
The Effects of a Multicomponent Social Support Intervention on Physical Fitness and Exercise Attitude in Children: A 12-Week Randomized Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
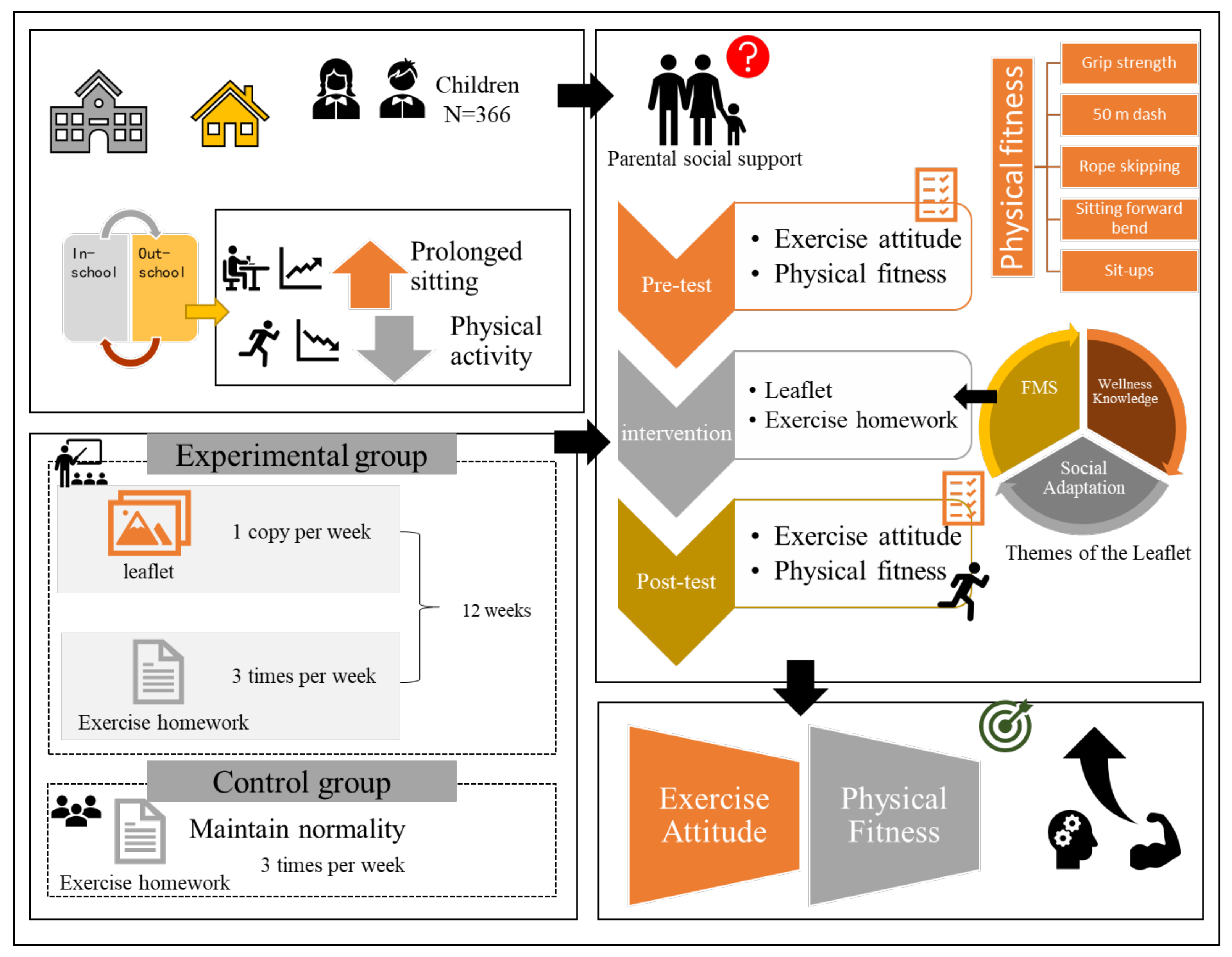
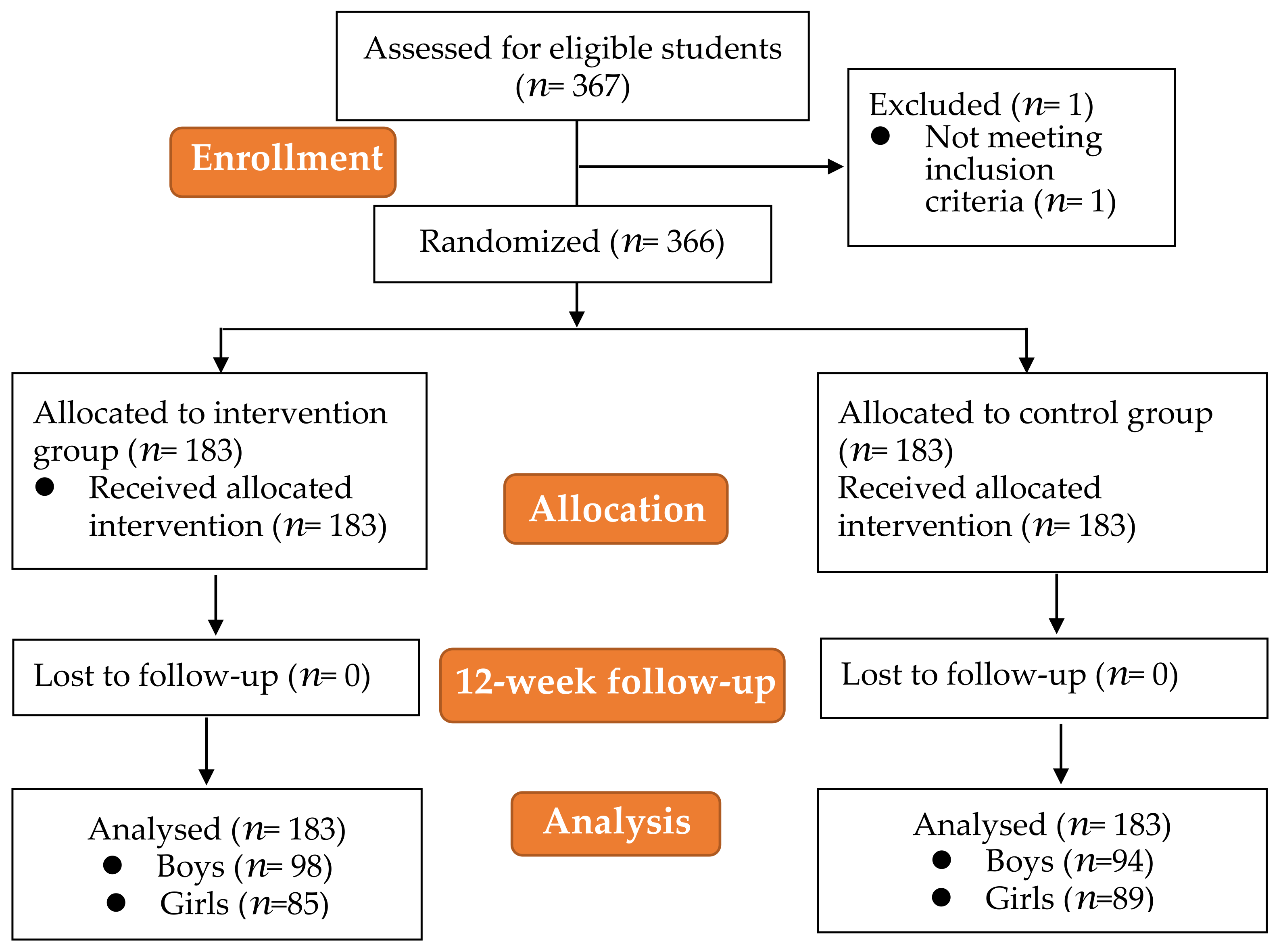
2.1. Study Design
2.2. Participants
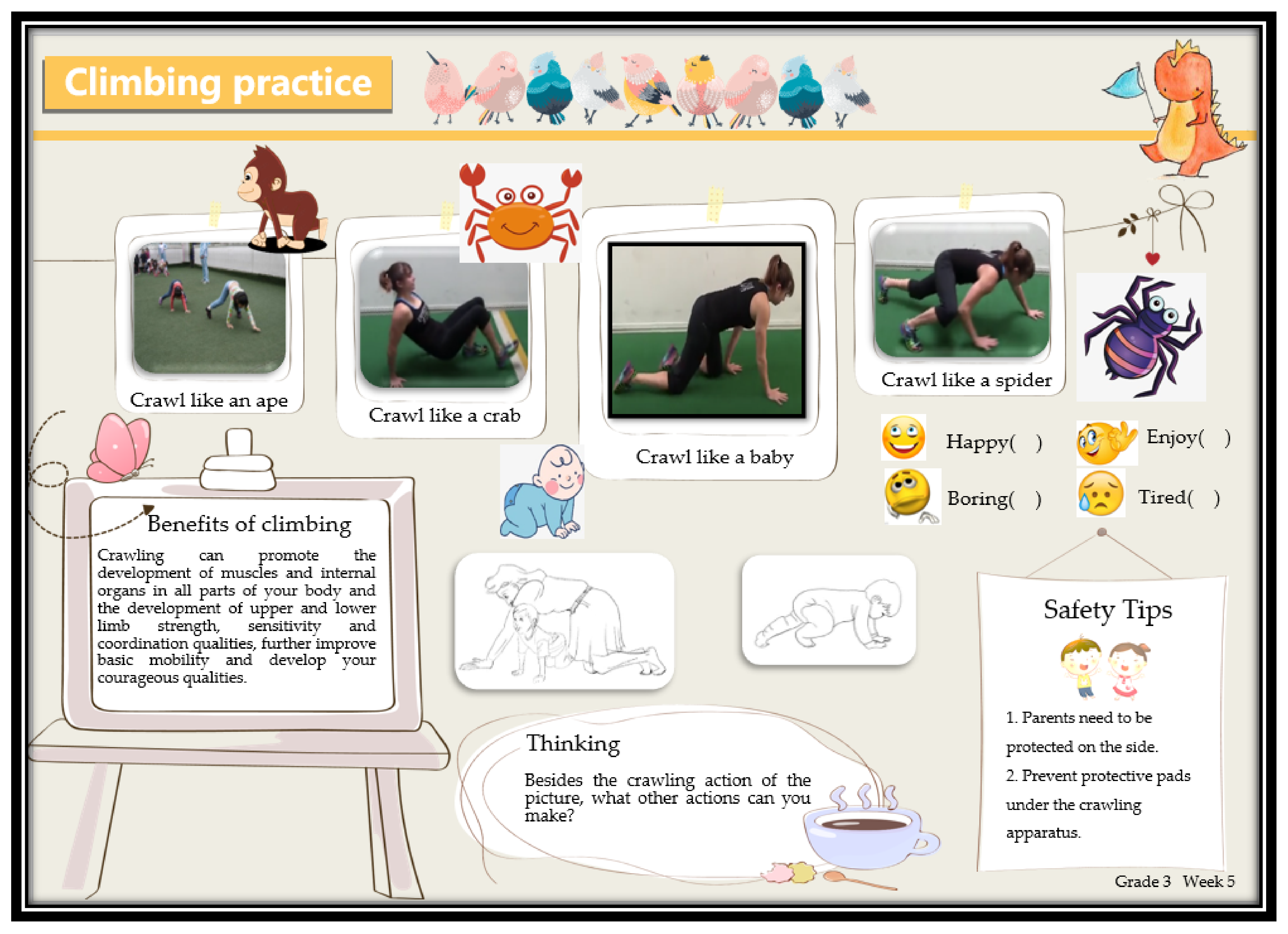
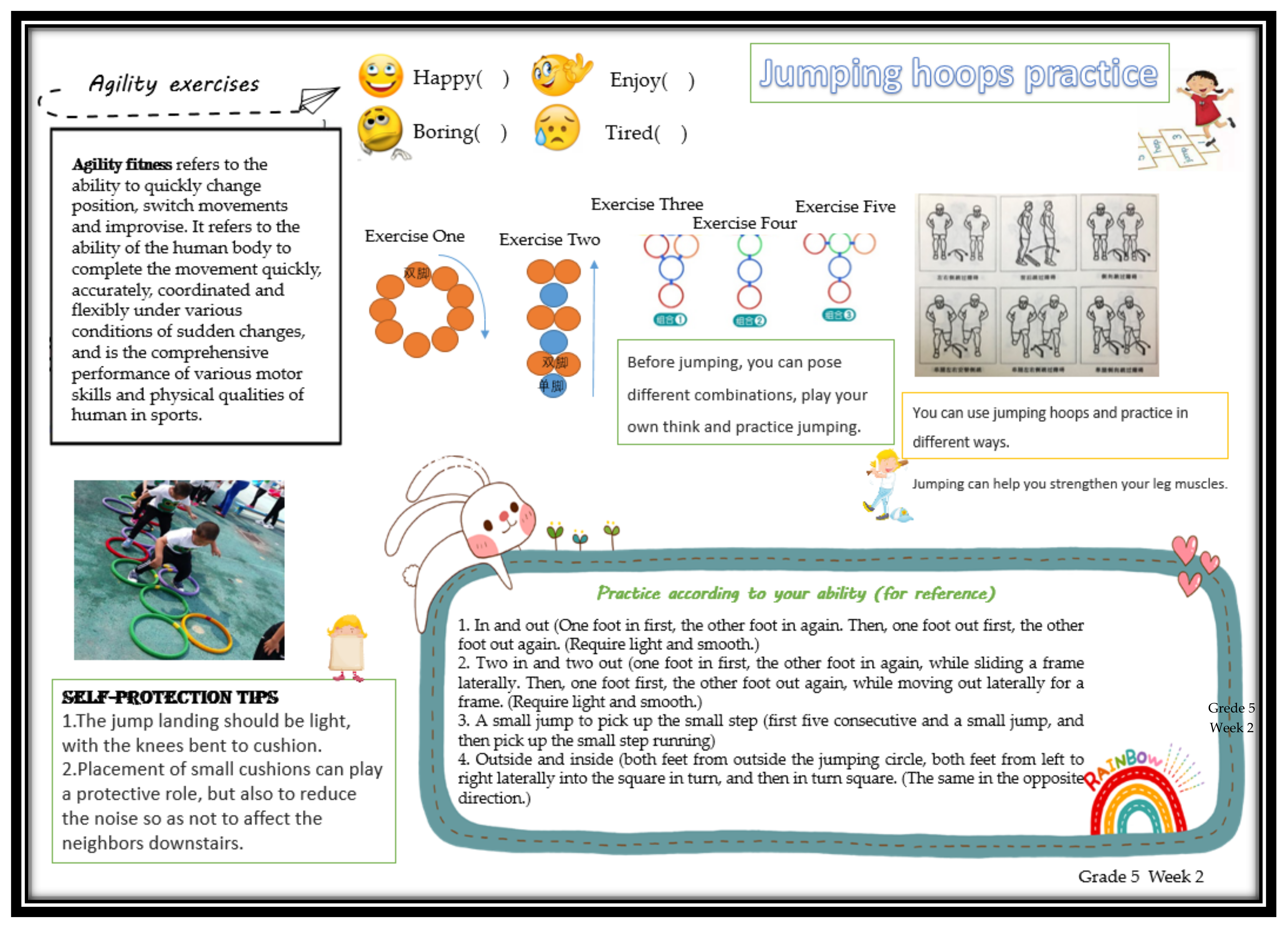
2.3. Intervention
2.4. Measurements
2.4.1. Exercise Attitude Test
2.4.2. Physical Fitness Test
2.5. Statistical Procedures
3. Results
3.1. Differences between Children in the Intervention and Control Groups at Baseline
3.2. Effects of Intervention on Childrens’ Physical Fitness
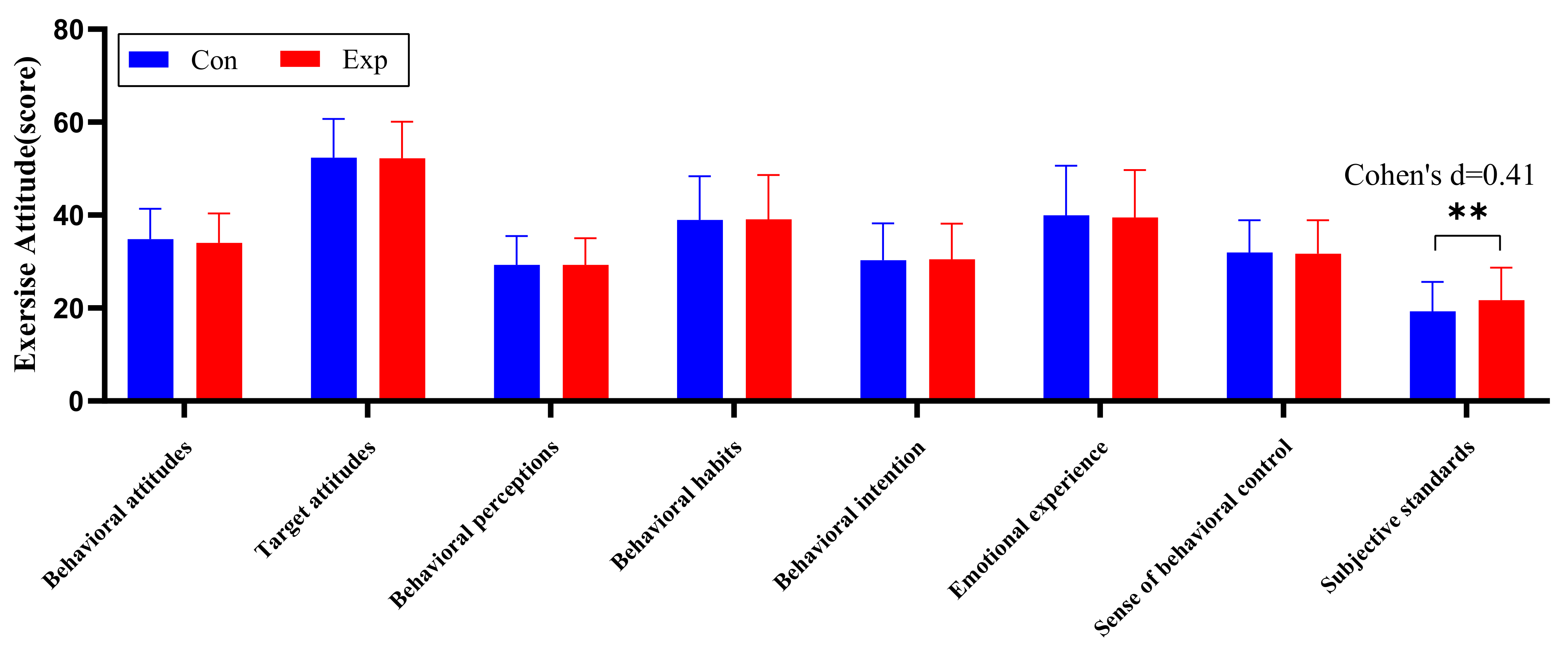
3.3. Effects of Intervention on Childrens’ Exercise Attitudes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Danqing, Z.; Yingli, L.; Yang, L. Factors influencing physical activity and static lifestyle—A systematic review based on our children and adolescents. China Sport Sci. 2019, 39, 62–75. [Google Scholar] [CrossRef]
- Telama, R.; Yang, X.; Viikari, J.; Välimäki, I.; Wanne, O.; Raitakari, O. Physical activity from childhood to adulthood: A 21-year tracking study. Am. J. Prev. Med. 2005, 28, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [PubMed]
- Chao, W.; Gang, H.; Xiaohong, C. The relationship between spatial characteristics of fitness venues and physical activity of adolescents—An empirical study based on GIS and accelerometers. J. Shanghai Univ. Sport 2018, 42, 36–43. [Google Scholar] [CrossRef]
- Silva, D.A.S.; Chaput, J.-P.; Katzmarzyk, P.T.; Fogelholm, M.; Hu, G.; Maher, C.; Olds, T.; Onywera, V.; Sarmiento, O.L.; Standage, M.; et al. Participation In Physical Education Classes And Physical Activity And Sedentary Behavior in Children: 1886 Board #147 May 31 2: 00 PM–3: 30 PM. Med. Sci. Sports Exerc. 2018, 50, 452. [Google Scholar] [CrossRef]
- Steele, R.M.; van Sluijs, E.M.; Sharp, S.J.; Landsbaugh, J.R.; Ekelund, U.; Griffin, S.J. An investigation of patterns of children’s sedentary and vigorous physical activity throughout the week. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 88. [Google Scholar] [CrossRef]
