
Using Open-Access Data to Explore Relations between Urban Landscapes and Diarrhoeal Diseases in Côte d’Ivoire


Abstract
:1. Introduction
2. Materials and Methods
2.1. Datasets
2.2. Data Pre-Processing
2.3. Statistical Models and Feature Selection
2.4. Addressing Spatial Dependence
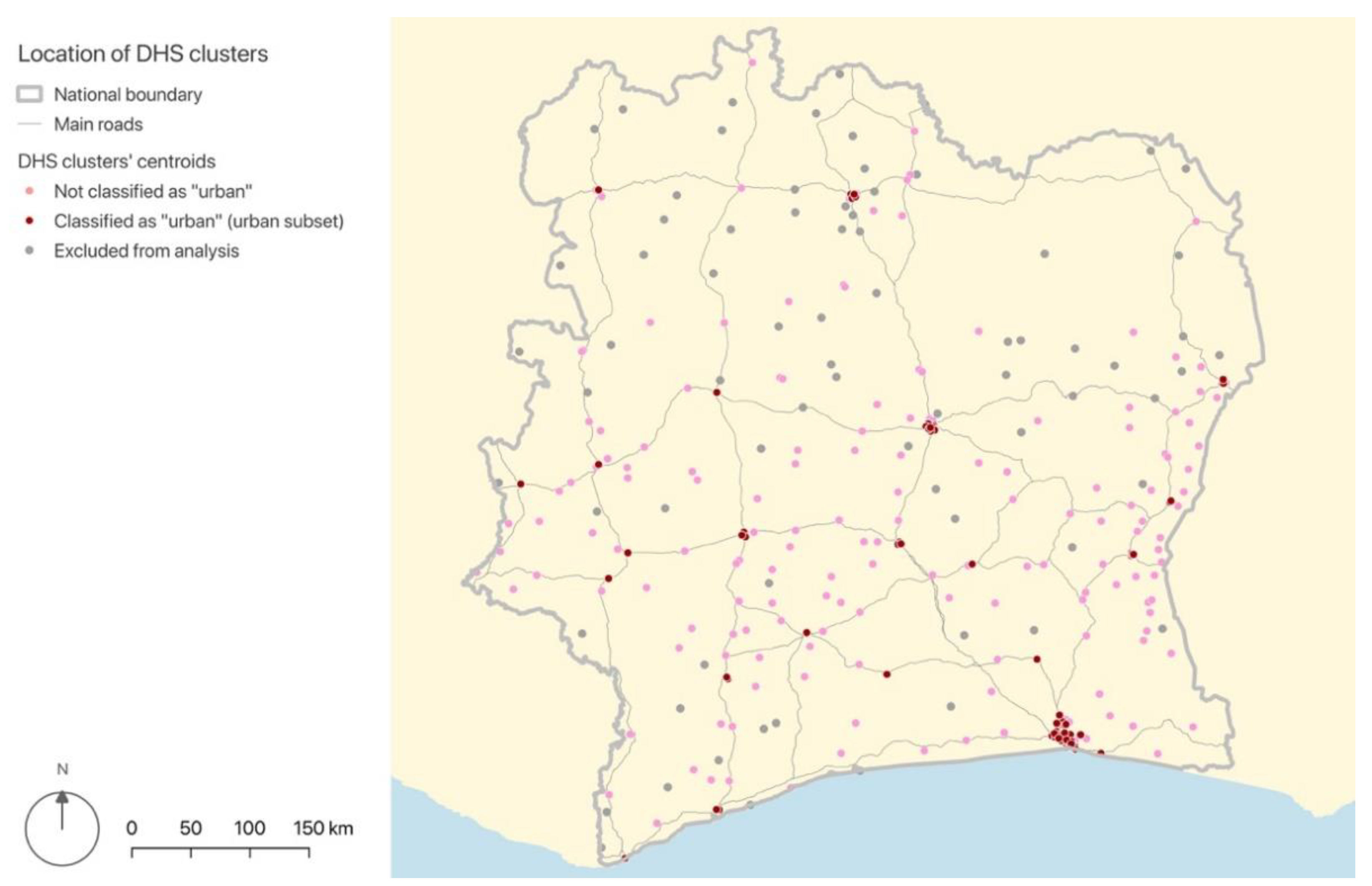
2.5. Inclusion Criteria and Stratification of Analysis
3. Results
3.1. Overall Clustering of Data and Need for Spatial Regressions
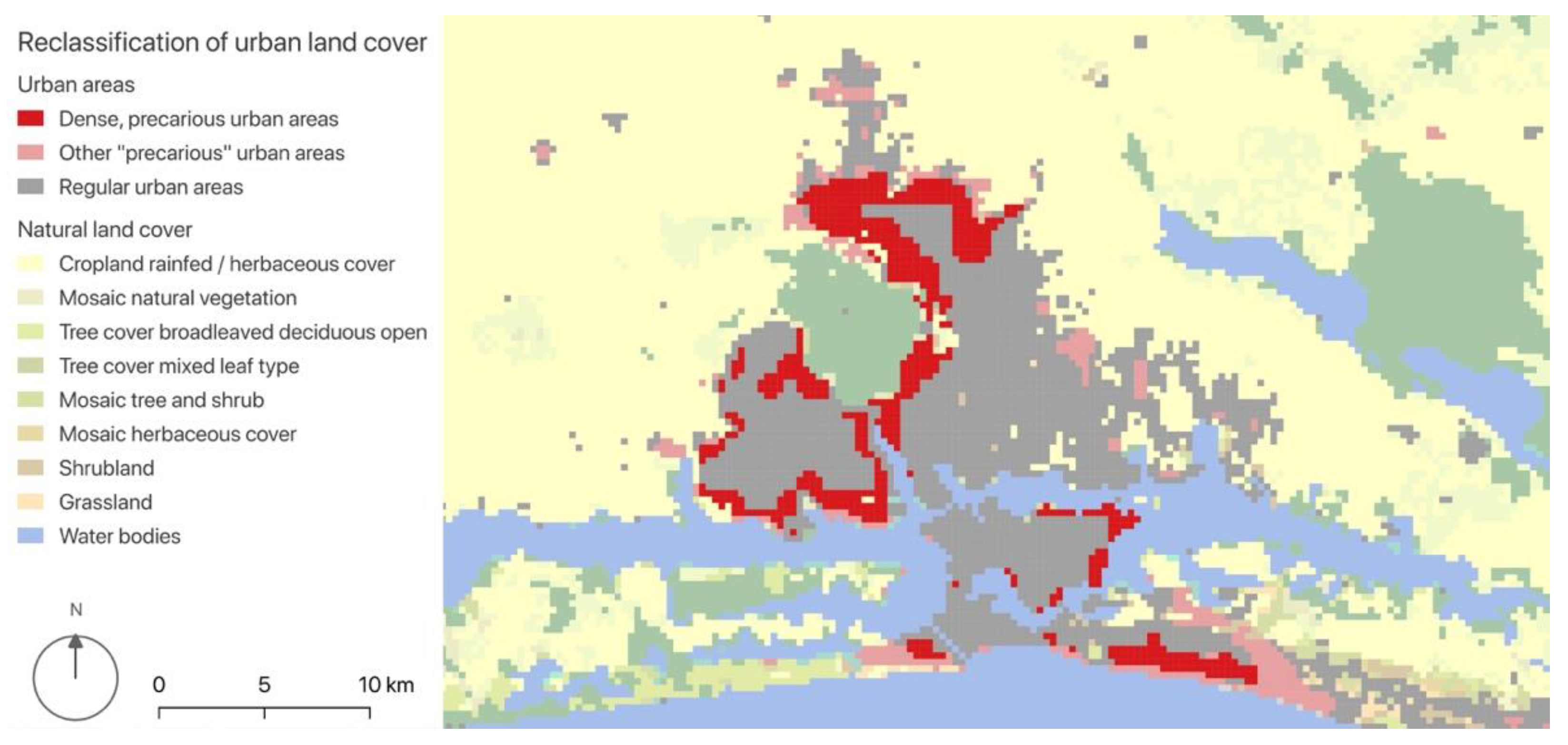
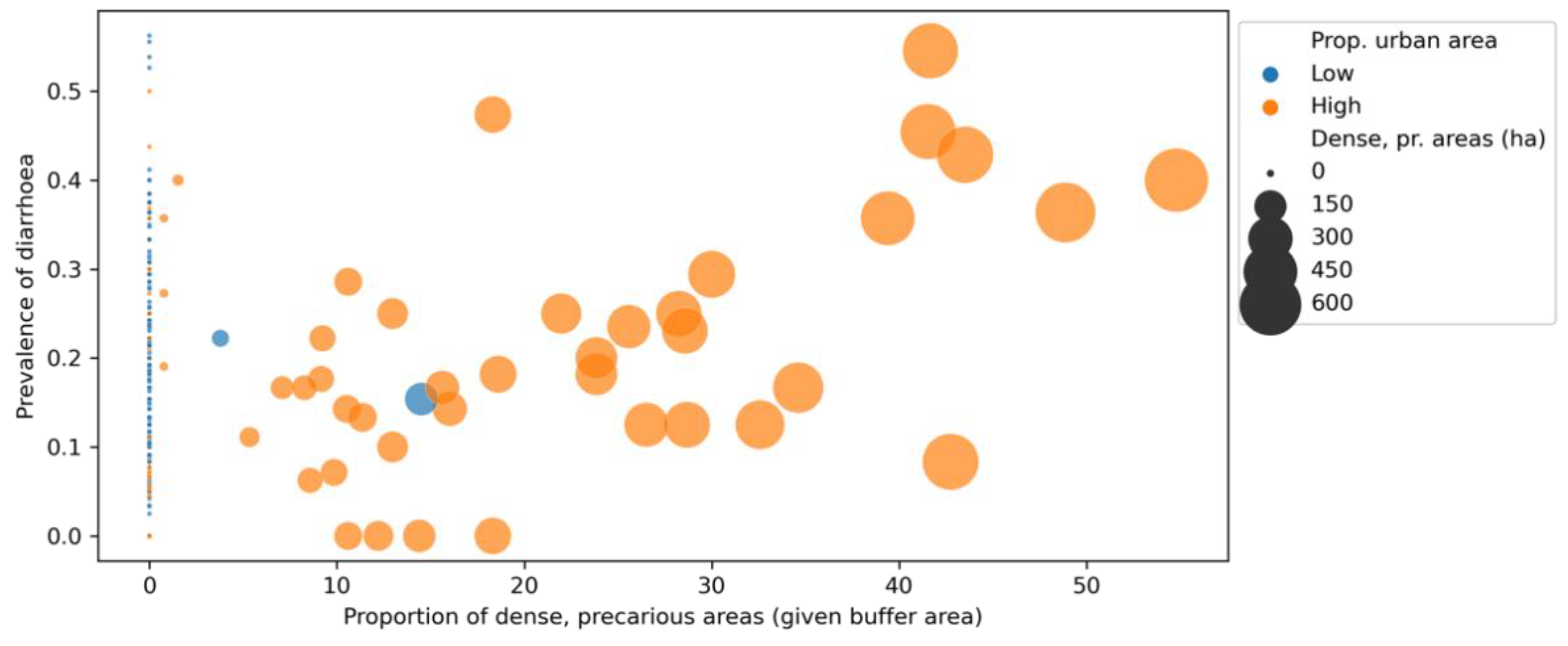
3.2. Significant Landscape Feature: Dense, Precarious Urban Areas
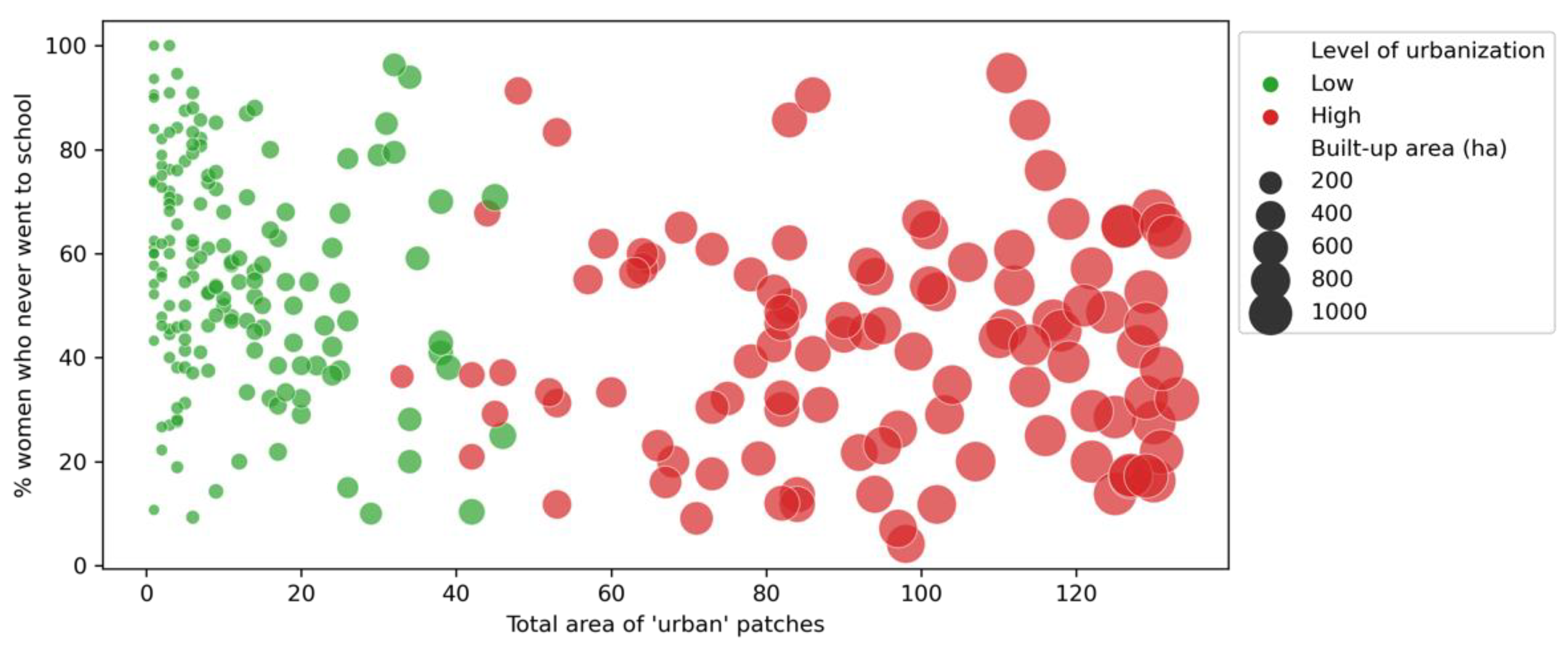
3.3. Stages of Urbanisation and Landscape Patterns
4. Discussion
4.1. Towards Spatial Predictors of Health Outcomes in Urban Areas
4.2. Saturation of Urban Settlements and Health Inequities
4.3. Study’s Limitations and Need for Further Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Computer Code and Software
Appendix A

Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Statistic | Prevalence of Diarrhoea (%) | Access to Basic 1 Water (%) | Access to Basic 1 Sanitation (%) | Women who Never Went to School (%) | ||||
|---|---|---|---|---|---|---|---|---|
| Excluded obs. (n = 84) | Retained obs. (n = 267) | Excluded obs. (n = 84) | Retained obs. (n = 267) | Excluded obs. (n = 84) | Retained obs. (n = 267) | Excluded obs. (n = 84) | Retained obs. (n = 267) | |
| Median value | 16.7 | 16.7 | 67.1 | 87.4 | 3.7 | 18.5 | 83.0 | 50.0 |
| Mean value | 17.8 | 18.2 | 61.0 | 78.1 | 6.2 | 27.0 | 80.1 | 51.0 |
| Standard deviation | 10.9 | 12.6 | 27.7 | 24.9 | 7.9 | 26.1 | 15.4 | 22.2 |
| Minimum value | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 34.8 | 4.2 |
| Maximum value | 42.9 | 56.3 | 100.0 | 100.0 | 33.3 | 100.0 | 100.0 | 100.0 |
Appendix C
| Location | Size and Category 1 | N° Clusters | Mean Prevalence of Diarrhoea 2 | Standard Deviation of Sample | Range (Min. and Max. Values) |
|---|---|---|---|---|---|
| Abidjan | Large (“global connector”) | 48 | 21.4 | 13.8 | 0.0/54.5 |
| Yamoussoukro | Medium (“global connector”) | 5 | 14.5 | 11.0 | 0.0/29.4 |
| San Pédro | Medium (“global connector”) | 4 | 14.5 | 13.2 | 0.0/28.6 |
| Bouaké | Medium-large (“regional connector”) | 16 | 12.1 | 9.4 | 0.0/33.3 |
