Abstract
Self-care behaviors are essential for the effective treatment of heart failure (HF), and poor self-care may lead to adverse clinical events in patients with HF. A growing body of literature addresses the need to analyze the characteristics of both patient and caregiver since they are in mutual, long-term interaction, and their reactions to events are dependent on each other. One of the most common approaches for analyzing data on HF self-care dyads is the Actor–Partner Interdependence Model (APIM). The purpose of this study was to conduct a scoping review to answer the following question: what did we learn from HF dyadic studies based on the APIM approach? Medline, Academic Search Ultimate, and CINAHL Complete databases were searched, using the terms “dyad,” “dyadic,” and “heart failure,” for studies published between 2009 and April 2021. Fifteen studies were reviewed from a pool of 106 papers. Studies using the APIM approach revealed interrelated patient and caregiver characteristics that influence self-care and explain many complex dyadic behaviors. Our analysis provided evidence that (1) APIM is a useful analytical approach; (2) a family-oriented approach can improve the functioning of a patient with HF; and (3) social support from caregivers significantly enhances patients’ adaptation to illness.
1. Introduction
Heart failure (HF) is a complex, heterogeneous, increasingly prevalent cardiovascular disorder with high morbidity and mortality [1,2]. Self-care behaviors are essential for the effective treatment of heart failure, and poor self-care may lead to adverse clinical events in patients with HF, including repeated hospitalizations, poor quality of life, and increased mortality [3]. Several factors contribute to adequacy of self-care. Depression [4], sleep disturbances [5], impaired cognition, multiple comorbid conditions [6], and low level of awareness of illness decline all limit self-care [7]. The involvement of the partner, i.e., the informal caregiver who assists the patient with daily self-care, is crucial. Caregiver mental health, strain, and contributions to self-care predict patient clinical events in heart failure [8,9,10]. A caregiver is often someone very close to the patient, such as a spouse or an adult child, who helps the patient with daily functioning and has the potential to influence the trajectory of this chronic disease. Increasingly, researchers are using a dyadic approach to study self-care in HF because they have realized that self-care is a dyadic phenomenon in which patients and their caregivers are an interdependent team working within their life context and that the way they appraise illness as a team influences management of the disorder [11]. HF patients usually have a partner with whom they make day-to-day decisions about symptom management but also about diet and how to deal with worsening symptoms. Dyadic HF research has shown that good relationships with a partner and other people [12,13], knowledge regarding HF of each member of the dyad [14], congruence in symptom assessment, and agreement on who is providing self-care [15] influence HF behavior and may determine a patient’s outcome. Within this dyad, caregivers influence patient self-care and patients influence caregiver’s contribution to self-care. Patients struggle to perform self-care; therefore, the contribution of informal caregivers is fundamental, and a dyadic approach is necessary. Therefore, the dyadic approach to self-care allows a more accurate assessment the factors determining effective self-care in HF by including both the patient and the caregiver [16].
2. Theoretical Background
Studies conducted on caregiver participation in self-care in HF and other chronic conditions have shown that taking the caregiver role into account improves patient outcomes. Since HF patients and their caregivers influence each other in self-care, investigators have started to approach self-care studies using dyadic approaches because they allow controlling for the interdependence between patients and caregivers. The theoretical framework for research on dyadic care in HF is a combination of three theories: the Theory of Dyadic Illness Management (TDIM) [11], Situation-Specific Theory of Heart Failure Self-Care (SSTHFSC) [17,18], and the Situation-Specific Theory of Caregiver Contribution to Heart Failure Self-Care (SSTCCHFSC) [19]. The TDIM illustrates that management of disease is a dyadic process and describes the interdependency of the patient and the caregiver. The Situation-Specific Theory of Heart Failure Self-Care illustrates the unique aspects of self-care in patients with HF. The Situation-Specific Theory of Caregiver Contribution to Heart Failure Self-Care describes factors influencing caregiver contribution to HF self-care as well as outcomes of this contribution. Research on dyadic self-care in HF focuses on the joint management of this specific disease by the adult patient and caregiver. Many previous studies of self-care in HF have focused on either the patient [20,21,22,23] or the caregiver [9,24,25]. There are also studies investigating dyads with chronic illnesses, but their focus was more about dyadic appraisal and coping (i.e., spousal involvement and communication between dyadic partners) [26]. A dyadic approach to the care of a patient with HF emphasizes the joint efforts of both members in coping with the disease and the interdependency of the two members of the dyad on effectiveness of HF self-care.
