
Applicability and Psychometric Comparison of the General-Population Viral Anxiety Rating Scales among Healthcare Workers in the COVID-19 Pandemic

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sampling Procedure
2.3. Measures
2.3.1. Stress and Anxiety to Viral Epidemics—9 Items and —6 Items (SAVE-9 and SAVE-6)
2.3.2. Coronavirus Anxiety Scale (CAS)
2.3.3. Fear of COVID-19 Scale (FCV-19S)
2.3.4. COVID-19 Anxiety Scale (CAS-7)
2.3.5. Generalized Anxiety Disorder-7 Items (GAD-7)
2.4. Statistical Analysis
3. Results
3.1. Reliability and Validity of the SAVE-9, SAVE-6, CAS, FCV-19S, and CAS-7 Scales among Healthcare Workers
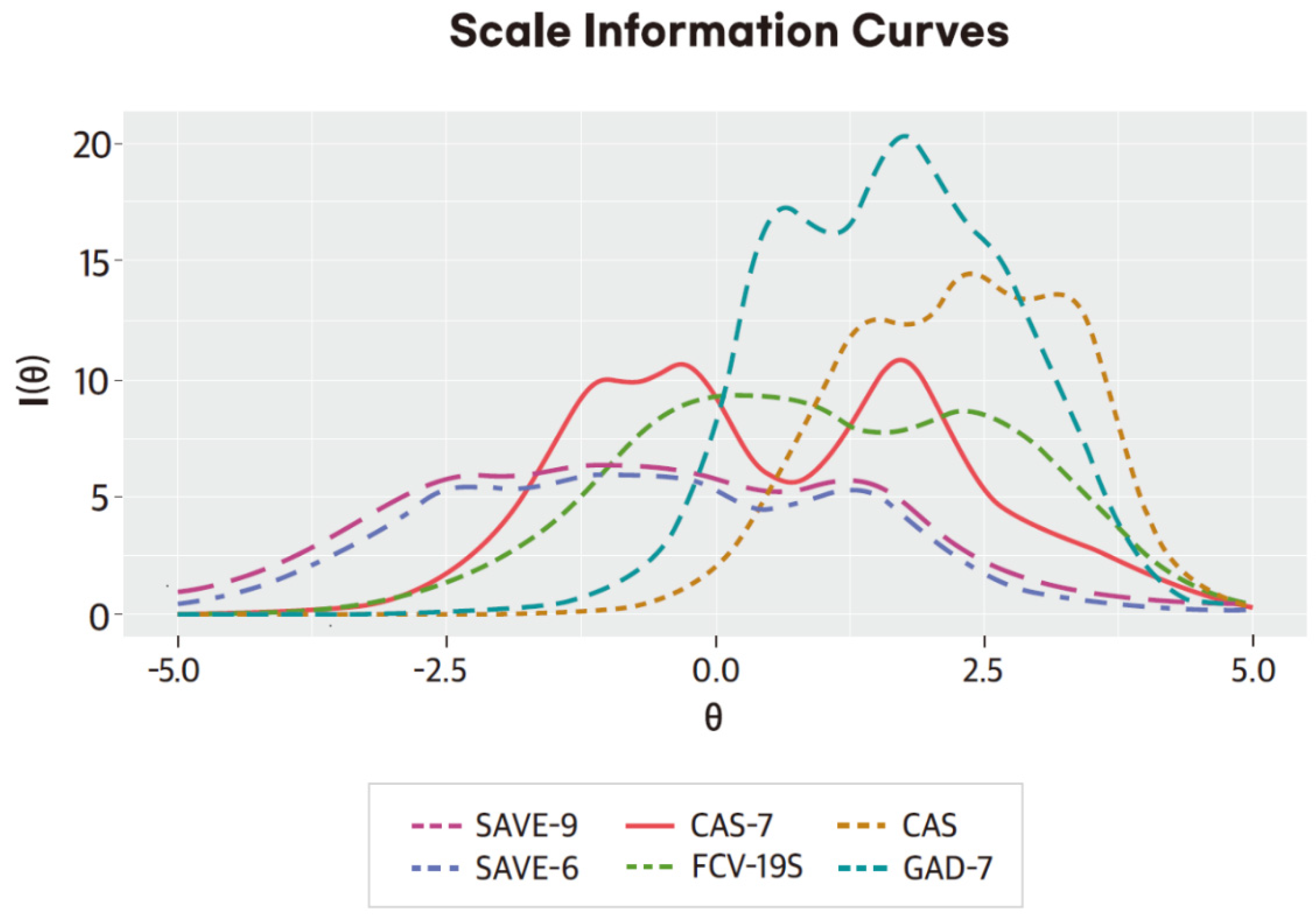
3.2. Graded Response Model
3.3. Rasch Analysis
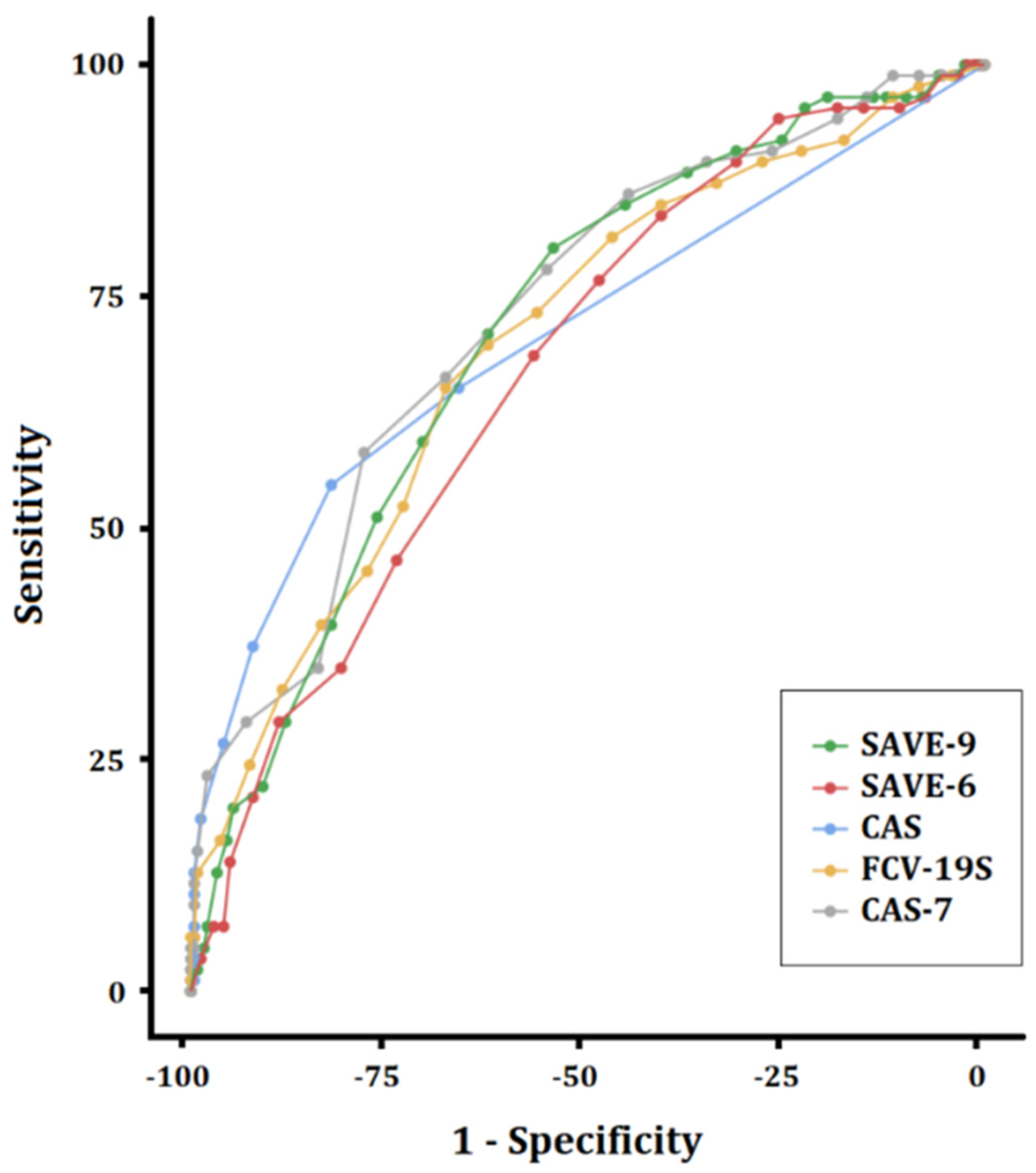
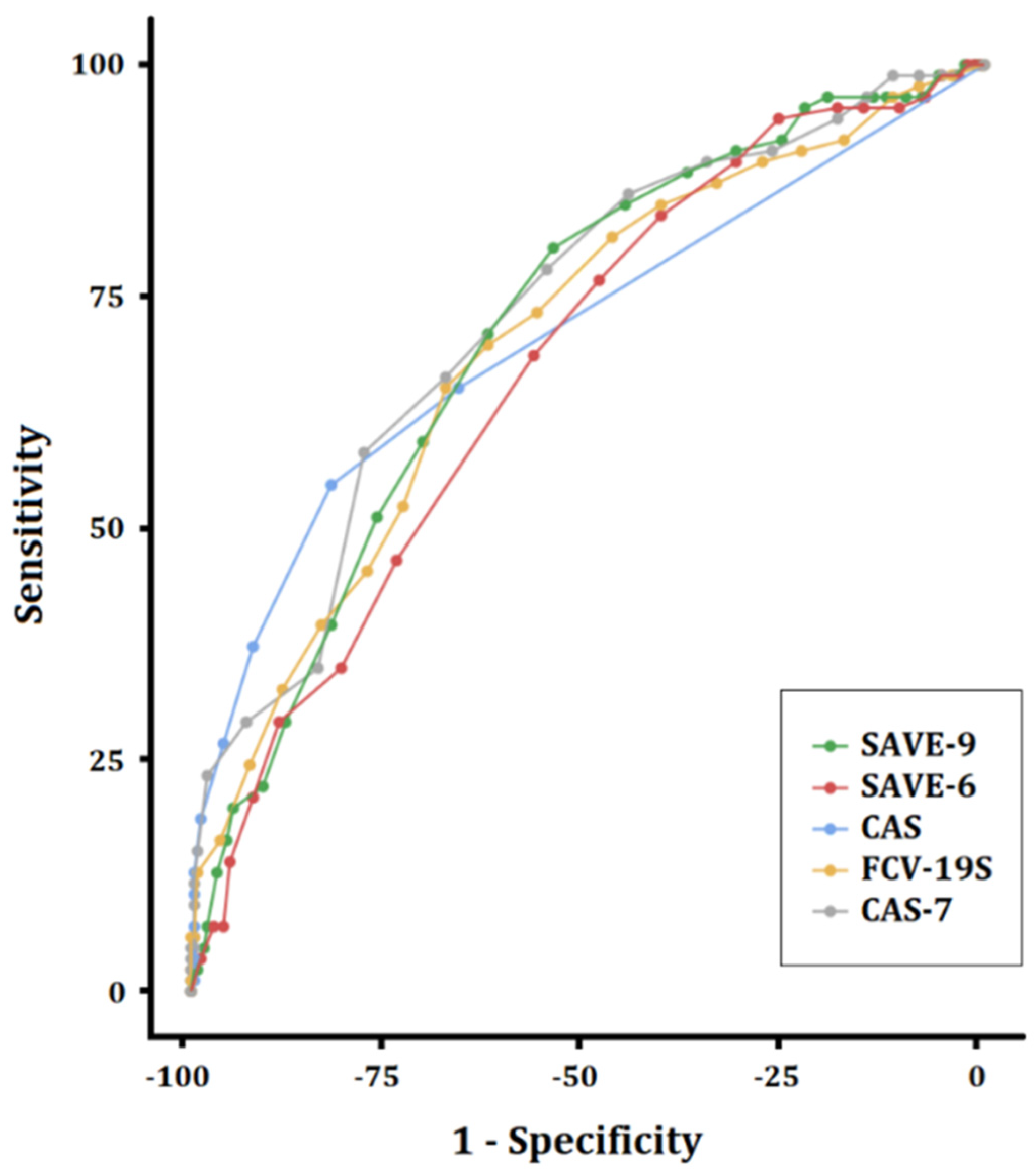
3.4. Comparison of the Psychometric Properties of the SAVE-9 with Other Viral Anxiety Rating Scales among Healthcare Workers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vizheh, M.; Qorbani, M.; Arzaghi, S.M.; Muhidin, S.; Javanmard, Z.; Esmaeili, M. The mental health of healthcare workers in the COVID-19 pandemic: A systematic review. J. Diabetes Metab. Disord. 2020, 20, 1967–1978. [Google Scholar] [CrossRef]
- Bhadoria, P.; Gupta, G.; Agarwal, A. Viral pandemics in the past two decades: And overview. J. Fam. Med. Prim. Care 2021, 10, 2745–2750. [Google Scholar] [CrossRef] [PubMed]
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 1 July 2022).