- Long, M.W.; Sobol, A.M.; Cradock, A.L.; Subramanian, S.V.; Blendon, R.J.; Gortmaker, S.L. School-day and overall physical activity among youth. Am. J. Prev. Med. 2013, 45, 150–157. [Google Scholar] [CrossRef]
- Hubbard, K.; Economos, C.D.; Bakun, P.; Boulos, R.; Chui, K.; Mueller, M.P.; Smith, K.; Sacheck, J. Disparities in moderate-to-vigorous physical activity among girls and overweight and obese schoolchildren during school- and out-of-school time. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 39. [Google Scholar] [CrossRef]
- Kipping, R.R.; Howe, L.D.; Jago, R.; Campbell, R.; Wells, S.; Chittleborough, C.R.; Mytton, J.; Noble, S.M.; Peters, T.J.; Lawlor, D.A. Effect of intervention aimed at increasing physical activity, reducing sedentary behaviour, and increasing fruit and vegetable consumption in children: Active for Life Year 5 (AFLY5) school based cluster randomised controlled trial. BMJ 2014, 348, g3256. [Google Scholar] [CrossRef]
- van Sluijs, E.M.; McMinn, A. Preventing obesity in primary schoolchildren. BMJ 2010, 340, c819. [Google Scholar] [CrossRef]
- van Sluijs, E.M.; McMinn, A.M.; Griffin, S.J. Effectiveness of interventions to promote physical activity in children and adolescents: Systematic review of controlled trials. BMJ 2007, 335, 703. [Google Scholar] [CrossRef]
- Brown, H.E.; Atkin, A.J.; Panter, J.; Wong, G.; Chinapaw, M.J.; van Sluijs, E.M. Family-based interventions to increase physical activity in children: A systematic review, meta-analysis and realist synthesis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2016, 17, 345–360. [Google Scholar] [CrossRef]
- Chen, J.L.; Weiss, S.; Heyman, M.B.; Vittinghoff, E.; Lustig, R. Pilot study of an individually tailored educational program by mail to promote healthy weight in Chinese American children. J. Spec. Pediatric Nurs. JSPN 2008, 13, 212–222. [Google Scholar] [CrossRef]
- Beech, B.M.; Klesges, R.C.; Kumanyika, S.K.; Murray, D.M.; Klesges, L.; McClanahan, B.; Slawson, D.; Nunnally, C.; Rochon, J.; McLain-Allen, B.; et al. Child- and parent-targeted interventions: The Memphis GEMS pilot study. Ethn. Dis. 2003, 13, S40–S53. [Google Scholar]