HF is a heterogeneous disease, both in terms of patient health status as well as caregiver experience and tasks. The time required in HF caregiving is highly variable and depends on several factors, including the severity and stability of HF, the presence of comorbidities, impairments to physical and/or cognitive function, the complexity of the treatment regimen, and other situational aspects [27]. During the disease, as the disease advances, the experience of HF becomes characterized by continuous management of progressive and pervasive symptoms (e.g., dyspnea, fatigue, edema, insomnia) that severely compromise the quality of life [18,28]. Additionally, patients with advanced heart failure have an uncertain disease trajectory, and this places a significant burden on heart failure caregivers [29]. Higher levels of comorbid conditions are associated with family caregivers feeling fewer positive feelings about providing care [30], and higher patient with HF functional class (worse symptom severity) is significantly associated with greater caregiver anxiety and general stress [31]. Studies across caregiving contexts suggest that caregivers of patients with more severe illness may need the most support [32,33,34].
3. Theory of Dyadic Illness Management
According to the TDIM [11], illness management is a dyadic process involving both the patient and the caregiver. A distinctive feature of the dyadic approach to patient care is the focus on dyadic health (i.e., the health of the dyad rather than the care of either the patient or the caregiver). According to the TDIM, the goal of care is to optimize the health of both members of the dyad. The way both members of the dyad appraise the illness can affect the health of them both. Because this dyad is an interdependent team, the way they appraise illness affects how they engage in management behaviors. In many aspects, congruent appraisals of the disease by both dyadic partners can lead to better collaboration in managing illness and ultimately better health. It is best if the patient and the caregiver have greater congruence in the appraisal of symptoms, care values, and preferences. Appraisal influences disease-management behaviors, which occur on a continuum within the dyad. Only one of the care partners is involved in disease management at the low end of the spectrum, whereas both members of the dyad participate in disease-management behaviors at the high end of the spectrum. The theory posits that higher levels of collaboration between the two members of the dyad are associated with better health [11,35]. Collaboration between dyadic partners should include decision making, symptom management, and general health behaviors of both partners. The TDIM also assumes that dyadic management behaviors are influenced by the state of health of the patient and caregiver, the dyadic typology, and the contextual factors linked with social support or culture.
3.1. The Situation-Specific Theory of Heart Failure Self-Care
The Situation-Specific Theory of HF self-care was created based on real-life experiences of caring for patients with HF. This theory was published in 2008 [17] and then updated in 2016 given recent empirical findings [18]. According to this theory, self-care includes three separate and interrelated processes: maintenance (adherence to recommendations and healthy behaviors, including taking medication, following low-salt diet, and maintaining physical activity), symptom perception (monitoring, detecting, interpreting, and labeling signals from the body), and management (a behavioral response to emerging symptoms). All processes require knowledge and skill, but the most demanding process is management. The SSTHFSC emphasizes that the “naturalistic decision-making” process occurs in real-life situations and dynamic environments with incomplete information, competing needs, time pressure, and high levels of stress due to the potentially life-threatening nature of the event. Patient decisions in self-care in HF are based on both objective data (e.g., weight gain) and subjective data (e.g., fatigue). The SSTHFSC identifies several factors that influence self-care decisions, including person-related factors (e.g., cultural identify, health literacy, socioeconomic status), problem-specific factors (e.g., co-morbidities, including cognitive impairment), and environmental factors (e.g., lack of social support). Given these factors, self-care decisions made by patients sometimes are inconsistent and even wrong.
