
Study on Spatial Distribution Equilibrium of Elderly Care Facilities in Downtown Shanghai


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Background
1.2. Framework
2. Research Site and Data Acquisition
2.1. Research Site
2.2. Data Acquisition
2.2.1. Acquisition of Community Location and Community Life Circle Data
2.2.2. Acquisition of Elderly Care Service Facilities and Service Circle Data
3. Method
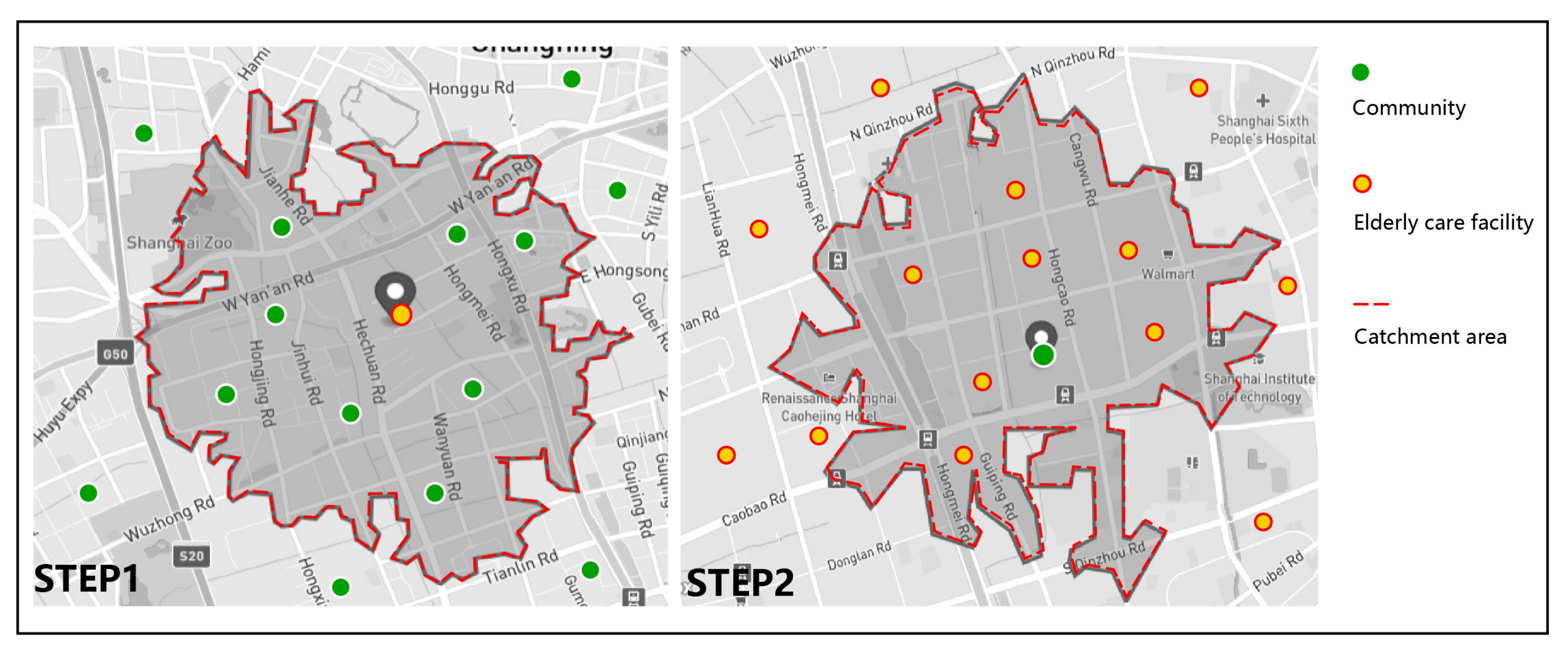
3.1. Calculating the Spatial Accessibility of Elderly Care Facilities
3.2. Calculation on Three Administrative Levels of Spatial Accessibility
3.3. Analysis on Spatial Distribution Equilibrium
4. Results and Discussion
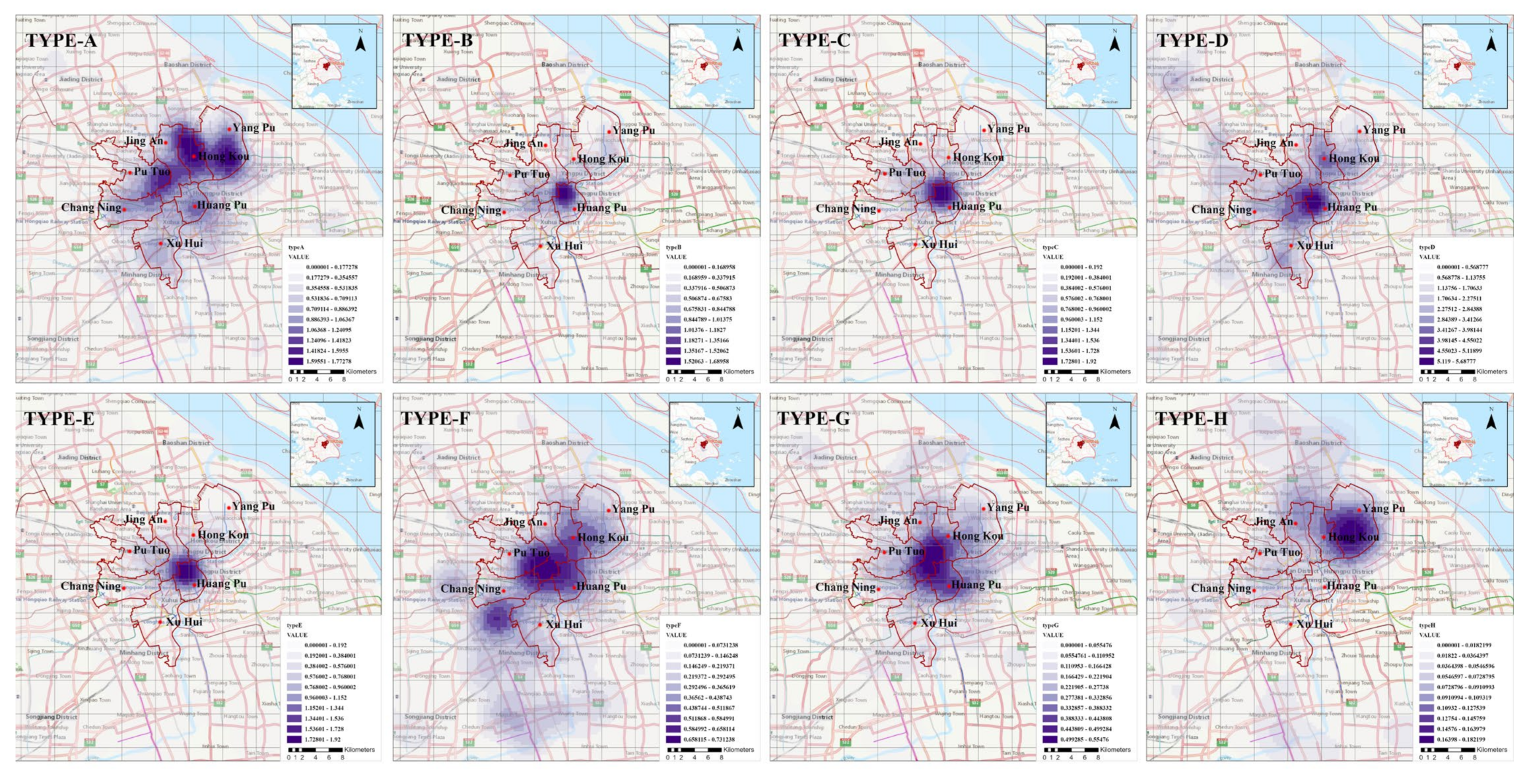
4.1. The Results of Elderly Care Facilities Density