- Pittman, A.F. Effect of a School-Based Activity Tracker, Companion Social Website, and Text Messaging Intervention on Exercise, Fitness, and Physical Activity Self-Efficacy of Middle School Students. J. Sch. Nurs. 2020, 36, 112–120. [Google Scholar] [CrossRef]
- Dishman, R.K.; Buckworth, J. Increasing physical activity: A quantitative synthesis. Med. Sci. Sports Exerc. 1996, 28, 706–719. [Google Scholar] [CrossRef]
- Noar, S.M.; Benac, C.N.; Harris, M.S. Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychol. Bull. 2007, 133, 673–693. [Google Scholar] [CrossRef]
- Arredondo, E.M.; Morello, M.; Holub, C.; Haughton, J. Feasibility and preliminary findings of a church-based mother-daughter pilot study promoting physical activity among young Latinas. Fam. Community Health 2014, 37, 6–18. [Google Scholar] [CrossRef]
- Cobb, S. Social Support as a Moderator of Life Stress. Psychosom. Med. 1976, 38, 300–314. [Google Scholar] [CrossRef]
- Dishman, R.K.; Dunn, A.L.; Sallis, J.F.; Vandenberg, R.J.; Pratt, C.A. Social-cognitive correlates of physical activity in a multi-ethnic cohort of middle-school girls: Two-year prospective study. J. Pediatric Psychol. 2010, 35, 188–198. [Google Scholar] [CrossRef]
- Bradley, R.H.; McRitchie, S.; Houts, R.M.; Nader, P.; O’Brien, M. Parenting and the decline of physical activity from age 9 to 15. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 33. [Google Scholar] [CrossRef]
- Mendonca, G.; Cheng, L.A.; Melo, E.N.; De Farias Junior, J.C. Physical activity and social support in adolescents: A systematic review. Health Educ. Res. 2014, 29, 822–839. [Google Scholar] [CrossRef]
- Davison, K.K.; Jago, R. Change in parent and peer support across ages 9 to 15 yr and adolescent girls’ physical activity. Med. Sci. Sports Exerc. 2009, 41, 1816–1825. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, R.E.; Perdew, M.; Malli, S. Correlates of Parental Support of Child and Youth Physical Activity: A Systematic Review. Int. J. Behav. Med. 2020, 27, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Qiang, G.; Xiaozan, W. Characterization and Cognitive Reconstruction of Sedentary Behavior: A Public Health Observation Based on Changes in Human Behavior Patterns. J. Phys. Educ. 2021, 28, 137–144. [Google Scholar] [CrossRef]
