
Is Dual-Task Training Clinically Beneficial to Improve Balance and Executive Function in Community-Dwelling Older Adults with a History of Falls?


Abstract
:1. Introduction
2. Materials and Methods
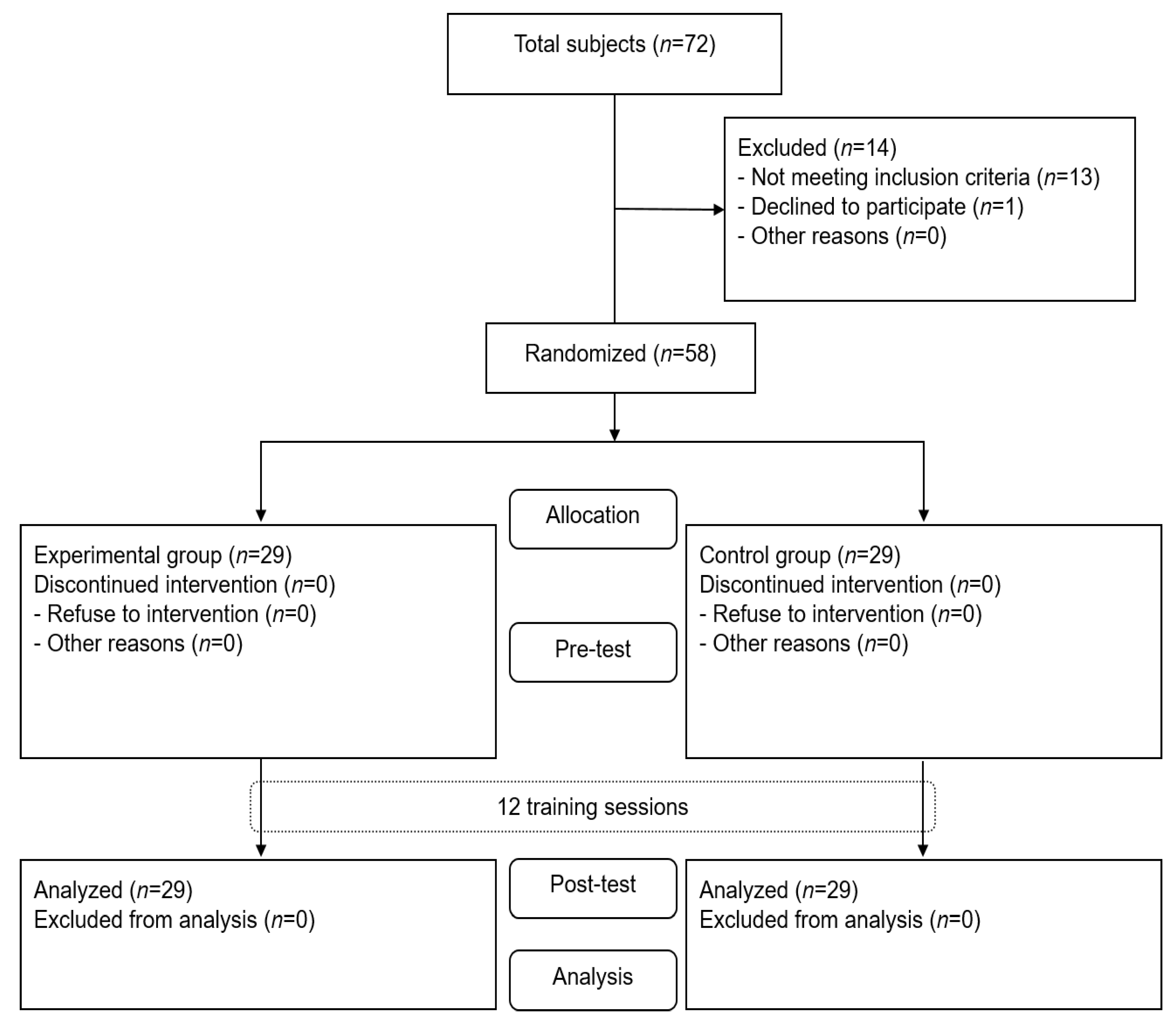
2.1. Study Design
2.2. Subjects
2.3. Intervention
2.4. Measurement
2.5. Statistical Analysis
3. Results
3.1. Subject’s Characteristics
3.2. Balance
3.3. Executive Function
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thomas, E.; Battaglia, G.; Patti, A.; Brusa, J.; Leonardi, V.; Palma, A.; Bellafiore, M. Physical activity programs for balance and fall prevention in elderly: A systematic review. Medicine 2019, 98, e16218. [Google Scholar] [CrossRef] [PubMed]
- Delbroek, T.; Vermeylen, W.; Spildooren, J. The effect of cognitive-motor dual task training with the biorescue force platform on cognition, balance and dual task performance in institutionalized older adults: A randomized controlled trial. J. Phys. Ther. Sci. 2017, 29, 1137–1143. [Google Scholar] [CrossRef] [PubMed]
- Al-Yahya, E.; Dawes, H.; Smith, L.; Dennis, A.; Howells, K.; Cockburn, J. Cognitive motor interference while walking: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2011, 35, 715–728. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.Y.; Wang, Y.L.; Cheng, F.Y.; Chao, Y.H.; Chen, C.L.; Yang, Y.R. Effects of combined exercise on gait variability in community-dwelling older adults. Age 2015, 37, 40. [Google Scholar] [CrossRef]
- Bergen, G.; Stevens, M.R.; Burns, E.R. Falls and fall injuries among adults aged ≥65 years—United States, 2014. MMWR 2016, 65, 993–998. [Google Scholar] [CrossRef]
- Falbo, S.; Condello, G.; Capranica, L.; Forte, R.; Pesce, C. Effects of physical-cognitive dual task training on executive function and gait performance in older adults: A randomized controlled trial. BioMed Res. Int. 2016, 2016, 5812092. [Google Scholar] [CrossRef]
- McCulloch, K.L.; Buxton, E.; Hackney, J.; Lowers, S. Balance, attention, and dual-task performance during walking after brain injury: Associations with falls history. J. Head. Trauma. Rehabil. 2010, 25, 155–163. [Google Scholar] [CrossRef]
- Tard, C.; Dujardin, K.; Girard, A.; Debaughrien, M.; Derambure, P.; Defebvre, L.; Delval, A. How does visuospatial attention modulate motor preparation during gait initiation? Exp. Brain Res. 2016, 234, 39–50. [Google Scholar] [CrossRef]
- Beauchet, O.; Dubost, V.; Aminian, K.; Gonthier, R.; Kressig, R.W. Dual-task-related gait changes in the elderly: Does the type of cognitive task matter? J. Mot. Behav. 2005, 37, 259–264. [Google Scholar]