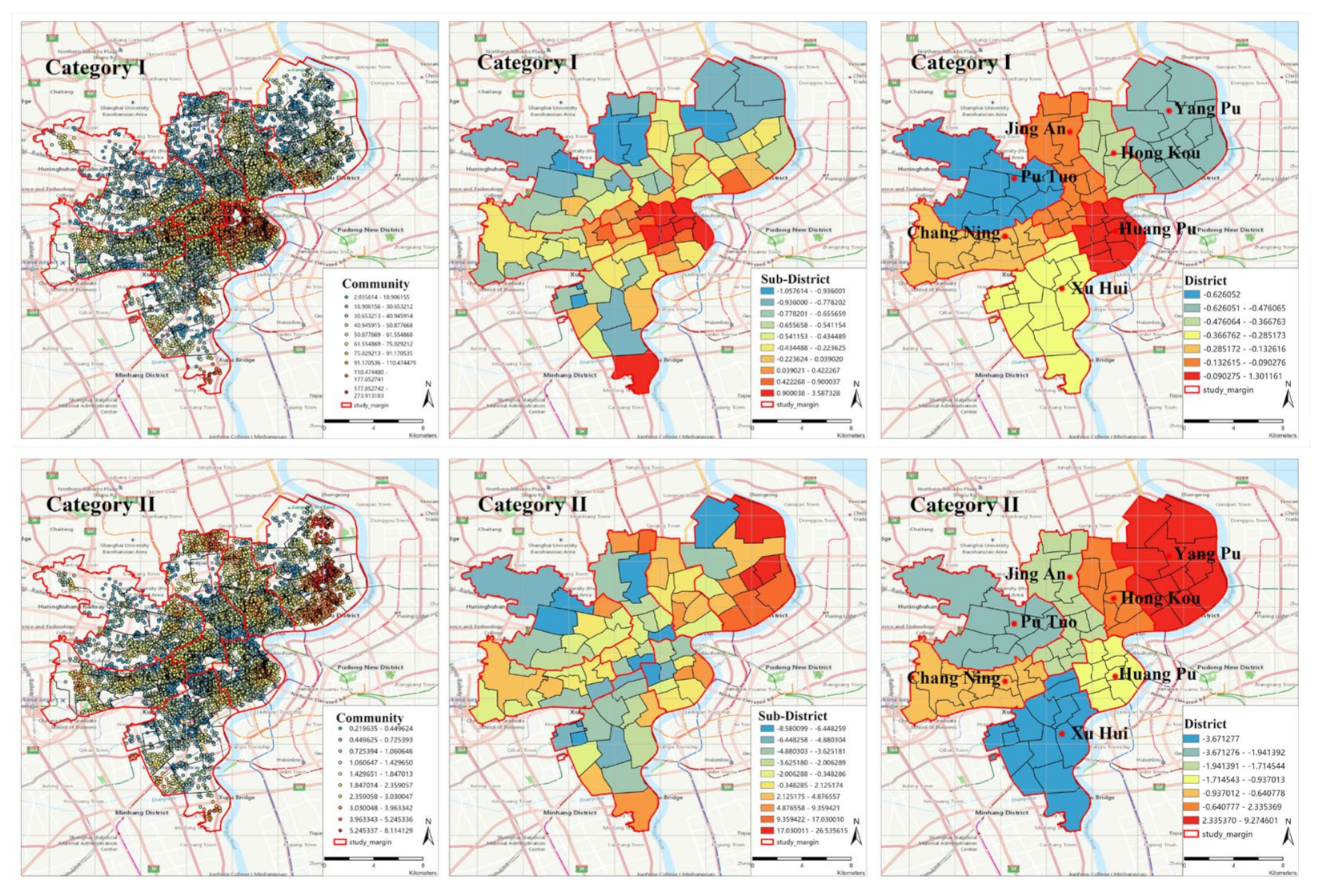
4.2. The Results of Statistical Analysis on Administrative Regions
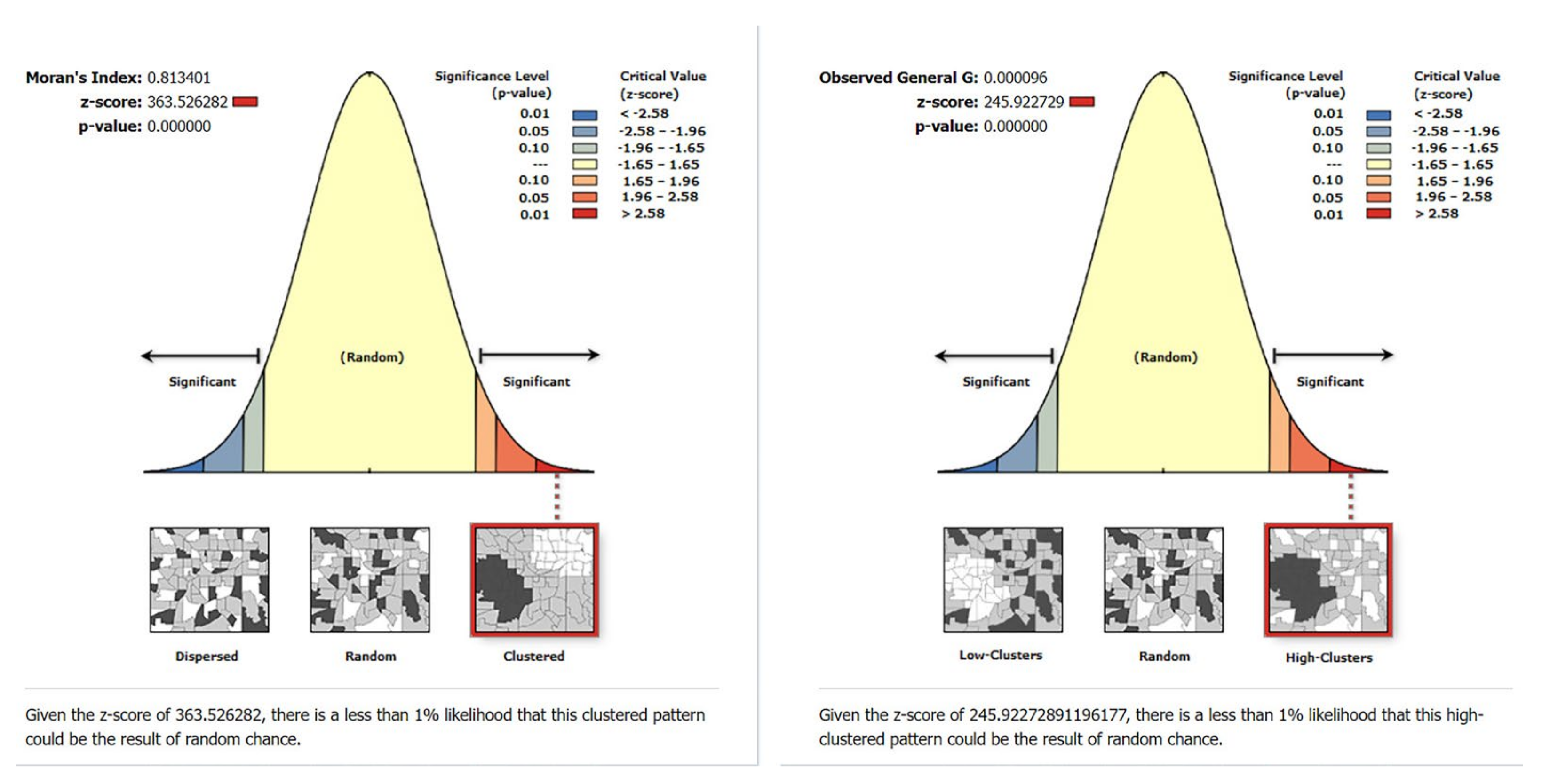
4.3. The Results of Global Autocorrelation Analysis
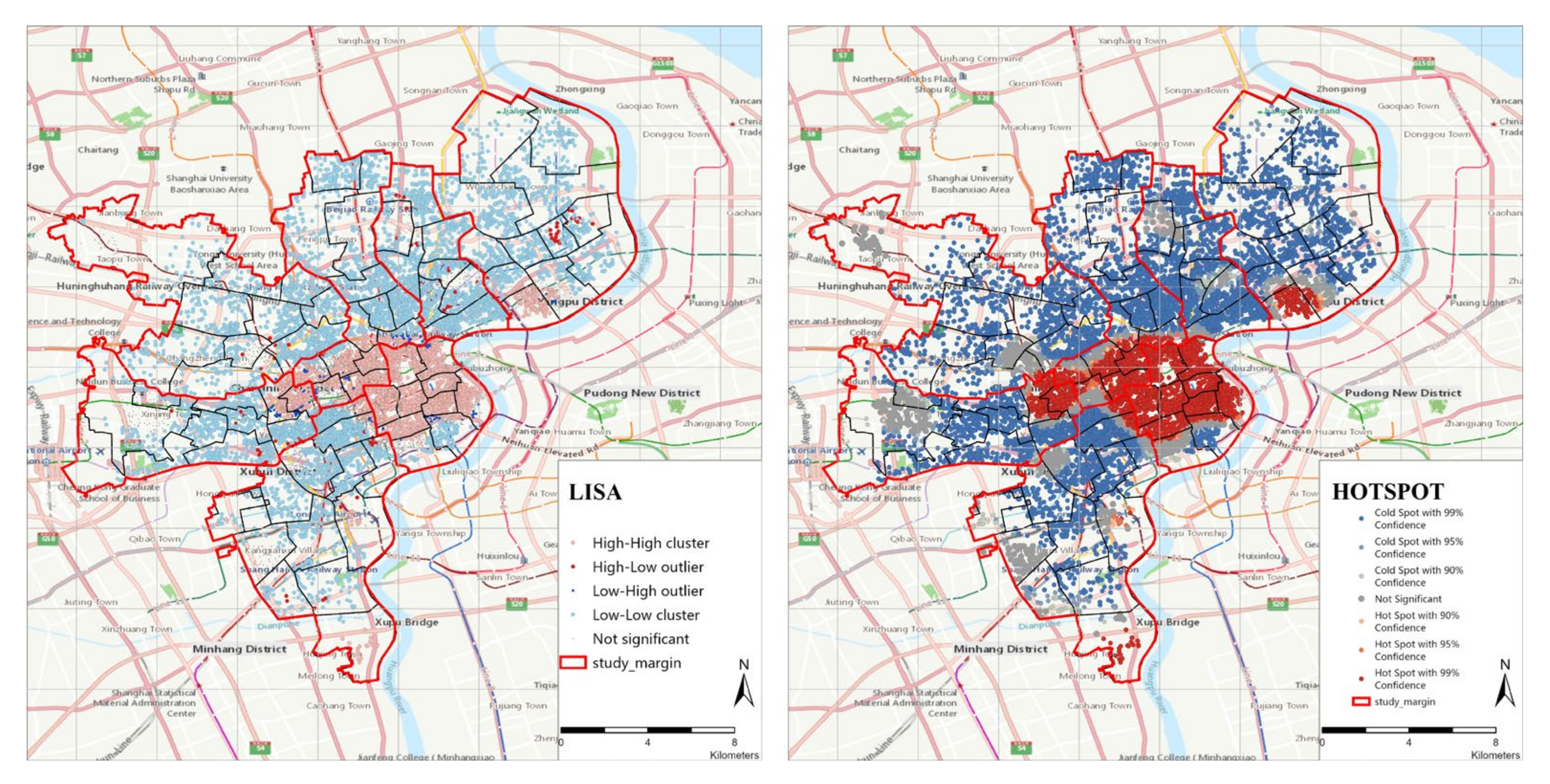
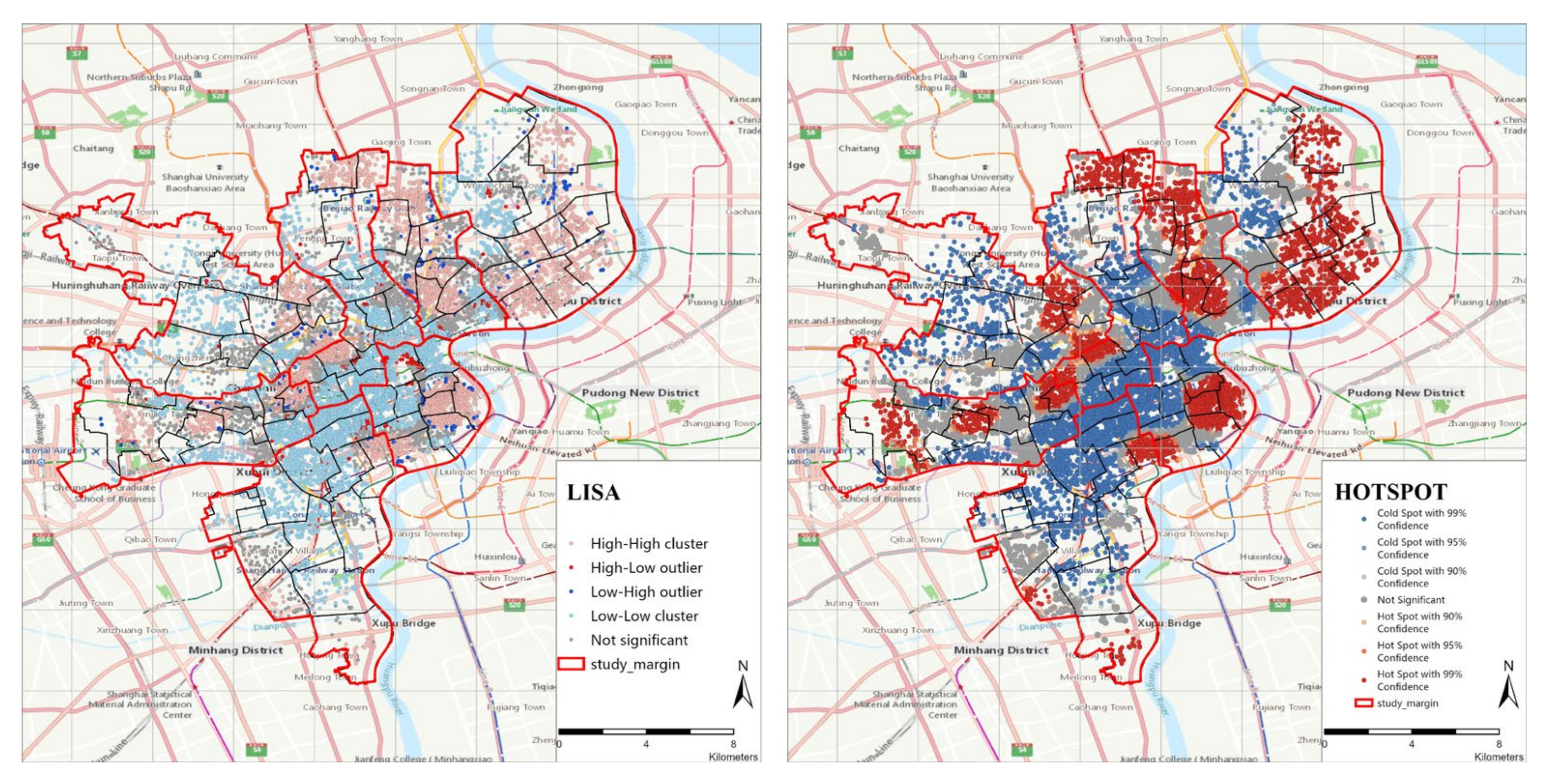
4.4. The Results of Local Autocorrelation Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lu, J.; Liu, Q. Four decades of studies on population aging in China. China Popul. Dev. Stud. 2019, 3, 24–36. [Google Scholar] [CrossRef] [Green Version]
- National Bureau of Statistics of China. Seventh National Census Bulletin (No.5). Available online: http://www.gov.cn/xinwen/2021-05/11/content_5605787.htm (accessed on 6 August 2021).