3.2. The Situation-Specific Theory of Caregiver Contribution to HF Self-Care
The Situation-Specific Theory of Caregiver Contribution to HF Self-Care is based both on the SSTHFSC and the Middle Range Theory of Self-Care of Chronic Illnesses [36] and describe factors at caregiver (e.g., age), patient (e.g., cognition), and dyadic level (e.g., the relationship between the patient and the caregiver) that influence the extent to which caregivers contribute to support HF patient self-care. Similar to the SSTHFSC, caregiver contributions to HF self-care include the dimensions of caregiver contribution to self-care maintenance, symptom monitoring, and perception and self-care management. In addition, the theory includes a mediator, which is the caregiver’s self-efficacy that mediates the relationship between the contributors and caregiver contributions to self-care, and the outcomes, which can be related to patient (e.g., quality of life) and caregiver (e.g., self-esteem).
3.3. The Actor–Partner Interdependence Model
The interdependency between the patient and the caregiver needs to be taken into consideration when analyzing data on dyads. The Actor–Partner Interdependence Model (APIM) is the most current methodology for analyzing data on HF self-care dyads. The APIM is based on the Interdependence Theory [37], which assumes that people influence each other’s experiences by interacting with each other. Researchers emphasize the need to analyze the characteristics of both patient and caregiver since they are in a mutual, long-term interaction, and their reactions to events are dependent on each other. The APIM model for HF dyadic care studies is usually supported by paired regression analyses of the relationship within the couple, i.e., a regression method that does not require independent observations (see Appendix A, Figure A1). The APIM model specifies how the independent variable of an individual may impact their own dependent variable (actor effects) as well as the partner’s dependent variable (partner effects) [38]. There are three types of variables in the APIM model: (1) between-dyads variables, (2) within-dyads variables, and (3) mixed variables. Between-dyads variables are those that vary across dyads but are the same for both members of the dyad (e.g., years spent in a relationship). A within-dyads variable varies across the members of the dyad, but each dyad would have the same total score as all other dyads (e.g., if the study consists only of heterosexual couples, this variable will be gender: male and female). A mixed variable is one that has variation both within and between dyads (e.g., age of members). It is possible to estimate actor and partner effects for mixed variables only. Between- and within-dyads variables can be estimated as main effects. Additionally, various interactions can be tested based on the model [39]. An extended model of the APIM, the Actor–Partner Interdependence Mediation Model (APIMeM), allows to assess mediation in dyadic data [40].
To date, there has been little consistency in how data on HF care dyads have been analyzed. As mentioned above, researchers suggest analyzing dyadic data with the APIM model because it takes interactions between dyadic partners into consideration. In recent studies, APIM has been shown to be effective in identifying the determinants of effective dyadic coping with HF. Many authors emphasize the need to continue using this method of analysis [9,28,29]. Since dyadic analysis is becoming a new approach to studying HF self-care, a systematic review of these studies would help orientate future studies on this topic. The purpose of our article was to review the existing evidence on self-care in HF patient/caregiver dyads based on the APIM approach. Establishing the status of existing research in self-care in HF allowed us to systematize recent findings and point out potential areas worthy of further exploration.
4. Data Search
Several databases, including Medline, Academic Search Ultimate, and CINAHL Complete, were searched for relevant literature. Search terms were entered as keywords and included dyad, dyadic, and heart failure. The search was restricted to 2009–April 2021. Citations of retrieved papers were hand-searched to identify additional relevant studies. Studies were eligible for inclusion if they (1) were published in peer-reviewed journals written in English; (2) used either the APIM or his extended version, the APIMeM, to analyze data; and (3) involved adult population (over 18 years old). The analysis excluded articles focusing on dyadic typologies, the development of methods and research instruments, qualitative tests, longitudinal studies, discussions and conceptualizations about the health of dyads as a unit, and dyadic interventions. We also excluded studies on mixed dyads, including patients with HF and other diseases.
