
Multilevel Analysis of Urban–Rural Variations of Body Weights and Individual-Level Factors among Women of Childbearing Age in Nigeria and South Africa: A Cross-Sectional Survey



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.1.1. Nigeria
2.1.2. South Africa
2.2. Study Design
2.3. Variables Used in the Study
2.3.1. Outcome of Interest
2.3.2. Independent Variables
2.4. Measurement of Independent Variables
2.5. Statistical Analysis
2.6. Ethical Consideration
3. Results
3.1. Descriptive Results
Characteristics of Respondents
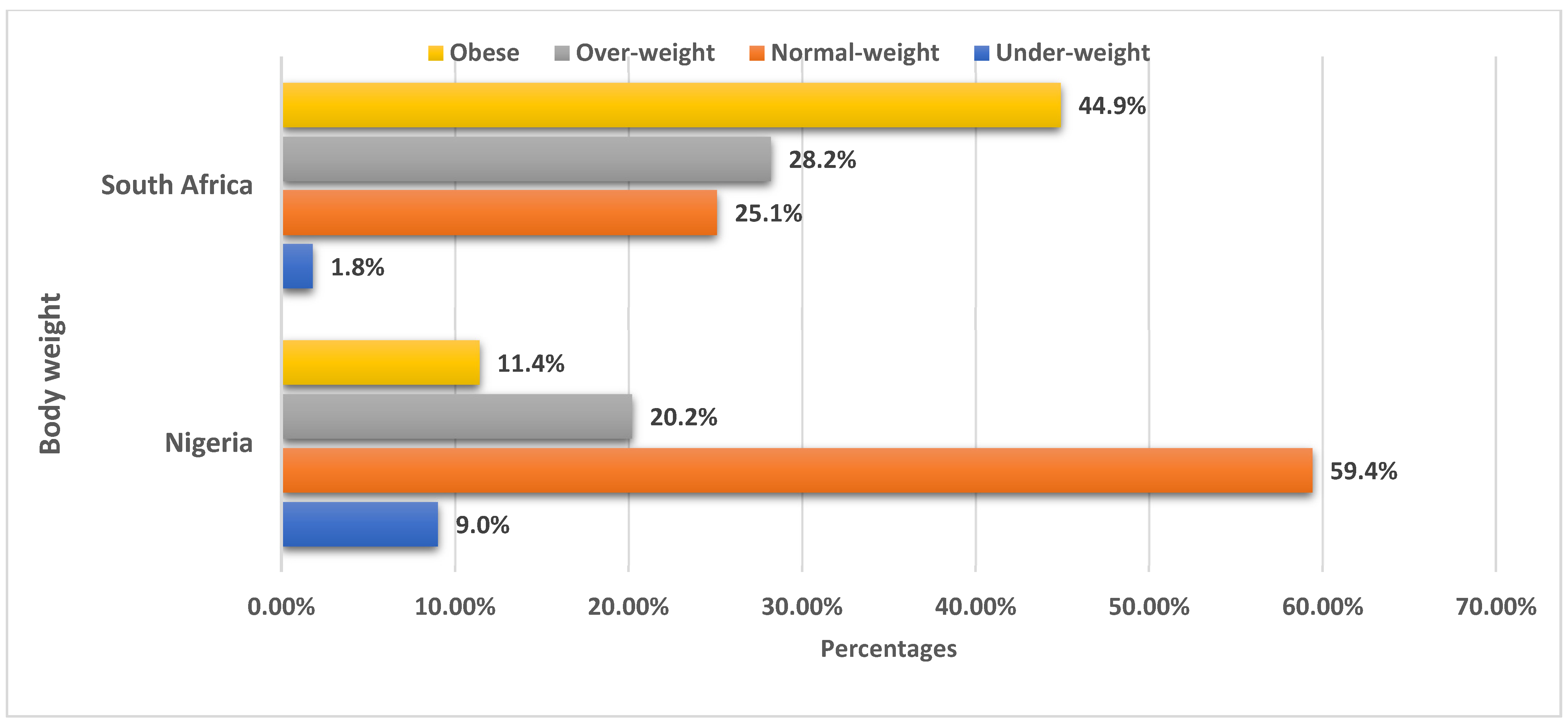
3.2. Overall Prevalence of Body Weight among Women of Childbearing Age by Country
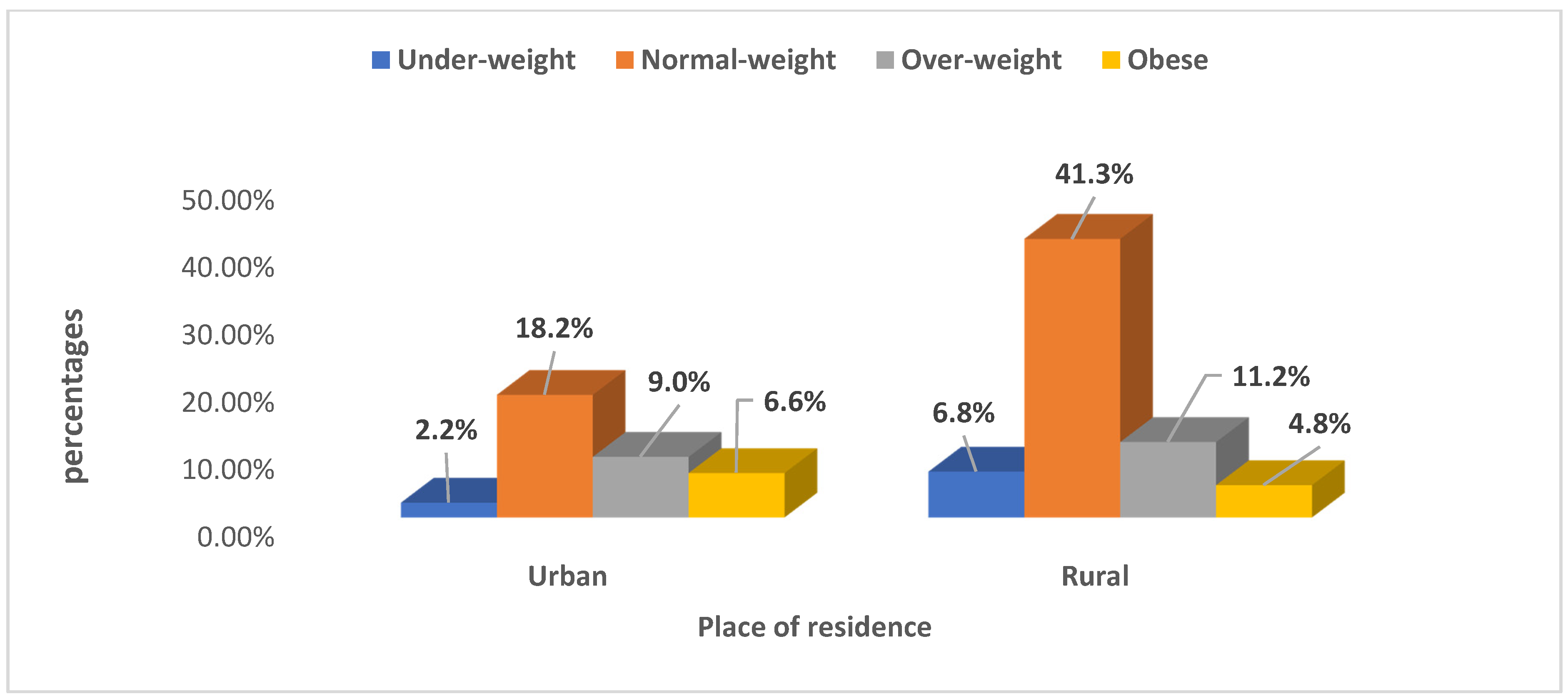
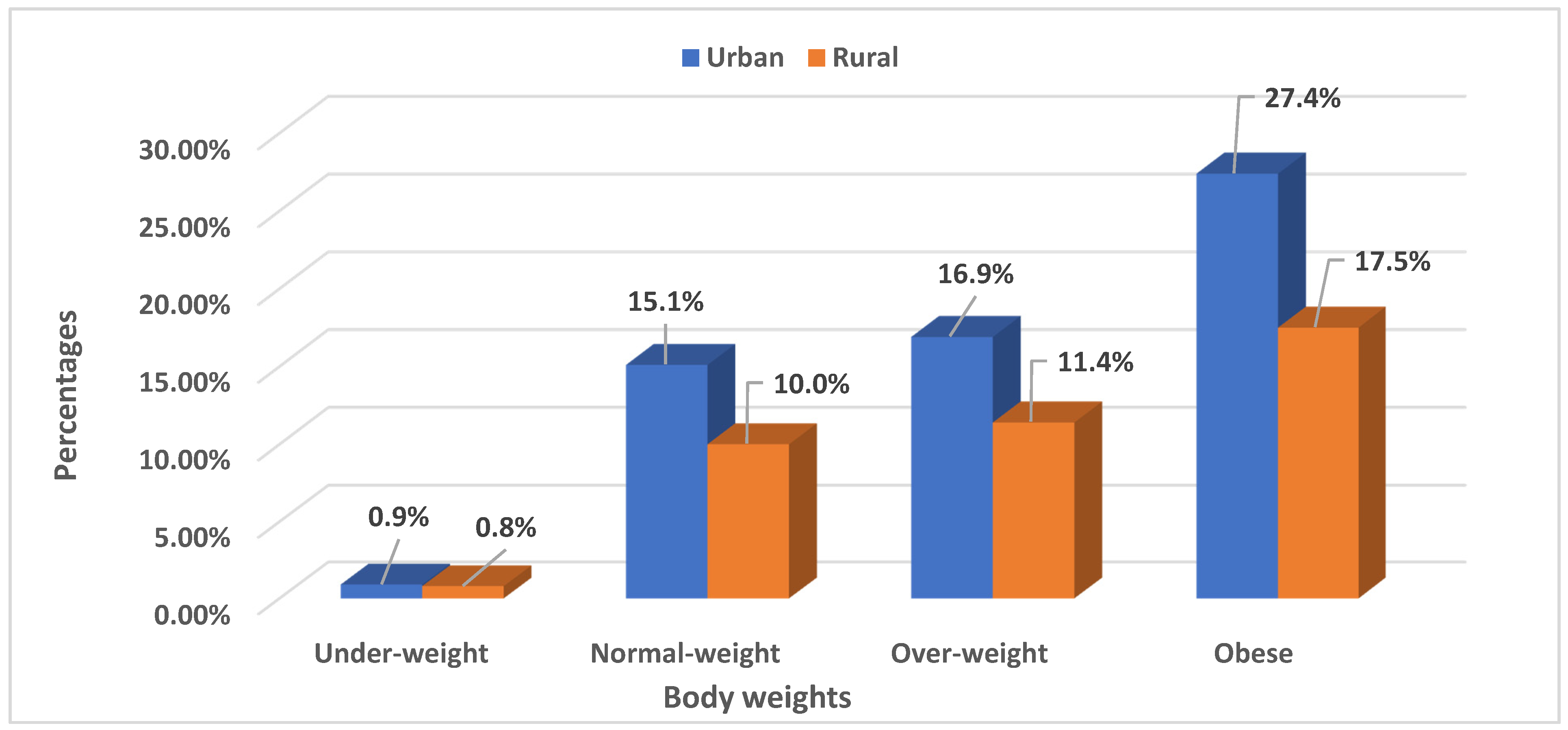
3.3. Prevalence of Body Weight among Women of Childbearing Age by Urban–Rural Variations in Nigeria and South Africa
3.4. Bivariate Analysis of Body Weight and Its Associated Factors
3.4.1. Bivariate Analysis of Women’s Body Weight and Associated Factors in Nigeria
3.4.2. Bivariate Analysis of Women’s Body Weight and Its Associated Factors in South Africa
3.5. Multivariate Analysis
4. Discussion
Strengths and Limitations
5. Conclusions
6. Contribution to the Field
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Adeboye, B.; Bermano, G.; Rolland, C. Obesity and its health impact in Africa: A systematic review. Cardiovasc. J. Afr. 2012, 23, 512–521. [Google Scholar] [CrossRef]
- Amugsi, D.A.; Dimbuene, Z.T.; Kyobutungi, C. Correlates of the double burden of malnutrition among women: An analysis of cross sectional survey data from sub-Saharan Africa. BMJ Open 2019, 9, e029545. [Google Scholar] [CrossRef] [Green Version]
- Monyeki, M.A.; Awotidebe, A.; Strydom, G.L.; De Ridder, J.H.; Mamabolo, R.L.; Kemper, H.C.G. The Challenges of Underweight and Overweight in South African Children: Are We Winning or Losing the Battle? A Systematic Review. Int. J. Environ. Res. Public Health 2015, 12, 1156–1173. [Google Scholar] [CrossRef] [Green Version]