- Yang, H. The choice of pension and retirement systems when post-1960s baby boomers start to retire in China. China Financ. Econ. Rev. 2016, 4, 481. [Google Scholar] [CrossRef] [Green Version]
- Poston, D.L.; Glover, K.S. Too many males: Marriage market implications of gender imbalances in China. Genus 2005, 61, 119–140. Available online: http://www.jstor.org/stable/29788854 (accessed on 10 May 2022).
- Zepinghongguan, A Minimalist Interpretation of the 2022 Government Work Report. Available online: http://www.china-cer.com.cn/guwen/2022031417263.html (accessed on 14 March 2022).
- Zhan, H.J. Chinese caregiving burden and the future burden of elder care in life-course perspective. Int. J. Aging Hum. Dev. 2002, 54, 267–290. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y. Definition of birth peak and analysis of some problems about the first and second birth peaks in China. Popul. Econ. 1994, 2, 11–19. Available online: http://www.cqvip.com/qk/95683x/199402/1003318274.html (accessed on 10 May 2022).
- OECD. “Elderly population” (indicator). 2022. Available online: https://www.oecd-ilibrary.org/social-issues-migration-health/elderly-population/indicator/english_8d805ea1-en (accessed on 26 June 2022).
- Fang, E.F.; Scheibye-Knudsen, M.; Jahn, H.J.; Li, J.; Ling, L.; Guo, H.; Zhu, X.; Preedy, V.; Lu, H.; Bohr, V.A.; et al. A research agenda for aging in China in the 21st century. Ageing Res. Rev. 2015, 24, 197–205. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Li, Y.; Zhu, X.; Ma, L. Medical and Old-Age Care Integration Model and Implementation of the Integrated Care of Older People (ICOPE) in China: Opportunities and Challenges. J. Nutr. Health Aging 2021, 25, 720–723. [Google Scholar] [CrossRef]
- Hu, B. Projecting future demand for informal care among older people in China: The road towards a sustainable long-term care system. Health Econ. Policy Law 2018, 14, 61–81. [Google Scholar] [CrossRef]
- Ma, Y.; Siu, K.W.M.; Zou, G. Contradictory and consistent views on designing an inclusive community-based centre for older people: A mixed-methods study of different age groups in China. Ageing Soc. 2019, 40, 1867–1886. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Civil Affairs of the People’s Republic of China. The Historical Context of the 70 Year Development of Pension ser-vices in New China. Available online: Mzzt.mca.gov.cn/article/zt_zl70n/zhbd/201909/20190900020005.shtml (accessed on 10 May 2022).
- Zhang, X. The Application of Spatial Information Technology in the Rural Elderly Care Model under the Strategy of “Building a Country with a Strong Transportation Network” in China. Transp. Res. Procedia 2022, 61, 481–486. [Google Scholar] [CrossRef]
- Cheng, Y.; Gao, S.Y.; Li, S.; Zhang, Y.C.; Rosenberg, M. Understanding the spatial disparities and vulnerability of population aging in China. Asia Pac. Policy Stud. 2019, 6, 73–89. [Google Scholar] [CrossRef]
- Cheng, L.; Yang, M.; De Vos, J.; Witlox, F. Examining geographical accessibility to multi-tier hospital care services for the elderly: A focus on spatial equity. J. Transp. Health 2020, 19, 100926. [Google Scholar] [CrossRef]
- Liu, S.; Wang, Y.; Zhou, D.; Kang, Y. Two-Step Floating Catchment Area Model-Based Evaluation of Community Care Facilities’ Spatial Accessibility in Xi’an, China. Int. J. Environ. Res. Public Health 2020, 17, 5086. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Wu, J.; Guo, P.; Yao, S. Evaluating service accessibility of residential care facilities in Shanghai for fulfilling basic needs. J. East China Norm. Univ. (Nat. Sci.) 2020, 3, 119–128. [Google Scholar] [CrossRef]
- Rantakokko, M.; Mänty, M.; Rantanen, T. Mobility Decline in Old Age. Exerc. Sport Sci. Rev. 2013, 41, 19–25. [Google Scholar] [CrossRef]
- Luiu, C.; Tight, M. Travel difficulties and barriers during later life: Evidence from the National Travel Survey in England. J. Transp. Geogr. 2021, 91, 102973. [Google Scholar] [CrossRef]
- Demura, S.; Sato, S. Relationships between Depression, Lifestyle and Quality of Life in the Community Dwelling Elderly: A Comparison between Gender and Age Groups. J. Physiol. Anthr. Appl. Hum. Sci. 2003, 22, 159–166. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.-W.; Kumar, P.; Cao, S.-J. Implementation of green infrastructure for improving the building environment of elderly care centres. J. Build. Eng. 2022, 54, 104682. [Google Scholar] [CrossRef]
- Youn, H.M.; Lee, D.W.; Park, E.-C. Association between community outpatient clinic care accessibility and the uptake of diabetic retinopathy screening: A multi-level analysis. Prim. Care Diabetes 2020, 14, 616–621. [Google Scholar] [CrossRef]
- Wong, R.; Szeto, W.; Yang, L.; Li, Y.; Wong, S.C. Public transport policy measures for improving elderly mobility. Transp. Policy 2018, 63, 73–79. [Google Scholar] [CrossRef] [Green Version]
- Ahuja, R.; Tiwari, G. Evolving term “accessibility” in spatial systems: Contextual evaluation of indicators. Transp. Policy 2021, 113, 4–11. [Google Scholar] [CrossRef]
- Jin, T.; Cheng, L.; Wang, K.; Cao, J.; Huang, H.; Witlox, F. Examining equity in accessibility to multi-tier healthcare services across different income households using estimated travel time. Transp. Policy 2022, 121, 1–13. [Google Scholar] [CrossRef]