- Ministry of Education of the People’s Republic of China. Physical Education and Health Curriculum Standards for Compulsory Education (2022 Edition). Available online: http://www.moe.gov.cn/srcsite/A26/s8001/202204/W020220420582362336303.pdf (accessed on 31 May 2022).
- Duncan, S.; McPhee, J.C.; Schluter, P.J.; Zinn, C.; Smith, R.; Schofield, G. Efficacy of a compulsory homework programme for increasing physical activity and healthy eating in children: The healthy homework pilot study. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 127. [Google Scholar] [CrossRef] [PubMed]
- Xiumei, Q.; Jianguo, T.; Huanbin, Z. Reflections on physical education for primary and secondary school students based on the concept of human movement development. J. Phys. Educ. 2010, 17, 80–82. [Google Scholar] [CrossRef]
- Rongjian, M. Development and Testing of a Nine-Factor Model of Adolescent Students’ Exercise Attitude-Behavior; Beijing Sport University: Beijing, China, 2003. [Google Scholar]
- Lu, Y.; Yu, K.; Gan, X. Effects of a SMART Goal Setting and 12-Week Core Strength Training Intervention on Physical Fitness and Exercise Attitudes in Adolescents: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 7715. [Google Scholar] [CrossRef]
- Rausch, J.R.; Maxwell, S.E.; Kelley, K. Analytic Methods for Questions Pertaining to a Randomized Pretest, Posttest, Follow-Up Design. J. Clin. Child Adolesc. Psychol. 2003, 32, 467–486. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Psychology Press: London, UK, 1988. [Google Scholar]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Processes 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Latimer, A.E.; Ginis, K.A.M. The importance of subjective norms for people who care what others think of them. Psychol. Health 2005, 20, 53–62. [Google Scholar] [CrossRef]
- Mahama, I.; Regine, K.; Amponsah, M.; Ansu. Head Teachers’ Perception of the Influence of Their Role Behaviours on Students Academic Performance in the Berekum Municipality; University of Cape Coast: Cape Coast, Ghana, 2018; Volume 6, pp. 10–30. [Google Scholar]
