
Impact of COVID-19 on Health-Related Quality of Life: A Longitudinal Study in a Spanish Clinical Sample

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Procedure
2.3. Measures
2.3.1. Sociodemographic and Clinical Data
2.3.2. SF-36 Questionnaire
2.4. Data Analysis
3. Results
3.1. General Characteristics
3.2. Differences in HRQoL between Patients with Post-COVID-19 Pneumonia and General Population
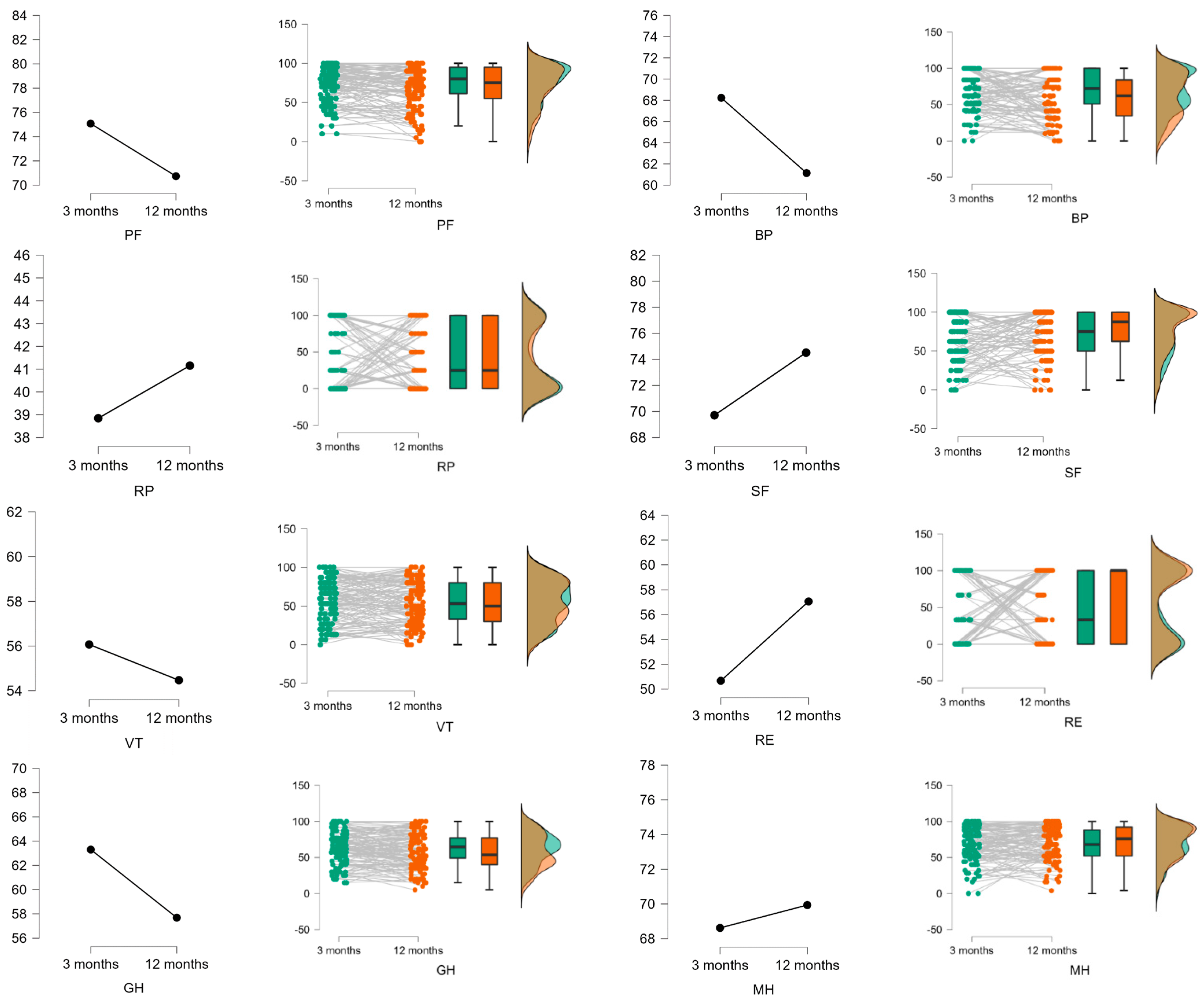
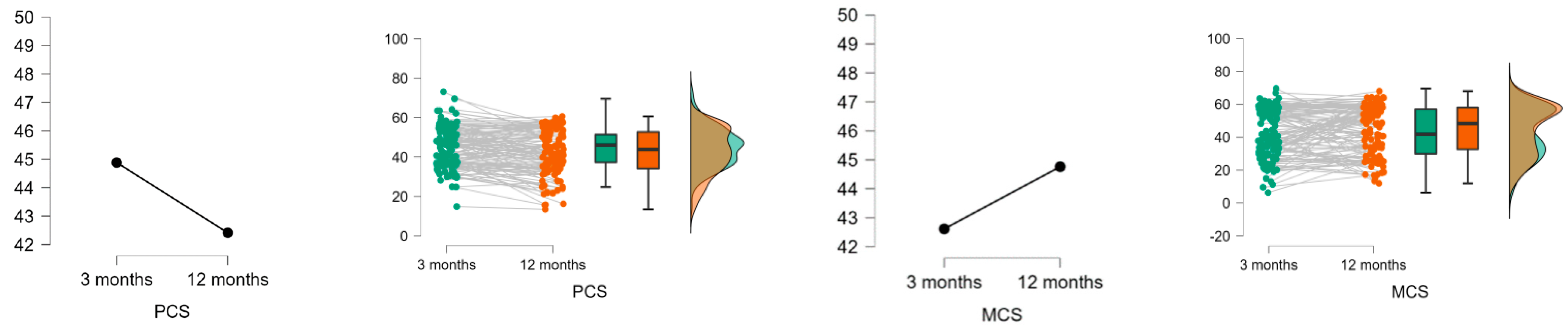
3.3. Evolution in HRQoL Scores in Patients with Post-COVID-19 Pneumonia at 3 and 12 Months after the Contagion
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 4 January 2022).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19). Outbreak in China: Summary of a Report of 72314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 23, 1239–1242. [Google Scholar] [CrossRef]
- Petrilli, C.M.; Jones, S.A. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: Prospective cohort study. BMJ 2020, 369, m1923. [Google Scholar] [CrossRef] [PubMed]
- Manual SEPAR. Available online: https://www.separ.es/node/2227 (accessed on 4 January 2022).
- Poudel, A.N.; Zhu, S.; Cooper, N.; Roderick, P.; Alwan, N. Impact of Covid-19 on health-related quality of life of patients: A structured review. PLoS ONE 2021, 10, e0259164. [Google Scholar] [CrossRef]
- Sanchez-Ramirez, D.; Normand, K.; Zhaoyun, Y.; Torres Castro, R. Long-Term Impact of COVID-19: A Systematic Review of the Literature and Meta-Analysis. Biomedicines 2021, 9, 900. [Google Scholar] [CrossRef] [PubMed]