| Korhogo | Medium (“regional connector”) | 6 | 12.5 | 11.5 | 0.0/29.4 |
| Daloa | Medium (“regional connector”) | 4 | 26.0 | 7.5 | 20.0/36.8 |
| Katiola | Small (“local connector”) | 2 | 5.9 | 8.3 | 0.0/11.8 |
| Douékoué | Small (“local connector”) | 1 | 43.8 | - | - |
| Divo | Small (“local connector”) | 1 | 15.4 | - | - |
Appendix D
| Pre-Selected Control Variables | Variance Inflation Factor | Weighted OLS (DHS Cluster Weights) R2 = 0.059/AIC = 46.45 Jarque-Bera Test for Normality of Errors: 31.090 (p < 0.001) Breusch-Pagan Test for Heteroskedasticity: 4.152 (p = 0.656) | ||
|---|---|---|---|---|
| Coef. | SE | Prob. | ||
| Constant | - | 0.448 | 0.079 | 0.000 |
| % of the population with access to basic water facilities 1 | 1.468 | 0.074 | 0.067 | 0.270 |
| % of the population with access to basic sanitation facilities 1 | 1.970 | −0.254 | 0.076 | 0.001 |
| % of the population with access to safe hygiene facilities 1 | 1.363 | −0.034 | 0.054 | 0.535 |
| % of the female population who never went to school | 1.744 | −0.261 | 0.079 | 0.001 |
| Mean accumulated precipitation (monthly values) in 2012 | 1.260 | 0.049 | 0.063 | 0.436 |
| Mean maximal temperature (monthly values) in 2012 | 1.165 | 0.0008 | 0.091 | 0.993 |
References
- Troeger, C.; Blacker, B.F.; Khalil, I.A.; Rao, P.C.; Cao, S.; Zimsen, S.R.; Albertson, S.B.; Stanaway, J.D.; Deshpande, A.; Abebe, Z.; et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1211–1228. [Google Scholar] [CrossRef] [Green Version]
- WHO. Water, Sanitation, Hygiene and Health: A Primer for Health Professionals; World Health Organization: Geneva, Switzerland, 2019; p. 36. Available online: https://www.who.int/publications/i/item/WHO-CED-PHE-WSH-19.149 (accessed on 17 May 2022).
- Prüss, A.; Kay, D.; Fewtrell, L.; Bartram, J. Estimating the burden of disease from water, sanitation, and hygiene at a global level. Environ. Health Perspect. 2002, 110, 6. [Google Scholar] [CrossRef]
- Koné, B.; Doumbia, M.; Sy, I.; Dongo, K.; Agbo-Houenou, Y.; Houenou, P.V.; Fayomi, B.; Bonfoh, B.; Tanner, M.; Cissé, G. Étude des diarrhées en milieu périurbain à Abidjan par l’approche écosanté. VertigO 2014, 19, 14976. [Google Scholar] [CrossRef]
