRISMA flow chart that describes selection process of GBV articles that met inclusion criteria.
Fifty articles met the inclusion criteria and were reviewed for data analysis and interpretation (Table 1). The majority of studies were cross-sectional studies; sample size ranged from 150 to 86,024, and random sampling techniques were used to attempt to reduce bias (Table S1).

Table 1.
Summarised description of studies on the risk of GBV.
3.2. Associated Factors of GBV
This systematic review and meta-analysis report has been organised using the ecological framework that correlates individual, relationship, community and societal levels.
3.2.1. Individual Level Risk Factors of GBV
Education status of women and partner- In this review, researchers found that women’s low levels of education attainment were associated with a higher number of GBV experiences [15,40,62,63]. Similarly, other researchers found that the educational level of the woman’s partner was an important factor for women experiencing GBV [6,22,31,40,56]. This review has highlighted that if both the woman and her partner have higher educational levels, they are less likely to experience GBV [31].
Overall, the meta-analysis showed that there was a significant association [OR: 1.35; 95% CI (1.13, 1.57)] between women and their partner’s educational level and experiences of GBV. Moreover, the subgroup analysis showed that the higher educational level of the woman was the most important factor [OR: 1.50; 95% CI (1.53, 1.78)] in reducing the chances of experiencing GBV (Figure 2). Egger’s test (p = 0.273) shows no publication bias (Figure S2). The I2 statistic describes the percentage of variation across studies that is due to heterogeneity rather than chance
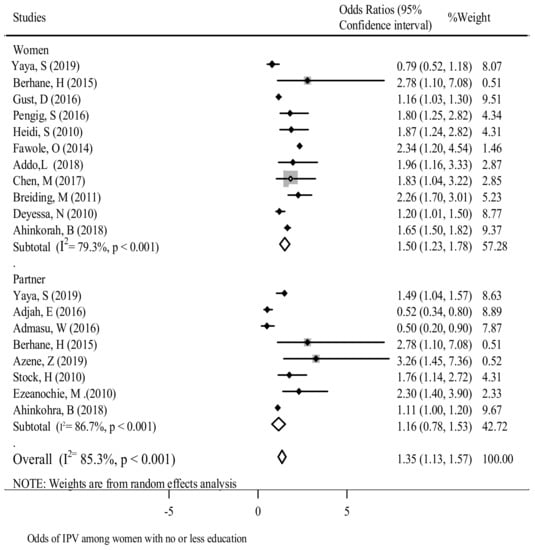
Figure 2.
The association between education and experience of reporting GBV in SSA.
Alcohol consumption - In various studies, alcohol consumption by women or their partner was found to be positively associated with GBV. Women who drank alcohol on a daily basis were more likely to experience GBV in comparison to women who did not drink alcohol [15,27,36,37,40,46,53]. Similarly, the likelihood of reporting GBV amongst women was very high when their partners consumed alcohol on a daily basis in comparison to women whose partners did not consume alcohol [16,21,40,48,49].
The pooled OR revealed that drinking alcohol increased the odds of women experiencing GBV by 2.4-fold [OR: 2.4; 95% CI (1.94, 2.85)]. The subgroup analysis showed the highest chances of violence occurred when women drank alcohol (Figure 3). The heterogeneity (Egger test p = 0.71) is shown in Figure S3.
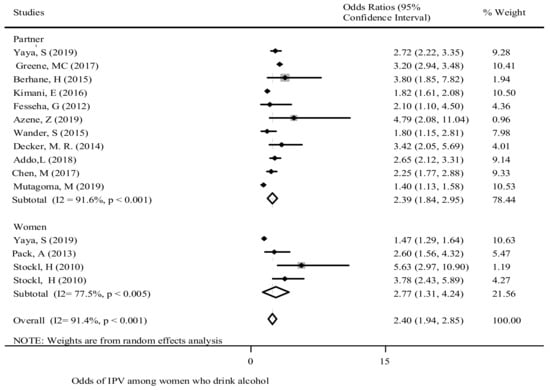
Figure 3.
The association of drinking alcohol and experience of reporting GBV in SSA.
Substance use - Substance use was one of the factors that was positively associated with women’s experiences of GBV [35,44]. A multi-country study showed that women who used marijuana over the course of their lifetime were 4.7 times more likely to experience GBV [OR: 4.66; 95% CI (2.21, 9.85)] in comparison to non-users. The pooled effect of substance use was significantly associated with women’s experience of GBV. Women using substances were twice as likely to experience GBV in comparison to those who did not [OR: 1.68; 95% CI (1.5, 1.89)] (Figure 4) with the Egger test (p = 0.551) (Figure S4).
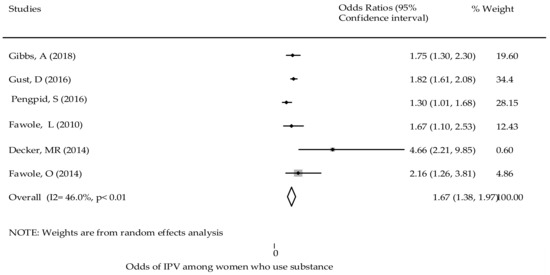
Figure 4.
The association of substance use and the experience of reporting GBV in SSA.
Age of women and partners - In this review, many of the findings revealed that young women who were 15 to 19 years of age experienced a higher prevalence of GBV than adult women [6,14,31,46,54,63,64]. Two studies found that moderate age differences between partners were associated with high levels of GBV [49,54]. In contrast, other studies showed greater differences in age were less likely to experience IPV [15,49] (Table 1).