- Van den Borst, B.; Peters, J.B.; Brink, M.; Schoon, Y.; Bleeker-Rovers, C.P.; Schers, H.; van Hees, H.W.H.; van Helvoort, H.; van den Boogaard, M.; van der Hoeven, H.; et al. Comprehensive Health Assessment 3 Months After Recovery from Acute Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2021, 73, 1089–1098. [Google Scholar] [CrossRef]
- Malik, P.; Patel, K.; Pinto, C.; Jaiswal, R.; Tirupathi, R.; Pillai, S.; Patel, U. Post-acute COVID-19 syndrome (PCS) and health-related quality of life (HRQoL)-A systematic review and meta-analysis. J. Med. Virol. 2021, 94, 253–262. [Google Scholar] [CrossRef]
- Hui, D.S.; Wong, K.T.; Ko, F.W.; Tam, L.S.; Chan, D.P.; Woo, J.; Sung, J.J. The 1-year impact of severe acute respiratory syndrome on pulmonary function, exercise capacity, and quality of life in a cohort of survivors. Chest 2005, 128, 2247–2261. [Google Scholar] [CrossRef] [Green Version]
- NICE. COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19; National Institute for Health and Care Excellence (NICE): London, UK, 2020. [Google Scholar]
- WHO. Support for Rehabilitation: Self-Management after COVID-19-Related Illness, 2nd ed.; WHO: Geneva, Switzerland, 2021. Available online: https://apps.who.int/iris/bitstream/handle/10665/344472/WHO-EURO-2021-855-40590-59892-eng.pdf?sequence=1&isAllowed=y (accessed on 7 August 2022).