- Wolf, J.; Prüss-Ustün, A.; Cumming, O.; Bartram, J.; Bonjour, S.; Cairncross, S.; Clasen, T.; Colford, J.M.; Curtis, V.; De France, J.; et al. Systematic review: Assessing the impact of drinking water and sanitation on diarrhoeal disease in low- and middle-income settings: Systematic review and meta-regression. Trop. Med. Int. Health 2014, 19, 928–942. [Google Scholar] [CrossRef]
- Thiam, S.; Cissé, G.; Stensgaard, A.-S.; Niang-Diène, A.; Utzinger, J.; Vounatsou, P. Bayesian conditional autoregressive models to assess spatial patterns of diarrhoea risk among children under the age of 5 years in Mbour, Senegal. Geospat. Health 2019, 14, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Reiner, R.C.; Wiens, K.E.; Deshpande, A.; Baumann, M.M.; Lindstedt, P.A.; Blacker, B.F.; Troeger, C.E.; Earl, L.; Munro, S.B.; Abate, D.; et al. Mapping geographical inequalities in childhood diarrhoeal morbidity and mortality in low-income and middle-income countries, 2000–2017: Analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 1779–1801. [Google Scholar] [CrossRef]
- Galea, S.; Vlahov, D. Urban health: Evidence, challenges, and directions. Annu. Rev. Public Health 2005, 26, 341–365. [Google Scholar] [CrossRef] [Green Version]
- Ezeh, A.; Oyebode, O.; Satterthwaite, D.; Chen, Y.-F.; Ndugwa, R.; Sartori, J.; Mberu, B.; Melendez-Torres, G.J.; Haregu, T.; Watson, S.I.; et al. The history, geography, and sociology of slums and the health problems of people who live in slums. Lancet 2017, 389, 547–558. [Google Scholar] [CrossRef]
- Mattioli, M.C.M.; Davis, J.; Boehm, A.B. Hand-to-Mouth Contacts Result in Greater Ingestion of Feces than Dietary Water Consumption in Tanzania: A Quantitative Fecal Exposure Assessment Model. Environ. Sci. Technol. 2015, 49, 1912–1920. [Google Scholar] [CrossRef]
- Turner, M.G.; Gardner, R.H. Landscape Ecology in Theory and Practice: Pattern and Process, 2nd ed.; Springer: New York, NY, USA, 2015; ISBN 978-1-4939-2793-7. [Google Scholar]
- Collins, J.P.; Kinzig, A.; Grimm, N.B.; Fagan, W.F.; Hope, D.; Wu, J.; Borer, E.T. A New Urban Ecology: Modeling human communities as integral parts of ecosystems poses special problems for the development and testing of ecological theory. Am. Sci. 2000, 88, 416–425. [Google Scholar]
- Forman, R.T.T.; Godron, M. Patches and Structural Components for a Landscape Ecology. BioScience 1981, 31, 733–740. [Google Scholar] [CrossRef]