- Sartorius, B.; Sartorius, K.; Green, R.; Lutge, E.; Scheelbeek, P.; Tanser, F.; Dangour, A.D.; Slotow, R. Spatial-temporal trends and risk factors for undernutrition and obesity among children (<5 years) in South Africa, 2008–2017: Findings from a nationally representative longitudinal panel survey. BMJ Open 2020, 10, e034476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pengpid, S.; Peltzer, K. Underweight and overweight/obesity among adults in Afghanistan: Prevalence and correlates from a national survey in 2018. J. Health Popul. Nutr. 2021, 40, 25. [Google Scholar] [CrossRef] [PubMed]
- Tekalegn, Y. Determinants of Overweight or Obesity among Men Aged 20–59 Years: A Case-Control Study Based on the 2016 Ethiopian Demographic and Health Survey. J. Obes. 2021, 2021, 6627328. [Google Scholar] [CrossRef] [PubMed]
- Menon, S.; Peñalvo, J.L. Actions Targeting the Double Burden of Malnutrition: A Scoping Review. Nutrients 2019, 12, 81. [Google Scholar] [CrossRef] [Green Version]
- Onyango, A.W.; Nikiema, L.; Kimokoti, R.W. Nutrition in health promotion policies and programs at the community level. In Handbook of Global Health; Haring, R., Kickbusch, I., Ganten, D., Moeti, M., Eds.; Springer: Singapore, 2021; pp. 1–36. [Google Scholar]
- Ogunlade, O.; Asafa, M. Pattern and prevalence of underweight, overweight and obesity among market women in South-West Nigeria. Niger. J. Health Sci. 2016, 16, 60. [Google Scholar] [CrossRef]
- Osunkwo, D.A.; Nguku, P.M.; Mohammed, A.; Umeokonkwo, C.D.; Kamateeka, M.; Ibrahim, M.; Kefas, I.B.; Abolade, O.S.; Nwokeukwu, H.I.; Zoakah, A.I. Prevalence of obesity and associated factors in Benue State, Nigeria: A population-based study. Ann. Afr. Med. 2021, 20, 9. [Google Scholar] [CrossRef]
- National Population Commission (NPC) [Nigeria] and ICF. Nigeria Demographic and Health Survey (NDHS), 2018; NPC and ICF: Abuja, Nigeria; Rockville, MD, USA, 2019; pp. 48–49. [Google Scholar]
- South Africa Demographic and Health Survey (SADHS). South Africa Demographic and Health Survey 2016: Key Indicators Report; National Department of Health (NDoH), Statistics South Africa (Stats SA), South African Medical Research Council (SAMRC) and ICF: Pretoria, South Africa; Rockvile, MD, USA, 2016.
