
Relationship between Dysphagia and Home Discharge among Older Patients Receiving Hospital Rehabilitation in Rural Japan: A Retrospective Cohort Study



Abstract
:1. Introduction
1.1. Dysphagia in Older Patients
1.2. Swallowing Mechanism
1.3. Relationship between Dysphagia and Health Outcomes
1.4. Difference in Rehabilitation between Urban and Rural Settings
1.5. Rationale and Purpose of This Study
2. Materials and Methods
2.1. Purpose
2.2. Design
2.3. Setting
2.4. Recovery Rehabilitation Unit
2.5. Participants
2.5.1. Inclusion Criteria
- -
- Aged over 65 years and discharged from the Unnan City Hospital after treatment of acute diseases and training in the rehabilitation unit
- -
- Discharged between 1 April 2016 and 31 March 2020
- -
- Consented to their data being used in this research
2.5.2. Exclusion Criteria
- -
- Lacked key outcomes and predictors: body mass index (BMI), blood albumin concentration, care level, duration of rehabilitation, dysphagia, and the discharge conditions.
- -
- Admitted to the rehabilitation unit and died or transferred to the acute unit in the hospital during the admission because of acute changes in their conditions.
2.6. Measurements
2.6.1. Primary Outcome
2.6.2. Independent Variable
2.6.3. Covariates
Polypharmacy
Charlson Comorbidity Index
Care Level Based on the Japanese Long-Term Care Insurance System
Functional Independence Measure
2.7. Statistical Analysis
2.8. Assessment of Ethical or Other Risks and Permissions
3. Results
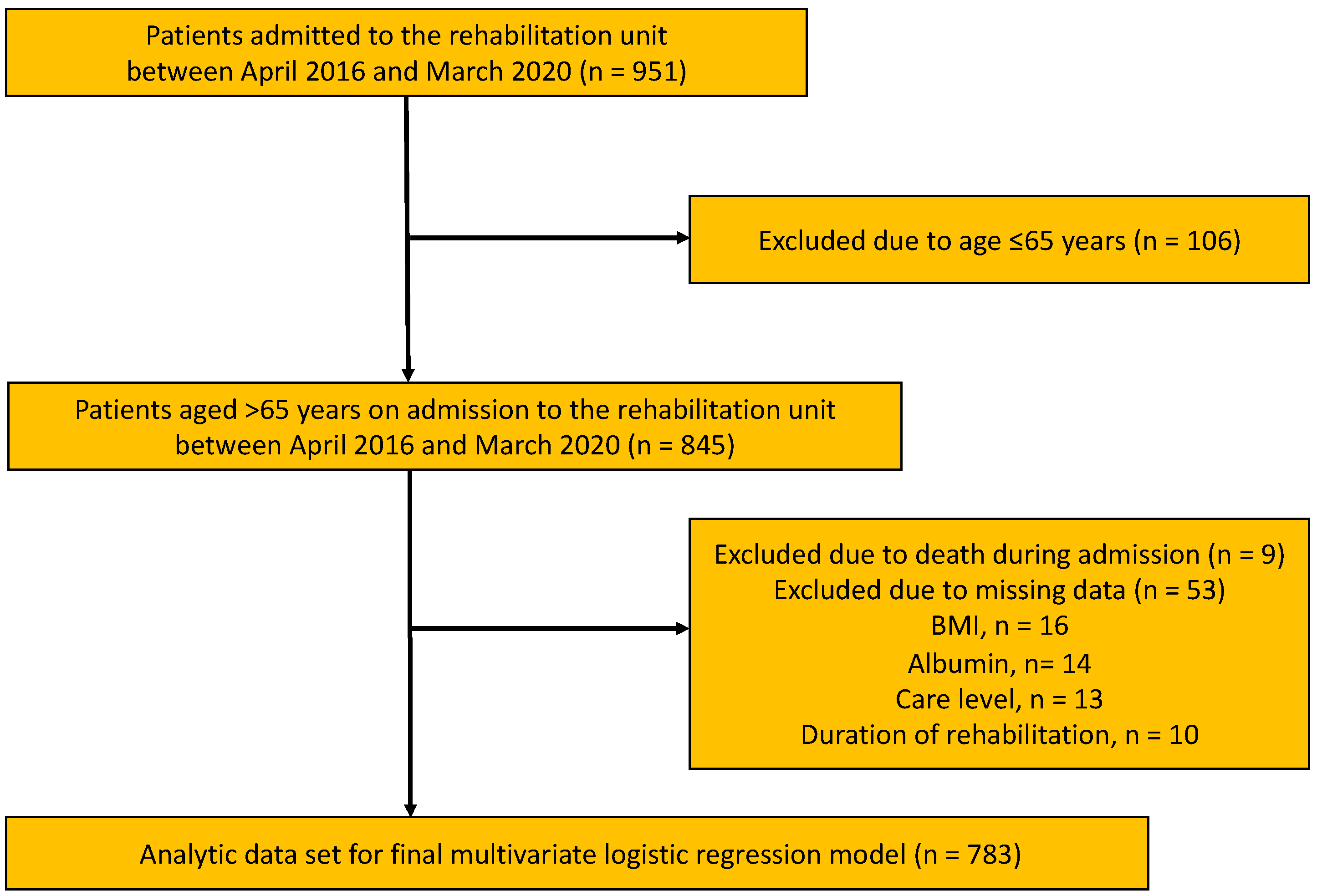
3.1. Participant Selection
3.2. Demographics of the Participants
3.3. Reasons for Hospital Admission
3.4. Relationship between Dysphagia and Home Discharge
4. Discussion
4.1. Dysphagia Impinges on Home Discharge of Older Patients in Rural Areas
4.2. Medicines Affecting Dysphagia in Internal Medicine
4.3. ADL Affecting Discharge to Home
4.4. Factors Not Related to Home Discharge among Older Patients
4.5. Comprehensive Methods to Address Dysphagia among Older Patients
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baijens, L.W.; Clave, P.; Cras, P.; Ekberg, O.; Forster, A.; Kolb, G.F.; Leners, J.C.; Masiero, S.; Mateos-Nozal, J.; Ortega, O.; et al. European Society for Swallowing Disorders—European Union Geriatric Medicine Society white paper: Oropharyngeal dysphagia as a geriatric syndrome. Clin. Interv. Aging 2016, 11, 1403–1428. [Google Scholar] [CrossRef] [PubMed]
- Fujishima, I.; Fujiu-Kurachi, M.; Arai, H.; Hyodo, M.; Kagaya, H.; Maeda, K.; Mori, T.; Nishioka, S.; Oshima, F.; Ogawa, S.; et al. Sarcopenia and dysphagia: Position paper by four professional organizations. Geriatr. Gerontol. Int. 2019, 19, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Ortega, O.; Martín, A.; Clavé, P. Diagnosis and management of oropharyngeal dysphagia among older persons. state of the art. J. Am. Med. Dir. Assoc. 2017, 18, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Carrión, S.; Cabré, M.; Monteis, R.; Roca, M.; Palomera, E.; Serra-Prat, M.; Rofes, L.; Clavé, P. Oropharyngeal dysphagia is a prevalent risk factor for malnutrition in a cohort of older patients admitted with an acute disease to a general hospital. Clin. Nutr. 2015, 34, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Sreedharan, S.E.; Sayed, J.V.; Vipina, V.P.; Mohan, M.P.; Paul, R.; Sylaja, P.N. Dysphagia and disability in minor strokes—An institutional study. J. Stroke Cerebrovasc. Dis. 2020, 29, 105070. [Google Scholar] [CrossRef] [PubMed]