- Rhodes, R.E.; Berry, T.; Faulkner, G.; Latimer-Cheung, A.E.; O’Reilly, N.; Tremblay, M.S.; Vanderloo, L.; Spence, J.C. Application of the Multi-Process Action Control Framework to Understand Parental Support of Child and Youth Physical Activity, Sleep, and Screen Time Behaviours. Appl. Psychol. Health Well-Being 2019, 11, 223–239. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Rebar, A.L. Conceptualizing and Defining the Intention Construct for Future Physical Activity Research. Exerc. Sport Sci. Rev. 2017, 45, 209–216. [Google Scholar] [CrossRef]
- Rhodes, R.E.; de Bruijn, G.-J. How big is the physical activity intention–behaviour gap? A meta-analysis using the action control framework. Br. J. Health Psychol. 2013, 18, 296–309. [Google Scholar] [CrossRef]
- Arokiasamy, P.; Selvamani, Y. Age, socioeconomic patterns and regional variations in grip strength among older adults (50+) in India: Evidence from WHO’s Study on Global Ageing and Adult Health (SAGE). Arch. Gerontol. Geriatr. 2018, 76, 100–105. [Google Scholar] [CrossRef]
- Peterson, M.D.; Gordon, P.M.; Smeding, S.; Visich, P. Grip Strength Is Associated with Longitudinal Health Maintenance and Improvement in Adolescents. J. Pediatrics 2018, 202, 226–230. [Google Scholar] [CrossRef]
- Rhodes, R.; Quinlan, A.; Naylor, P.; Warburton, D.; Blanchard, C. Predicting Family and Child Physical Activity across Six-Months of a Family-Based Intervention: An Application of Theory of Planned Behaviour, Planning and Habit. J. Sports Sci. 2021, 39, 1461–1471. [Google Scholar] [CrossRef]
- Pezzoli, A.; Cristofori, E. Climatological Analysis, Weather Forecast and Sport Performance: Which are the Connections? J. Climatol. Weather Forecast. 2016, 1, 1000e105. [Google Scholar] [CrossRef]
- Thornes, J.E. The effect of weather on sport. Weather 1977, 32, 258–268. [Google Scholar] [CrossRef]