Decision-making skills - In this review, women’s autonomy to make a decision was an important predictor in whether she was likely to experience GBV. For instance, women were classified as participating in decision-making if they made decisions alone or jointly with their partner and included when women decided on major purchases, own health care access and visits to family. Women having strong decision-making skills were positively associated with lower levels of experience of GBV [15,29,45,47,50,65]. The overall pooled effects of decision-making skills with experiences of GBV were significant [OR: 0.68; 95% CI (0.41, 0.95)]. Women who have better decision-making skills had a 32% lower chance of experiencing GBV in comparison to those who had little decision-making skills (Figure 5). Egger’s test demonstrated no publication bias (p = 0.426) (Figure S5).
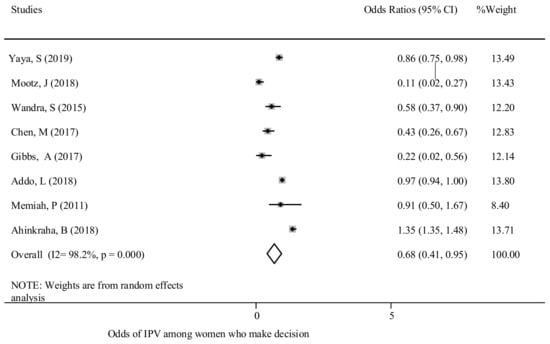
Figure 5.
The association between GBV experience and decision-making power.
Attitudes of women and partners - This review found that experiences of GBV were associated with attitudes of women and their partners. Women and men who are more tolerant of GBV are more likely to consider abuse against women as being normal [17,37,47,48,49]. The overall pooled effect showed that women who were more tolerant towards GBV were twice as likely [OR: 2.38; 95% CI (1.26, 3.5] to experience GBV in comparison to those who were intolerant (Figure 6). Egger’s test (p = 0.033) results are shown in Figure S6.
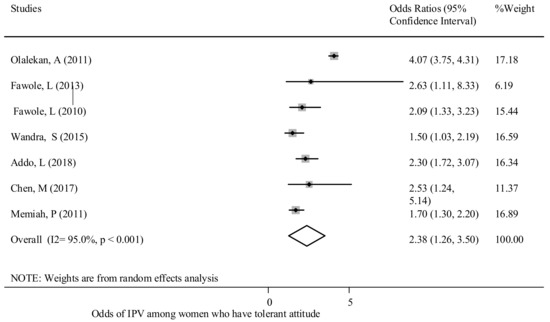
Figure 6.
The association between tolerant attitude and experience of reporting GBV in SSA.
Experiencing depression - This review found that GBV was positively associated with experiencing depression. In six studies, the findings showed that women experiencing depression or depressive symptoms were more likely to experience GBV [20,40,46,48,66]. For instance, a study conducted in SSA countries showed that women were almost two-thirds (63%) more likely to experience sexual violence if they were experiencing post-traumatic stress disorder (PTSD) [40]. A similar trend was reported in other studies [20,46].
History of child abuse - Researchers found that experiences of child abuse were positively associated with experiences of GBV against women [35,53,67]. The occurrence of GBV was found to be higher among women that had experienced physical, sexual and emotional abuse as a child [48,52,53]. Overall, experiencing child abuse was found to be a predictor of GBV in the later life span of women. Women who experienced child abuse were 2.3 times more likely to experience GBV in comparison to women who did not experience child abuse [OR: 2.33; 95% CI (1.71, 2.96)] (Figure 7). The test showed no publication bias (Egger’s test p = 0.61) (Figure S7).
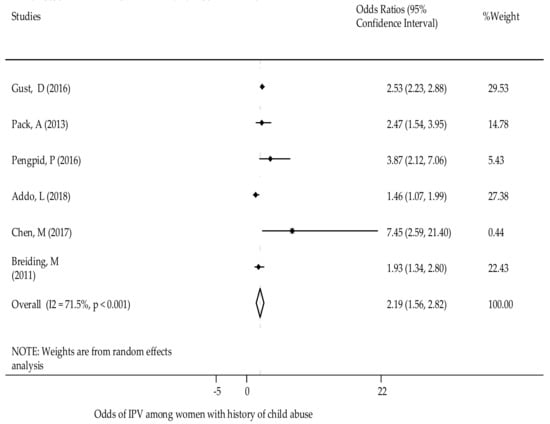
Figure 7.
The association of history of child abuse and GBV experience.
3.2.2. Relationship Risk Factors of GBV
Males having multiple sexual partners - The odds of reporting GBV was found to be higher amongst women whose partners had multiple sexual partners [23,35,36,46,48]. A study conducted in African countries indicated that males with two or more sexual partners over the past year increased the chance of women experiencing GBV by 1.78 times [35]. Similarly, a study in Nigeria showed polygamous unions doubled the chance of experiencing GBV [36].
Previous history of parental abuse - A previous history of parental abuse (if women experienced abuse as a child by a parent) was positively associated with current experiences of GBV [21,48,68]. The chances of experiences of violence against women were higher if a woman had a parental history of violence [21,36] (Table 1). The overall pooled estimate found there was an association between a previous family history of violence and experiences of GBV. Women who had a parental history of violence were twice as likely to experience GBV (Figure 8). There was no publication bias (Egger’s test p = 0.715) (Figure S8).
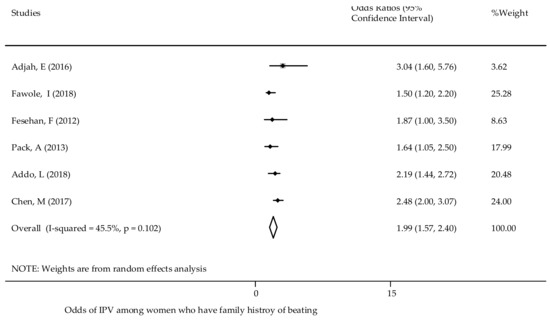
Figure 8.
The association of family history of physical violence and experience of reporting GBV in SSA.