- Maeshima, S.; Osawa, A.; Miyazaki, Y.; Seki, Y.; Miura, C.; Tazawa, Y.; Tanahashi, N. Influence of dysphagia on short-term outcome in patients with acute stroke. Am. J. Phys. Med. Rehabil. 2011, 90, 316–320. [Google Scholar] [CrossRef]
- Taylor, J.K.; Fleming, G.B.; Singanayagam, A.; Hill, A.T.; Chalmers, J.D. Risk factors for aspiration in community acquired pneumonia: Analysis of a hospitalized UK cohort. Am. J. Med. 2013, 126, 995–1001. [Google Scholar] [CrossRef]
- Broadley, S.; Croser, D.; Cottrell, J.; Creevy, M.; Teo, E.; Yiu, D.; Pathi, R.; Taylor, J.; Thompson, P.D. Predictors of prolonged dysphagia following acute stroke. J. Clin. Neurosci. 2003, 10, 300–305. [Google Scholar] [CrossRef]
- Yokota, J.; Ogawa, Y.; Takahashi, Y.; Yamaguchi, N.; Onoue, N.; Shinozaki, T.; Kohzuki, M. Dysphagia hinders hospitalized patients with heart failure from being discharged to home. Tohoku J. Exp. Med. 2019, 249, 163–171. [Google Scholar] [CrossRef]
- Paranji, S.; Paranji, N.; Wright, S.; Chandra, S. A nationwide study of the impact of dysphagia on hospital outcomes among patients with dementia. Am. J. Alzheimers Dis. Other Demen. 2017, 32, 5–11. [Google Scholar] [CrossRef]
- Cabré, M.; Serra-Prat, M.; Force, L.; Almirall, J.; Palomera, E.; Clavé, P. Oropharyngeal dysphagia is a risk factor for readmission for pneumonia in the very elderly persons: Observational prospective study. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, H.; Yoshimura, Y.; Fujita, S.; Maeno, Y. Incidence of dysphagia and its association with functional recovery and 1-year mortality in hospitalized older patients with heart failure: A prospective cohort study. JPEN J. Parenter. Enteral. Nutr. 2021, 45, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Morishita, S.; Ohara, Y.; Iwasaki, M.; Edahiro, A.; Motokawa, K.; Shirobe, M.; Furuya, J.; Watanabe, Y.; Suga, T.; Kanehisa, Y.; et al. Relationship between mortality and oral function of older people requiring long-term care in rural areas of Japan: A four-year prospective cohort study. Int. J. Environ. Res. Public Health 2021, 18, 1723. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, L.; Iburg, K.M.; Adair, T.; Fürst, T.; Hegnauer, M.; von der Lippe, E.; Moran, L.; Nomura, S.; Sakamoto, H.; Shibuya, K.; et al. Assessing the quality of cause of death data in six high-income countries: Australia. Canada, Denmark, Germany, Japan and Switzerland. Int. J. Public Health 2020, 65, 17–28. [Google Scholar] [CrossRef]
- Momosaki, R.; Yasunaga, H.; Matsui, H.; Horiguchi, H.; Fushimi, K.; Abo, M. Effect of dysphagia rehabilitation on oral intake in elderly patients with aspiration pneumonia. Geriatr. Gerontol. Int. 2015, 15, 694–699. [Google Scholar] [CrossRef]
- Nakashima, T.; Maeda, K.; Tahira, K.; Taniguchi, K.; Mori, K.; Kiyomiya, H.; Akagi, J. Silent aspiration predicts mortality in older adults with aspiration pneumonia admitted to acute hospitals. Geriatr. Gerontol. Int. 2018, 18, 828–832. [Google Scholar] [CrossRef]
- Park, C.H.; Kim, D.K.; Lee, Y.T.; Yi, Y.; Lee, J.S.; Kim, K.; Park, J.H.; Yoon, K.J. Quantitative analysis of swallowing function between dysphagia patients and healthy subjects using high-resolution manometry. Ann. Rehabil. Med. 2017, 41, 776–785. [Google Scholar] [CrossRef]