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef]
- Thomas, J.; Barbato, M.; Verlinden, M.; Gaspar, C.; Moussa, M.; Ghorayeb, J.; Menon, A.; Figueiras, M.J.; Arora, T.; Bentall, R.P. Psychosocial correlates of depression and anxiety in the United Arab Emirates during the COVID-19 pandemic. Front. Psychiatry 2020, 11, 564172. [Google Scholar] [CrossRef] [PubMed]
- Fioravanti, G.; Bocci Benucci, S.; Prostamo, A.; Banchi, V.; Casale, S. Effects of the COVID-19 pandemic on psychological health in a sample of Italian adults: A three-wave longitudinal study. Psychiatry Res. 2022, 315, 114705. [Google Scholar] [CrossRef] [PubMed]
- Reading Turchioe, M.; Grossman, L.V.; Myers, A.C.; Pathak, J.; Creber, R.M. Correlates of mental health symptoms among US adults during COVID-19, March-April 2020. Public Health Rep. 2021, 136, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Bello, U.M.; Kannan, P.; Chutiyami, M.; Salihu, D.; Cheong, A.M.Y.; Miller, T.; Pun, J.W.; Muhammad, A.S.; Mahmud, F.A.; Jalo, H.A.; et al. Prevalence of anxiety and depression among the general population in Africa during the COVID-19 pandemic: A systematic review and meta-analysis. Front. Public Health 2022, 10, 814981. [Google Scholar] [CrossRef] [PubMed]
- Khaing, N.E.E.; Lim, C.S.; Soon, S.P.; Oh, H.C. Prevalence and correlates of psychological distress and coronavirus anxiety among hospital essential services workers in Singapore. Ann. Acad. Med. Singap. 2022, 51, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Jia, R.; Ayling, K.; Chalder, T.; Massey, A.; Gasteiger, N.; Broadbent, E.; Coupland, C.; Vedhara, K. The prevalence, incidence, prognosis and risk factors for symptoms of depression and anxiety in a UK cohort during the COVID-19 pandemic. BJPsych Open 2022, 8, e64. [Google Scholar] [CrossRef] [PubMed]
- Cho, I.K.; Lee, J.; Kim, K.; Lee, J.; Lee, S.; Yoo, S.; Suh, S.; Chung, S. Schoolteachers’ resilience does but self-efficacy does not mediate the influence of stress and anxiety due to the COVID-19 pandemic on depression and subjective well-being. Front. Psychiatry 2021, 12, 756195. [Google Scholar] [CrossRef] [PubMed]
- Jeong, D.; Cho, I.K.; Kim, K.; Lee, J.; Choi, J.M.; Kim, J.; Kim, C.; Yoo, S.; Chung, S. Mediating effect of public service motivation and resilience on the association between work-related stress and work engagement of public workers in the COVID-19 pandemic. Psychiatry Investig. 2022, 29, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Pace, T.W.W.; Zeiders, K.H.; Cook, S.H.; Sarsar, E.D.; Hoyt, L.T.; Mirin, N.L.; Wood, E.P.; Tatar, R.; Davidson, R.J. Feasibility, acceptability, and preliminary efficacy of an app-based meditation intervention to decrease Firefighter psychological distress and burnout: A one-group pilot study. JMIR Res. 2022, 6, e34951. [Google Scholar] [CrossRef] [PubMed]
- Braquehais, M.D.; Vargas-Caceres, S.; Gomez-Duran, E.; Nieva, G.; Valero, S.; Casas, M.; Bruguera, E. The impact of the COVID-19 pandemic on the mental health of healthcare professionals. QJM 2020, 113, 613–617. [Google Scholar] [CrossRef]
- Jalili, M.; Niroomand, M.; Hadavand, F.; Zeinali, K.; Fotouhi, A. Burnout among healthcare professionals during COVID-19 pandemic: A cross-sectional study. Int. Arch. Occup. Envrion. Health 2021, 94, 1345–1352. [Google Scholar] [CrossRef]