Living arrangement with partner and early marriage - Studies have found that early marriage was associated with GBV [14,63]. The odds of GBV were higher if the woman was married, cohabiting, or having a relationship [26,31,54]. Similarly, studies showed women living without their partner were less likely to experience GBV as compared to women living with their partner [31,40] (Table 1).
3.2.3. Community Level Risk Factors of GBV
Community Attitude towards violence - Community attitudes towards GBV were a strong predictor for the occurrence of any form of GBV [49,60,67]. Women with more tolerant attitudes towards GBV in the community were 41% more likely to experience spousal violence [67]. Another study found that if the community accepted violence, women were four times more likely to experience IPV [49]. A study was conducted in Rwanda about health workers’ experience of workplace violence or any form of discrimination, including gender discrimination (defined as “any distinction, exclusion or restriction made on the basis of socially constructed gender roles and norms that prevents a person from enjoying full human rights”) [69]. Gender equality lowered the odds of health workers experiencing violence [60,69].
Employment and occupational status - Researchers found that employment increased the likelihood of experiencing or reporting GBV [50,58]. A multi-country study revealed the odds of experiencing IPV was 33% higher amongst women who were employed in comparison to those who were unemployed [58]. Researchers found that health care workers were more likely to experience GBV [57,58,61], particularly emotional violence. Nurses and midwives [OR: 4.06; 95% CI (1.20, 13.74)] were more likely to experience workplace violence in comparison to other health care workers [28,30] (Table 1).
Area of residence - Some studies found that women residing in rural areas were more likely to experience GBV in comparison to women in urban settings [31,34,63]. In contrast, a multi-country study indicated that women living in rural residences were 20% less likely to experience GBV in comparison to women living in urban residences [15,21,50].
3.2.4. Societal Level Risk Factors
Socioeconomic status - Nine studies reported the association between socioeconomic status and GBV. Most studies found that lower socioeconomic status was positively associated with experiencing GBV [15,16,49,50,58,62]. Researchers identified that women with a poor wealth index were more likely to report GBV in comparison to women with a higher wealth index [50,58] (Table 1).
Food and Social Security - Researchers found that poor food security had a positive association with violence against women. Two studies in South Africa found that household food insecurity was positively associated with women experiencing GBV [38,45]. A study conducted in Côte d’Ivoire [50] found that poor social security and lack of social freedom were associated with experiencing IPV. Additionally, this review showed that police refusing to protect women against violence was associated with physical [OR: 2.8; 95% CI (1.7, 4.4)] and sexual violence [OR: 3.0; 95% CI (1.9, 4.8)] [50].
4. Discussion
This comprehensive systematic review provides a plethora of information on the overall associated factors that augment the occurrences of GBV in SSA countries. This systematic review has identified that women’s experiences of GBV in SSA are associated with many factors that are related to individual, interpersonal, community and societal levels.
4.1. Individual and Relationship Factors
Poor education status, alcohol consumption, substance use, young age, limited decision-making skills, tolerant attitudes towards violence, experiencing depression, history of child abuse and parental abuse (if woman was abused by a parent), males having multiple sexual partners, living arrangements and early marriage were the most consistently identified individual and relationship risk factors that increased the experiences of GBV in SSA countries. Women’s alcohol consumption, tolerant attitudes towards violence and substance use were positively associated with experiencing GBV. This might be related to women’s inability to anticipate the potential risks, consequences and lack of conscious reflection towards GBV as a result of alcohol and substance use. Hence, women that do not consume alcohol or substances may reflect more positively about their circumstances in comparison to those who practise risky behaviours [47]. This is consistent with many other studies [10,50,64]. Women may be exposed to GBV from an early age and this might be related to the patriarchal situation of men’s dominance in SSA countries [24,70]. The following paragraphs will provide a more comprehensive discussion about these factors.
Secondary and higher educational status is the most important factor that will reduce experiences of GBV. Studies have shown that women who are better educated have a heightened understanding about preventing GBV as they are more conscious and aware of GBV in their community [15,36,71,72]. Higher education predisposes women to the effects of GBV in society and exposes women to global discourses and discussions that reject any form of violence. Women who are less educated may not understand how to implement mitigation measures against violence. They are also more likely to have limited exposure to legal support and herald tolerant attitudes to GBV. Women in SSA are mostly uneducated and, therefore, are likely to be subjected to the patriarchal male dominance that infiltrates their communities and increases the chances of being exposed to GBV. This situation poses other health and economical challenges.
Increased decision-making skills enable women to be empowered about understanding the availability of resources and this may contribute to varying power levels within the couple’s relationship that may influence more accessibility to health, social and economic services. As a result, if women are able to exercise choice and control within their relationship, they are less likely to experience GBV [73,74]. However, researchers suggest that developing shared decision-making skills will assist in preventing IPV. If women have high decision-making skills and are not inclusive of their spouse, they are more likely to experience GBV [19,29,58,65]. Decision-making skills are more compromised when the woman and her partner drink excessive alcohol and this may influence and increase any violence or criminal activities [3]. If women or their partners consume excessive amounts of alcohol, this may impair a person’s judgement and increase the likelihood of violence [19,29,65].
Women who experience depression were more likely to experience GBV. These findings are consistent with studies conducted in various countries [20,75]. GBV is more likely to occur in women with low self-esteem and women who fear humiliation, stigma and discrimination that further aggravate experiences of depression [2]. Women experiencing depression are more likely to roam the streets in SSA and are, therefore, more prone to experiencing GBV [20,75].
Women who have experienced previous child abuse are more likely to experience GBV as adult women. In this study, we found that previous child abuse doubles the chances of adult women experiencing GBV. This intergenerational cycle of violence might be attributed to continual exposure to violence during their childhood and increases the chances of women experiencing GBV later in their adult life. Children’s exposure to GBV poses long-term health and social consequences. This is strongly correlated with the sociological theory of violence. This means that violent acts within a family are reinforced during childhood and increases the chances of violence being experienced as adults. There is an assumption that there is an “intergenerational transmission” or “cycle of violence” [7]. This positive association has been described in many other studies [1,7].