- Helldén, J.; Bergström, L.; Karlsson, S. Experiences of living with persisting post-stroke dysphagia and of dysphagia management—A qualitative study. Int. J. Qual Stud. Health Well-Being 2018, 13 (Suppl. S1), 1522194. [Google Scholar] [CrossRef]
- Payne, M.; Morley, J.E. Editorial: Dysphagia. dementia and frailty. J. Nutr. Health Aging 2018, 22, 562–565. [Google Scholar] [CrossRef]
- Perry, S.E.; Miles, A.; Fink, J.N.; Huckabee, M.L. The dysphagia in stroke protocol reduces aspiration pneumonia in patients with dysphagia following acute stroke: A clinical audit. Transl. Stroke Res. 2019, 10, 36–43. [Google Scholar] [CrossRef]
- Zahuranec, D.B.; Skolarus, L.E.; Feng, C.; Freedman, V.A.; Burke, J.F. Activity limitations and subjective well-being after stroke. Neurology 2017, 89, 944–950. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Maeki, N.; Maniwa, S.; Miyakoshi, K. Predicting factors of elderly patients discharge to home after rehabilitation in rural Japan: A retrospective cohort study. Rural. Remote Health 2021, 21, 6406. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, H.; Sakuma, K. Rehabilitation nutrition for sarcopenia with disability: A combination of both rehabilitation and nutrition care management. J. Cachexia Sarcopenia Muscle 2014, 5, 269–277. [Google Scholar] [CrossRef]
- Kaysar, M.; Augustine, T.; Jim, L.; Benjamin, C. Predictors of length of stay between the young and aged in hospitalized community-acquired pneumonia patients. Geriatr. Gerontol. Int. 2008, 8, 227–233. [Google Scholar] [CrossRef]
- Vluggen, T.P.M.M.; van Haastregt, J.C.M.; Tan, F.E.S.; Kempen, G.I.J.M.; Schols, J.M.G.A.; Verbunt, J.A. Factors associated with successful home discharge after inpatient rehabilitation in frail older stroke patients. BMC Geriatr. 2020, 20, 25. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, Y.; Wakabayashi, H.; Bise, T.; Nagano, F.; Shimazu, S.; Shiraishi, A.; Yamaga, M.; Koga, H. Sarcopenia is associated with worse recovery of physical function and dysphagia and a lower rate of home discharge in Japanese hospitalized adults undergoing convalescent rehabilitation. Nutrition 2019, 61, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Low, J.; Wyles, C.; Wilkinson, T.; Sainsbury, R. The effect of compliance on clinical outcomes for patients with dysphagia on videofluoroscopy. Dysphagia 2001, 16, 123–127. [Google Scholar] [CrossRef]
- Jia, H.; Cowper, D.C.; Tang, Y.; Litt, E.; Wilson, L. Post acute stroke rehabilitation utilization: Are there differences between rural-urban patients and taxonomies? J. Rural Health 2012, 28, 242–247. [Google Scholar] [CrossRef]
- Daras, L.C.; Ingber, M.J.; Deutsch, A.; Hefele, J.G.; Perloff, J. Geographic region and profit status drive variation in hospital readmission outcomes among inpatient rehabilitation facilities in the United States. Arch. Phys. Med. Rehabil. 2018, 99, 1060–1066. [Google Scholar] [CrossRef]
- Field, P.E.; Franklin, R.C.; Barker, R.N.; Ring, I.; Leggat, P.A. Cardiac rehabilitation services for people in rural and remote areas: An integrative literature review. Rural Remote Health 2018, 18, 4738. [Google Scholar] [CrossRef]
- Tanaka, K.; Iwasawa, M. Aging in rural Japan—limitations in the current social care policy. J. Aging Soc. Policy 2010, 22, 394–406. [Google Scholar] [CrossRef] [PubMed]
- Aude, T.; Hill, P.D.; Anderson, M.A. Quality of life after participation in a rural phase II cardiac rehabilitation program. J. Nurs. Care Qual. 2006, 21, 56–62. [Google Scholar] [PubMed]