- Kyzar, E.J.; Purpura, L.J.; Shah, J.; Cantos, A.; Nordvig, A.S.; Yin, M.T. Anxiety, depression, insomnia, and trauma-related symptoms following COVID-19 infection at long-term follow-up. Brain Behav. Immun. Health 2021, 16, 100315. [Google Scholar] [CrossRef]
- Shanafelt, T.; Ripp, J.; Trockel, M. Understanding and Addressing Sources of Anxiety Among Health Care Professionals During the COVID-19 Pandemic. JAMA 2020, 323, 2133–2134. [Google Scholar] [CrossRef]
- Weibelzahl, S.; Reiter, J.; Duden, G. Depression and anxiety in healthcare professionals during the COVID-19 pandemic. Epidemiol. Infect. 2021, 149, e46. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.A. Coronavirus Anxiety Scale: A brief mental health screener for COVID-19 related anxiety. Death Stud. 2020, 44, 393–401. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2022, 20, 1537–1545. [Google Scholar] [CrossRef]
- Silva, W.A.D.; de Sampaio Brito, T.R.; Pereira, C.R. COVID-19 anxiety scale (CAS): Development and psychometric properties. Curr. Psychol. 2020, 1–10. [Google Scholar] [CrossRef]
- Chung, S.; Ahn, M.H.; Lee, S.; Kang, S.; Suh, S.; Shin, Y.W. The Stress and Anxiety to Viral Epidemics-6 Items (SAVE-6) Scale: A New Instrument for Assessing the Anxiety Response of General Population to the Viral Epidemic During the COVID-19 Pandemic. Front. Psychol. 2021, 12, 669606. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.; Kim, H.J.; Ahn, M.H.; Yeo, S.; Lee, J.; Kim, K.; Kang, S.; Suh, S.; Shin, Y.W. Development of the Stress and Anxiety to Viral Epidemics-9 (SAVE-9) Scale for Assessing Work-related Stress and Anxiety in Healthcare Workers in Response to Viral Epidemics. J. Korean Med. Sci. 2021, 36, e319. [Google Scholar] [CrossRef] [PubMed]
- Moraleda-Cibrian, M.; Ahmed, O.; Albares-Tendero, J.; Chung, S. Validity and Reliability of the Stress and Anxiety to Viral Epidemics-6 (SAVE-6) Scale to Measure Viral Anxiety of Healthcare Workers in Spain During the COVID-19 Pandemic. Front. Psychiatry 2021, 12, 796225. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Choi, E.; Lee, J.; Lee, S.A. Validation of the Korean version of the obsession with COVID-19 scale and the Coronavirus anxiety scale. Death Stud. 2020, 46, 608–614. [Google Scholar] [CrossRef]
- Han, J.W.; Park, J.; Lee, H. Validity and Reliability of the Korean Version of the Fear of COVID-19 Scale. Int. J. Environ. Res. Public Health 2021, 18, 7402. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- PHQ Screeners. Available online: www.phqscreeners.com (accessed on 1 July 2022).
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Byrne, B.M. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming; Lawrence Erlbaum Associates: New York, NY, USA, 2001. [Google Scholar]
- Linacre, J.M. A User’s Guide to Winsteps and Ministep Rasch Model Computer Programs: Program Manual, 3.75. 2012. Available online: www.winsteps.com/winman/copyright.htm (accessed on 1 July 2022).
- Duncan, P.W.; Bode, R.K.; Min Lai, S.; Perera, S.; Glycine Antagonist in Neuroprotection Americans, I. Rasch analysis of a new stroke-specific outcome scale: The Stroke Impact Scale. Arch. Phys. Med. Rehabil. 2003, 84, 950–963. [Google Scholar] [CrossRef]
- Meyer, J.P. Applied Measurement with jMetrik; Routledge: London, UK, 2014. [Google Scholar]