- Bosch, M.; Chenal, J.; Joost, S. Addressing Urban Sprawl from the Complexity Sciences. Urban Sci. 2019, 3, 3020060. [Google Scholar] [CrossRef] [Green Version]
- Baptista, E.A.; Queiroz, B.L. Spatial analysis of mortality by cardiovascular disease in the adult population: A study for brazilian micro-regions between 1996 and 2015. Spat. Demogr. 2019, 7, 83–101. [Google Scholar] [CrossRef]
- Arino, J. Spatio-temporal spread of infectious pathogens of humans. Infect. Dis. Model. 2017, 2, 218–228. [Google Scholar] [CrossRef] [PubMed]
- Araujo, R.V.; Albertini, M.R.; Costa-da-Silva, A.L.; Suesdek, L.; Franceschi, N.C.S.; Bastos, N.M.; Katz, G.; Cardoso, V.A.; Castro, B.C.; Capurro, M.L.; et al. São Paulo urban heat islands have a higher incidence of dengue than other urban areas. Braz. J. Infect. Dis. 2015, 19, 146–155. [Google Scholar] [CrossRef] [Green Version]
- Rossi, J.-P.; Kadaouré, I.; Godefroid, M.; Dobigny, G. Landscape epidemiology in urban environments: The example of rodent-borne Trypanosoma in Niamey, Niger. Infect. Genet. Evol. 2018, 63, 307–315. [Google Scholar] [CrossRef]
- WHO. Urban HEART: Urban Health Equity Assessment and Response Tool; World Health Organization, The WHO Centre for Health Development: Kobe, Japan, 2010; ISBN 978-92-4-150014-2.
- Elsey, H.; Thomson, D.R.; Lin, R.Y.; Maharjan, U.; Agarwal, S.; Newell, J. Addressing inequities in urban health: Do decision-makers have the data they need? Report from the urban health data special session at International Conference on Urban Health Dhaka 2015. J. Urban Health 2016, 93, 526–537. [Google Scholar] [CrossRef] [Green Version]
- OECD; Sahel and West Africa Club. Africa’s Urbanisation Dynamics 2020: Africapolis, Mapping a New Urban Geography; West African Studies; OECD: Paris, France, 2020; ISBN 978-92-64-57958-3. [Google Scholar]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Fall, M.; Coulibaly, S. (Eds.) Diversified Urbanization: The Case of Côte d’Ivoire; World Bank: Washington, DC, USA, 2016; ISBN 978-1-4648-0809-8. [Google Scholar]
- Chenal, J. La Ville Ouest-Africaine: Modèles de Planification de L’espace Urbain; Vuesdensemble; Metispresses: Genève, Switzerland, 2013; ISBN 978-2-940406-18-0. [Google Scholar]
- WHO; UNICEF. WHO/UNICEF Joint Monitoring Programme for Water Supply, Sanitation and Hygiene. Available online: https://washdata.org/data/household#!/ (accessed on 11 May 2022).