- Allen, J.; Greene, M.; Sabido, I.; Stretton, M.; Miles, A. Economic costs of dysphagia among hospitalized patients. Laryngoscope 2020, 130, 974–979. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Sano, C. Risk of hospital readmission among older patients discharged from the rehabilitation unit in a rural community hospital: A retrospective cohort study. J. Clin. Med. 2021, 10, 659. [Google Scholar] [CrossRef] [PubMed]
- Onoue, H.; Koyama, T.; Zamami, Y.; Hagiya, H.; Tatebe, Y.; Mikami, N.; Shinomiya, K.; Kitamura, Y.; Hinotsu, S.; Sendo, T.; et al. Trends in polypharmacy in Japan: A nationwide retrospective study. J. Am. Geriatr. Soc. 2018, 66, 2267–2273. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Meyer-Massetti, C.; Meier, C.R.; Guglielmo, B.J. The scope of drug-related problems in the home care setting. Int. J. Clin. Pharm. 2018, 40, 325–334. [Google Scholar] [CrossRef]
- Niikawa, H.; Okamura, T.; Ito, K.; Ura, C.; Miyamae, F.; Sakuma, N.; Ijuin, M.; Inagaki, H.; Sugiyama, M.; Awata, S. Association between polypharmacy and cognitive impairment in an elderly Japanese population residing in an urban community. Geriatr Gerontol. Int. 2017, 17, 1286–1293. [Google Scholar] [CrossRef]
- Ambrose, A.F.; Cruz, L.; Paul, G. Falls and fractures: A systematic approach to screening and prevention. Maturitas 2015, 82, 85–93. [Google Scholar]
- Shimizutani, S. The future of long-term care in Japan. Asia-Pacific Rev. 2014, 21, 88–119. [Google Scholar] [CrossRef]
- Nakaguchi, T.; Ishimoto, T.; Akazawa, N. Minimal clinically important difference for functional independence measure gain in post-acute rehabilitation ward patients with motor disorders. Rigakuryoho Kagaku 2018, 33, 235–240. [Google Scholar]
- Hayashi, H.; Iwai, M.; Matsuoka, H.; Nakashima, D.; Nakamura, S.; Kubo, A.; Tomiyama, N. Factors affecting the discharge destination of hip fracture patients who live alone and have been admitted to an inpatient rehabilitation unit. J. Phys. Ther. Sci. 2016, 28, 1228–1232. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software EZR for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [PubMed]
- Bath, P.M.; Lee, H.S.; Everton, L.F. Swallowing therapy for dysphagia in acute and subacute stroke. Cochrane Database Syst. Rev. 2018, 10, CD000323. [Google Scholar]
- Chadwick, D.D.; Jolliffe, J.; Goldbart, J. Carer knowledge of dysphagia management strategies. Int. J. Lang. Commun. Disord. 2002, 37, 345–357. [Google Scholar] [PubMed]
- Shune, S.E.; Namasivayam-MacDonald, A. Dysphagia-related caregiver burden: Moving beyond the physiological impairment. Perspect. ASHA Spec. Interest Groups 2020, 5, 1282–1289. [Google Scholar] [CrossRef]
- Namasivayam-MacDonald, A.M.; Shune, S.E. The burden of dysphagia on family caregivers of the elderly: A systematic review. Geriatrics 2018, 3, 30. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Ryu, Y.; Kataoka, D.; Sano, C. Effectiveness and challenges in local self-governance: Multifunctional autonomy in Japan. Int. J. Environ. Res. Public Health 2021, 18, 574. [Google Scholar]
- Ohta, R.; Ryu, Y.; Katsube, T. Home care workers judgments about users acute conditions: A qualitative study on interprofessional collaboration. Home Health Care Serv. Q. 2020, 39, 184–195. [Google Scholar] [CrossRef]