- Ahn, M.H.; Shin, Y.W.; Suh, S.; Kim, J.H.; Kim, H.J.; Lee, K.U.; Chung, S. High work-related stress and anxiety as a response to COVID-19 among health care workers in South Korea: Cross-sectional online survey study. JMIR Public Health Surveill 2021, 7, e25489. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | N (%) Mean ± SD |
|---|---|
| Sex (female) | 267 (81.4%) |
| Age | 35.8 ± 14.3 |
| Years of employment | 9.7 ± 7.7 |
| Job | |
| Nursing professionals | 194 (59.0%) |
| Doctors | 23 (7.0%) |
| Other healthcare workers | 112 (34.0%) |
| Marital Status | |
| Single | 157 (47.7%) |
| Married, without kids | 51 (15.5%) |
| Married, with kids | 121 (36.8%) |
| Are you a shift worker? (yes) | 73 (22.3%) |
| Questions on COVID-19 | |
| Did you experience being quarantined due to infection with COVID-19? (Yes) | 45 (13.7%) |
| Did you experience being infected with COVID-19? (Yes) | 2 (0.6%) |
| Did you get vaccinated? (Yes) | 327 (99.4%) |
| Psychiatric history | |
| Did you experience or treated depression, anxiety, or insomnia? (Yes) | 46 (13.9%) |
| At present, do you think you are depressed or anxious, or do you need help for your mood state? (Yes) | 24 (7.3%) |
| Psychometric Properties | SAVE-9 | SAVE-6 | CAS | FCV-19 | CAS-7 | GAD-7 | Suggested Cutoff |
|---|---|---|---|---|---|---|---|
| Floor effect | 0 | 0 | 59.0 | 3.5 | 4.1 | 29.3 | 15% |
| Ceiling effect | 0.9 | 1.9 | 0.3 | 0.3 | 0.6 | 0 | 15% |
| Mean inter-item correlation | 0.314 | 0.403 | 0.544 | 0.474 | 0.477 | 0.572 | 0.15~0.50 |
| Cronbach’s alpha | 0.799 | 0.799 | 0.838 | 0.861 | 0.865 | 0.899 | ≥0.7 |
| McDonald’s omega | 0.800 | 0.802 | 0.837 | 0.865 | 0.868 | 0.892 | ≥0.7 |
| Split-half reliability (odd–even) | 0.821 | 0.810 | 0.818 | 0.891 | 0.856 | 0.904 | ≥0.7 |
| Standard error of measurement | 2.54 | 1.88 | 0.85 | 2.00 | 1.44 | 1.42 | <SD (5.25)/2 |
| Rho coefficient | 0.800 | 0.798 | 0.861 | 0.866 | 0.882 | 0.897 | ≥0.7 |
| IRT reliability | 0.846 | 0.832 | 0.633 | 0.875 | 0.881 | 0.804 | ≥0.7 |
| Model fits of confirmatory factor analysis | |||||||
| χ2 (df, p value) | 27.969 | 5.794 | 0.988 | 14.125 | 45.123 | 3.081 | Nonsignificant |
| CFI | 0.999 | 1.000 | 1.000 | 1.000 | 0.974 | 1.000 | >0.95 |
| TLI | 0.999 | 1.000 | 1.114 | 1.000 | 0.960 | 1.023 | >0.95 |
| RMSEA | 0.011 | 0.000 | 0.000 | 0.005 | 0.084 | 0.000 | <0.08 |
| SRMR | 0.049 | 0.034 | 0.059 | 0.041 | 0.089 | 0.034 | <0.08 |
| Items | SAVE-9 | SAVE-6 | CAS | FCV-19S | CAS-7 | GAD-7 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CITC | FL | CITC | FL | CITC | FL | CITC | FL | CITC | FL | CITC | FL | |
| Item 1 | 0.495 | 0.565 | 0.504 | 0.570 | 0.638 | 0.704 | 0.618 | 0.658 | 0.647 | 0.701 | 0.707 | 0.758 |
| Item 2 | 0.661 | 0.758 | 0.682 | 0.787 | 0.652 | 0.728 | 0.580 | 0.610 | 0.629 | 0.644 | 0.800 | 0.865 |
| Item 3 | 0.568 | 0.663 | 0.611 | 0.699 | 0.678 | 0.735 | 0.598 | 0.645 | 0.745 | 0.822 | 0.650 | 0.688 |
| Item 4 | 0.558 | 0.656 | 0.604 | 0.686 | 0.647 | 0.727 | 0.591 | 0.646 | 0.695 | 0.767 | 0.772 | 0.828 |
| Item 5 | 0.458 | 0.506 | 0.445 | 0.497 | 0.711 | 0.773 | 0.733 | 0.802 | 0.610 | 0.641 | 0.689 | 0.734 |
| Item 6 | 0.312 | 0.332 | 0.504 | 0.569 | 0.660 | 0.721 | 0.549 | 0.545 | 0.615 | 0.645 | ||