- Pezzoli, A.; Matteo, M.; Boscolo, A.; Cristofori, E.I.; Giacometto, F.; Gastaldi, S.; Vercelli, G. The meteo-hydrological analysis and the sport performance: Which are the connections? The case of the XXI Winter Olympic Games, Vancouver 2010. J. Sports Med. Phys. Fit. 2010, 50, 19–20. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Social Support | Contents | Elements of the Intervention |
|---|---|---|
| Emotional support | ||
| The provision of love, trust, care, etc. |
| |
| Instrumental Support | ||
| Providing direct and practical help and necessary services |
| |
| Informational Support | ||
| Providing consultation, advice, information, etc. on available problems to be solved |
| |
| Evaluation Support | ||
| Feedback, affirmation, and comparative information to facilitate self-evaluation |
|
| Theme | Content |
|---|---|
| FMS (Fundamental Movement Skill) |
|
| Wellness knowledge |
|
| Social adaptation |
|
| Intervention Group n = 183 | Control Group n = 183 | Total n = 366 | p | |
|---|---|---|---|---|
| Grade | ||||
| 7 | 94 (51.4%) | 92 (50.3%) | 186 | 0.792 |
| 8 | 89 (48.6%) | 91 (49.7%) | 180 | |
| Gender | ||||
| Boys | 98 (53.6%) | 94 (51.4%) | 183 | 0.445 |
| Girls | 85 (46.4%) | 89 (48.6%) | 183 | |
| Hight (cm) | 139.94 (8.95) | 139.84 (9.11) | 139.89 (9.02) | 0.791 |
| Weight (kg) | 33.00 (8.07) | 33.23 (8.27) | 33.11 (8.16) | 0.525 |
| BMI (kg/m2) | 16.66 (2.69) | 16.79 (2.69) | 16.73 (2.69) | 0.795 |
| Age (year) | ||||
| Age, Mean (SD) | 9.37 (1.14) | 9.33 (1.11) | 9.35 (1.12) | 0.584 |
| 8 | 60 (33.3%) | 60 (32.8%) | ||
| 9 | 31 (16.9%) | 32 (17.5%) | ||
| 10 | 60 (32.8%) | 54 (29.5%) | ||
| 11 | 31 (16.9%) | 37 (20.2%) |
| Week | Grade 3 | Grade 5 |
|---|---|---|
| 1 | Various running exercises | Speed quality exercises |
| 2 | Various jumping exercises | Agility exercises |
| 3 | Flexibility exercises | Flexibility exercises |
| 4 | Throwing exercises | Strength exercises (I) |
| 5 | Climbing exercises | Strength exercises (II) |
| 6 | Catching exercises | Endurance exercises |
| 7 | Exercise and nutrition | Develop a personal fitness program |
| 8 | Exercise and weight | Exercise and weight |
| 9 | Exercise and disease prevention | Exercise and disease prevention |
| 10 | Exercise and eyes health | Exercise and eye health |