- Kuroda, M.; Ohta, R.; Kuroda, K.; Yamashiro, S.; Kita, K. The seamless communication on a rural island in Japan: A qualitative study from the perspective of healthcare professionals. Int. J. Environ. Res. Public Health 2021, 18, 2021. [Google Scholar]
- Campbell, J.C.; Ikegami, N. Long-term care insurance comes to Japan. Health Aff. 2000, 19, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Chi, W.C.; Wolff, J.; Greer, R.; Dy, S. Multimorbidity and decision-making preferences among older adults. Ann. Fam. Med. 2017, 15, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Steinman, L.E.; Frederick, J.T.; Prohaska, T.; Satariano, W.A.; Dornberg-Lee, S.; Fisher, R.; Graub, P.B.; Leith, K.; Presby, K.; Sharkey, J.; et al. and Late Life Depression Special Interest Project (SIP) Panelists. Recommendations for treating depression in community-based older adults. Am. J. Prev. Med. 2007, 33, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Katona, C.; Lyketsos, K.; Blazer, D.; Brodaty, H.; Rabins, P.; de Mendonça Lima, C.A.; Livingston, G. A systematic review of treatments for refractory depression in older people. Am. J. Psychiatry 2011, 168, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Olesen, M.D.; Modlinski, R.M.; Poulsen, S.H.; Rosenvinge, P.M.; Rasmussen, H.H.; Holst, M. Prevalence of signs of dysphagia and associated risk factors in geriatric patients admitted to an acute medical unit. Clin. Nutr. ESPEN 2021, 41, 208–216. [Google Scholar] [CrossRef]
- Cockburn, N.; Pradhan, A.; Taing, M.W.; Kisely, S.; Ford, P.J. Oral health impacts of medications used to treat mental illness. J. Affect. Disord. 2017, 223, 184–193. [Google Scholar] [CrossRef]
- Inouye, S.K.; Westendorp, R.G.J.; Saczynski, J.S. Delirium in elderly people. Lancet 2014, 383, 911–922. [Google Scholar] [CrossRef]
- Fong, T.G.; Tulebaev, S.R.; Inouye, S.K. Delirium in elderly adults: Diagnosis. prevention and treatment. Nat. Rev. Neurol. 2009, 5, 210–220. [Google Scholar] [CrossRef]
- Marcott, S.; Dewan, K.; Kwan, M.; Baik, F.; Lee, Y.J.; Sirjani, D. Where dysphagia begins: Polypharmacy and xerostomia. Fed. Pract. 2020, 37, 234–241. [Google Scholar]
- Pu, D.; Wong, M.C.H.; Yiu, E.M.L.; Chan, K.M.K. Profiles of polypharmacy in older adults and medication associations with signs of aspiration. Expert Rev. Clin. Pharmacol. 2021, 14, 643–649. [Google Scholar] [CrossRef]
- Hein, C.; Forgues, A.; Piau, A.; Sommet, A.; Vellas, B.; Nourhashémi, F. Impact of polypharmacy on occurrence of delirium in elderly emergency patients. J. Am. Med. Dir. Assoc. 2014, 15, 850.e11–850.e15. [Google Scholar] [CrossRef] [PubMed]
- Elliott, A.M.; McAteer, A.; Hannaford, P.C. Revisiting the symptom iceberg in todays primary care: Results from a UK population survey. BMC Fam. Pract. 2011, 12, 16. [Google Scholar] [CrossRef] [PubMed]
- Soril, L.J.; Leggett, L.E.; Lorenzetti, D.L.; Noseworthy, T.W.; Clement, F.M. Characteristics of frequent users of the emergency department in the general adult population: A systematic review of international healthcare systems. Health Policy 2016, 120, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Smits, F.T.; Brouwer, H.J.; Zwinderman, A.H.; Mohrs, J.; Schene, A.H.; van Weert, H.C.; ter Riet, G. Why do they keep coming back? Psychosocial etiology of persistence of frequent attendance in primary care: A prospective cohort study. J. Psychosom. Res. 2014, 77, 492–503. [Google Scholar] [CrossRef]