| Item 7 | 0.373 | 0.401 | 0.651 | 0.718 | 0.585 | 0.626 | 0.722 | 0.769 | ||||
| Item 8 | 0.545 | 0.611 | ||||||||||
| Item 9 | 0.496 | 0.546 | ||||||||||
| Items | Item Fits | Slope Parameter (α) | Threshold Parameter (b) | |||||
|---|---|---|---|---|---|---|---|---|
| S-χ2 | df | p-Value | b1 | b2 | b3 | b4 | ||
| (A) SAVE-9 | ||||||||
| Item 1 | 26.061 | 31 | 0.808 | 1.581 | −3.345 | −2.352 | −1.057 | 0.767 |
| Item 2 | 29.117 | 33 | 0.808 | 2.597 | −2.367 | −1.218 | −0.244 | 1.352 |
| Item 3 | 58.998 | 33 | 0.036 | 2.000 | −2.855 | −1.188 | −0.234 | 1.515 |
| Item 4 | 39.634 | 37 | 0.807 | 1.777 | −2.492 | −1.068 | −0.369 | 1.346 |
| Item 5 | 40.471 | 42 | 0.807 | 1.127 | −1.207 | 0.558 | 1.691 | 3.034 |
| Item 6 | 48.593 | 53 | 0.807 | 0.700 | −2.784 | 0.155 | 1.727 | 3.776 |
| Item 7 | 38.557 | 42 | 0.807 | 0.797 | −4.781 | −1.654 | −0.056 | 3.126 |
| Item 8 | 21.989 | 36 | 0.968 | 1.470 | −3.455 | −2.194 | −1.065 | 0.904 |
| Item 9 | 41.397 | 41 | 0.808 | 1.195 | −3.852 | −1.812 | −0.983 | 0.992 |
| (B) SAVE-6 | ||||||||
| Item 1 | 22.124 | 24 | 0.572 | 1.584 | −3.339 | −2.345 | −1.051 | 0.771 |
| Item 2 | 21.922 | 20 | 0.572 | 2.778 | −2.316 | −1.191 | −0.242 | 1.330 |
| Item 3 | 18.369 | 20 | 0.572 | 2.101 | −2.796 | −1.163 | −0.230 | 1.492 |
| Item 4 | 26.666 | 26 | 0.572 | 1.827 | −2.450 | −1.054 | −0.368 | 1.334 |
| Item 5 | 30.776 | 30 | 0.572 | 1.099 | −1.226 | 0.570 | 1.720 | 3.084 |
| Item 6 | 42.030 | 29 | 0.336 | 1.340 | −3.681 | −2.319 | −1.123 | 0.962 |
| (C) CAS | ||||||||
| Item 1 | - | 0 | - | 2.314 | 0.977 | 2.109 | 2.740 | 3.093 |
| Item 2 | - | 0 | - | 2.872 | 0.584 | 1.753 | 2.589 | 3.098 |
| Item 3 | - | 0 | - | 4.158 | 1.574 | 2.303 | 2.826 | 3.332 |
| Item 4 | 3.706 | 2 | 0.157 | 2.712 | 1.109 | 2.270 | 3.569 | - |
| Item 5 | 4.582 | 1 | 0.064 | 3.786 | 1.217 | 2.361 | 3.390 | - |
| (D) FCV-19S | ||||||||
| Item 1 | 15.162 | 26 | 0.954 | 1.695 | −1.517 | −0.407 | 1.053 | 3.045 |
| Item 2 | 13.292 | 22 | 0.954 | 1.848 | −1.982 | −1.321 | −0.594 | 1.931 |
| Item 3 | 20.402 | 23 | 0.954 | 2.357 | 0.117 | 1.181 | 2.143 | 3.530 |
| Item 4 | 39.578 | 31 | 0.954 | 1.745 | −0.683 | 0.374 | 1.171 | 2.849 |
| Item 5 | 18.478 | 23 | 0.954 | 2.828 | −0.895 | 0.013 | 0.630 | 2.357 |
| Item 6 | 18.976 | 21 | 0.954 | 2.628 | −0.085 | 0.910 | 2.112 | 2.997 |
| Item 7 | 42.543 | 28 | 0.273 | 2.157 | −0.420 | 0.555 | 1.092 | 2.845 |
| (E) CAS-7 | ||||||||
| Item 1 | 16.315 | 13 | 0.408 | 2.393 | −1.730 | −0.743 | 1.519 | |
| Item 2 | 14.246 | 13 | 0.469 | 2.234 | −0.004 | 1.398 | 3.401 | |
| Item 3 | 18.595 | 12 | 0.250 | 3.930 | −1.111 | −0.249 | 1.733 | |
| Item 4 | 13.485 | 14 | 0.489 | 2.743 | −1.193 | −0.267 | 1.951 | |
| Item 5 | 16.745 | 16 | 0.469 | 1.867 | −0.369 | 1.016 | 2.636 | |
| Item 6 | 18.312 | 12 | 0.250 | 1.826 | 0.357 | 2.092 | 3.430 | |
| Item 7 | 35.166 | 16 | 0.028 | 1.999 | −1.860 | −0.841 | 1.616 | |
| (F) GAD-7 | ||||||||
| Item 1 | 7.351 | 6 | 0.565 | 3.236 | 0.401 | 1.923 | 3.281 | |
| Item 2 | 4.719 | 7 | 0.694 | 4.745 | 0.572 | 1.553 | 2.665 | |
| Item 3 | 15.837 | 14 | 0.565 | 2.152 | −0.029 | 1.308 | 2.030 | |
| Item 4 | 8.328 | 5 | 0.490 | 3.774 | 0.383 | 1.773 | 2.467 | |
| Item 5 | 3.899 | 6 | 0.694 | 4.026 | 1.122 | 2.015 | - | |
| Item 6 | 11.637 | 12 | 0.665 | 1.791 | −0.048 | 1.359 | 2.475 | |
| Item 7 | 8.307 | 5 | 0.490 | 3.786 | 0.924 | 1.943 | 3.257 | |