5. Results
The initial search yielded 106 articles. After removal of duplicates, 48 original articles remained. Full text of all resulting papers were reviewed for further assessment, and another 33 were excluded because they did not meet the inclusion criteria, leaving 15 studies for inclusion in this review (see Figure 1). Table 1 provides a detailed description of each study in terms of country, the sample, the aim of the study, main outcome measures, findings, results, and conclusions.
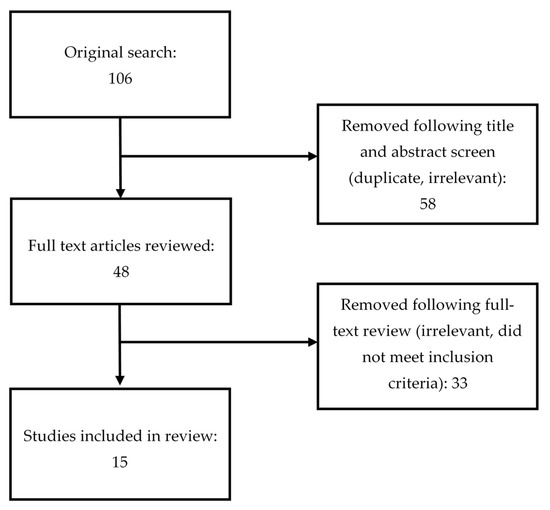
Figure 1.
PRISMA table outlining literature search.

Table 1.
Characteristic of eligible studies.
5.1. Summary of Findings
5.1.1. Quality of Life and Emotional Aspects of Dealing with HF
Analysis of the dyadic studies demonstrates that managing HF can be very emotional for both the patient and the caregiver [42]. Both partners in the dyad experience high levels of emotional distress [43]; however, patients seem to experience more depressive symptoms than their spouses [41,51]. Greater emotional distress has been associated with poor quality of life. Two studies focused on the caregiver and provided evidence that quality of life of the patient is better if the care partner has no depressive symptoms or anxiety [42,43]. Sleep also is particularly important for caregivers. It has been empirically demonstrated that the presence of sleep disorders significantly affects the mental health of the caregiver [44]. What positively affects the caregiver’s quality of life is the patient’s adherence to therapy [48]. Better emotional well-being of the dyad also is associated with better relationship quality [41]; however, having a good relationship is not “protective” against anxiety and depression for caregivers [53]. If either member of the dyad senses that they are not in control over HF, the emotional well-being of the dyad may become worse [50]. Incongruent collaboration of partners in HF management also affects the emotional well-being of the dyad [51]. Studies on emotional state and quality of life in dyadic caring in HF conclude that interventions are needed to alleviate depressive symptoms in both dyadic partners [42,43]. It appears that nurses can increase dyadic caring by providing the dyadic partners with social support [49].
5.1.2. Dyadic HF Self-Care Confidence
Self-care confidence, or self-care self-efficacy, is the extent to which one feels able to perform regular self-care (patient) and contribute to patient self-care (caregiver) despite difficulties [47]. Research on dyadic self-care has shown that poor self-efficacy affects the ability of the patient and caregiver to engage. Patients with greater self-care confidence are more engaged in self-care behaviors [45]. Studies on dyadic care in HF also show that self-care confidence is not typically equal between the members of the dyad, with caregivers demonstrating greater self-care confidence than patients [16]. However, there has also been heterogeneity in confidence across the dyads, suggesting self-care confidence is adequate in some dyads but is insufficient to support self-care in others [16].
Several factors are associated with better self-care confidence, including female gender, education, social support experienced by both partners, caregiver’s mental health, relationship quality [16], and mutuality within the dyad [45]. Mutuality, defined as the extent to which there is an emotional investment and mutual support in the dyad, was predictive of reduced burden in the caregiver [45]. Therefore, it is best when the caregiver perceives and recognizes mutuality in the relationship with the patient [52].