This review has shown that partners’ promiscuous behaviour is an important predictor of experiencing GBV amongst women. The identified relational factors include alcohol consumption, having multiple sexual partners, previous history of abuse, and negative attitudes of partners, which significantly increased the occurrences of GBV. Consistent with these findings, many other developed countries and some African countries found an association between the partner’s promiscuous behaviour and experiences of GBV amongst women [9,63,72,73]
Although there is a tendency of reducing polygamy throughout SSA, men continue to exercise sexual freedom by having multiple sexual partners even whilst they are married or cohabitating with a woman. Having multiple sexual partners was found to be an important relationship risk factor for occurrences of GBV. This may be related to disrespect towards their female partners and may cause detachment, resulting in poor psychological and emotional bonding. The partner’s promiscuous behaviour may also expose women to sexually transmitted infections including HIV [4,73].
Similarly, the review revealed women are at higher risk of IPV if they marry before the age of 18 years. In many African countries, one of the drivers of early marriage is the family belief that if a young woman marries before having sexual intercourse, they will be protected from physical and sexual assaults, although this does not occur in reality in terms of IPV. There are a myriad of potential reasons why early marriage leads to higher levels of violence and this might be attributed to married women being less educated, being disempowered economically, and being influenced by her partner and the community, resulting in low decision-making skills and lack of autonomy. At the same time, greater age differences between partners are more likely to result in increased levels of GBV [14,34,63,64]
4.2. Community and Societal Factors
In this review, a limited number of factors were identified at the community and societal levels. This is mainly due to the limited research available about risk factors, rather than reflecting a true picture about experiences of GBV.
A community harbouring tolerant attitudes to violence was positively associated with higher levels of women experiencing GBV. Communities that harboured adverse attitudes towards violence were less likely to experience GBV. These communities were likely to support gender equities. Unfortunately, in most African countries, the system is patriarchal and prejudiced towards promoting male dominance, and fear was also a contributory factor of not reporting violence [1,2,16,67,69].
This review found that GBV was more likely to occur amongst employed women in comparison to unemployed women. This finding could reflect men’s disapproval of women’s independence and them being socially and financially stable. There could be a community expectation that a woman’s place is in the home as a family carer. Consequently, partners may be more likely to abuse women, especially if the partner is not the main breadwinner and is unemployed. The majority of employed workers in SSA are male and this predisposes the workplace towards more lenient laws against GBV. Women are also more likely to work in lower paid positions, increasing the chance of supervisors being perpetrators of violence. Alternatively, women who are unemployed are more likely to remain silent about experiencing violence due to fear of unrest within the family, harbouring tolerant attitudes towards violence and being economically dependent on their partner [2,24,67,70].
The socioeconomic status of women in the community and food security were found to be important societal predictors for experiencing GBV. Lower socioeconomic status and limited food security were generally associated with higher levels of experiences of GBV. Women may have limited access to different services, including educational services. Other reasons may be due to overcrowding of living areas and being dependent on others, which predisposes them to subordinate acts of violence [2,76]. Many women migrate to urban settings and engage in prostitution to earn their income and this increases the chance of GBV in many young African women. Studies showed that female sex workers are more likely to experience higher GBV in comparison to other women [1,5,74,77].
Furthermore, this review has highlighted that if both a woman and her partner have higher educational levels, resources or higher socioeconomic class, this is positively associated with lower levels of GBV. However, the level of violence was also associated with the partner’s individual risk factors. Gender inequalities could also account for consequences such as divorce and increased revenge including homicide, trafficking and stigmatising women, which is consistent with various studies [75,76].
4.3. Strengths and Limitations of This Review
This is the first systematic review and meta-analysis that has further explored SSA countries and will assist in designing an intervention. A rigorous search was conducted from multiple electronic databases. A quality assessment was conducted and two independent reviewers conducted the screening. Stringent eligibility criteria were developed. Despite this, the search only included articles published in English. All the studies were observational in design and only established relationships between variables, rather than causative factors. The quality of the evidence was dependent on the credibility of the original research findings. The study was not supported by qualitative studies.
4.4. Implications for Social Policy, Practice, and Research
This study provides vital evidence to inform policy and guide social and health organisations to respond and to prevent violence in alignment with the Sustainable Development Goals (SDGs) (also known as the Global goals and adopted by all United Nations Member States in 2015 as a universal call to action to end poverty, protect the planet and ensure that all people enjoy peace and prosperity by 2030). SDG 1 relates to no poverty and SDG 5 relates to gender equality [78]. Many factors were identified that are associated with increased experiences of GBV. Hence, prioritising the factors and the prevention of violence is an integral component of individual, human, social and economic development agendas that should commence sooner rather than later.
These research findings provide extensive evidence to develop integrated individual- and family-tailored interventions that address the prevention of GBV. This work should extend to the community to initiate social changes that will address gender inequity and economic development to improve the living conditions and socioeconomic status of women and their families. This research has provided further stimulus to develop interventions that target GBV in SSA countries and has narrowed existing gaps in the literature. However, there is a need for further studies, including qualitative studies, to focus on interventions to reduce GBV.