- Fernandes, Â.; Rocha, N.; Santos, R.; Tavares, J.M.R. Effects of dual-task training on balance and executive functions in Parkinson’s disease: A pilot study. Somatosens. Mot. Res. 2015, 32, 122–127. [Google Scholar] [CrossRef]
- Shin, S.S.; An, D.H. The effect of motor dual-task balance training on balance and gait of elderly women. J. Phys. Ther. Sci. 2014, 26, 359–361. [Google Scholar] [CrossRef] [PubMed]
- Wollesen, B.; Schulz, S.; Seydell, L.; Delbaere, K. Does dual task training improve walking performance of older adults with concern of falling? BMC Geriatr. 2017, 17, 213. [Google Scholar] [CrossRef] [PubMed]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. The role of executive function and attention in gait. Mov. Disord. 2008, 23, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Dorfman, M.; Herman, T.; Brozgol, M.; Shema, S.; Weiss, A.; Hausdorff, J.M.; Mirelman, A. Dual-task training on a treadmill to improve gait and cognitive function in elderly idiopathic fallers. J. Neurol. Phys. Ther. 2014, 38, 246–253. [Google Scholar] [CrossRef]
- Daneshjoo, A.; Mokhtar, A.H.; Rahnama, N.; Yusof, A. The effects of comprehensive warm-up programs on proprioception, static and dynamic balance on male soccer players. PLoS ONE 2012, 7, e51568. [Google Scholar] [CrossRef]
- Lee, S.-B.; Cha, Y.-N.; Lee, S.-H. The effects of dual task training on balance for elderly. Neurotherapy 2015, 19, 41–47. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Wolf, B.; Feys, H.; De Weerdt, W.; van der Meer, J.; Noom, M.; Aufdemkampe, G. Effect of a physical therapeutic intervention for balance problems in the elderly: A single-blind, randomized, controlled multicentre trial. Clin. Rehab. 2001, 15, 624–636. [Google Scholar] [CrossRef]
- Ageberg, E.; Zätterström, R.; Moritz, U. Stabilometry and one-leg hop test have high test-retest reliability. Scand. J. Med. Sci. Sports 1998, 8, 198–202. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The Timed “Up and Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Tombaugh, T.N. Trail Making Test A and B: Normative data stratified by age and education. Arch. Clin. Neuropsychol. 2004, 19, 203–214. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Science, 2nd ed.; Routledge Academic: Hillsdale, MI, USA, 1998. [Google Scholar]
- Park, J.-H. The effects of plantar perception training on balance and falls efficacy of the elderly with a history of falls: A single-blind, randomized controlled trial. Arch. Gerontol. Geriatr. 2018, 77, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-H. The effects of eyeball exercise on balance ability and falls efficacy of the elderly who have experienced a fall: A single-blind, randomized controlled trial. Arch. Gerontol. Geriatr. 2017, 68, 181–185. [Google Scholar] [CrossRef]