- UN-Habitat. World Cities Report 2016. Urbanization and Development: Emerging Futures; World Cities Report; UN-Habitat: Nairobi, Kenya, 2016; ISBN 978-92-1-133395-4. [Google Scholar]
- Mberu, B.U.; Haregu, T.N.; Kyobutungi, C.; Ezeh, A.C. Health and health-related indicators in slum, rural, and urban communities: A comparative analysis. Glob. Health Action 2016, 9, 33163. [Google Scholar] [CrossRef]
- DHS. The DHS Program—Available Datasets. Available online: https://dhsprogram.com/data/available-datasets.cfm (accessed on 11 May 2022).
- INS [Côte d’Ivoire]; ICF International. Demographic and Health Survey 2011–2012 [Dataset]. CIGE61FL.SHP; Institut National de la Statistique-INS/Côte d’Ivoire and ICF International [Producers]; ICF International [Distributor]: Calverton, MD, USA, 2013. [Google Scholar]
- INS [Côte d’Ivoire]; ICF International. Demographic and Health Survey 2011–2012 [Dataset]. CIHR62FL.DTA; Institut National de la Statistique-INS/Côte d’Ivoire and ICF International [Producers]; ICF International [Distributor]: Calverton, MD, USA, 2013. [Google Scholar]
- INS [Côte d’Ivoire]; ICF International. Demographic and Health Survey 2011–2012 [Dataset]. CIIR62FL.DTA; Institut National de la Statistique-INS/Côte d’Ivoire and ICF International [Producers]; ICF International [Distributor]: Calverton, MD, USA, 2013. [Google Scholar]
- INS [Côte d’Ivoire]; ICF International. Demographic and Health Survey 2011–2012 [Dataset]. CIKR62FL.DTA; Institut National de la Statistique-INS/Côte d’Ivoire and ICF International [Producers]; ICF International [Distributor]: Calverton, MD, USA, 2013. [Google Scholar]
- Abatzoglou, J.T.; Dobrowski, S.Z.; Parks, S.A.; Hegewisch, K.C. TerraClimate, a high-resolution global dataset of monthly climate and climatic water balance from 1958–2015. Sci. Data 2018, 5, 170191. [Google Scholar] [CrossRef] [Green Version]
- Carlton, E.J.; Woster, A.P.; DeWitt, P.; Goldstein, R.S.; Levy, K. A systematic review and meta-analysis of ambient temperature and diarrhoeal diseases. Int. J. Epidemiol. 2016, 45, 117–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NASA. Earth at Night. Available online: https://earthobservatory.nasa.gov/features/NightLights/page3.php (accessed on 11 May 2022).