5. Conclusions and Recommendation
Predictors that increase experiences of GBV include women and men with lower levels of education, increased levels of alcohol consumption by the woman and/or her partner, adolescent and young mothers, women with limited decision-making skills, women with a previous history of child abuse, women who have experienced depression, individual and community tolerant attitudes to GBV, employed women, low socioeconomic status and limited food security. Due to the complexity of factors associated with GBV, the need to develop an integrated comprehensive intervention approach is a top priority to eliminate GBV and reach the United Nation SDG targets of 2030 in SSA. This would include introducing socio-behavioural change communication interventions at both individual and community levels. Primary preventative methods that will address GBV in SSA should incorporate interventions that target both child and family abuse, increase access to educational facilities and result in women’s empowerment in their struggle towards elimination of all forms of violence.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/ijerph18094407/s1, Figure S1: Prisma flow chart that describes selection process of GBV articles that met inclusion criteria; Table S1. Appraisal of Quantitative Studies using CASP; Figure S2. Funnel plot for studies focused on education and GBV; Figure S3: Funnel plot for studies on alcohol consumption and GBV; Figure S4: Funnel plot for studies focused on substance use and GBV; Figure S5. Funnel plot for studies on decision-making skills and GBV; Figure S6. Funnel plot for studies on tolerant attitudes and GBV; Figure S7. Funnel plot for studies on history of child abuse and GBV; and Figure S8. Funnel plot for studies on family history of abuse and GBV.
Author Contributions
M.D.M., L.F., K.A. & V.S. were involved in the conceptualization of this study. M.D.M. carried out the analysis and drafted the manuscript. V.S., L.F., and K.A. were involved in the revision and editing of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study used secondary data that are available in the public domain. In addition, ethical approval was secured from Western Sydney University Ethics Committee as a requirement for academic study.
Informed Consent Statement
Not applicable.
Acknowledgments
We would like to thank the Western Sydney University web library for access and Maereg Wagnew who supported us during data extractions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Garcia-Moreno, C.; Jansen, H.A.; Ellsberg, M.; Heise, L.; Watts, C.H. Prevalence of intimate partner violence: Findings from the WHO multi-country study on women’s health and domestic violence. Lancet 2006, 368, 1260–1269. [Google Scholar] [CrossRef]
- Palermo, T.; Bleck, J.; Peterman, A. Tip of the Iceberg: Reporting and Gender-Based Violencein Developing Coun-tries. Am. J. Epidemiol. 2014, 179, 602–612. [Google Scholar] [CrossRef] [PubMed]
- García-Moreno, C.; Amin, A. The Sustainable Development Goals, Violence and Women’s and Children’s Health; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Abrahams, N.; Jewkes, R.; Laubscher, R.; Hoffman, M. Intimate partner violence: Prevalence and risk factors for men in Cape Town, South Africa. Violence Vict. 2006, 21, 247–264. [Google Scholar] [CrossRef]
- Muluneh, M.D.; Stulz, V.; Francis, L.; Agho, K. Gender Based Violence against Women in Sub-Saharan Africa: A System-atic Review and Meta-Analysis of Cross-Sectional Studies. Int. J. Environ. Res. Public Health 2020, 17, 903. [Google Scholar] [CrossRef] [PubMed]
- Fawole, O.I.; Dagunduro, A.T. Prevalence and predictors of violence against female sex workers in Abuija. Niger. Afr. Health Sci. 2014, 14, 215. [Google Scholar]
- Heise, L.L. Determinants of partner violence in low and middle-income countries: Exploring variation in individual and population-level risk. Lond. Sch. Hyg. Trop. Med. 2012. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Center for Evidence Based Management. Critical Appraisal Checklist for Cross-Sectional Study. Available online: https://www.cebm.net/2014/06/critical-appraisal/ (accessed on 20 August 2014).
- Devries, K.M.; Mak, J.Y.; Garcia-Moreno, C.; Petzold, M.; Child, J.C.; Falder, G.; Lim, S.; Bacchus, L.J.R.; Engell, L.E.; Watts, C.H.; et al. The Global Prevalence of Intimate Partner Violence against Women. Science 2013, 340, 1527–1528. [Google Scholar] [CrossRef]
- UN. Population Preview. 2019. Available online: http://worldpopulationreview.com/continents/sub-saharan-africa-population/ (accessed on 11 November 2019).
- Statistics Sierra Leone (SSL) and ICF International. Sierra Leone Demographic and Health Survey 2013; SSL and ICF International: Freetown, MD, USA, 2014. [Google Scholar]
- Patsopoulos, N.A.; Evangelou, E.; Ioannidis, J.P. Sensitivity of between-study heterogeneity in meta-analysis: Proposed metrics and empirical evaluation. Int. J. Epidemiol. 2008, 37, 1148–1157. [Google Scholar] [CrossRef]
- Bleck, J.; Palermo, T. Age and intimate partner violence: An analysis of global trends among women experiencing victim-ization in 30 developing countries. J. Adolesc. Health 2015, 57, 624–630. [Google Scholar]