- Alonso, J.; Regidor, E.; Barrio, J. Valores poblacionales de referencia de la versión española del Cuestionario de Salud SF-36. Med. Clin. 1998, 111, 410–416. [Google Scholar]
- Sibila, O.; Molina-Molina, M.; Valenzuela, C. Documento de consenso de la Sociedad Española de Neumología y Cirugía Torácica (SEPAR) para el seguimiento clínico post-COVID-19. Open Respir. Arch. 2020, 2, 278–283. [Google Scholar] [CrossRef]
- Warren, M.A.; Zhao, Z.; Koyama, T.; Bastarache, J.A.; Shaver, C.M.; Semler, M.W. Severity scoring of lung oedema on the chest radiograph is associated with clinical outcomes in ARDS. Thorax 2018, 73, 840–846. [Google Scholar] [CrossRef]
- Martínez Chamorro, E.; Díez Tascón, A.; Ibáñez Sanz, L.; Ossaba Vélez, S.; Borruel Nacenta, S. Radiologic diagnosis of patients with COVID-19. Diagnóstico radiológico del paciente con COVID-19. Radiologia 2021, 63, 56–73. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.; Prieto, L.; Anto, J.M. La versión española del SF-36 Health Survey (Cuestionario de Salud SF-36): Un instrumento para la medida de los resultados clínicos. Med. Clin. 1995, 104, 771–776. [Google Scholar]
- Vilaguta, V.; Ferrera, M.; Rajmi, L. El Cuestionario de Salud SF-36 español: Una década de experiencia y nuevos desarrollos. Gac. Sanit. 2005, 19, 135–150. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge Academic: New York, NY, USA, 1988. [Google Scholar]
- Van der Sar-van der Brugge, S.; Talman, S.; Boonman-de Winter, L.; de Mol, M.; Hoefman, E.; van Etten, R.W.; de Backer, I.C. Pulmonary function and health-related quality of life after COVID-19 pneumonia. Respir. Med. 2021, 176, 106272. [Google Scholar] [CrossRef] [PubMed]
- Valent, A.; Dudoignon, E.; Ressaire, Q.; Dépret, F.; Plaud, B. Three-month quality of life in survivors of ARDS due to COVID-19: A preliminary report from a French academic centre. Anaesth. Crit. Care Pain Med. 2020, 39, 740–741. [Google Scholar] [CrossRef]
- Aranda, J.; Oriol, I.; Martín, M.; Feria, L.; Vázquez, N.; Rhyman, N.; Vall-Llosera, E.; Pallarés, N.; Coloma, A.; Pestaña, M.; et al. Long-term impact of COVID-19 associated acute respiratory distress syndrome. J. Infect. 2021, 83, 581–588. [Google Scholar] [CrossRef]
- Eberst, G.; Claudé, F.; Laurent, L.; Meurisse, A.; Roux-Claudé, P.; Barnig, C.; Vernerey, D.; Paget-Bailly, S.; Bouiller, K.; Chirouze, C.; et al. Result of one-year, prospective follow-up of intensive care unit survivors after SARS-CoV-2 pneumonia. Ann. Intensive Care 2022, 12, 23. [Google Scholar] [CrossRef]
- Wu, X.; Liu, X.; Zhou, Y.; Yu, H.; Li, R.; Zhan, Q.; Ni, F.; Fang, S.; Lu, Y.; Ding, X.; et al. 3-month, 6-month, 9-month, and 12-month respiratory outcomes in patients following COVID-19-related hospitalisation: A prospective study. Lancet Respir. Med. 2021, 9, 747–754. [Google Scholar] [CrossRef]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 Long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef]