- ESA. Land Cover CCI Product User Guide Version 2. 2017. Available online: http://maps.elie.ucl.ac.be/CCI/viewer/download/ESACCI-LC-Ph2-PUGv2_2.0.pdf (accessed on 11 May 2022).
- Stevens, F.R.; Gaughan, A.E.; Linard, C.; Tatem, A.J. Disaggregating census data for population mapping using random forests with remotely-sensed and ancillary data. PLoS ONE 2015, 10, e0107042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friesen, J.; Friesen, V.; Dietrich, I.; Pelz, P.F. Slums, space, and state of health—a link between settlement morphology and health data. Int. J. Environ. Res. Public. Health 2020, 17, 2022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosch, M. PyLandStats: An open-source Pythonic library to compute landscape metrics. PLoS ONE 2019, 14, e0225734. [Google Scholar] [CrossRef] [Green Version]
- Perry, M.; Goodman, S.; Özak, Ö.; Smith, T.J.; Rykov, D.; Taylor, S.; Collins, B.; Valgur, M.; Amdal, H.; Pounder, N.; et al. Rasterstats. Available online: https://github.com/perrygeo/python-rasterstats (accessed on 13 May 2022).
- Gillies, S.; Perry, M.; Wurster, K.; Ward, B.; Jonas; Snow, A.D.; McBride, J.; Talbert, C.; Seglem, E.; Fitzsimmons, S.; et al. Rasterio: Geospatial Raster I/O for Python Programmers. Available online: https://github.com/rasterio/rasterio (accessed on 13 May 2022).
- Wasser, L.; Joseph, M.; McGlinchy, J.; Palomino, J.; Korinek, N.; Holdgraf, C.; Head, T. EarthPy: A Python package that makes it easier to explore and plot raster and vector data using open source Python tools. J. Open Source Softw. 2019, 4, 1886. [Google Scholar] [CrossRef] [Green Version]
- Gillies, S.; Buffat, R.; Arnott, J.; Wurster, K.; Cochran, M.; Perry, M.; de Andrade, E.S.; Jordahl, K.; Young, P.; Norris, S.; et al. Fiona. Available online: https://github.com/Toblerity/Fiona (accessed on 13 May 2022).
- McKinney, W. Data structures for statistical computing in Python. In Proceedings of the 9th Python in Science Conference, Austin, TX, USA, 28 June–3 July 2010; pp. 56–61. [Google Scholar]
- Jordahl, K.; den Bossche, J.V.; Fleischmann, M.; McBride, J.; Wasserman, J.; Gerard, J.; Badaracco, A.G.; Snow, A.D.; Tratner, J.; Perry, M.; et al. Geopandas/Geopandas: v0.9.0. Available online: https://zenodo.org/record/4569086 (accessed on 17 May 2022).
- Harris, C.R.; Millman, K.J.; van der Walt, S.J.; Gommers, R.; Virtanen, P.; Cournapeau, D.; Wieser, E.; Taylor, J.; Berg, S.; Smith, N.J.; et al. Array programming with NumPy. Nature 2020, 585, 357–362. [Google Scholar] [CrossRef]
- Seabold, S.; Perktold, J. Statsmodels: Econometric and statistical modeling with Python. In Proceedings of the the 9th Python in Science Conference (SciPy 2010), Austin, TX, USA, 28 June–3 July 2010; pp. 92–96. [Google Scholar]
- Rey, S.J.; Anselin, L. PySAL: A Python library of spatial analytical methods. Rev. Reg. Stud. 2007, 37, 5–27. [Google Scholar] [CrossRef]
- Hunter, J.D. Matplotlib: A 2D graphics environment. Comput. Sci. Eng. 2007, 9, 90–95. [Google Scholar] [CrossRef]
- Waskom, M. Seaborn: Statistical data visualization. J. Open Source Softw. 2021, 6, 3021. [Google Scholar] [CrossRef]
- Grace, K.; Nagle, N.N.; Burgert-Brucker, C.R.; Rutzick, S.; Van Riper, D.C.; Dontamsetti, T.; Croft, T. Integrating environmental context into DHS analysis while protecting participant confidentiality: A new remote sensing method. Popul. Dev. Rev. 2019, 45, 197–218. [Google Scholar] [CrossRef]
- UNICEF; WaterAid; WSUP. Female-Friendly Public and Community Toilets: A Guide for Planners and Decision Makers; WaterAid: London, UK, 2018; p. 56. Available online: https://washmatters.wateraid.org/publications/female-friendly-public-and-community-toilets-a-guide-for-planners-and-decision-makers (accessed on 17 May 2022).