- Huang, Y.; Meyer, P.; Jin, L. Neighborhood socioeconomic characteristics, healthcare spatial access, and emergency department visits for ambulatory care sensitive conditions for elderly. Prev. Med. Rep. 2018, 12, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhou, K.; Wang, Z. Spatial distribution of community pension facilities from the perspective of health equity: A case study of the central city of shanghai. Hum. Geogr. 2021, 36, 48–55. [Google Scholar] [CrossRef]
- Zhai, S.; He, X.; Kong Yg Luo, J.; Song, G. Spatial accessibility analysis of public facilities based on optimal supply and demand allocation. Acta Geogr. Sin. 2022, 77, 1028–1038. [Google Scholar]
- Hsu, Y.-Y.; Hawken, S.; Sepasgozar, S.; Lin, Z.-H. Beyond the Backyard: GIS Analysis of Public Green Space Accessibility in Australian Metropolitan Areas. Sustainability 2022, 14, 4694. [Google Scholar] [CrossRef]
- Tanimoto, R.; Hanibuchi, T. Associations between the sense of accessibility, accessibility to specific destinations, and personal factors: A cross-sectional study in Sendai, Japan. Transp. Res. Interdiscip. Perspect. 2021, 12, 100491. [Google Scholar] [CrossRef]
- Serrano-Jiménez, A.; Blandón-González, B.; Barrios-Padura, A. Towards a built environment without physical barriers: An accessibility assessment procedure and action protocol for social housing occupied by the elderly. Sustain. Cities Soc. 2021, 76, 103456. [Google Scholar] [CrossRef]
- Cho, H.; Choi, J.; No, W.; Oh, M.; Kim, Y. Accessibility of welfare facilities for elderly people in Daejeon, South Korea considering public transportation accessibility. Transp. Res. Interdiscip. Perspect. 2021, 12, 100514. [Google Scholar] [CrossRef]
- Kotavaara, O.; Nivala, A.; Lankila, T.; Huotari, T.; Delmelle, E.; Antikainen, H. Geographical accessibility to primary health care in Finland–Grid-based multimodal assessment. Appl. Geogr. 2021, 136, 102583. [Google Scholar] [CrossRef]
- Reddy, B.P.; O’Neill, S.; O’Neill, C. Explaining spatial accessibility to high-quality nursing home care in the US using machine learning. Spat. Spatio-Temporal Epidemiol. 2022, 41, 100503. [Google Scholar] [CrossRef]
- Zou, T.; Aemmer, Z.; MacKenzie, D.; Laberteaux, K. A framework for estimating commute accessibility and adoption of ridehailing services under functional improvements from vehicle automation. J. Transp. Geogr. 2022, 102, 103357. [Google Scholar] [CrossRef]
- Rathore, M.M.; Ahmad, A.; Paul, A.; Rho, S. Urban planning and building smart cities based on the Internet of Things using Big Data analytics. Comput. Netw. 2016, 101, 63–80. [Google Scholar] [CrossRef]
- Wang, F.; He, P.; Yuan, C.; Wang, S. Isolated or integrated? Evaluation of ageing-friendly communities in Old Beijing City based on accessibility, social inclusion and equity. Indoor Built Environ. 2020, 29, 465–479. [Google Scholar] [CrossRef]
- Chen, W.; Cheng, L.; Chen, X.; Chen, J.; Cao, M. Measuring accessibility to health care services for older bus passengers: A finer spatial resolution. J. Transport Geogr. 2021, 93, 103068. [Google Scholar] [CrossRef]
- Linggui, L.; Jing, H.; Dian, Z. Research on the convenient life of the elderly in urban based on POI digital technique: A case study of Xi’an City. In Proceedings of the 2020 International Conference on Innovation Design and Digital Technology (ICIDDT), Zhenjing, China, 5–6 December 2020; pp. 466–470. [Google Scholar] [CrossRef]
- He, H.; Lin, X.; Yang, Y.; Lu, Y. Association of street greenery and physical activity in older adults: A novel study using pedestrian-centered photographs. Urban. For. Urban. Green. 2020, 55, 126789. [Google Scholar] [CrossRef]
- Lv, M.; Wang, N.; Yao, S.; Wu, J.; Fang, L. Towards Healthy Aging: Influence of the Built Environment on Elderly Pedestrian Safety at the Micro-Level. Int. J. Environ. Res. Public Health 2021, 18, 9534. [Google Scholar] [CrossRef]
- Yang, L.; Ao, Y.; Ke, J.; Lu, Y.; Liang, Y. To walk or not to walk? Examining non-linear effects of streetscape greenery on walking propensity of older adults. J. Transp. Geogr. 2021, 94, 103099. [Google Scholar] [CrossRef]
- Wang, R.; Lu, Y.; Zhang, J.; Liu, P.; Yao, Y.; Liu, Y. The relationship between visual enclosure for neighbourhood street walkability and elders’ mental health in China: Using street view images. J. Transp. Health 2019, 13, 90–102. [Google Scholar] [CrossRef]
- Liu, S.; Yamamoto, T.; Yao, E.; Nakamura, T. Examining public transport usage by older adults with smart card data: A longitudinal study in Japan. J. Transp. Geogr. 2021, 93, 103046. [Google Scholar] [CrossRef]
- Guo, S.; Song, C.; Pei, T.; Liu, Y.; Ma, T.; Du, Y.; Chen, J.; Fan, Z.; Tang, X.; Peng, Y.; et al. Accessibility to urban parks for elderly residents: Perspectives from mobile phone data. Landsc. Urban. Plan. 2019, 191, 103642. [Google Scholar] [CrossRef]
- Shi, Z. Spatial Big Data Analytics of Spatiotemporal Mobility Characteristics of the Elderly. 2020. Available online: https://theses.lib.polyu.edu.hk/bitstream/200/10721/3/5124.pdf (accessed on 20 April 2022).