- Ohta, R.; Sato, M.; Kitayuguchi, J.; Maeno, T.; Sano, C. The association between the self-management of mild symptoms and quality of life of elderly populations in rural communities: A cross-sectional study. Int. J. Environ. Res. Public Health 2021, 18, 8857. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Ryu, Y.; Sano, C. Older peoples help-seeking behaviors in rural contexts: A systematic review. Int. J. Environ. Res. Public Health 2022, 19, 3233. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Sato, M.; Ryu, Y.; Kitayuguchi, J.; Maeno, T.; Sano, C. What resources do elderly people choose for managing their symptoms? Clarification of rural older peoples choices of help-seeking behaviors in Japan. BMC Health Serv. Res. 2021, 21, 640. [Google Scholar] [CrossRef]
- Akirov, A.; Masri-Iraqi, H.; Atamna, A.; Shimon, I. Low albumin levels are associated with mortality risk in hospitalized patients. Am. J. Med. 2017, 130, 1465.e1411–1465.e1419. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Kitayuguchi, J.; Gomi, T.; Katsube, T. Challenges and solutions in the continuity of home care for rural older people: A thematic analysis. Home Health Care Serv. Q. 2020, 39, 126–139. [Google Scholar] [CrossRef]
- Samaras, N.; Chevalley, T.; Samaras, D.; Gold, G. Older patients in the emergency department: A review. Ann. Emerg. Med. 2010, 56, 261–269. [Google Scholar] [CrossRef]
- Nathan, R.H.; Aronsky, D. Systematic review of emergency department crowding: Causes, effects, and solutions. Ann. Emerg. Med. 2008, 52, 126–136.e121. [Google Scholar] [CrossRef]
- Wetzels, R.; Geest, T.A.; Wensing, M.; Ferreira, P.L.; Grol, R.; Baker, R. GPs views on involvement of older patients: A European qualitative study. Patient Educ Couns 2004, 53, 183–188. [Google Scholar] [CrossRef]
- Stringer, K.; Curran, V.; Asghari, S. Pharmacists and family physicians: Improving interprofessional collaboration through joint understanding of our competencies. Front. Pharmacol. 2013, 4, 151. [Google Scholar] [CrossRef] [PubMed]
- Silvaggi, A.; Nabhani-Gebara, S.; Reeves, S. Expanding pharmacy roles and the interprofessional experience in primary healthcare: A qualitative study. J. Interprof. Care 2017, 31, 110–111. [Google Scholar] [CrossRef] [PubMed]
- Löffler, C.; Koudmani, C.; Böhmer, F.; Paschka, S.D.; Höck, J.; Drewelow, E.; Stremme, M.; Stahlhacke, B.; Altiner, A. Perceptions of interprofessional collaboration of general practitioners and community pharmacists—A qualitative study. BMC Health Serv. Res. 2017, 17, 224. [Google Scholar] [CrossRef]
- Sangaleti, C.; Schveitzer, M.C.; Peduzzi, M.; Zoboli, E.; Soares, C.B. Experiences and shared meaning of teamwork and interprofessional collaboration among health care professionals in primary health care settings: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2017, 15, 2723–2788. [Google Scholar] [CrossRef]
- Hopman, P.; de Bruin, S.R.; Forjaz, M.J.; Rodriguez-Blazquez, C.; Tonnara, G.; Lemmens, L.C.; Onder, G.; Baan, C.A.; Rijken, M. Effectiveness of comprehensive care programs for patients with multiple chronic conditions or frailty: A systematic literature review. Health Policy 2016, 120, 818–832. [Google Scholar] [CrossRef]
- Raheem, D.; Carrascosa, C.; Ramos, F.; Saraiva, A.; Raposo, A. Texture-modified food for dysphagic patients: A comprehensive review. Int. J. Environ. Res. Public Health 2021, 18, 5125. [Google Scholar] [CrossRef]