- Szcześniak, D.; Gładka, A.; Misiak, B.; Cyran, A.; Rymaszewska, J. The SARS-CoV-2 and mental health: From biological mechanisms to social consequences. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 104, 110046. [Google Scholar] [CrossRef]
- The Lancet. Facing up to long COVID. Lancet 2020, 396, 1861. [Google Scholar] [CrossRef]
- Rogers, J.P.; Chesney, E.; Oliver, D. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Patients (N = 305) Frequency (%) | Total Enrolled Patients (N = 130) Frequency (%) |
|---|---|---|
| Male | 157 (51.5%) | 63 (48.5%) |
| Female | 148 (48.5%) | 67 (51.5%) |
| Hypertension | 104 (34.1%) | 50 (38.5%) |
| Diabetes Mellitus | 34 (11.1%) | 13 (10.0%) |
| Pulmonary disease 1 | 50 (16.4%) | 20 (15.4%) |
| Immunosuppression | 13 (4.3%) | 7 (5.4%) |
| Obesity | 88 (28.9%) | 37 (28.5%) |
| Smoking history | 134 (43.9%) | 28 (21.5%) |
| Cough | 66 (21.6%) | 28 (21.5%) |
| Dyspnea | 100 (32.8%) | 48 (36.9%) |
| Asthenia | 102 (33.4%) | 47 (36.2%) |
| Myalgias-arthralgias | 56 (18.4%) | 25 (19.2%) |
| Anosmia-dysgeusia | 59 (19.3%) | 31 (23.8%) |
| Gastrointestinal disorders | 33 (10.8%) | 17 (13.1%) |
| Memory loss | 44 (14.4%) | 14 (10.8%) |
| Dermatological disorders | 25 (8.2%) | 12 (9.2%) |
| Headache | 55 (18.0%) | 20 (15.4%) |
| Visual loss | 15 (4.9%) | 7 (5.4%) |
| Back low pain | 11 (3.6%) | 6 (4.6%) |
| Crackles | 18 (5.9%) | 12 (9.2%) |
| Post-COVID-19 sequels | 31 (10.2%) | 27 (20.8%) |
| Characteristics | Total Patients (N = 305) Mean (SD) (Range) | Total Enrolled Patients (N = 130) Mean (SD) (Range) |
|---|---|---|
| Age, years | 54.7 (15.9) | 55.9 (15.9) |
| (18.0–89.0) | (18.0–88.0) | |
| Charlson Index | 1.9 (2.1) | 1.9 (1.8) |
| (0.0–11.0) | (0.0–9.0) | |
| Modified RALE score | 0.8 (1.5) | 1.1 (1.8) |
| (0.0–9.0) | (0.0–9.0) | |
| Pulmonary function | ||
| FVC, mL | 4027.5 (1177.2) | 3836.1 (1071.1) |
| (1450.0–7410.0) | (1550.0–7270.0) | |
| FVC, % | 111.6 (18.3) | 109.8 (17.2) |
| (64.7–161.1) | (64.9–150.6) | |
| FEV1, mL | 3104.3 (983.9) | 2989.2 (897.6) |
| (101.3–5770.0) | (940.0–5530.0) | |
| FEV1, % | 107.1 (20.1) | 106.1 (18.8) |
| (38.7–152.6) | (50.2–147.8) | |
| FEV1/FVC % | 77.0 (0.1) | 77.8 (8.9) |
| (45.0–122.0) | (54.0–122.0) |
| SF-36 Domains | General Population (N = 9151) | Overall Series (N = 130) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 3 Months | 12 Months | ||||||||||
| Mean (SD) (Range) | MD (SE) CI 95% | t | p | d | Mean (SD) (Range) | MD (SE) CI 95% | t | p | d | ||
| PF | 84.7 (24.0) (0.0–100.0) | 75.1 (23.1) (10.0–100.0) | −9.6 (2.1) (−13.8–5.4) | −4.5 | <0.001 | 0.4 | 70.7 (26.5) (0.0–100.0) | −14.0 (2.1) (−18.2–9.8) | −6.6 | <0.001 | 0.6 |
| RP | 83.2 (35.2) (0.0–100.0) | 38.8 (44.5) (0.0–100.0) | −44.4 (3.1) (−50.5–38.3) | −14.2 | <0.001 | 1.1 | 41.1 (42.9) (0.0–100.0) | −42.1 (3.1) (−48.2–36.0) | −13.5 | <0.001 | 1.0 |
| BP | 79.0 (27.9) (0.0–100.0) | 68.2 (27.3) (0.0–100.0) | −10.8 (2.5) (−15.6–6.0) | −4.4 | <0.001 | 0.4 | 60.6 (31.1) (0.0–100.0) | −18.4 (2.5) (−23.2–13.6) | −7.5 | <0.001 | 0.6 |