5.1.3. Maintenance and Management
Data from APIM studies show low levels of daily HF maintenance and management in both partners in HF self-care [46,47]. Not surprisingly, mild cognitive impairment in the patient reduces self-care [46]. Better self-care maintenance is usually achieved in dyads where the caregiver is a woman. Indeed, there is evidence that female gender of the caregiver was a significant predictor of better patient self-care maintenance [46]. This most likely arises from a traditional role of women, who mainly care about family health in many societies. There also is evidence that a caregiver is more likely to contribute to HF self-care management if the caregiver is not the patient’s spouse [46]. Involvement in self-care also is associated with the emotional state of the caregiver, the quality of the relationship between the HF patient and the caregiver [47,52,54], and the caregiver’s knowledge of self-care [47]. Patients are more adherent to recommendations when they have a decreased physical quality of life [48]. It seems, therefore, that a greater problem in engaging patients in self-care may arise in patients with a relatively high physical quality of life. Furthermore, an agreement between dyad partners who are responsible for performing self-care tasks may also be an important issue for self-care. Dyads that were congruent not only reported fewer psychosocial problems [55], but also in these dyads, the caregivers were more engaged in caregiving [47].
6. Discussion
In this paper, we reviewed studies using the APIM model to summarize how adult patients and their caregivers interact to perform HF self-care. The APIM is a useful analytical approach to evaluating partner and actor effects in the presence of interdependencies between the dyad partners. Using this model, the studies we reviewed provided evidence of several factors that influence effectiveness of HF self-care in dyads. This review showed which topics and tools have already been used and will help researchers identify new areas that have not yet been explored.
Many studies have focused on the emotional aspects of coping with heart failure and the quality of life of dyadic partners [41,42,43,44,51,53]. The analysis of the studies presented here provides evidence that these factors are crucial in the self-care of patients with HF. Previous studies have also found that effective HF coping is highly dependent on the emotional state of both the patient and the caregiver [29,30,56]. It is exhausting for both of them to deal with the issues of HF daily. The quality of relationships as well as the socio-cultural background are all crucial factors in coping with the disease [35,57,58,59]. Clinicians should evaluate the emotional status of HF patients at each visit, specifically looking for depressive symptoms or anxiety. According to APIM studies, sleep disturbances in caregivers are also worth focusing on and should be treated because they affect the patient’s well-being. Clinicians also should inquire about the quality of the relationship, as strained relationships are less successful with self-care. Studies on dyadic partners and the quality of their relationship have highlighted the impact of social support for self-care of patients with HF. Therefore, in addition to the relationship with the caregiver, clinicians should identify other sources of social support.
Qualities of the caregiver are another factor that contributes to success of the dyad. Care partners who are female and are not the spouse of the patient demonstrate better self-care. Notably, however, cultural differences in caregiving have been identified. Gender and partner roles may vary among cultures and should be considered when developing plans for self-care. Clinicians should speak to both the patient and the family to identify the person best-suited to taking on the role of caregiver. Studies using APIM also have shown the importance of caregiver’s knowledge in the management of HF self-care. After identifying the appropriate caregiver, clinicians should include care partners in self-care education and even tailor education so it corresponds with specific responsibilities of each member of the dyad.
The review revealed that the variables in APIM studies of dyadic care in HF are often the same. The advantage of using the same research measure is the ability to compare studies worldwide and across different groups. The disadvantage of this approach is related to the limited scope of research topics devoted to self-care in HF. For example, we found that relatively little research has been dedicated to evaluating the sense of control over the HF trajectory, which is an essential for understanding the illness, developing coping strategies, and appreciating the importance of appropriate self-care [60].