- Yaya, S.; Ghose, B. Alcohol Drinking by Husbands/Partners is Associated with Higher Intimate Partner Violence against Women in Angola. Safety 2019, 5, 5. [Google Scholar] [CrossRef]
- Greene, M.C.; Furr-Holden, D.M.; Tol, W.A. Alcohol use and intimate partner violence among women and their partners in Sub-Saharan Africa. Drug Alcohol Depend. 2017, 171, e77. [Google Scholar] [CrossRef][Green Version]
- Fawole, O.I.; Asekun-Olarinmoye, E.O.; Osungbade, K.O. Are very poor women more vulnerable to violence against women? Comparison of experiences of female beggars with homemakers in an urban slum settlement in Ibadan, Nigeria. J. Health Care Poor Underserved 2013, 24, 1460–1473. [Google Scholar] [CrossRef]
- Ezeanochie, M.C.; Olagbuji, B.N.; Ande, A.B.; Kubeyinje, W.E.; Okonofua, F.E. Prevalence and correlates of intimate partner violence against HIV-seropositive pregnant women in a Nigerian population. Acta Obs. Gynecol. Scand. 2011, 90, 535–539. [Google Scholar] [CrossRef] [PubMed]
- Mootz, J.J.; Muhanguzi, F.K.; Panko, P.; Mangen, P.O.; Wainberg, M.L.; Pinsky, I.; Khoshnood, K. Armed conflict, alcohol misuse, decision-making, and intimate partner violence among women in Northeastern Uganda: A population level study. Confl. Health 2018, 12, 37. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, A.; Jewkes, R.; Willan, S.; Washington, L. Associations between poverty, mental health and substance use, gender power, and intimate partner violence amongst young (18–30) women and men in urban informal settlements in South Africa: A cross-sectional study and structural equation model. PLoS ONE 2018, 13, e0204956. [Google Scholar] [CrossRef]
- Adjah, E.S.O.; Agbemafle, I. Determinants of domestic violence against women in Ghana. BMC Public Health 2016, 16, 368. [Google Scholar] [CrossRef]
- Abate, B.A.; Wossen, B.A.; Degfie, T.T. Determinants of intimate partner violence during pregnancy among married women in Abay Chomen district, Western Ethiopia: A community based cross sectional study. BMC Women’s Health 2016, 16, 16. [Google Scholar] [CrossRef] [PubMed]
- Fawole, O.I.; Balogun, O.D.; Olaleye, O. Experience of gender-based violence to students in public and private secondary schools in Ilorin, Nigeria. Ghana Med. J. 2018, 52, 66–73. [Google Scholar] [CrossRef]
- Okenwa, L.E.; Lawoko, S.; Jansson, B. Exposure to Intimate Partner Violence amongst Women of Reproductive Age in Lagos, Nigeria: Prevalence and Predictors. J. Fam. Violence 2009, 24, 517–530. [Google Scholar] [CrossRef]
- Berhanie, E.; Gebregziabher, D.; Berihu, H.; Gerezgiher, A.; Kidane, G. Intimate partner violence during pregnancy and adverse birth outcomes: A case-control study. Reprod. Health 2019, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Gust, D.A.; Yi, F.; Otieno, T.; Hayes, T.; Omoro, P.A.; Phillips-Howard, F.; Odongo, G.O. Factors associ-ated with physical violence by a sexual partner among girls and women in rural Kenya. J. Glob. Health 2017, 7, 125–135. [Google Scholar]
- Kimani, E.; Osero, J.; Akunga, D. Factors increasing vulnerability to sexual violence of adolescent girls in Limuru sub-county, Kenya. Afr. J. Midwifery Women’s Health 2016, 10, 188–191. [Google Scholar] [CrossRef]
- Fute, M.; Mengesha, Z.B.; Wakgari, N.; Tessema, G.A. High prevalence of workplace violence among nurses working at public health facilities in Southern Ethiopia. BMC Nurs. 2015, 14, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Zegenhagen, S.; Ranganathan, M.; Buller, A.M. Household decision-making and its association with intimate partner violence: Examining differences in men’s and women’s perceptions in Uganda. SSM Popul. Health 2019, 8, 100442. [Google Scholar] [CrossRef] [PubMed]
- Feseha, G.; G’mariam, A.; Gerbaba, M. Intimate partner physical violence among women in Shimelba refugee camp, northern Ethiopia. BMC Public Health 2012, 12, 125. [Google Scholar] [CrossRef]
- Fidan, A.; Bui, H.N. Intimate Partner Violence against Women in Zimbabwe. Violence Against Women 2016, 22, 1075–1096. [Google Scholar] [CrossRef]
- Pack, A.P.; L’Engle, K.; Mwarogo, P.; Kingola, N. Intimate partner violence against female sex workers in Mombasa, Kenya. Cult. Health Sex. 2013, 16, 217–230. [Google Scholar] [CrossRef]
- Matseke, G.; Rodriguez, V.J.; Peltzer, K.; Jones, D. Intimate partner violence among HIV positive pregnant women in South Africa. J. Psychol. Afr. 2016, 26, 259–266. [Google Scholar] [CrossRef]
- Azene, Z.N.; Yeshita, H.Y.; Mekonnen, F.A. Intimate partner violence and associated factors among pregnant women attending antenatal care service in Debre Markos town health facilities, Northwest Ethiopia. PLoS ONE 2019, 14, e0218722. [Google Scholar] [CrossRef]
- Pengpid, S.; Peltzer, K. Intimate Partner Violence Victimization and Associated Factors among Male and Female Univer-sity Students in 22 Countries in Africa, Asia and the Americas. Afr. J. Reprod. Health 2016, 20, 29–39. [Google Scholar]
- Fawole, O.L.; Salawu, T.A.; Olarinmoye EO, A. Intimate partner violence: Prevalence and Pereceptions of married men in Ibadan, Nigeria. Int. Q. Community Health Educ. 2010, 30, 349–364. [Google Scholar] [CrossRef]
- Wandera, S.O.; Kwagala, B.; Ndugga, P.; Kabagenyi, A. Partners’ controlling behaviors and intimate partner sexual violence among married women in Uganda Global health. BMC Public Health 2015, 15, 1–9. [Google Scholar] [CrossRef]