- Tao, Z.; Cheng, Y.; Dai, T. Evaluation of spatial accessibility of elderly care facilities in Beijing. Prog. Geogr. 2014, 33, 616–624. [Google Scholar] [CrossRef]
- Van Heerden, Q.; Karsten, C.; Holloway, J.; Petzer, E.; Burger, P.; Mans, G. Accessibility, affordability, and equity in long-term spatial planning: Perspectives from a developing country. Transport Policy. 2022, 120, 104–119. [Google Scholar] [CrossRef]
- Luo, W.; Wang, F. Measures of Spatial Accessibility to Health Care in a GIS Environment: Synthesis and a Case Study in the Chicago Region. Environ. Plan. B Plan. Des. 2003, 30, 865–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.; Meyer, P.; Jin, L. Spatial access to health care and elderly ambulatory care sensitive hospitalizations. Public Health 2019, 169, 76–83. [Google Scholar] [CrossRef]
- He, J.; Zhou, D.; Xu, Y.; Dai, J. The study on spatial accessibility measurement of pension facilities in urban community. Archit. J. 2018, S1, 18–22. Available online: http://www.cqvip.com/qk/94827x/2018s1/74908866504849568349484852.html (accessed on 20 April 2022).
- Zhang, F.; Li, D.; Ahrentzen, S.; Zhang, J. Assessing spatial disparities of accessibility to community-based service resources for Chinese older adults based on travel behavior: A city-wide study of Nanjing, China. Habitat Int. 2019, 88, 101984. [Google Scholar] [CrossRef]
- Zhang, F.; Li, D. Multiple Linear Regression-Structural Equation Modeling Based Development of the Integrated Model of Perceived Neighborhood Environment and Quality of Life of Community-Dwelling Older Adults: A Cross-Sectional Study in Nanjing, China. Int. J. Environ. Res. Public Health 2019, 16, 4933. [Google Scholar] [CrossRef] [Green Version]
- Han, F.; Luo, R. Matching of Supply and Demand for Community Service-Oriented Home Care Facilities Based on Accessibility Measurement: A Case Study of Nanjing. Econ. Geogr. 2020, 40, 91–101. [Google Scholar] [CrossRef]
- Li, H.P.; Liang, Z.H. Research on spatial equilibrium of urban community elderly care facilities and its configuration. J. Geo-Inf. Sci. 2021, 23, 467–478. [Google Scholar] [CrossRef]
- Cheng, L.; Caset, F.; De Vos, J.; Derudder, B.; Witlox, F. Investigating walking accessibility to recreational amenities for elderly people in Nanjing, China. Transp. Res. Part D Transp. Environ. 2019, 76, 85–99. [Google Scholar] [CrossRef]
- Luo, W.; Qi, Y. An enhanced two-step floating catchment area (E2SFCA) method for measuring spatial accessibility to primary care physicians. Health Place 2009, 15, 1100–1107. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.; Huang, W. Evaluation of spatial accessibility of elderly care facilities in Shanghai based on Gauss two-step floating catchment area method. J. Fudan Univ. (Nat. Sci.) 2020, 59, 129–136. [Google Scholar] [CrossRef]
- Xu, X.; Zhao, Y. Spatial Distribution Pattern and Accessibility Assessment of Pension Service Facilities in Nanjing: Two-step Floating Catchment Area Method Based on Time Cost. Mod. Urban Res. 2017, 2, 2–11. Available online: https://www.cnki.com.cn/Article/CJFDTotal-XDCS201702002.htm (accessed on 20 April 2022).
- Shanghai Municipal Bureau of Planning and Natural Resources, Shanghai Planning Guidance of 15-Minute Community-Life Circle. Available online: https://hd.ghzyj.sh.gov.cn/zcfg/ghss/201609/P020160902620858362165.pdf (accessed on 20 April 2022).
- Liu, T.; Chai, Y. Daily life circle reconstruction: A scheme for sustainable development in urban China. Habitat Int. 2015, 50, 250–260. [Google Scholar] [CrossRef]
- Shanghai Municipal People’s Government. Shanghai Master Plan 2017–2035. Available online: https://www.shanghai.gov.cn/newshanghai/xxgkfj/2035002.pdf (accessed on 20 April 2022).
- Shanghai Municipal Bureau of Planning and Natural Resources. Layout of Shanghai Elderly Care Facilities (2021–2035). Available online: https://ghzyj.sh.gov.cn/cmsres/9f/9f44c4d8e21d4fde9066d3ecaeebf690/1dcd32946ed78cd11ee4a8194e859089.pdf (accessed on 20 April 2022).
- Yue, W.; Chen, Y.; Zhang, Q.; Liu, Y. Spatial Explicit Assessment of Urban Vitality Using Multi-Source Data: A Case of Shanghai, China. Sustainability 2019, 11, 638. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Chen, H.; Yan, W. Exploring Spatial Distribution of Urban Park Service Areas in Shanghai Based on Travel Time Estimation: A Method Combining Multi-Source Data. ISPRS Int. J. Geo-Inf. 2021, 10, 608. [Google Scholar] [CrossRef]
- Shanghai Municipal Bureau of Statistics. Shanghai Statistical Yearbook. 2021. Available online: https://tjj.sh.gov.cn/tjnj/nj21.htm?d1=2021tjnj/C0207.htm (accessed on 20 April 2022).