Our review identified several dyadic studies on self-care maintenance, management, and confidence; however, the concept of symptom perception has not yet been explored. Although research on symptom perception and clinical outcomes has been done, it has not been done in the context of a dyad. Future research should evaluate how symptom perception is influenced by dyad typology and emotional factors that have been found to influence other aspects of self-care. Furthermore, studies should be expanded to investigate the relationship between symptom perception, maintenance, management, and risk perception regarding the probability of desired and undesirable effects of HF self-care in both dyadic partners. There is still a lack of studies on risk perception in terms of the likelihood of desired and undesirable effects of HF therapy and how risk perception affects current behavior in both couples. Both partners’ beliefs about health and health conditions could play a role in determining health-related behaviors. Very often, a person’s perception of the condition influences the health choices more than the condition itself [61,62]. Perceived illness susceptibility, perceived benefits of self-care, perceived barriers to healthy habits, and the seriousness of the condition may be other important factors for dyadic partners’ behavior [63,64], and they seem to be worth exploring in the context of self-care in HF. Lastly, although cognitive dysfunction is common in HF and may influence the effectiveness of the dyad, the association between self-care and cognitive dysfunction within the self-care dyad has not been investigated. Given the high prevalence of cognitive dysfunction in HF, it is unknown how cognitive dysfunction influences dyad typology, the roles of each member of the dyad, and the influence of cognitive dysfunction on self-care effectiveness in the context of the dyad.
Some limitations should be mentioned. HF is a very heterogeneous condition, and each patient has different degrees of dependency. Studies that entered the analysis are not consistent with HF criteria. Since, in the review, we did not consider the degree of independence and type of patient, the generalizability of our results is limited. In addition, studies included in the review look at different variables with different types of dyads in each case, which also suggests that the conclusions based on the research should be interpreted with caution.
This article was limited to analysis of studies based on the APIM and the extended APIM, the Actor–Partner Interdependence Mediation Model (APIMeM). Therefore, studies that evaluated HF self-care in dyads but did not use one of these models were not included. The APIM model appears to be appropriate for analyzing the experiences and decisions in a dyad since it uses an approach that takes into account the lack of independence of the dyadic partners. Nonetheless, so far, researchers have identified more complex associations between self-care and other important variables in the context of a HF self-care dyad. Certainly, the reported APIM findings on the factors associated with adherence, symptom management, dyadic confidence, quality of life, and emotional aspects of coping with HF do not exhaust all the dyadic factors.. We did not include in our review studies on types of HF management and studies on the effectiveness of interventions in HF dyads in our review since they did not match the criteria for inclusion.
Considering caregiving factors together with patient factors significantly increases our understanding of patient clinical event risk in HF [8]. The complex interrelationships between patient and caregiver factors revealed by APIM research are depicted in Figure A2 (Appendix A). Figure A2 shows, for instance, that a patient’s self-care outcome (i.e., maintenance, management, symptom perception, or confidence) is significantly related to relationship quality [16,46], dyad congruence [54], as well as caregivers’ depressive symptoms and anxiety [47], mental quality of life [16], satisfaction with dyadic type [54], and patient mutuality [45,52]. Figure A3 (Appendix A), in turn, shows results of APIM research on caregiver quality of life and emotional aspects of dealing with HF patients. Although prior studies indicated similar patterns of relationships [55,56,65,66,67,68], an analysis employing the APIM revealed complex interrelationships between patient and caregiver features. Researchers should consider exploring self-care phenomena using the APIM model to analyze the interdependence between the members of the dyad.