- Hatcher, A.M.; Stockl, H.; McBride, R.S.; Khumalo, M.; Christofides, N. Pathways From Food Insecurity to Intimate Partner Violence Perpetration Among Peri-Urban Men in South Africa. Am. J. Prev. Med. 2019, 56, 765–772. [Google Scholar] [CrossRef]
- Lyons, C.; Diouf, D.; Drame, F.; Kouame, A.; Ezouatchi, R.; Bamba, A.; Thiam, M.; Liestman, B.; Ketende, S.; Baral, S. Physi-cal and sexual violence against female sex workers in Cote d’Ivoire: Prevalence, and the relationship between violence and structural determinants of HIV. J. Int. Aids Soc. 2016, 19, 17–18. [Google Scholar]
- Stöckl, H.; Watts, C.; Mbwambo, J.K.K. Physical violence by a partner during pregnancy in Tanzania: Prevalence and risk factors. Reprod. Health Matters 2010, 18, 171–180. [Google Scholar] [CrossRef]
- Mahenge, B.; Stöckl, H.; Abubakari, A.; Mbwambo, J.; Jahn, A. Physical, Sexual, Emotional and Economic Intimate Partner Violence and Controlling Behaviors during Pregnancy and Postpartum among Women in Dar es Salaam, Tanzania. PLoS ONE 2016, 11, e0164376. [Google Scholar] [CrossRef]
- Selin, A.; Delong, S.M.; Julien, A.; MacPhail, C.; Twine, R.; Hughes, J.P.; Agyei, Y.; Hamilton, E.L.; Kahn, K.; Pettifor, A. Prevalence and Associations, by Age Group, of IPV Among AGYW in Rural South Africa. Sage Open 2019, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Delamou, A.; Samandari, G.; Camara, B.S.; Traore, P.; Diallo, F.G.; Millimono, S.; Wane, D.; Toliver, M.; Laffe, K.; Verani, F. Prevalence and correlates of intimate partner violence among family planning clients in Conakry, Guinea. BMC Res. Notes 2015, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, M.; Mchome, B.; Ostermann, J.; Itemba, D.; Njau, B.; Thielman, N.; Kiwakkuki-Duke VCT Study Group. Prevalence and correlates of intimate partner violence among women attending HIV voluntary counseling and testing in northern Tanzania, 2005–2008. Int. J. Gynecol. Obs. 2011, 113, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, A.; Carpenter, B.; Crankshaw, T.; Hannass-Hancock, J.; Smit, J.; Tomlinson, M.; Butler, L. Prevalence and factors associated with recent intimate partner violence and relationships between disability and depression in post-partum women in one clinic in eThekwini Municipality, South Africa. PLoS ONE 2017, 12, e0181236. [Google Scholar] [CrossRef] [PubMed]
- Decker, M.R.; Peitzmeier, S.; Olumide, A.; Acharya, R.; Ojengbede, O.; Covarrubias, L.; Gao, E.; Cheng, Y.; Delany-Moretlwe, S.; Brahmbhatt, H. Prevalence and Health Impact of Intimate Partner Violence and Non-partner Sexual Violence Among Female Adolescents Aged 15–19 Years in Vulnerable Urban Environments: A Multi-Country Study. J. Adolesc. Health 2014, 55, S58–S67. [Google Scholar] [CrossRef] [PubMed]
- Malan, M.; Spedding, M.; Sorsdahl, K. The prevalence and predictors of intimate partner violence among pregnant women attending a midwife and obstetrics unit in the Western Cape. Glob. Ment. Health 2018, 5, e18. [Google Scholar] [CrossRef] [PubMed]
- Alangea, D.O.; Addo-Lartey, A.A.; Sikweyiya, Y.; Chirwa, E.D.; Coker-Appiah, D.; Jewkes, R.; Adanu, R.M.K. Prevalence and risk factors of intimate partner violence among women in four districts of the central region of Ghana: Baseline findings from a cluster randomised controlled trial. PLoS ONE 2018, 13, e0200874. [Google Scholar] [CrossRef]
- Reese, B.M.; Chen, M.S.; Nekkanti, M.; Mulawa, M.I. Prevalence and Risk Factors of Women’s Past-Year Physical IPV Perpetration and Victimization in Tanzania. J. Interpers. Violence 2021, 36, 1141–1167. [Google Scholar] [CrossRef]
- Memiah, P.; Mu, T.A.; Prevot, K.; Cook, C.K.; Mwangi, M.M.; Mwangi, E.W.; Owuor, K.; Biadgilign, S. The Prevalence of Intimate Partner Violence, Associated Risk Factors, and Other Moderating Effects: Findings From the Kenya National Health Demographic Survey. J. Interpers. Violence 2018. [Google Scholar] [CrossRef]
- Were, E.; Curran, K.; Delany-Moretlwe, S.; Nakku-Joloba, E.; Mugo, N.R.; Kiarie, J.; Bukusi, E.A.; Celum, C.; Baeten, J.M.; Prevention, H.H.P. A prospective study of frequency and correlates of intimate partner violence among African het-erosexual HIV serodiscordant couples. Aids 2011, 25, 2009–2018. [Google Scholar] [CrossRef] [PubMed]
- Falb, K.L.; Annan, J.; Kpebo, D.; Gupta, J. Reproductive coercion and intimate partner violence among rural women in Côte d’Ivoire: A cross-sectional study. Afr. J. Reprod. Health 2014, 18, 61–69. [Google Scholar]
- Breiding, M.J.; Reza, A.; Gulaid, J.; Blanton, C.; Mercy, J.; Dahlberg, L.L.; Dlamini, N.; Bamrah, S. Risk factors associated with sexual violence towards girls in Swaziland. Bull. World Health Organ. 2011, 89, 203–210. [Google Scholar] [CrossRef]
- Mutagoma, M.; Nyirazinyoye, L.; Sebuhoro, D.; Riedel, D.J.; Ntaganira, J. Sexual and physical violence and associated factors among female sex workers in Rwanda: A cross-sectional survey. Int. J. Std Aids 2018, 30, 241–248. [Google Scholar] [CrossRef]
- Bamiwuye, S.O.; Odimegwu, C. Spousal violence in sub-Saharan Africa: Does household poverty-wealth matter? Reprod. Health 2014, 11, 45. [Google Scholar] [CrossRef]
- Deyessa, N.; Berhane, Y.; Ellsberg, M.; Emmelin, M.; Kullgren, G.; Hogberg, U. Violence against women in relation to liter-acy and area of residence in Ethiopia. Glob. Health Action 2010, 3, 9. [Google Scholar] [CrossRef]