- Adegoke, O.; Ozoh, O.B.; Odeniyi, I.A.; Bello, B.T.; Akinkugbe, A.O.; Ojo, O.O.; Agabi, O.P.; Okubadejo, N.U. Prevalence of obesity and an interrogation of the correlation between anthropometric indices and blood pressures in urban Lagos, Nigeria. Sci. Rep. 2021, 11, 3522. [Google Scholar] [CrossRef]
- Pisa, P.T.; Pisa, N.M.; Chikandiwa, P.; Chikandiwa, A. Economic growth as an underlying probable systemic driver for childhood obesity in South Africa: A Joint Point regression and ecological analysis over 10 years. S. Afr. Med. J. 2021, 112, 220–226. [Google Scholar] [CrossRef]
- Tydeman-Edwards, R.; Van Rooyen, F.C.; Walsh, C.M. Obesity, undernutrition and the double burden of malnutrition in the urban and rural southern Free State, South Africa. Heliyon 2018, 4, e00983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adegbenga, B.A.; Abiola, A.; Arinpade, I.; Jokotade, A.; Babatope, K.; Olufemi, F.; Augustine, O. Pattern of underweight and over-weight in Lagos Southwest Nigeria. J. Appl. Biotechnol. Bioeng. 2017, 4, 534–538. [Google Scholar] [CrossRef] [Green Version]
- Afolabi, R.F.; Palamuleni, M.E. Multilevel analysis of unhealthy bodyweight among women in Malawi: Does urbanisation matter? PLoS ONE 2021, 16, e0249289. [Google Scholar] [CrossRef]
- Ssentongo, P.; Ssentongo, A.E.; Ba, D.M.; Ericson, J.E.; Na, M.; Gao, X.; Fronterre, C.; Chinchilli, V.M.; Schiff, S.J. Global, regional and national epidemiology and prevalence of child stunting, wasting and underweight in low- and middle-income countries, 2006–2018. Sci. Rep. 2021, 11, 5204. [Google Scholar] [CrossRef]
- Monakali, S.; Ter Goon, D.; Seekoe, E.; Owolabi, E.O. Prevalence and factors associated with abdominal obesity among primary healthcare professional nurses in Eastern Cape. S. Afr. Fam. Pract. 2018, 60, 146–150. [Google Scholar] [CrossRef] [Green Version]
- Mahlangu, K.; Modjadji, P.; Madiba, S. The Nutritional Status of Adult Antiretroviral Therapy Recipients with a Recent HIV Diagnosis; a Cross-Sectional Study in Primary Health Facilities in Gauteng, South Africa. Healthcare 2020, 8, 290. [Google Scholar] [CrossRef]
- Adeloye, D.; Ige-Elegbede, J.O.; Ezejimofor, M.; Owolabi, E.O.; Ezeigwe, N.; Omoyele, C.; Mpazanje, R.G.; Dewan, M.T.; Agogo, E.; Gadanya, M.A.; et al. Estimating the prevalence of overweight and obesity in Nigeria in 2020: A systematic review and meta-analysis. Ann. Med. 2021, 53, 495–507. [Google Scholar] [CrossRef]
- Onyeji, G.N.; Sanusi, R.A. Prevalence of overweight and obesity among women of reproductive age in South-east Nigeria. Niger. J. Nutr. Sci. 2018, 39, 73–81. [Google Scholar]
- Gordon, T.; Booysen, F.; Mbonigaba, J. Socio-economic inequalities in the multiple dimensions of access to healthcare: The case of South Africa. BMC Public Health 2020, 20, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolnicar, S.; Grün, B.; Leisch, F. Increasing sample size compensates for data problems in segmentation studies. J. Bus. Res. 2016, 69, 992–999. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation; WHO Technical Report Series 894; WHO: Geneva, Switzerland, 2000; 252p. [Google Scholar]
- Ibrahim, H.; Tengku Alina Tengku, I.M.; Noran, H.M. Comparison of body weight among hormonal and non-hormonal users in a Malaysian cohort. J. Taibah Univ. Med. Sci. 2019, 14, 25–30. [Google Scholar] [CrossRef]
- Ciesla, E.; Stochmal, E.; Gluszek, S.; Suliga, E. Breastfeeding history and the risk of overweight and obesity in middle-aged women. BMC Women’s Health 2021, 21, 196. [Google Scholar]
- Senanayake, P.; O’Connor, E.; Ogbo, F.A. National and rural-urban prevalence and determinants of early initiation of breastfeeding in India. BMC Public Health 2019, 19, 896. [Google Scholar] [CrossRef] [Green Version]
- Ogbo, F.A.; Dhami, M.V.; Awosemo, A.O.; Olusanya, B.O.; Olusanya, J.; Osuagwu, U.L.; Ghimire, P.R.; Page, A.; Agho, K.E. Regional prevalence and determinants of exclusive breastfeeding in India. Int. Breastfeed. J. 2019, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, W.; Kuriki, K.; Shizuoka-Sakuragaoka J-MICC Study Group. Associations between family factors and body weight gain from 20 years old. BMC Women’s Health 2019, 19, 33. [Google Scholar] [CrossRef] [Green Version]
- Virtanen, M.; Jokela, M.; Lallukka, T.; Hanson, L.M.; Pentti, J.; Nyberg, S.T.; Alfredsson, L.; Batty, G.D.; Casini, A.; Clays, E.; et al. Long working hours and change in body weight: Analysis of individual-participant data from 19 cohort studies. Int. J. Obes. 2019, 44, 1368–1375. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q. Smoking and body weight: Evidence from China health and nutrition survey. BMC Public Health 2015, 15, 1238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Killip, S.; Mahfoud, Z.; Pearce, K. What Is an Intracluster Correlation Coefficient? Crucial Concepts for Primary Care Researchers. Ann. Fam. Med. 2004, 2, 204–208. [Google Scholar] [CrossRef]
- MacLeod, C.K.; Bailey, R.L.; Dejene, M.; Shafi, O.; Kebede, B.; Negussu, N.; Mpyet, C.; Olobio, N.; Alada, J.; Abdala, M.; et al. Estimating the Intracluster Correlation Coefficient for the Clinical Sign “Trachomatous Inflammation-Follicular” in Population-Based Trachoma Prevalence Surveys: Results From a Meta-Regression Analysis of 261 Standardized Preintervention Surveys Carried Out in Ethiopia, Mozambique, and Nigeria. Am. J. Epidemiol. 2019, 189, 68–76. [Google Scholar] [CrossRef]
- Snijders, T.A.B. Multilevel analysis. In International Encyclopedia of Statistical Science; Lovric, M., Ed.; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar] [CrossRef]
- Peer, N.; Lombard, C.; Steyn, K.; Gwebushe, N.; Levitt, N. Differing Patterns of Overweight and Obesity among Black Men and Women in Cape Town: The CRIBSA Study. PLoS ONE 2014, 9, e107471. [Google Scholar] [CrossRef]
- Cois, A.; Day, C. Obesity trends and risk factors in the South African adult population. BMC Obes. 2015, 2, 42. [Google Scholar] [CrossRef] [Green Version]