| GH | 68.3 (22.3) (0.0–100.0) | 63.3 (21.7) (15.0–100.0) | −5.0 (2.0) (−8.9–1.1) | −2.5 | 0.011 | 0.2 | 57.2 (24.3) (5.0–100.0) | −11.1 (1.9) (−15.0–7.2) | −5.6 | <0.001 | 0.5 |
| VT | 66.9 (22.1) (0.0–100.0) | 56.1 (27.3) (0.0–100.0) | −10.8 (2.0) (−14.6–6.9) | −5.5 | <0.001 | 0.4 | 54.7 (27.6) (0.0–100.0) | −12.2 (1.9) (−16.0–8.4) | −6.2 | <0.001 | 0.5 |
| SF | 90.1 (20.0) (0.0–100.0) | 69.7 (29.8) (0.0–100.0) | −20.4 (1.8) (−23.9–16.9) | −11.5 | <0.001 | 0.8 | 74.5 (29.0) (0.0–100.0) | −15.6 (1.8) (−19.0–12.1) | −8.8 | <0.001 | 0.6 |
| RE | 88.6 (30.1) (0.0–100.0) | 50.7 (46.5) (0.0–100.0) | −37.9 (2.7) (−43.2–32.6) | −14.2 | <0.001 | 1.0 | 56.7 (46.7) (0.0–100.0) | −31.9 (2.7) (−37.2–26.6) | −11.9 | <0.001 | 0.8 |
| MH | 73.3 (20.1) (0.0–100.0) | 68.6 (24.1) (0.0–100.0) | −4.7 (1.8) (−8.2–1.2) | −2.6 | 0.008 | 0.2 | 70.1 (23.8) (4.0–100.0) | −3.2 (1.78) (−6.7–0.3) | −1.8 | 0.072 | 0.1 |
| SF-36 Domains | t | p | CI95% | d |
|---|---|---|---|---|
| PF | −0.594 | 0.554 | −9.99 to 5.38 | −0.005 |
| RP | 0.717 | 0.474 | −2.82 to 6.02 | 0.05 |
| BP | −1.87 | 0.064 | −9.89 to 0.28 | −0.16 |
| GH | −1.368 | 0.174 | −15.66 to 2.86 | 0.13 |
| VT | −0.648 | 0.518 | −5.36 to 2.70 | −0.06 |
| SF | 2.495 | 0.014 | 0.89 to 7.78 | 0.17 |
| RE | 2.595 | 0.011 | 1.68 to 12.49 | 0.25 |
| MH | 3.215 | 0.002 | 2.16 to 9.07 | 0.26 |
| PCS | 2.981 | 0.003 | 0.088 to 0.448 | 0.269 |
| MCS | −1.606 | 0.111 | −0.322 to 0.033 | −0.145 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Galán, I.; Albaladejo-Blázquez, N.; Ruiz-Robledillo, N.; Pascual-Lledó, J.F.; Ferrer-Cascales, R.; Gil-Carbonell, J. Impact of COVID-19 on Health-Related Quality of Life: A Longitudinal Study in a Spanish Clinical Sample. Int. J. Environ. Res. Public Health 2022, 19, 10421. https://doi.org/10.3390/ijerph191610421
Rodríguez-Galán I, Albaladejo-Blázquez N, Ruiz-Robledillo N, Pascual-Lledó JF, Ferrer-Cascales R, Gil-Carbonell J. Impact of COVID-19 on Health-Related Quality of Life: A Longitudinal Study in a Spanish Clinical Sample. International Journal of Environmental Research and Public Health. 2022; 19(16):10421. https://doi.org/10.3390/ijerph191610421
Chicago/Turabian StyleRodríguez-Galán, Irene, Natalia Albaladejo-Blázquez, Nicolás Ruiz-Robledillo, José Francisco Pascual-Lledó, Rosario Ferrer-Cascales, and Joan Gil-Carbonell. 2022. "Impact of COVID-19 on Health-Related Quality of Life: A Longitudinal Study in a Spanish Clinical Sample" International Journal of Environmental Research and Public Health 19, no. 16: 10421. https://doi.org/10.3390/ijerph191610421
APA StyleRodríguez-Galán, I., Albaladejo-Blázquez, N., Ruiz-Robledillo, N., Pascual-Lledó, J. F., Ferrer-Cascales, R., & Gil-Carbonell, J. (2022). Impact of COVID-19 on Health-Related Quality of Life: A Longitudinal Study in a Spanish Clinical Sample. International Journal of Environmental Research and Public Health, 19(16), 10421. https://doi.org/10.3390/ijerph191610421