- Yenealem, D.G.; Woldegebriel, M.K.; Olana, A.T.; Mekonnen, T.H. Violence at work: Determinants & prevalence among health care workers, northwest Ethiopia: An institutional based cross sectional study. Ann. Occup. Environ. Med. 2019, 31, 8. [Google Scholar] [CrossRef] [PubMed]
- Ahinkorah, B.O.; Dickson, K.S.; Seidu, A.-A. Women decision-making capacity and intimate partner violence among women in sub-Saharan Africa. Arch. Public Health 2018, 76, 5. [Google Scholar] [CrossRef]
- Sisawo, E.J.; Ouédraogo, S.Y.Y.A.; Huang, S.-L. Workplace violence against nurses in the Gambia: Mixed methods design. Bmc Health Serv. Res. 2017, 17, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Newman, C.J.; de Vries, D.H.; Kanakuze, J.D.; Ngendahimana, G. Workplace violence and gender discrimination in Rwanda’s health workforce: Increasing safety and gender equality. Hum. Resour. Health 2011, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Hendrickson, Z.M.; Leddy, A.M.; Galai, N.; Mbwambo, J.K.; Likindikoki, S.; Kerrigan, D.L. Work-related mobility and ex-periences of gender-based violence among female sex workers in Iringa, Tanzania: A crosssectional analysis of baseline data from Project Shikamana. BMJ Open 2018, 8, e022621. [Google Scholar] [CrossRef]
- Deyessa, N.; Berhane, Y.; Alem, A.; Ellsberg, M.; Emmelin, M.; Hogberg, U.; Kullgren, G. Intimate partner violence and depression among women in rural Ethiopia: A cross-sectional study. Clin. Pr. Epidemiol. Ment. Health 2009, 5. [Google Scholar] [CrossRef]
- Gebrezgi, B.H.; Badi, M.B.; Cherkose, E.A.; Weldehaweria, N.B. Factors associated with intimate partner physical violence among women attending antenatal care in Shire Endaselassie town, Tigray, northern Ethiopia: A cross-sectional study, July 2015. Reprod. Health 2017, 14, 76. [Google Scholar] [CrossRef]
- Uthman, O.A.; Lawoko, S.; Moradi, T. Factors associated with attitudes towards intimate partner vio-lence against women: A comparative analysis of 17 sub-Saharan countries. BMC Int. J. Hum. Rights 2009, 9, 1–5. [Google Scholar]
- Muluneh, M.D.; Francis, L.; Agho, K.; Stulz, V. Mapping of Intimate Partner Violence: Evidence From a National Population Survey. 21. J. Interpers. Violence 2021. [Google Scholar] [CrossRef] [PubMed]
- Decker, M.R.; Latimore, A.D.; Yasutake, S.; Haviland, M.; Ahmed, S.; Blum, R.W. Gender-Based Violence Against Adolescent and Young Adult Women in Low- and Middle-Income Countries. J. Adolesc. Health 2015, 56, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Uthman, O.A.; Moradi, T.; Lawoko, S. Are Individual and Community Acceptance and Witnessing of Intimate Partner Violence Related to Its Occurrence? Multilevel Structural Equation Model. PLoS ONE 2011, 6, e27738. [Google Scholar] [CrossRef] [PubMed]
- Umeora, O.U.J.; Dimejesi, B.I.; Ejikeme, B.N.; Egwuatu, V.E. Pattern and determinants of domestic violence among pre-natal clinic attendees in a referral centre, South-east Nigeria. J. Obstet. Gynaecol. 2008, 28, 769–774. [Google Scholar] [CrossRef]
- Dessalegn, M.; Ayele, M.; Hailu, Y.; Addisu, G.; Abebe, S.; Solomon, H.; Mogess, G.; Stulz, V. Gender Inequality and the Sexual and Reproductive Health Status of Young and Older Women in the Afar Region of Ethiopia. Int. J. Environ. Res. Public Health 2020, 17, 4592. [Google Scholar] [CrossRef]
- Reichel, D. Determinants of Intimate Partner Violence in Europe: The Role of Socioeconomic Status, Inequality, and Partner Behavior. J. Interpers. Violence 2017, 32, 1853–1873. [Google Scholar] [CrossRef]
- Gibbs, A.; Dunkle, K.; Mhlongo, S.; Chirwa, E.; Hatcher, A.; Christofides, N.J.; Jewkes, R. Which men change in intimate partner violence prevention interventions? A trajectory analysis in Rwanda and South Africa. BMJ Glob. Health 2020, 5, e002199. [Google Scholar] [CrossRef]
- Marteau, T.M.; Hollands, G.J.; Fletcher, P.C. Changing Human Behavior to Prevent Disease: The Importance of Targeting Automatic Processes. Science 2012, 337, 1492–1495. [Google Scholar] [CrossRef]
- Finnoff, K. Intimate partner violence, female employment, and male backlash in Rwanda. Econ. Peace Secur. J. 2012, 7, 14. [Google Scholar] [CrossRef]
- Muluneh, M.D.; Alemu, Y.W.; Meazaw, M.W. Geographic variation and determinants of help seeking behaviour among married women subjected to intimate partner violence: Evidence from national population survey. Int. J. Equity Health 2021, 20, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.; Baron, E.; Davies, T.; Munodawafa, M.; Lund, C. Patterns of intimate partner violence among perinatal women with depression symptoms in Khayelitsha, South Africa: A longitudinal analysis. Glob. Ment. Health 2018, 5, e13. [Google Scholar] [CrossRef] [PubMed]
- World Bank. Violence against Women and Girls. Available online: https://www.worldbank.org/en/topic/socialdevelopment/brief/violence-against-women-and-girls (accessed on 29 July 2019).
- Ackerson, L.K.; Subramanian, S.V. Domestic Violence and Chronic Malnutrition among Women and Children in India. Am. J. Epidemiol. 2008, 167, 1188–1196. [Google Scholar] [CrossRef] [PubMed]
- Sustainable Development Goals—SDGs—The United Nations. Available online: https://sdgs.un.org/goals (accessed on 20 January 2020).








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).