- Njoku, P.U.; Dienye, P.O.; Olaniyan, F.A.; Iloh, G.U.P.; Njoku, R.A.N. Obesity among women of reproductive age using contraceptive methods in Port Harcourt, Nigeria. World J. Adv. Res. Rev. 2020, 06, 159–165. [Google Scholar] [CrossRef]
- Yaya, S.; Glose, B. Trend in overweight and obesity among women of reproductive age in Uganda: 1995–2016. Obes. Sci. Pract. 2019, 5, 312–323. [Google Scholar] [CrossRef] [Green Version]
- Kassie, A.M.; Abate, B.B.; Kassaw, M.W. Education and prevalence of overweight and obesity among reproductive age group women in Ethiopia: Analysis of the 2016 Ethiopian demographic and health survey data. BMC Public Health 2020, 20, 1189. [Google Scholar] [CrossRef]
- Morakinyo, O.M.; Adebowale, A.S.; Obembe, T.A.; Oloruntoba, E.O. Association between household environmental conditions and nutritional status of women of childbearing age in Nigeria. PLoS ONE 2020, 15, e0243356. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, S.F.; Haregu, T.N.; Khayeka-Wandabwa, C.; Muthuri, S.K.; Kyobutungi, C. Magnitude and predictors of normal-weight central obesity– the AWI-Gen study findings. Glob. Health Action 2019, 12, 1685809. [Google Scholar] [CrossRef] [Green Version]
- Pengpid, S.; Peltzer, K. The prevalence and associated factors of underweight and overweight/obesity among adults in Kenya: Evidence from a national cross-sectional community survey. Pan Afr. Med. J. 2020, 36, 338. [Google Scholar] [CrossRef] [PubMed]
- Mchiza, Z.J.-R.; Parker, W.-A.; Hossin, M.Z.; Heshmati, A.; Labadarios, D.; Falkstedt, D.; Koupil, I. Social and Psychological Predictors of Body Mass Index among South Africans 15 Years and Older: SANHANES-1. Int. J. Environ. Res. Public Health 2019, 16, 3919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajayi, I.O.; Adebamowo, C.; Adami, H.-O.; Dalal, S.; Diamond, M.B.; Bajunirwe, F.; Guwatudde, D.; Njele Kela, M.; Nankya-Mutyoba, J.; Chiwanga, F.S.; et al. Ur-ban-rural and geographic differences in overweight and obesity in four sub-Saharan African adult populations: A multi-country cross-sectional study. BMC Public Health 2016, 16, 1126. [Google Scholar] [CrossRef] [Green Version]
- Kayode, O.O.; Alabi, Q.K. Food consumption patterns, physical activity and overweight and obesity among undergraduates of a private university in Nigeria. Clin. Nutr. Exp. 2020, 31, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Ikechukwu, E.C.; Gloria, M.U.; Ikenna, U.C.; Chinonso, U.V.; Mmanwanne, U.E.; Chinedu, O.O.; Chukwudi, A.C.; Nene, J.J.; Chinwe, O.; Nkechi, A.C. Physical Activity Level and Factors Affecting Exercise Participation among Nigerian Adults with and Without Diabetes. Eur. Med. J. 2021, 6, 1–10. [Google Scholar] [CrossRef]
- Rai, A.; Gurung, S.; Thapa, S.; Saville, N.M. Correlates and inequality of underweight and overweight among women of repro-ductive age: Evidence from the 2016 Nepal Demographic Health Survey. PLoS ONE 2019, 14, e0216644. [Google Scholar] [CrossRef] [PubMed]
- Al Kibria, G.M.; Swasey, K.; Hasan, M.Z.; Sharmeen, A.; Day, B. Prevalence and factors associated with underweight, overweight and obesity among women of reproductive age in India. Glob. Health Res. Policy 2019, 4, 24. [Google Scholar] [CrossRef] [Green Version]
- Schwinger, C.; Chandyo, R.K.; Ulak, M.; Hysing, M.; Shrestha, M.; Ranjitkar, S.; Strand, T.A. Prevalence of Underweight, Overweight, and Obesity in Adults in Bhaktapur, Nepal in 2015–2017. Front. Nutr. 2020, 7, 567164. [Google Scholar] [CrossRef]
- Onah, M.N. Women’s empowerment and child nutrition in South-Central Asia; how important is socioeconomic status? SSM Popul. Health 2021, 13, 100718. [Google Scholar] [CrossRef]
- Bishwajit, G. Household wealth status and overweight and obesity among adult women in Bangladesh and Ban. Obes. Sci. Pract. 2017, 3, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Biswas, T.; Garnett, S.P.; Pervin, S.; Rawal, L.B. The prevalence of underweight, overweight and obesity in Bangladeshi adults: Data from a national survey. PLoS ONE 2017, 12, e0177395. [Google Scholar] [CrossRef]
- Jaacks, L.; Slining, M.M.; Popkin, B.M. Recent Underweight and Overweight Trends by Rural–Urban Residence among Women in Low- and Middle-Income Countries. J. Nutr. 2014, 145, 352–357. [Google Scholar] [CrossRef] [Green Version]
- Hashan, M.R.; Rabbi, F.; Haider, S.S.; Das Gupta, R. Prevalence and associated factors of underweight, overweight and obesity among women of reproductive age group in the Maldives: Evidence from a nationally representative study. PLoS ONE 2020, 15, e0241621. [Google Scholar] [CrossRef]
- Ahmed, K.Y.; Rwabilimbo, A.G.; Abrha, S.; Page, A.; Arora, A.; Tadese, F.; Beyene, T.Y.; Seiko, A.; Endris, A.A.; Agho, K.E.; et al. On behalf of the Global Maternal and Child Health Research Collaboration (GloMACH). Factors associated with underweight, overweight, and obesity in reproductive age Tanzanian women. PLoS ONE 2020, 15, e0237720. [Google Scholar] [CrossRef] [PubMed]
- Masood, M.; Reidpath, D.D. Intraclass correlation and design effect in BMI, physical activity and diet: A cross-sectional study of 56 countries. BMJ Open 2016, 6, e008173. [Google Scholar] [CrossRef] [Green Version]
- Agyapong, N.A.F.; Annan, R.A.; Apprey, C.; Aduku, L.N.E. Body Weight, Obesity Perception, and Actions to Achieve Desired Weight among Rural and Urban Ghanaian Adults. J. Obes. 2020, 2020, 7103251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagos, A.; Tsadik, M.; Belachew, A.B.; Tesfahunegn, A. Individual and community-level factors influencing optimal breastfeeding: A multilevel analysis from a national survey study of Ethiopia. PLoS ONE 2021, 16, e0241428. [Google Scholar] [CrossRef]
- Doku, D.T.; Neupane, S. Double burden of malnutrition: Increasing overweight and obesity and stall under-weight trends among Ghanaian women. BMC Public Health 2015, 15, 670. [Google Scholar] [CrossRef] [Green Version]
- Sossi, F. Prevalence and determinants of undernutrition in women in Nepal. Acta Sci. Nutr. Health 2019, 3, 184–203. [Google Scholar]