| 11 | Exercise and safety | Exercise and injury (self-protection) |
| 12 | Exercise and social adaptation | Building good body shape and body posture |
| Variables | Exp | Con | ||||
|---|---|---|---|---|---|---|
| Pre | Post | d | Pre | Post | d | |
| Left-hand grip strength (kg) | 8.62, 3.34 | 8.94, 3.39 | 0.10 * | 8.72, 3.18 | 8.89, 4.09 | 0.05 |
| Right-hand grip strength (kg) | 9.52, 3.55 | 9.83, 3.61 | 0.09 * | 9.98, 3.31 | 9.73, 3.89 | 0.07 |
| 50 m (s) | 10.14, 1.05 | 10.14, 1.14 | <0.01 | 9.95, 0.89 | 10.14, 1.12 | 0.19 ** |
| Rope-skipping (pcs) | 178.23, 20.57 | 176.93, 21.23 | 0.06 | 182.32, 18.42 | 182.41, 22.02 | <0.01 |
| Sit-ups (pcs) | 42.02, 11.97 | 41.24, 10.30 | 0.07 | 42.87, 12.15 | 41.20, 11.32 | 0.14 * |
| Sit-and-reach (cm) | 16.16, 5.05 | 14.58, 5.43 | 0.3 *** | 15.60, 5.14 | 13.06, 5.89 | 0.46 *** |
| Variables | Group | Gender | Interaction Effects | PairwiseComparison | |||
|---|---|---|---|---|---|---|---|
| F | η2p | F | η2p | F | η2p | (Post) | |
| Left-hand grip strength (kg) | 0.229 | 0.001 | 1.266 | 0.004 | 2.082 | 0.006 | —— |
| Right-hand grip strength (kg) | 7.109 | 0.020 *** | 2.194 | 0.006 | 2.083 | 0.006 | Exp > Con |
| 50 m (s) | 1.678 | 0.005 | 2.060 | 0.006 | 0.024 | <0.001 | —— |
| Rope-skipping (pcs) | 2.997 | 0.008 | 15.007 | 0.041 *** | <0.001 | <0.001 | —— |
| Sit-ups (pcs) | 0.215 | 0.001 | 1.932 | 0.005 | 1.169 | 0.003 | —— |
| Sit-and-reach (cm) | 11.255 | 0.031 *** | 17.720 | 0.048 *** | 3.273 | 0.009 | Exp > Con |
| Variables | Exp | Con | ||||
|---|---|---|---|---|---|---|
| [Score] | Pre | Post | d | Pre | Post | d |
| Behavioral attitudes | 34.53, 5.27 | 34.05, 6.34 | 0.08 | 35.76, 4.47 | 34.84, 6.51 | 0.16 |
| Target attitudes | 53.02, 6.60 | 52.24, 7.89 | 0.11 | 54.58, 6.62 | 52.36, 8.33 | 0.30 *** |
| Behavioral perceptions | 28.78, 5.81 | 29.27, 5.75 | 0.08 | 30.68, 4.52 | 29.27, 6.25 | 0.26 ** |
| Behavioral habits | 38.30, 8.66 | 39.13, 9.50 | 0.09 | 39.56, 8.24 | 38.94, 9.43 | 0.07 |
| Behavioral intention | 29.22, 7.62 | 30.53, 7.62 | 0.17 ** | 30.55, 7.06 | 30.28, 7.93 | 0.04 |
| Emotional experience | 39.11, 9.30 | 39.50, 10.17 | 0.04 | 40.94, 8.85 | 39.97, 10.66 | 0.10 |