- Mulatya, D.M.; Ochieng, C. Disease burden and risk factors of diarrhoea in children under five years: Evidence from Kenya’s demographic health survey 2014. Int. J. Infect. Dis. 2020, 93, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Manesh, A.O.; Sheldon, T.A.; Pickett, K.E.; Carr-Hill, R. Accuracy of child morbidity data in demographic and health surveys. Int. J. Epidemiol. 2008, 37, 194–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawlings, J.O.; Pantula, S.G.; Dickey, D.A. Applied Regression Analysis: A Research Tool, 2nd ed.; Springer Texts in Statistics; Springer: New York, NY, USA, 1998; ISBN 978-0-387-98454-4. [Google Scholar]
- Nilima, N.; Kamath, A.; Shetty, K.; Unnikrishnan, B.; Kaushik, S.; Rai, S.N. Prevalence, patterns, and predictors of diarrhea: A spatial-temporal comprehensive evaluation in India. BMC Public Health 2018, 18, 1288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rey, S.J.; Arribas-Bel, D.; Wolf, L.J. Geographic Data Science with Python [Open Book]. Available online: https://geographicdata.science/book/intro.html# (accessed on 14 June 2022).
- Anselin, L. Spatial regression. In The SAGE Handbook of Spatial Analysis; Fotheringham, A.S., Rogerson, P., Eds.; SAGE Publications: Los Angeles, CA, USA; London, UK, 2009; pp. 255–275. ISBN 978-1-4129-1082-8. [Google Scholar]
- Wurm, M.; Taubenböck, H. Detecting social groups from space–assessment of remote sensing-based mapped morphological slums using income data. Remote Sens. Lett. 2018, 9, 41–50. [Google Scholar] [CrossRef]
- Wang, J.; Georganos, S.; Kuffer, M.; Abascal, A.; Vanhuysse, S. On the knowledge gain of urban morphology from space. Comput. Environ. Urban Syst. 2022, 95, 101831. [Google Scholar] [CrossRef]
- Pickering, A.J.; Null, C.; Winch, P.J.; Mangwadu, G.; Arnold, B.F.; Prendergast, A.J.; Njenga, S.M.; Rahman, M.; Ntozini, R.; Benjamin-Chung, J.; et al. The WASH Benefits and SHINE trials: Interpretation of WASH intervention effects on linear growth and diarrhoea. Lancet Glob. Health 2019, 7, e1139–e1146. [Google Scholar] [CrossRef] [Green Version]
- Njoh, A.J. Urbanization and development in sub-Saharan Africa. Cities 2003, 20, 167–174. [Google Scholar] [CrossRef]
- Rydin, Y.; Bleahu, A.; Davies, M.; Dávila, J.D.; Friel, S.; De Grandis, G.; Groce, N.; Hallal, P.C.; Hamilton, I.; Howden-Chapman, P.; et al. Shaping cities for health: Complexity and the planning of urban environments in the 21st century. Lancet 2012, 379, 2079–2108. [Google Scholar] [CrossRef] [Green Version]
- Nana, N.; Kouakou, A.B.; Kougouindiga, A. Chroniques D’investissements dans le Logement en Côte d’Ivoire; Centre for Affordable Housing Finance in Africa: Johannesburg, South Africa, 2019; p. 34. Available online: https://housingfinanceafrica.org/fr/documents/chroniques-dinvestissement-du-logement-cas-de-la-cote-divoire/ (accessed on 13 May 2022).
- Morgenstern, H. Ecologic studies in epidemiology: Concepts, principles, and methods. Annu. Rev. Public Health 1995, 16, 61–81. [Google Scholar] [CrossRef]
- Møller, A.P.; Jennions, M.D. How much variance can be explained by ecologists and evolutionary biologists? Oecologia 2002, 132, 492–500. [Google Scholar] [CrossRef]
- Mari, L.; Bertuzzo, E.; Righetto, L.; Casagrandi, R.; Gatto, M.; Rodriguez-Iturbe, I.; Rinaldo, A. Modelling cholera epidemics: The role of waterways, human mobility and sanitation. J. R. Soc. Interface 2012, 9, 376–388. [Google Scholar] [CrossRef] [PubMed]
- G’Sell, M.G.; Wager, S.; Chouldechova, A.; Tibshirani, R. Sequential selection procedures and false discovery rate control. J. R. Stat. Soc. 2016, 78, 423–444. [Google Scholar] [CrossRef] [Green Version]




| Data Layer | Source | Description | Available Years | Spatial Resolution | Type |
|---|---|---|---|---|---|
| Geolocation of DHS cluster | DHS | Cluster location with a geographic blur of 2 to 5 km | 1998/1999 2011/2012 | 2 to 5 km | Vector (shp 1) |
| Cases of diarrhoea | DHS | Cases of diarrhoea (under-5), geocoded to cluster location | 1998/1999 2011/2012 | 2 to 5 km | Vector (table) |
| Access to water and sanitation | DHS | Type of facility used by household, geocoded to cluster location | 1998/1999 2011/2012 | 2 to 5 km | Vector (table) |
| Education attainment | DHS | Education attainment of women (15–49 years), geocoded to cluster location | 1998/1999 2011/2012 | 2 to 5 km | Vector (table) |
| Climatic conditions | Terra-climate | Accumulated precipitation and mean temperature | 1958–2020 | 1/24th degr. (~4 km) | Raster |