- Akokuwebe, M.E.; Idemudia, E.S. Prevalence and Socio-Demographic Correlates of Body Weight Categories among South African Women of Reproductive Age: A Cross-Sectional Study. Front. Public Health 2021, 9, 715956. [Google Scholar] [CrossRef]
- Ratib, M.; Nabasirye, C.K.; Mulira, J.; Nakidde, C.; Kalyango, F.; Dolorence, M.A.W.; Schumacher, T.; Lawoko, S.; Sharma, K.N. Socio-economic status and exclusive breastfeeding among infants in a Ugandan cross-sectional study. J. Food Nutr. Sci. 2019, 7, 16–24. [Google Scholar] [CrossRef]
- Bishay, R.H.; Kormas, N. Self-empowerment and health outcomes in obese adults with type 2 diabetes following completion of a multi-disciplinary metabolic rehabilitation program. Endocrinol. Metab. Int. J. 2017, 5, 197–203. [Google Scholar] [CrossRef] [Green Version]
- Mokwena, K. Strategies to increase the health literacy needed to complement health-promoting legislation in South Africa. S. Afr. J. Clin. Nutr. 2015, 28, 197. [Google Scholar] [CrossRef]
- Fisher, H.; Erasmus, A.C.; Viljoen, A. Developing a food literacy definition for South Africa. Afr. J. Hosp. Tour. Leis. 2019, 8, 1–22. Available online: https://www.ajhtl.com (accessed on 18 May 2021).
- Abrha, S.; Shiferaw, S.; Ahmed, K.Y. Overweight and obesity and its socio-demographic correlates among urban Ethiopian women: Evidence from the 2011 EDHS. BMC Public Health 2016, 16, 636. [Google Scholar] [CrossRef] [Green Version]
- Akokuwebe, M.E.; Odimegwu, C. Socioeconomic Determinants of Knowledge of Kidney Disease among Residents in Nigerian Communities in Lagos State, Nigeria. Oman Med. J. 2019, 34, 444–455. [Google Scholar] [CrossRef] [PubMed]
- Struzzo, P.; Fumato, R.; Tillati, S.; Cacitti, A.; Gangi, F.; Stefani, A.; Torcutti, A.; Crapesi, L.; Tubaro, G.; Balestrieri, M. Individuals empowerment in overweight and obese patients: A study protocol. BMJ Open 2013, 3, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tehranian, A.; Hosseini, L.; Nariman, S.; Eslami, B.; Rastad, H.; Aghajani, F. The association between pregnancy body mass index and breastfeeding duration in Iranian women. J. Compr. Pediatrics 2017, 8, e12361. [Google Scholar] [CrossRef] [Green Version]
- Akokuwebe, M.E. “Healthy women, healthy world”: A theoretical discourse of general health status of women in Nigeria. West Afr. J. Archaeol. (Revue Quest Afr. Archeol.) 2016, 46, 87–111. [Google Scholar]
- Akokuwebe, M.E.; Amusan, L.; Odularu, G. Women development in agriculture as agency for fostering innovative agricultural financing in Nigeria. Afr. J. Food Agric. Nutr. Dev. 2021, 21, 18279–18299. [Google Scholar] [CrossRef]
- Akokuwebe, M.E.; Odimegwu, C.; Omololu, F. Prevalence, risk-inducing lifestyle, and perceived susceptibility to kidney diseases by gender among Nigerians residents in South Western Nigeria. Afr. Health Sci. 2020, 20, 860–870. [Google Scholar] [CrossRef]
- Akokuwebe, M.E.; Okunola, R.A.; Falayi, S.E. Youths and risky sexual behaviour: A KAP study on HIV/AIDS amongst University of Ibadan student. Eur. J. Soc. Sci. 2015, 49, 140–152. [Google Scholar]
- Odularu, G.; Aluko, O.A.; Odularu, A.; Akokuwebe, M.; Adedugbe, A. Conclusion: Fostering nutrition security, climate adaptation and sustainable agriculture strategies amid COVID-19 pandemic. In Nutrition, Sustainable Agriculture and Climate Change in Africa; Springer: Singapore, 2020; pp. 175–182. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| S/No | Variable Name | Categorization |
|---|---|---|
| 1 | Age | 15–19 = 1; 20–24 = 2; 25–29 = 3; 30–34 = 4; 35–39 = 5; 40–44 = 6; 45–49 = 7 |
| 2 | Place of residence | urban = 1; rural = 2 |
| 3 | Woman education | no education = 1; primary = 2; secondary = 3; higher education = 4 |
| 4 | Employment status | unemployed = 1; self-employed = 2; employed = 3 |
| 5 | Wealth index | poorest = 1; poorer = 2; average = 3; richer = 4; richest = 5 |
| 6 | Marital status | single = 1; married = 2; cohabiting = 3; widowed = 4; divorced/separated = 5 |
| 7 | Geopolitical zone | North central = 1, North east = 2, North west = 3, South east = 4, South west = 5, South south = 6 |
| 8 | Province | Western Cape = 1; Eastern Cape = 2; Northern Cape = 3; Free State = 4; KwaZulu-Natal = 5; North West = 6; Gauteng = 7; Mpumalanga = 8; Limpopo = 9. |
| 9 | Height | below average = 1; above average = 2 |
| 10 | Weight | below average = 1 and above average = 2 |
| 11 | Children ever born | 1–3 = 1; 4–6 = 2; 7+ = 3 |
| 12 | Contraceptive method | none = 1; folkloric = 2; traditional = 3; modern = 4 |
| 13 | Breastfeeding | no = 1; yes = 2 |
| 14 | Living with partners | no = 1; yes = 2 |
| 15 | Long working hours | no = 1; yes = 2 |
| 16 | Cigarette smoking | no = 1; yes = 2 |
| Characteristics | Nigeria | South Africa | ||
|---|---|---|---|---|
| Frequency (n) | Percentage (%) | Frequency (n) | Percentage (%) | |
| Age group | ||||
| 15–19 | 1489 | 1.2 | 194 | 1.4 |
| 20–24 | 8568 | 6.8 | 1123 | 7.9 |
| 25–29 | 19,202 | 15.2 | 2188 | 15.5 |
| 30–34 | 24,026 | 19.0 | 2687 | 19.0 |
| 35–39 | 26,641 | 21.1 | 2646 | 18.7 |
| 40–44 | 23,080 | 18.2 | 2628 | 18.6 |
| 45–49 | 23,532 | 18.6 | 2675 | 18.9 |
| Residence | ||||
| Urban | 48,493 | 38.3 | 9010 | 63.7 |
| Rural | 78,045 | 61.7 | 5134 | 36.3 |
| Education | ||||
| No education | 65,030 | 51.4 | 512 | 3.6 |
| Primary | 23,683 | 18.7 | 1999 | 14.1 |
| Secondary | 29,876 | 23.6 | 10,219 | 72.3 |
| Tertiary | 7948 | 6.3 | 1413 | 10.0 |
| Employment status | ||||
| Unemployed | 228 | 0.2 | 10,656 | 75.3 |
| Self-employed | 91,157 | 92.7 | 1596 | 11.3 |
| Employed | 7000 | 7.1 | 1892 | 13.4 |
| Wealth index | ||||
| Poorest | 19,586 | 23.4 | 3109 | 22.0 |
| Poorer | 29,135 | 23.0 | 3107 | 22.0 |
| Average | 25,754 | 20.4 | 3155 | 22.3 |
| Richer | 23,326 | 18.4 | 2643 | 18.7 |
| Richest | 18,736 | 14.8 | 2129 | 15.1 |
| Marital status | ||||
| Single | 1437 | 1.14 | 5587 | 39.5 |
| Married | 113,851 | 90.0 | 4971 | 35.1 |
| Cohabiting | 2861 | 2.26 | 2311 | 16.3 |
| Widowed | 5215 | 4.12 | 556 | 3.9 |
| Divorced/separated | 3173 | 2.51 | 718 | 5.1 |
| Geopolitical zone | ||||
| North central | 16,460 | 13.0 | - | - |
| Northeast | 22,686 | 17.9 | - | - |
| Northwest | 47,751 | 37.7 | - | - |