| Scale | Items | MnSq | Difficulty | Separation Index | Reliability | |||
|---|---|---|---|---|---|---|---|---|
| Infit | Outfit | Item | Person | Item | Person | |||
| SAVE-9 | Item 1 | 0.91 | 0.90 | −0.85 | 9.984 | 2.047 | 0.990 | 0.807 |
| Item 2 | 0.62 | 0.61 | −0.13 | |||||
| Item 3 | 0.77 | 0.78 | −0.07 | |||||
| Item 4 | 0.96 | 0.96 | −0.11 | |||||
| Item 5 | 1.12 | 1.09 | 1.41 | |||||
| Item 6 | 1.42 | 1.52 | 0.96 | |||||
| Item 7 | 1.10 | 1.12 | 0.13 | |||||
| Item 8 | 0.86 | 0.86 | −0.75 | |||||
| Item 9 | 1.12 | 1.19 | −0.59 | |||||
| SAVE-6 | Item 1 | 1.06 | 1.02 | −0.93 | 10.856 | 2.086 | 0.992 | 0.813 |
| Item 2 | 0.08 | 0.68 | −0.05 | |||||
| Item 3 | 0.83 | 0.83 | 0.02 | |||||
| Item 4 | 1.01 | 1.00 | −0.03 | |||||
| Item 5 | 1.26 | 1.29 | 1.79 | |||||
| Item 6 | 1.10 | 1.16 | −0.80 | |||||
| CAS | Item 1 | 1.30 | 1.20 | −0.54 | 4.585 | 0.999 | 0.955 | 0.500 |
| Item 2 | 1.04 | 1.04 | −1.31 | |||||
| Item 3 | 0.90 | 0.53 | 1.29 | |||||
| Item 4 | 1.03 | 0.99 | 0.04 | |||||
| Item 5 | 0.80 | 0.77 | 0.51 | |||||
| FCV-19S | Item 1 | 1.00 | 1.15 | −0.54 | 12.943 | 2.430 | 0.994 | 0.855 |
| Item 2 | 1.05 | 0.95 | −2.10 | |||||
| Item 3 | 0.87 | 0.78 | 1.40 | |||||
| Item 4 | 1.26 | 1.24 | 0.15 | |||||
| Item 5 | 0.87 | 0.85 | −0.36 | |||||
| Item 6 | 0.74 | 0.74 | 1.11 | |||||
| Item 7 | 1.10 | 1.07 | 0.34 | |||||
| CAS-7 | Item 1 | 1.07 | 1.02 | −1.94 | 15.090 | 2.485 | 0.996 | 0.861 |
| Item 2 | 0.82 | 0.74 | 1.97 | |||||
| Item 3 | 0.80 | 0.73 | −0.94 | |||||
| Item 4 | 0.93 | 0.87 | 0.90 | |||||
| Item 5 | 1.10 | 1.14 | 1.19 | |||||
| Item 6 | 0.89 | 1.00 | 2.64 | |||||
| Item 7 | 1.22 | 1.33 | −2.01 | |||||
| GAD-7 | Item 1 | 0.88 | 0.89 | 0.02 | 7.434 | 2.012 | 0.982 | 0.802 |
| Item 2 | 0.71 | 0.58 | 0.23 | |||||
| Item 3 | 1.39 | 1.36 | −1.52 | |||||
| Item 4 | 0.76 | 0.77 | −0.11 | |||||
| Item 5 | 0.79 | 0.50 | 1.67 | |||||
| Item 6 | 1.46 | 1.49 | −1.45 | |||||
| Item 7 | 0.80 | 0.60 | 1.15 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, C.; Ahmed, O.; Silva, W.A.D.; Park, C.H.K.; Yoo, S.; Chung, S. Applicability and Psychometric Comparison of the General-Population Viral Anxiety Rating Scales among Healthcare Workers in the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 9946. https://doi.org/10.3390/ijerph19169946
Kim C, Ahmed O, Silva WAD, Park CHK, Yoo S, Chung S. Applicability and Psychometric Comparison of the General-Population Viral Anxiety Rating Scales among Healthcare Workers in the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(16):9946. https://doi.org/10.3390/ijerph19169946
Chicago/Turabian StyleKim, Changnam, Oli Ahmed, Washington Allysson Dantas Silva, C. Hyung Keun Park, Soyoung Yoo, and Seockhoon Chung. 2022. "Applicability and Psychometric Comparison of the General-Population Viral Anxiety Rating Scales among Healthcare Workers in the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 16: 9946. https://doi.org/10.3390/ijerph19169946
APA StyleKim, C., Ahmed, O., Silva, W. A. D., Park, C. H. K., Yoo, S., & Chung, S. (2022). Applicability and Psychometric Comparison of the General-Population Viral Anxiety Rating Scales among Healthcare Workers in the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 19(16), 9946. https://doi.org/10.3390/ijerph19169946