- Shimizu, A.; Ohta, R.; Otani, H.; Sano, C. The contribution of temporal flat lateral position on the mortality and discharge rates of older patients with severe dysphagia. Int. J. Environ. Res. Public Health 2021, 18, 8443. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Definitions |
|---|---|
| Primary outcome | Discharge destination (Home or long-term care facilities) |
| Patient demographics | Age (years) |
| Sex (male or female) | |
| Body mass index (kg/m2) at admission | |
| Serum albumin (g/dL) at admission | |
| Number of medications at admission | |
| Charlson Comorbidity Index score at admission | |
| Care level based on the Japanese long-term insurance at admission | |
| Cognitive and motor component scores of the Functional Independence Measure at admission Reasons for admission (orthopedic or medical condition) |
| Standards | Explanation |
|---|---|
| 7 | Complete independence (timely, safety) |
| 6 | Modified independence (with device) |
| 5 | Supervision (subject = 100%) |
| 4 | Minimal assistance (subject = 75% or more) |
| 3 | Moderate assistance (subject = 50% or more) |
| 2 | Maximal assistance (subject = 25% or more) |
| 1 | Total assistance or not testable (subject less than 25%) |
| Dysphagia | ||||
|---|---|---|---|---|
| Factor | Total | Yes | No | p-Value |
| N | 783 | 101 | 682 | |
| Age (years), mean (SD) | 82.12 (10.77) | 81.71 (8.87) | 82.18 (11.03) | 0.684 |
| Male sex (%) | 270 (34.5) | 53 (52.5) | 217 (31.8) | <0.001 |
| Albumin (g/dL), mean (SD) | 3.76 (0.56) | 3.70 (0.58) | 3.77 (0.56) | 0.305 |
| BMI (kg/m2), mean (SD) | 21.37 (4.91) | 20.75 (3.81) | 21.47 (5.04) | 0.181 |
| Medicines taken, mean (SD) | 4.91 (3.00) | 5.45 (3.44) | 4.83 (2.93) | 0.055 |
| Patients with polypharmacy, n (%) | 402 (51.3) | 57 (56.4) | 345 (50.6) | 0.288 |
| Reasons for admission, n (%) | ||||
| Medical | 314 (40.1) | 72 (71.3) | 242 (35.5) | <0.001 |
| Orthopedic | 469 (59.9) | 29 (28.7) | 440 (64.5) | |
| FIM score at admission | ||||
| Total FIM score (median) | 109.00 (13.00, 126.00) | 86.00 (18.00, 126.00) | 111.00 (13.00, 126.00) | <0.001 |
| Motor domain score (median) | 78.00 (2.00, 91.00) | 61.00 (13.00, 91.00) | 79.00 (2.00, 91.00) | <0.001 |
| Cognitive domain score (median) | 32.00 (0.00, 35.00) | 28.00 (5.00, 35.00) | 32.00 (0.00, 35.00) | <0.001 |
| Discharge to home (%) | 643 (82.1) | 54 (53.5) | 589 (86.4) | <0.001 |
| Care level (%) | ||||
| 0 | 567 (72.4) | 68 (67.3) | 499 (73.2) | 0.024 |
| 1 | 39 (5.0) | 1 (1.0) | 38 (5.6) | |
| 2 | 72 (9.2) | 10 (9.9) | 62 (9.1) | |
| 3 | 48 (6.1) | 8 (7.9) | 40 (5.9) | |
| 4 | 29 (3.7) | 6 (5.9) | 23 (3.4) | |
| 5 | 28 (3.6) | 8 (7.9) | 20 (2.9) | |
| Dependent condition (%) | 216 (27.6) | 33 (32.7) | 183 (26.8) | 0.234 |
| CCI score (%) | ||||
| 2 | 40 (5.1) | 1 (1.0) | 47 (6.9) | <0.001 |
| 3 | 66 (8.4) | 7 (6.9) | 59 (8.7) | |
| 4 | 209 (26.7) | 20 (19.8) | 189 (27.7) | |
| 5 | 163 (20.8) | 24 (23.8) | 139 (20.4) | |
| 6 | 150 (19.2) | 24 (23.8) | 126 (18.5) | |
| 7 | 80 (10.2) | 14 (13.9) | 66 (9.7) | |
| 8 | 37 (4.7) | 4 (4.0) | 33 (4.8) | |
| 9 | 20 (2.6) | 5 (5.0) | 15 (2.2) | |
| 10 | 9 (1.1) | 2 (2.0) | 7 (1.0) | |
| 12 | 1 (0.1) | 0 (0.0) | 1 (0.1) | |
| CCI score ≥ 5 (%) | 460 (58.7) | 73 (72.3) | 387 (56.7) | 0.003 |
| Heart failure (%) | 100 (12.8) | 16 (15.8) | 84 (12.3) | 0.338 |