- Shanghai Municipal Bureau of Statistics. Shanghai Statistical Yearbook. 2021. Available online: https://tjj.sh.gov.cn/tjnj/nj21.htm?d1=2021tjnj/C0201.htm (accessed on 20 April 2022).
- Yang, D.-H.; Goerge, R.; Mullner, R. Comparing GIS-Based Methods of Measuring Spatial Accessibility to Health Services. J. Med. Syst. 2006, 30, 23–32. [Google Scholar] [CrossRef]
- Li, Z.; Fan, Z.; Song, Y.; Chai, Y. Assessing equity in park accessibility using a travel behavior-based G2SFCA method in Nanjing, China. J. Transp. Geogr. 2021, 96, 103179. [Google Scholar] [CrossRef]
- Chen, B.Y.; Cheng, X.-P.; Kwan, M.-P.; Schwanen, T. Evaluating spatial accessibility to healthcare services under travel time uncertainty: A reliability-based floating catchment area approach. J. Transp. Geogr. 2020, 87, 102794. [Google Scholar] [CrossRef]
- Radke, J.; Mu, L. Spatial Decompositions, Modeling and Mapping Service Regions to Predict Access to Social Programs. Ann. GIS 2000, 6, 105–112. [Google Scholar] [CrossRef]
- Tao, Z.; Cheng, Y.; Dai, T.; Li, X. Sensitivity Analysis of Parameters in Measuring Spatial Accessibility to Public Service Facilities. Mod. Urban Res. 2017, 3, 30–35. [Google Scholar] [CrossRef]
- McGrail, M.R.; Humphreys, J.S. Measuring spatial accessibility to primary care in rural areas: Improving the effectiveness of the two-step floating catchment area method. Appl. Geogr. 2009, 29, 533–541. [Google Scholar] [CrossRef]
- Luo, W.; Whippo, T. Variable catchment sizes for the two-step floating catchment area (2SFCA) method. Health Place 2012, 18, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Mao, L.; Nekorchuk, D. Measuring spatial accessibility to healthcare for populations with multiple transportation modes. Health Place 2013, 24, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Cheng, Y.; Wei, W.; Zhao, B. Evaluating Spatial Disparity of Access to Public Parks in Gated and Open Communities with an Improved G2SFCA Model. Sustainability 2019, 11, 5910. [Google Scholar] [CrossRef] [Green Version]
- Polzin, P.; Borges, J.; Coelho, A. An Extended Kernel Density Two-Step Floating Catchment Area Method to Analyze Access to Health Care. Environ. Plan. B Plan. Des. 2014, 41, 717–735. [Google Scholar] [CrossRef]
- Dai, D. Racial/ethnic and socioeconomic disparities in urban green space accessibility: Where to intervene? Landsc. Urban. Plan. 2011, 102, 234–244. [Google Scholar] [CrossRef]
- Lam, N.S.-N. Spatial Interpolation Methods: A Review. Am. Cartogr. 1983, 10, 129–150. [Google Scholar] [CrossRef]
- Zhan, D.; Zhang, W.; Dang, Y.; Yu, X.; Wu, Q. Spatial Clustering Analysis of Public Service Facilities in Beijing. Econ. Geogr. 2018, 38, 76–82. [Google Scholar] [CrossRef]
- Kang, Y.X.; Gui, Z.P.; Ding, J.C.; Wu, J.H.; Wu, H.Y. Parallel Ripley’s K function based on Hilbert spatial partitioning and Geohash indexing. J. Geo-Inf. Sci. 2022, 24, 74–86. [Google Scholar] [CrossRef]
- Song, W.; Wang, C.; Chen, W.; Zhang, X.; Li, H.; Li, J. Unlocking the spatial heterogeneous relationship between Per Capita GDP and nearby air quality using bivariate local indicator of spatial association. Resour. Conserv. Recycl. 2020, 160, 104880. [Google Scholar] [CrossRef]
- Guo, L.; Du, S.; Haining, R.; Zhang, L. Global and local indicators of spatial association between points and polygons: A study of land use change. Int. J. Appl. Earth Obs. Geoinf. ITC J. 2013, 21, 384–396. [Google Scholar] [CrossRef]
- Bivand, R.S.; Wong, D.W.S. Comparing implementations of global and local indicators of spatial association. TEST 2018, 27, 716–748. [Google Scholar] [CrossRef]
- Anselin, L. Local Indicators of Spatial Association—LISA. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Hilmola, O.-P.; Henttu, V. Transportation costs do matter: Simulation study from hospital investment decision. J. Model. Manag. 2016, 11, 560–584. [Google Scholar] [CrossRef]
- Yeom, H.A.; Fleury, J.; Keller, C. Risk Factors for Mobility Limitation in Community-Dwelling Older Adults: A Social Ecological Perspective. Geriatr. Nurs. 2008, 29, 133–140. [Google Scholar] [CrossRef]
- Cinnamon, J.; Schuurman, N.; Crooks, V.A. A method to determine spatial access to specialized palliative care services using GIS. BMC Health Serv. Res. 2008, 8, 140. [Google Scholar] [CrossRef] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, X.; Gong, P.; White, M. Study on Spatial Distribution Equilibrium of Elderly Care Facilities in Downtown Shanghai. Int. J. Environ. Res. Public Health 2022, 19, 7929. https://doi.org/10.3390/ijerph19137929
Huang X, Gong P, White M. Study on Spatial Distribution Equilibrium of Elderly Care Facilities in Downtown Shanghai. International Journal of Environmental Research and Public Health. 2022; 19(13):7929. https://doi.org/10.3390/ijerph19137929
Chicago/Turabian StyleHuang, Xiaoran, Pixin Gong, and Marcus White. 2022. "Study on Spatial Distribution Equilibrium of Elderly Care Facilities in Downtown Shanghai" International Journal of Environmental Research and Public Health 19, no. 13: 7929. https://doi.org/10.3390/ijerph19137929