| Illumination (night lights) | NASA | Intensity of night illumination | 2012 & 2016 | 500 m | Raster |
| Land use | ESA Land Cover CCI | Discrete categories of land cover | 1992–2019 | 300 m | Raster |
| Population density | WorldPop | Estimated demographic densities (WorldPop’s model) | 2000–2020 | 100 m | Raster |
| Roads | OpenStreetMap | Surveyed roads and pathways | 2019 | 5 to 20 m | Vector (shp 1) |
| Variable | Role in Analysis | Aggregation Operation |
|---|---|---|
| Prevalence of diarrhoea, under −5 | Dependent variable | |
| % access to basic 1 water | Control variable | |
| % access to basic 1 sanitation | Control variable | |
| % women 2 with no education | Control variable | |
| Edge of land cover patches 3 | Independent variables | Total length (m) of edges of given land cover |
| Shape index of land cover patches 3 | Independent variables | |
| Proportion of land cover patches 3 | Independent variables | |
| % dense urban areas | Independent variable | |
| % precarious urban areas | Independent variable | |
| Km of roads per urban area | Independent variable |
| Included Features | Variance Inflation Factor | Unweighted OLS R2 = 0.06/AIC = −50.4 JB 2: 12.020 (p = 0.003) BP 3: 4.880 (p = 0.300) | Weighted OLS R2 = 0.129/AIC = 21.75 JB 2: 10.676 (p = 0.005) BP 3: 2.881 (p = 0.578) | Spatial Lag Pseudo R2 = 0.09/AIC = −56.3 JB 2: 11.407 (p = 0.003) BP 3: 5.807 (p = 0.214) | Spatial Error Pseudo R2 = 0.059/AIC = −58.2 JB 2: 11.859 (p = 0.003) BP 3: 4.693 (p = 0.320) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Coef. | SE | Prob. | Coef. | SE | Prob. | Coef. | SE | Prob. | Coef. | SE | Prob. | ||
| Constant | - | 0.426 | 0.070 | 0.000 | 0.460 | 0.066 | 0.000 | 0.297 | 0.076 | 0.000 | 0.366 | 0.073 | 0.000 |
| % basic water | 1.372 | 0.001 | 0.063 | 0.986 | 0.014 | 0.062 | 0.820 | 0.032 | 0.061 | 0.606 | 0.049 | 0.064 | 0.439 |
| % basic sanitation | 1.810 | −0.186 | 0.069 | 0.007 | −0.257 | 0.069 | 0.000 | −0.181 | 0.067 | 0.007 | −0.166 | 0.068 | 0.015 |
| % women with no ed. | 1.674 | −0.141 | 0.075 | 0.061 | −0.221 | 0.076 | 0.004 | −0.123 | 0.073 | 0.092 | −0.108 | 0.074 | 0.148 |
| Dense, prec. areas 1 | 1.074 | 0.257 | 0.081 | 0.002 | 0.291 | 0.062 | 0.000 | 0.227 | 0.081 | 0.005 | 0.275 | 0.094 | 0.004 |
| Included Features | Variance Inflation Factor | Unweighted OLS R2 = 0.141/AIC = −14.04 JB 2: 4.316 (p = 0.116) BP 3: 4.444 (p = 0.349) | Weighted OLS R2 = 0.196/AIC = 23.56 JB 2: 6.395 (p = 0.041) BP 3: 7.101 (p = 0.131) | Spatial Lag Pseudo R2 = 0.141/AIC = −12.05 JB 2: 4.364 (p = 0.113) BP 3: 4.391 (p = 0.356) | Spatial Error Pseudo R2 = 0.141/AIC = −14.09 JB 2: 4.285 (p = 0.117) BP 3: 4.424 (p = 0.352) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Coef. | SE | Prob. | Coef. | SE | Prob. | Coef. | SE | Prob. | Coef. | SE | Prob. | ||
| Constant | - | 0.282 | 0.137 | 0.042 | 0.325 | 0.157 | 0.040 | 0.290 | 0.143 | 0.043 | 0.275 | 0.134 | 0.041 |
| % basic water | 1.172 | 0.082 | 0.118 | 0.488 | 0.112 | 0.136 | 0.412 | 0.081 | 0.115 | 0.483 | 0.089 | 0.115 | 0.439 |
| % basic sanitation | 1.769 | −0.168 | 0.107 | 0.119 | −0.252 | 0.107 | 0.021 | −0.167 | 0.105 | 0.111 | −0.168 | 0.105 | 0.110 |
| % women with no ed. | 1.810 | −0.013 | 0.127 | 0.917 | −0.088 | 0.136 | 0.520 | −0.012 | 0.124 | 0.925 | −0.012 | 0.124 | 0.922 |
| Dense, prec. areas 1 | 1.029 | 0.315 | 0.090 | 0.001 | 0.316 | 0.079 | 0.000 | 0.318 | 0.093 | 0.001 | 0.318 | 0.090 | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pessoa Colombo, V.; Chenal, J.; Koné, B.; Bosch, M.; Utzinger, J. Using Open-Access Data to Explore Relations between Urban Landscapes and Diarrhoeal Diseases in Côte d’Ivoire. Int. J. Environ. Res. Public Health 2022, 19, 7677. https://doi.org/10.3390/ijerph19137677
Pessoa Colombo V, Chenal J, Koné B, Bosch M, Utzinger J. Using Open-Access Data to Explore Relations between Urban Landscapes and Diarrhoeal Diseases in Côte d’Ivoire. International Journal of Environmental Research and Public Health. 2022; 19(13):7677. https://doi.org/10.3390/ijerph19137677
Chicago/Turabian StylePessoa Colombo, Vitor, Jérôme Chenal, Brama Koné, Martí Bosch, and Jürg Utzinger. 2022. "Using Open-Access Data to Explore Relations between Urban Landscapes and Diarrhoeal Diseases in Côte d’Ivoire" International Journal of Environmental Research and Public Health 19, no. 13: 7677. https://doi.org/10.3390/ijerph19137677