| Myocardial infarction (%) | 38 (4.9) | 4 (4.0) | 35 (5.1) | 0.807 |
| Asthma (%) | 36 (4.6) | 5 (5.0) | 31 (4.5) | 0.8 |
| Kidney diseases (%) | 151 (19.3) | 17 (16.8) | 134 (19.6) | 0.589 |
| Peptic ulcer (%) | 36 (4.6) | 2 (2.0) | 34 (5.0) | 0.303 |
| Liver diseases (%) | 26 (3.3) | 8 (7.9) | 17 (2.5) | 0.016 |
| COPD (%) | 24 (3.1) | 1 (1.0) | 23 (3.4) | 0.348 |
| DM (%) | 143 (18.3) | 21 (20.8) | 122 (17.9) | 0.491 |
| Brain hemorrhage (%) | 90 (11.5) | 8 (7.9) | 82 (12.0) | 0.314 |
| Brain infarction (%) | 171 (21.8) | 24 (23.8) | 147 (21.6) | 0.607 |
| Hemiplegia (%) | 28 (3.6) | 2 (2.0) | 26 (3.8) | 0.564 |
| Dementia (%) | 65 (8.3) | 10 (9.9) | 55 (8.1) | 0.561 |
| Connective tissue diseases (%) | 37 (4.7) | 5 (5.0) | 32 (4.7) | 0.805 |
| Cancer (%) | 134 (17.0) | 13 (14.0) | 111 (17.4) | 0.226 |
| Medical Condition | Orthopedic Condition | ||||
|---|---|---|---|---|---|
| Diagnosis | Number | Percentage | Diagnosis | Number | Percentage |
| Brain stroke | 139 | 44.3% | Femoral fracture | 201 | 42.9% |
| Brain hemorrhage | 75 | 23.9% | Compression fracture | 122 | 26.0% |
| Pneumonia * | 21 | 6.7% | Knee osteoarthritis | 50 | 10.7% |
| Pyelonephritis | 15 | 4.8% | Pelvic fracture | 34 | 7.2% |
| Dehydration | 12 | 3.8% | Spinal canal stenosis | 15 | 3.2% |
| Other infections * | 12 | 3.8% | Hip osteoarthritis | 11 | 2.3% |
| Heart failure | 11 | 3.5% | Patella fracture | 11 | 2.3% |
| Cancer * | 7 | 2.2% | Tibial fracture | 9 | 1.9% |
| Intracranial hypertension | 4 | 1.3% | Spinal cord injury | 7 | 1.5% |
| Guillain–Barre Syndrome | 4 | 1.3% | Radius fracture | 4 | 0.9% |
| Aortic dissection | 3 | 1.0% | Neck fracture | 2 | 0.4% |
| Hernia | 3 | 1.0% | Amputation | 1 | 0.2% |
| Autoimmune diseases * | 3 | 1.0% | Brachial plexus injury | 1 | 0.2% |
| Bowel obstruction | 2 | 0.6% | Clavicular fracture | 1 | 0.2% |
| Epilepsy | 2 | 0.6% | |||
| Pulmonary embolism | 1 | 0.3% | |||
| Factor | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|
| Presence of dysphagia | 0.38 | 0.20–0.73 | 0.0032 |
| Age | 1 | 0.97–1.03 | 0.85 |
| Males | 1.37 | 0.78–2.41 | 0.28 |
| Albumin | 1.09 | 0.69–1.70 | 0.72 |
| Polypharmacy | 0.53 | 0.32–0.90 | 0.018 |
| Reasons for admission, internal medicine | 0.44 | 0.26–0.77 | 0.0041 |
| FIM score at admission | |||
| Motor domain score | 1.07 | 1.05–1.08 | <0.001 |
| Cognitive domain score | 1.00 | 0.96–1.04 | 0.9 |
| Dependent condition | 1.26 | 0.74–2.17 | 0.4 |
| CCI score ≥ 5 (%) | 1.62 | 0.90–2.93 | 0.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohta, R.; Weiss, E.; Mekky, M.; Sano, C. Relationship between Dysphagia and Home Discharge among Older Patients Receiving Hospital Rehabilitation in Rural Japan: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 10125. https://doi.org/10.3390/ijerph191610125
Ohta R, Weiss E, Mekky M, Sano C. Relationship between Dysphagia and Home Discharge among Older Patients Receiving Hospital Rehabilitation in Rural Japan: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(16):10125. https://doi.org/10.3390/ijerph191610125
Chicago/Turabian StyleOhta, Ryuichi, Emily Weiss, Magda Mekky, and Chiaki Sano. 2022. "Relationship between Dysphagia and Home Discharge among Older Patients Receiving Hospital Rehabilitation in Rural Japan: A Retrospective Cohort Study" International Journal of Environmental Research and Public Health 19, no. 16: 10125. https://doi.org/10.3390/ijerph191610125