| Southeast | 12275 | 9.7 | - | - |
| Southwest | 11,228 | 8.9 | - | - |
| South south | 16,138 | 12.8 | - | - |
| Provinces | ||||
| Western Cape | - | - | 1547 | 10.9 |
| Eastern Cape | - | - | 1648 | 11.7 |
| Northern Cape | - | - | 289 | 2.0 |
| Free State | - | - | 681 | 4.8 |
| KwaZulu–Natal | - | - | 2553 | 18.1 |
| Northwest | - | - | 1057 | 7.5 |
| Gauteng | - | - | 3673 | 26.0 |
| Mpumalanga | - | - | 1235 | 8.7 |
| Limpopo | - | - | 1459 | 10.3 |
| Height | ||||
| Below average | 19,664 | 48.3 | 2334 | 45.1 |
| Above average | 21,016 | 51.7 | 2843 | 54.9 |
| Weight | ||||
| Below average | 27,592 | 59.3 | 3019 | 52.2 |
| Above average | 18,979 | 40.8 | 2763 | 47.8 |
| Children borne | ||||
| 1–3 | 27,958 | 22.1 | 9746 | 68.9 |
| 4–6 | 48,973 | 38.7 | 3832 | 27.1 |
| 7+ | 49,606 | 39.2 | 566 | 4.0 |
| Contraceptive method | ||||
| None | 105,955 | 83.7 | 6186 | 43.7 |
| Folkloric | 900 | 0.7 | 0 | 0.0 |
| Traditional | 4430 | 3.5 | 35 | 0.3 |
| Modern | 15,253 | 12.1 | 7923 | 56.0 |
| Breastfeeding | ||||
| No | 85,963 | 67.9 | 12,516 | 88.5 |
| Yes | 40,575 | 32.1 | 1628 | 11.5 |
| Living with partner | ||||
| No | 8083 | 6.9 | 1229 | 17.7 |
| Yes | 108,630 | 93.1 | 5735 | 82.4 |
| Long working hours | ||||
| No | 32,692 | 25.8 | 8376 | 59.2 |
| Yes | 93,846 | 74.2 | 5770 | 40.8 |
| Cigarette smoking | ||||
| No | 126,272 | 99.8 | 6702 | 94.8 |
| Yes | 266 | 0.2 | 371 | 5.3 |
| Total | 126,538 | 100.0 | 14,144 | 100.0 |
| Factors | Underweight | Overweight | Obese | |||
|---|---|---|---|---|---|---|
| AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | |
| Age group | ||||||
| 15–19 | 1.00 | 1.00 | 1.00 | |||
| 20–24 | 0.92 | 0.75–1.13 | 1.80 | 0.72–4.46 | 13.56 *** | 8.91–20.63 |
| 25–29 | 0.75 *** | 0.70–0.79 | 3.13 * | 1.21–8.11 | 31.66 *** | 14.57–68.78 |
| 30–34 | 0.86 * | 0.76–0.96 | 3.92 ** | 1.81–8.48 | 48.99 *** | 36.30–66.10 |
| 35–39 | 0.74 *** | 0.64–0.83 | 5.02 *** | 2.06–12.19 | 67.22 *** | 33.65–134.24 |
| 40–44 | 0.61 *** | 0.55–0.68 | 4.20 ** | 1.70–10.32 | 71.98 *** | 35.75–144.91 |
| 45–49 | 0.69 *** | 0.62–0.77 | 4.99 ** | 1.74–14.25 | 98.01 *** | 41.65–230.62 |
| Education | ||||||
| No education | 1.00 | 1.00 | 1.00 | |||
| Primary | 0.49 *** | 0.36–0.66 | 1.98 *** | 1.79–2.16 | 2.76 *** | 1.96–3.91 |
| Secondary | 0.45 *** | 0.35–0.58 | 2.36 *** | 1.87–2.96 | 3.91 *** | 2.10–7.27 |
| Tertiary | 0.34 ** | 0.17–0.65 | 3.43 *** | 2.69–4.35 | 7.30 *** | 4.99–10.66 |
| Employment status | ||||||
| Unemployed | 1.00 | 1.00 | 1.00 | |||
| Self-employed | 1.49 *** | 1.20–1.84 | 1.46 | 0.25–8.35 | 4.70 ** | 1.76–12.56 |
| Employed | 0.97 | 0.48–1.99 | 2.19 | 0.32–14.88 | 9.02 *** | 3.09–26.33 |
| Wealth index | ||||||
| Poorest | 1.00 | 1.00 | 1.00 | |||
| Poorer | 0.71 * | 0.51–0.97 | 1.78 *** | 1.75–1.82 | 3.39 *** | 2.09–5.48 |
| Average | 0.49 *** | 0.41–0.57 | 2.51 *** | 2.18–2.88 | 5.32 *** | 4.12–6.89 |
| Richer | 0.43 *** | 0.38–0.47 | 4.24 *** | 4.14–4.34 | 12.49 *** | 9.92–15.73 |
| Richest | 0.34 *** | 0.27–0.42 | 6.49 *** | 6.18–6.82 | 29.12 *** | 23.24–36.48 |
| Marital status | ||||||
| Single | 1.00 | 1.00 | 1.00 | |||
| Married | 1.01 | 0.40–2.52 | 1.02 | 0.60–1.73 | 1.18 *** | 1.08–1.28 |
| Cohabiting | 0.58 *** | 0.52–0.65 | 0.94 | 0.45–1.98 | 1.23 | 0.73–2.07 |
| Widowed | 0.61 * | 0.38–0.96 | 0.89 * | 0.81–0.98 | 1.58 *** | 1.23–2.02 |
| Divorced/separated | 1.16 | 0.57–2.33 | 1.40 ** | 1.14–1.71 | 1.53 | 0.65–3.59 |
| Geopolitical zone | ||||||
| North central | 1.00 | 1.00 | 1.00 | |||
| Northeast | 2.91 *** | 2.34–3.61 | 0.64 ** | 0.47–0.86 | 0.63 * | 0.42–0.92 |
| Northwest | 1.48 *** | 1.22–1.77 | 0.62 *** | 0.52–0.74 | 0.40 | 0.16–1.00 |
| Southeast | 0.75 | 0.34–1.59 | 1.36 | 0.94–1.98 | 1.55 * | 1.03–2.32 |
| South south | 0.69 | 0.41–1.15 | 1.99 *** | 1.52–2.61 | 2.45 *** | 2.13–2.80 |
| Southwest | 0.99 | 0.45–2.17 | 1.37 *** | 1.15–1.61 | 1.40 *** | 1.32–1.48 |
| Height | ||||||
| Below average | 1.00 | 1.00 | 1.00 | |||
| Above average | 1.11 | 0.92–1.33 | 1.07 | 0.98–1.16 | 1.32 ** | 1.12–1.54 |
| Weight | ||||||
| Below average | 1.00 | 1.00 | ||||
| Above average | 50.53 *** | 33.87–75.35 | 1783.32 *** | 530.8–5991.1 | ||
| Children borne | ||||||
| 1–3 | 1.00 | 1.00 | 1.00 | |||
| 4–6 | 0.89 *** | 0.86–0.92 | 1.22 *** | 1.14–1.29 | 1.50 *** | 1.39–1.61 |
| 7+ | 1.04 | 0.89–1.23 | 0.98 | 0.76–1.26 | 0.98 | 0.91–1.08 |
| Contraceptive method | ||||||
| None | 1.00 | 1.00 | 1.00 | |||
| Folkloric | 1.05 | 0.65–1.66 | 1.33 | 0.91–1.93 | 0.63 | 0.14–2.79 |
| Traditional | 0.64 ** | 0.49–0.84 | 2.62 *** | 1.92–3.58 | 3.36 *** | 2.81–4.01 |
| Modern | 0.66 *** | 0.58–0.74 | 2.03 *** | 1.89–2.17 | 2.04 *** | 1.86–2.23 |
| Breastfeeding | ||||||
| No | 1.00 | 1.00 | 1.00 | |||
| Yes | 1.26 *** | 1.16–1.37 | 0.71 *** | 0.710–0.714 | 0.45 *** | 0.37–0.55 |
| Living with partner | ||||||
| No | 1.00 | 1.00 | 1.00 | |||
| Yes | 1.55 | 0.93–2.56 | 0.77 | 0.57–1.05 | 0.80 | 0.54–1.17 |
| Long working hours | ||||||
| No | 1.00 | 1.00 | 1.00 | |||
| Yes | 0.87 *** | 0.81–0.93 | 1.50 | 1.07–2.08 | 1.87 | 0.90–3.88 |
| Cigarette smoking | ||||||
| No | - | 1.00 | 1.00 | |||
| Yes | - | - | 0.76 | 0.09–6.59 | 4.52 *** | 3.43–5.93 |
| Factors | Underweight | Overweight | Obese | |||
|---|---|---|---|---|---|---|
| AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | |
| Age group | ||||||
| 15–19 | 1.00 | 1.00 | 1.00 | |||
| 20–24 | 3.73 | 0.58–23.85 | 3.44 *** | 1.89–6.24 | 2.74 ** | 1.44–5.21 |
| 25–29 | 3.95 | 0.63–24.41 | 4.01 *** | 2.24–7.15 | 4.60 *** | 2.48–8.53 |
| 30–34 | 3.27 | 0.52–20.51 | 4.77 *** | 2.67–8.52 | 7.89 *** | 4.26–14.59 |
| 35–39 | 7.22 * | 1.18–44.01 | 4.34 *** | 2.41–7.79 | 12.31 *** | 6.65–22.76 |
| 40–44 | 1.55 | 0.22–10.72 | 5.68 *** | 3.17–10.17 | 11.51 *** | 6.21–21.30 |
| 45–49 | 1.59 | 0.22–11.28 | 6.30 *** | 3.50–11.33 | 16.04 *** | 8.65–29.77 |
| Education | ||||||
| No education | 1.00 | 1.00 | 1.00 | |||
| Primary | 1.67 | 0.07–36.65 | 1.57 * | 1.05–2.34 | 0.99 | 0.71–1.37 |
| Secondary | 1.41 | 0.25–7.65 | 1.81 ** | 1.25–2.59 | 1.21 | 0.90–1.63 |