- Schaefer, S.; Schumacher, V. The interplay between cognitive and motor functioning in healthy older adults: Findings from dual-task studies and suggestions for intervention. Gerontology 2011, 57, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Wollesen, B.; Voelcker-Rehage, C. Training effects on motor–cognitive dual-task performance in older adults. Eur. Rev. Aging Phys. Act. 2014, 11, 5–24. [Google Scholar] [CrossRef]
- Wang, X.; Pi, Y.; Chen, P.; Liu, Y.; Wang, R.; Chan, C. Cognitive motor interference for preventing falls in older adults: A systematic review and meta-analysis of randomised controlled trials. Age Aging 2015, 44, 205–212. [Google Scholar] [CrossRef]
- Abuin-Porras, V.; Villafañe, J.H.; Jiménez-Antona, C.; Palacios, A.; Martínez-Pascual, B.; Rodríguez-Costa, I. Relationship between attention and balance: A dual-task condition study in children. J. Exerc. Rehab. 2018, 14, 349–355. [Google Scholar] [CrossRef]
- Lefaivre, S.C.; Almeida, Q.J. Can sensory attention focused exercise facilitate the utilization of proprioception for improved balance control in PD? Gait Posture 2015, 41, 630–633. [Google Scholar] [CrossRef]
- Cassady, K.; Ruitenberg, M.F.; Reuter-Lorenz, P.A.; Tommerdahl, M.; Seidler, R.D. Neural dedifferentiation across the lifespan in the motor and somatosensory systems. Cereb. Cortex 2020, 30, 3704–3716. [Google Scholar] [CrossRef]
- Hunter, S.W.; Divine, A.; Madou, E.; Omana, H.; Hill, K.D.; Johnson, A.M.; Holmes, J.D.; Wittich, W. Executive function as a mediating factor between visual acuity and postural stability in cognitively healthy adults and adults with Alzheimer’s dementia. Arch. Gerontol. Geriatr. 2020, 89, 104078. [Google Scholar] [CrossRef]
- Cuevas-Trisan, R. Balance problems and fall risks in the elderly. Clin. Geriatr. Med. 2019, 35, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Li, K.Z.; Bherer, L.; Mirelman, A.; Maidan, I.; Hausdorff, J.M. Cognitive involvement in balance, gait and dual-tasking in aging: A focused review from a neuroscience of aging perspective. Front. Neurol. 2018, 9, 913. [Google Scholar] [CrossRef] [PubMed]
- Beurskens, R.; Helmich, I.; Rein, R.; Bock, O. Age-related changes in prefrontal activity during walking in dual-task situations: A fNIRS study. Int. J. Psychophysiol. 2014, 92, 122–128. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Programs | Contents | Periods (Minute) |
|---|---|---|
| Warm-up |
| 5 |
| Dual-task training contents |
| 10 |
| 10 | |
| 10 | |
| 10 |
| Programs | Contents | Periods (Minute) |