| Sense of behavioral control | 32.26, 6.50 | 31.70, 7.22 | 0.08 | 33.07, 6.02 | 31.98, 6.93 | 0.17 * |
| Subjective standards | 20.71, 5.99 | 21.71, 6.96 | 0.15 | 21.14, 6.23 | 19.28, 6.34 | 0.30 *** |
| Variables [Score] | Group | Gender | Interaction effects | PairwiseComparison | |||
|---|---|---|---|---|---|---|---|
| F | η2p | F | η2p | F | η2p | Post | |
| Behavioral attitudes | 0.015 | <0.001 | 0.074 | <0.001 | 0.463 | 0.001 | —— |
| Target attitudes | 0.977 | 0.003 | 0.019 | <0.001 | 1.205 | 0.004 | —— |
| Behavioral perceptions | 3.192 | 0.009 | 0.013 | <0.001 | 0.382 | 0.001 | —— |
| Behavioral habits | 2.400 | 0.007 | 0.610 | 0.002 | 1.160 | 0.003 | —— |
| Behavioral intention | 3.642 | 0.011 | 0.859 | 0.003 | 0.220 | 0.001 | —— |
| Emotional experience | 0.541 | 0.002 | 0.007 | <0.001 | 0.900 | 0.003 | —— |
| Sense of behavioral control | 0.036 | <0.001 | 0.026 | <0.001 | 0.161 | <0.001 | —— |
| Subjective standards | 15.461 | 0.043 *** | 5.518 | 0.016 * | 0.542 | 0.002 | Exp > Con |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, Y.; Yu, K.; Jin, J.; Gan, X. The Effects of a Multicomponent Social Support Intervention on Physical Fitness and Exercise Attitude in Children: A 12-Week Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 9922. https://doi.org/10.3390/ijerph19169922
Lu Y, Yu K, Jin J, Gan X. The Effects of a Multicomponent Social Support Intervention on Physical Fitness and Exercise Attitude in Children: A 12-Week Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(16):9922. https://doi.org/10.3390/ijerph19169922
Chicago/Turabian StyleLu, Yijuan, Kehong Yu, Jun Jin, and Xiaomei Gan. 2022. "The Effects of a Multicomponent Social Support Intervention on Physical Fitness and Exercise Attitude in Children: A 12-Week Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 16: 9922. https://doi.org/10.3390/ijerph19169922
APA StyleLu, Y., Yu, K., Jin, J., & Gan, X. (2022). The Effects of a Multicomponent Social Support Intervention on Physical Fitness and Exercise Attitude in Children: A 12-Week Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(16), 9922. https://doi.org/10.3390/ijerph19169922