| Tertiary | 0.11 *** | 0.04–0.29 | 2.14 *** | 1.37–3.35 | 1.56 * | 1.07–2.28 |
| Employment status | ||||||
| Unemployed | 1.00 | 1.00 | 1.00 | |||
| Self-employed | 0.83 | 0.28–2.43 | 1.47 ** | 1.16–1.85 | 1.06 | 0.84–1.33 |
| Employed | 0.35 | 0.02–5.62 | 1.95 *** | 1.47–2.56 | 2.59 *** | 2.02–3.34 |
| Wealth index | ||||||
| Poorest | 1.00 | 1.00 | 1.00 | |||
| Poorer | 2.36 *** | 1.56–3.56 | 0.98 | 0.80–1.20 | 1.21 * | 1.00–1.46 |
| Average | 2.07 | 0.44–9.66 | 1.13 | 0.92–1.39 | 1.64 *** | 1.34–1.99 |
| Richer | 1.35 | 0.53–3.43 | 1.14 | 0.92–1.43 | 1.68 *** | 1.34–2.10 |
| Richest | 1.33 | 1.02–1.74 | 2.48 *** | 1.91–3.21 | ||
| Marital status | ||||||
| Single | 1.00 | 1.00 | 1.00 | |||
| Married | 0.47 * | 0.25–0.87 | 1.78 | 1.48–2.12 | 2.52 *** | 2.14–2.96 |
| Cohabiting | 0.60 | 0.33–1.09 | 1.20 | 0.98–1.46 | 1.04 | 0.86–1.26 |
| Widowed | 2.49 | 0.93–6.60 | 2.33 | 1.42–3.82 | 4.63 *** | 2.98–7.18 |
| Divorced/separated | 0.36 | 0.06–1.95 | 2.58 | 1.79–3.71 | 2.34 *** | 1.64–3.31 |
| Provinces | ||||||
| Western Cape | 1.00 | 1.00 | 1.00 | |||
| Eastern Cape | 0.61 | 0.26–1.43 | 1.08 | 0.77–1.51 | 0.78 | 0.58–1.06 |
| Northern Cape | 1.08 | 0.34–3.38 | 0.78 | 0.46–1.3 | 0.46 ** | 0.28–0.77 |
| Free State | 0.72 | 0.24–2.18 | 1.17 | 0.77–1.79 | 0.94 | 0.64–1.38 |
| KwaZulu-Natal | 0.27 ** | 0.10–0.69 | 0.87 | 0.63–1.20 | 0.83 | 0.62–1.10 |
| Northwest | 0.72 | 0.29–1.78 | 0.87 | 0.60–1.25 | 0.76 | 0.55–1.06 |
| Gauteng | 0.40 * | 0.18–0.90 | 0.95 | 0.69–1.28 | 0.73 * | 0.55–0.95 |
| Mpumalanga | 0.51 | 0.19–1.34 | 1.06 | 0.74–1.51 | 0.74 | 0.53–1.02 |
| Limpopo | 1.33 | 0.62–2.85 | 0.92 | 0.65–1.29 | 0.77 | 0.56–1.05 |
| Height | ||||||
| Below average | 1.00 | 1.00 | 1.00 | |||
| Above average | 1.63 * | 1.05–2.52 | 1.15 | 0.99–1.35 | 1.05 | 0.91–1.20 |
| Weight | ||||||
| Below average | 1.00 | 1.00 | 1.00 | |||
| Above average | - | - | 329.67 | 60.95–1783.1 | 11,773.93 *** | 2168.7–63,919.9 |
| Children borne | ||||||
| 1–3 | 1.00 | 1.00 | 1.00 | |||
| 4–6 | 0.96 | 0.59–1.57 | 1.13 | 0.95–1.33 | 1.47 *** | 1.27–1.71 |
| 7 and above | 0.88 | 0.31–2.51 | 1.09 | 0.77–1.54 | 1.00 | 0.72–1.38 |
| Contraceptive method | ||||||
| None | 1.00 | 1.00 | 1.00 | |||
| Traditional | - | - | 0.049 | 0.01–1.29 | 0.04 * | 0.01–0.72 |
| Modern | 1.43 | 0.93–2.17 | 1.14 | 0.98–1.32 | 1.21 ** | 1.06–1.38 |
| Breastfeeding | ||||||
| No | 1.00 | 1.00 | 1.00 | |||
| Yes | 1.55 | 0.92–2.60 | 1.07 | 0.86–1.31 | 0.48 *** | 0.38–0.59 |
| Living with partner | ||||||
| No | 1.00 | 1.00 | 1.00 | |||
| Yes | 2.74 | 0.77–9.72 | 1.50 ** | 1.11–2.01 | 1.07 | 0.83–1.37 |
| Long working hours | ||||||
| No | 1.00 | 1.00 | 1.00 | |||
| Yes | 1.06 | 0.68–1.67 | 1.51 *** | 1.29–1.76 | 1.87 *** | 1.62–2.15 |
| Cigarette smoking | ||||||
| No | 1.00 | 1.00 | 1.00 | |||
| Yes | 2.65 ** | 1.40–5.00 | 0.58 | 0.41–0.82 | 0.60 ** | 0.44–0.81 |
| Factors | Underweight | Overweight | Obese | |||
|---|---|---|---|---|---|---|
| UOR | 95% CI | UOR | 95% CI | UOR | 95% CI | |
| Age group | ||||||
| 15–19 | 1.00 | 1.00 | 1.00 | |||
| 20–24 | 1.35 ** | 1.08−1.66 | 2.61 * | 1.05−6.44 | 1 | - |
| 25–29 | 1.11 ** | 1.03−1.18 | 3.94 ** | 1.75−8.86 | 0.34 | 0.07−1.64 |
| 30–34 | 1.39 *** | 1.20−1.58 | 5.18 *** | 2.39−11.19 | 0.37 *** | 0.34−0.39 |
| 35–39 | 1.01 | 0.69−1.45 | 6.67 *** | 3.00−14.82 | 0.72 *** | 0.69−0.76 |
| 40–44 | 0.83 ** | 0.82−0.83 | 6.34 ** | 2.12−18.91 | 0.72 | 0.50−1.05 |
| 45–49 | 1.05 | 0.82−1.35 | 7.51 *** | 2.84−19.48 | 0.93 | 0.79−1.08 |
| Education | ||||||
| No education | 1.00 | 1.00 | 1.00 | |||
| Primary | 0.48 *** | 0.41–0.56 | 1.22 ** | 1.07–1.39 | 1.35 *** | 1.33–1.36 |
| Secondary | 0.56 *** | 0.50–0.63 | 1.18 | 0.71–1.94 | 1.86 * | 1.11–3.12 |
| Tertiary | 0.400 *** | 0.25–0.66 | 1.40 | 0.94–2.07 | 2.45 *** | 1.79–3.35 |
| Employment status | ||||||
| Unemployed | 1.00 | 1.00 | 1.00 | |||
| Self–employed | 1.37 *** | 1.26–1.48 | 0.82 | 0.22–3.01 | 14.49 *** | 9.18–22.85 |
| Employed | 1.26 | 0.80–1.98 | 0.77 | 0.18–3.20 | 13.59 *** | 4.61–40.06 |
| Wealth index | ||||||
| Poorest | 1.00 | 1.00 | 1.00 | |||
| Poorer | 0.95 | 0.60–1.49 | 1.82 *** | 1.57–2.12 | 1.31 | 0.71–2.42 |
| Average | 0.71 *** | 0.66–0.77 | 1.99 ** | 1.40–2.81 | 1.27 | 0.73–2.21 |
| Richer | 0.90 | 0.57–1.43 | 2.89 *** | 1.62–5.15 | 2.08 | 0.81–5.28 |
| Richest | 0.92 | 0.51–1.65 | 4.04 *** | 2.31–7.06 | 2.96 * | 1.19–7.35 |
| Marital Status | ||||||
| Single | 1.00 | 1.00 | 1.00 | |||
| Married | 1.13 | 0.64–1.99 | 1.64 | 0.78–3.45 | 1.05 | 0.71–1.57 |
| Cohabiting | - | - | - | - | - | - |
| Widowed | - | - | - | - | - | - |
| Divorced/separated | - | - | - | - | - | - |
| Geopolitical zone | ||||||
| North central | 1.00 | 1.00 | 1.00 | |||
| Northeast | 3.16 *** | 2.68–3.71 | 0.98 | 0.76–1.26 | 0.99 | 0.95–1.03 |
| Northwest | 1.31 | 0.94–1.82 | 0.83 | 0.67–1.03 | 0.59 ** | 0.44–0.79 |
| Southeast | 1.27 | 0.27–5.83 | 1.21 *** | 1.12–1.31 | 0.95 | 0.54–1.69 |
| South south | 1.18 | 0.76–1.85 | 1.38 *** | 1.28–1.46 | 1.10 | 0.70–1.71 |
| Southwest | 1.50 | 0.48–4.61 | 1.12 | 0.90–1.38 | 0.85 | 0.46–1.58 |
| Height | ||||||
| Below average | 1.00 | 1.00 | 1.00 | |||
| Above average | 1.07 | 0.98–1.16 | 0.89 | 0.76–1.04 | 0.03 *** | 0.01–0.13 |
| Weight | ||||||
| Below average | − | − | 1.00 | |||
| Above average | − | − | − | − | 36,169.13 *** | 7536.5–173,583.4 |
| Children borne | ||||||
| 1–3 | 1.00 | 1.00 | 1.00 | |||
| 4–6 | 0.77 | 0.68–0.88 | 1.03 | 0.89–1.18 | 1.41 | 0.88–2.25 |
| 7 and above | 0.96 | 0.79–1.16 | 1.07 | 0.92–1.25 | 1.26 | 0.81–1.97 |
| Contraceptive method | ||||||
| None | 1.00 | 1.00 | 1.00 | |||
| Folkloric | 1.32 | 0.23–7.47 | 0.54 ** | 0.36–0.81 | 0.75 | 0.47–1.18 |
| Traditional | 0.73 | 0.23–2.27 | 1.79 *** | 1.46–2.19 | 2.23 *** | 1.79–2.76 |
| Modern | 0.94 | 0.41–2.11 | 1.61 ** | 1.21–2.14 | 1.27 * | 1.03–1.57 |
| Breastfeeding | ||||||
| No | 1.00 | 1.00 | 1.00 | |||
| Yes | 1.27 *** | 1.21–1.33 | 0.96 | 0.87–1.06 | 0.94 | 0.69–1.27 |
| Living with partner | ||||||
| No | 1.00 | 1.00 | 1.00 | |||
| Yes | 1.23 | 0.85–1.77 | 0.91 *** | 0.89–0.94 | 1.05 *** | 1.01–1.07 |