|---|---|---|
| Warm-up |
| 5 |
| Functional balance training contents |
| 10 |
| 10 | |
| 10 | |
| 10 |
| Characteristics | Dual-Task Group (n = 29) | Balance Training Group (n = 29) | χ2/t |
|---|---|---|---|
| Age, years (SD) | 71.76 ± 3.14 | 70.97 ± 2.78 | 1.022 |
| Height (cm) | 158.61 ± 3.83 | 157.86 ± 4.07 | 0.670 |
| Weight (kg) | 61.70 ± 3.82 | 61.62 ± 3.47 | 0.602 |
| K-MMSE | 27.86 ± 1.24 | 28.03 ± 1.18 | −0.540 |
| Variables | Dual-Task Group (n = 29) | Balance Training Group (n = 29) | Between-Group Differences | p | η2 |
|---|---|---|---|---|---|
| OLST (seconds) | |||||
| Pre-intervention | 3.50 ± 0.48 | 3.47 ± 0.45 | 1.97 (1.22 to 2.71) | <0.001 | 0.332 *** |
| Post-intervention | 7.52 ± 1.57 | 5.25 ± 1.57 | |||
| Within-group changes | 3.74 (3.19 to 4.29) | 1.77 (1.25 to 2.30) | |||
| TUG test (seconds) | |||||
| Pre-intervention | 13.81 ± 1.41 | 14.11 ± 1.48 | 1.64 (1.08 to 2.20) | <0.001 | 0.375 *** |
| Post-intervention | 10.63 ± 1.11 | 12.57 ± 1.54 | |||
| Within-group changes | 3.74 (3.19 to 4.29) | 1.54 (1.25 to 1.82) |
| Variables | Dual-Task Group (n = 29) | Balance Training Group (n = 29) | Between-Group Differences | p | η2 |
|---|---|---|---|---|---|
| TMT-B (seconds) | |||||
| Pre-intervention | 89.98 ± 9.78 | 89.07 ± 10.82 | 1.55 (0.78 to 2.31) | <0.001 | 0.224 *** |
| Post-intervention | 87.65 ± 10.00 | 88.29 ± 10.83 | |||
| Within-group changes | 2.33 (1.64 to 3.02) | 0.78 (0.39 to 1.17) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.-H. Is Dual-Task Training Clinically Beneficial to Improve Balance and Executive Function in Community-Dwelling Older Adults with a History of Falls? Int. J. Environ. Res. Public Health 2022, 19, 10198. https://doi.org/10.3390/ijerph191610198
Park J-H. Is Dual-Task Training Clinically Beneficial to Improve Balance and Executive Function in Community-Dwelling Older Adults with a History of Falls? International Journal of Environmental Research and Public Health. 2022; 19(16):10198. https://doi.org/10.3390/ijerph191610198
Chicago/Turabian StylePark, Jin-Hyuck. 2022. "Is Dual-Task Training Clinically Beneficial to Improve Balance and Executive Function in Community-Dwelling Older Adults with a History of Falls?" International Journal of Environmental Research and Public Health 19, no. 16: 10198. https://doi.org/10.3390/ijerph191610198
APA StylePark, J.-H. (2022). Is Dual-Task Training Clinically Beneficial to Improve Balance and Executive Function in Community-Dwelling Older Adults with a History of Falls? International Journal of Environmental Research and Public Health, 19(16), 10198. https://doi.org/10.3390/ijerph191610198