| Long working hours | ||||||
| No | 1.00 | 1.00 | 1.00 | |||
| Yes | 1.04 | 0.83–1.29 | 0.75 * | 0.59–0.95 | 0.93 | 0.66–1.29 |
| Cigarette smoking | ||||||
| No | − | − | − | − | 1.00 | − |
| Yes | − | − | − | − | 2.62 | 0.02–233.26 |
| Residence | ||||||
| Sd (cons) | 0.21 | 0.20–0.21 | 0.31 | 0.31–0.32 | 0.62 | 0.61–0.62 |
| Factors | Underweight | Overweight | Obese | |||
|---|---|---|---|---|---|---|
| UOR | 95% CI | UOR | 95% CI | UOR | 95% CI | |
| Age group | ||||||
| 15–19 | 1.00 | 1.00 | 1.00 | |||
| 20–24 | 0.032 | 0.001–10.2 | 0.32 ** | 0.14–0.70 | 51.46 | 0.61–113.42 |
| 25–29 | 0.051 | 0.002–12.2 | 0.45 ** | 0.25–0.79 | 43.84 | 0.58–104.32 |
| 30–34 | 0.010 | 0.001–2.31 | 0.61 * | 0.37–0.99 | 22.72 | 0.31–91.17 |
| 35–39 | 0.00004 * | 1.5 × 10−8–0.16 | 0.89 | 0.54–1.48 | 97.83 | 0.93–161.74 |
| 40–44 | 0.0036 | 7.1 × 10−6–1.82 | 1.05 | 0.65–1.67 | 63.47 | 0.83–117.48 |
| 45–49 | 0.0015 * | 2.3 × 10−6–0.98 | 1.00 | - | 109.24 | 0.96–191.83 |
| Education | ||||||
| No education | 1.00 | 1.00 | 1.00 | |||
| Primary | 0.03 | 0.003–2.46 | 2.72 * | 1.23–5.95 | 0.02 ** | 0.002–0.212 |
| Secondary | 1.79 | 0.04–71.96 | 6.64 *** | 3.03–14.50 | 1.35 | 0.18–9.85 |
| Tertiary | − | − | 2.92 * | 1.07–7.93 | 0.001 *** | 0.0001–0.014 |
| Employment status | ||||||
| Unemployed | 1.00 | 1.00 | 1.00 | |||
| Self–employed | 0.44 ** | 0.28–0.70 | 1.38 | 0.82–2.33 | 11.98 ** | 1.86–77.09 |
| Employed | − | − | 2.44 * | 1.17–5.03 | 161,820.6 *** | 2560.6–1.2 × 107 |
| Wealth index | ||||||
| Poorest | 1.00 | 1.00 | 1.00 | |||
| Poorer | 4.91 | 0.39–61.14 | 0.68 | 0.44–1.05 | 1.91 | 0.56–6.48 |
| Average | 8.82 | 0.45–171.9 | 1.41 | 0.91–2.16 | 0.20 * | 0.04–0.89 |
| Richer | 208.16 ** | 6.2–6887.6 | 3.05 *** | 1.83–5.07 | 0.56 | 0.09–3.29 |
| Richest | − | − | 0.61 | 0.34–1.09 | 0.02 ** | 0.001–0.35 |
| Marital status | ||||||
| Single | 1.00 | 1.00 | 1.00 | |||
| Married | 0.48 | 0.06–3.70 | 0.85 | 0.61–1.18 | 0.69 | 0.22–2.08 |
| Cohabiting | - | - | - | - | - | - |
| Widowed | - | - | - | - | - | - |
| Divorced/Separated | - | - | - | - | - | - |
| Provinces | ||||||
| Western Cape | 1.00 | 1.00 | 1.00 | |||
| Eastern Cape | 0.49 | 0.05–4.87 | 5.25 *** | 2.36–11.64 | 144.32 *** | 8.89–2342.66 |
| Northern Cape | 0.14 | 0.07–2.49 | 0.63 | 0.22–1.77 | 9.94 | 0.84–116.62 |
| Free State | 0.46 | 0.02–7.92 | 2.19 | 0.83–5.74 | 1477.11 *** | 55.47–39,329.67 |
| KwaZulu-Natal | 1 | − | 4.87 *** | 2.31–10.25 | 1717.30 *** | 77.11–38,244.93 |
| Northwest | 0.12 | 0.005–2.74 | 3.05 ** | 1.35–6.89 | 1626.01 *** | 109.41–24,163.2 |
| Gauteng | 1 | − | 1.73 | 0.90–3.33 | 14.51 * | 1.41–148.97 |
| Mpumalanga | 0.04 | 0.002–0.69 | 2.63 * | 1.23–5.60 | 58.84 ** | 3.77–916.98 |
| Limpopo | 0.74 | 0.03–15.36 | 4.56 *** | 2.07–10.04 | 2.25 | 0.13–38.31 |
| Height | ||||||
| Below average | 1.00 | 1.00 | 1.00 | |||
| Above average | 0.10 * | 0.018–0.66 | 0.39 *** | 0.29–0.54 | - | - |
| Weight | ||||||
| Below average | 1.00 | 1.00 | 1.00 | |||
| Above average | - | - | 569.35 *** | 99.6–3255.8 | 2.9 × 1019 *** | 2.5 × 1017–3.4 × 1021 |
| Children borne | ||||||
| 1–3 | 1.00 | 1.00 | 1.00 | |||
| 4–6 | 0.09 | 0.004–2.24 | 0.51 *** | 0.35–0.74 | 0.57 | 0.21–1.49 |
| 7+ | 273.08 ** | 6.2–11,859.8 | 1.28 | 0.65–2.50 | 0.0004 *** | 1.2 × 10−6–0.0013 |
| Contraceptive method | ||||||
| None | 1.00 | 1.00 | 1.00 | |||
| Traditional | 1 | - | 1 | - | 1 | - |
| Modern | 0.49 | 0.06–3.66 | 1.43 * | 1.05–1.92 | 0.66 | 0.22–1.98 |
| Breastfeeding | ||||||
| No | 1.00 | 1.00 | 1.00 | |||
| Yes | 0.82 | 0.09–6.73 | 1.69 * | 1.07–2.63 | 22.68 ** | 3.48–147.47 |
| Currently living with partner | ||||||
| No | 1.00 | 1.00 | 1.00 | |||
| Yes | 17.75 | 0.67–464.7 | 1.81 ** | 1.22–2.67 | 0.93 | 0.32–3.70 |
| Long working hours | ||||||
| No | 1.00 | 1.00 | 1.00 | |||
| Yes | 5.44 | 0.51–57.14 | 0.82 | 0.54–1.23 | 0.29 * | 0.08–0.96 |
| Cigarette smoking | ||||||
| No | 1.00 | 1.00 | 1.00 | |||
| Yes | 2.14 ** | 1.27–3.61 | 0.41 ** | 0.21–0.78 | 145.99 *** | 16.22–1313.38 |
| Residence | ||||||
| Sd (cons) | 0.16 | 0.16–0.17 | 0.29 | 0.28–0.29 | 0.48 | 0.48–0.49 |
| Multilevel Model for Nigeria BMI Categories ‘ICC Estimate’ | |||
|---|---|---|---|
| Models | ICC | Standard Error | 95% CI |
| Model 1 (Underweight) | 0.0127 | 0.0003 | 0.0121–0.0133 |
| Model 2 (Overweight) | 0.0289 | 0.0001 | 0.0288–0.0289 |
| Model 3 (Obese) | 0.1040 | 0.0001 | 0.1038–0.1041 |
| Multilevel Model for South Africa BMI Categories ‘ICC Estimate’ | |||
| Models | ICC | Standard Error | 95% CI |
| Model 1 (Underweight) | 0.0102 | 0.0002 | 0.0092–0.0121 |
| Model 2 (Overweight) | 0.0271 | 0.0001 | 0.0238–0.0316 |
| Model 3 (Obese) | 0.0819 | 0.0007 | 0.0801–0.0864 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akokuwebe, M.E.; Idemudia, E.S. Multilevel Analysis of Urban–Rural Variations of Body Weights and Individual-Level Factors among Women of Childbearing Age in Nigeria and South Africa: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2022, 19, 125. https://doi.org/10.3390/ijerph19010125
Akokuwebe ME, Idemudia ES. Multilevel Analysis of Urban–Rural Variations of Body Weights and Individual-Level Factors among Women of Childbearing Age in Nigeria and South Africa: A Cross-Sectional Survey. International Journal of Environmental Research and Public Health. 2022; 19(1):125. https://doi.org/10.3390/ijerph19010125
Chicago/Turabian StyleAkokuwebe, Monica Ewomazino, and Erhabor Sunday Idemudia. 2022. "Multilevel Analysis of Urban–Rural Variations of Body Weights and Individual-Level Factors among Women of Childbearing Age in Nigeria and South Africa: A Cross-Sectional Survey" International Journal of Environmental Research and Public Health 19, no. 1: 125. https://doi.org/10.3390/ijerph19010125
APA StyleAkokuwebe, M. E., & Idemudia, E. S. (2022). Multilevel Analysis of Urban–Rural Variations of Body Weights and Individual-Level Factors among Women of Childbearing Age in Nigeria and South Africa: A Cross-Sectional Survey. International Journal of Environmental Research and Public Health, 19(1), 125. https://doi.org/10.3390/ijerph19010125