7. Conclusions
The frameworks of the Theory of Dyadic Illness Management and the Situation-Specific Theory of Heart Failure Self-Care and Caregiver Contribution to Heart Failure Self-Care are in line with conceptualizing the dyad as a system with interdependence between members of the system. This posited interdependence between the patient and the caregiver has long been used for behavioral treatment (e.g., addictions) and recently became increasingly important for treating chronic diseases [26]. It seems that the APIM model is well suited for dyadic system analysis. Studies using APIM approaches reveal interrelated characteristics of the patient and the caregiver that affect self-care and may explain many complex dyadic behaviors. In this fashion, this approach contributes to a better understanding of the dynamics of the interaction between the caregiver and HF patient. Most of the studies reviewed here conclude that (1) a family-oriented approach can improve the functioning of a patient with heart failure condition, and (2) social support from caregivers significantly enhances patients’ adaptation to illness. Our work’s emerging view is that patient–caregiver interconnections are still enigmatic, and more studies are needed to provide a more complete and coherent picture of self-care in HF. Thus, further research should be carried out to clarify this concept and identify the most critical factors for effective dyadic functioning in HF.
Our review showing the interrelationship of patient and caregiver highlighted the need to include both care partners. It seems necessary not only to continue research showing how the HF patient and caregiver interact but also to simultaneously undertake educational interventions involving members of the dyad as well as nurses and physicians. All caregivers of the HF patient must know and, more importantly, have the aids to facilitate collaboration with the patient. As a preventive measure, some authors have emphasized the importance of physical activity and fitness in HF patients [69,70] as well as the role of nurses in helping HF patients manage their symptoms, particularly through nurse-led educational interventions and assistance with home monitoring through advanced technologies [71,72]. The important role of the social support experienced by the dyad for the effectiveness of its functioning, as revealed in the review, also suggests that some efforts should be made to initiate patient and caregiver support groups in all settings where HF care is provided. In turn, the associations revealed in the review between the psychological status of both dyadic partners and coping with HF suggest that perhaps some patients should receive additional psychological care. Improving the psychological functioning of the dyad could have a positive impact on adherence and help cope with all the challenges posed by the unpredictable trajectory of HF.
Author Contributions
I.U. contributed to the design of the study, analysis, and write-up of the manuscript. K.M.F., E.V., A.S., R.S. and A.O.-K. contributed to the design, drafting, and edition of the manuscripts. All authors contributed to data analysis, drafting, revising the article, approved the final version, and agreed to be accountable for all aspects of the work. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by Wroclaw Medical University grant no. SUB.E020.21.002.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors report no conflict of interest.
Appendix A

Figure A1.
The Actor–Partner Interdependence Model (APIM) used to analyze dyadic data.
Figure A1.
The Actor–Partner Interdependence Model (APIM) used to analyze dyadic data.


Figure A2.
Relationships between caregiver and patient characteristics in studies employing APIM.
Figure A2.
Relationships between caregiver and patient characteristics in studies employing APIM.


Figure A3.
Results regarding caregiver quality of life and emotional aspects of dealing with HF patient.
Figure A3.
Results regarding caregiver quality of life and emotional aspects of dealing with HF patient.

References
- Friedman, M.M.; Quinn, J.R. Heart Failure Patients’ Time, Symptoms, and Actions before a Hospital Admission. J. Cardiovasc. Nurs. 2008, 23, 506–512. [Google Scholar] [CrossRef] [PubMed]
- Hauptman, P.J.; Masoudi, F.A.; Weintraub, W.S.; Pina, I.; Jones, P.G.; Spertus, J.A. Variability in the Clinical Status of Patients with Advanced Heart Failure. J. Card. Fail. 2004, 10, 397–402. [Google Scholar] [CrossRef]
- Lee, C.S.; Moser, D.K.; Lennie, T.A.; Riegel, B. Event-Free Survival in Adults with Heart Failure Who Engage in Self-Care Management. Heart Lung J. Acute Crit. Care 2011, 40, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Holzapfel, N.; Löwe, B.; Wild, B.; Schellberg, D.; Zugck, C.; Remppis, A.; Katus, H.A.; Haass, M.; Rauch, B.; Jünger, J.; et al. Self-Care and Depression in Patients with Chronic Heart Failure. Heart Lung 2009, 38, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Riegel, B.; Moelter, S.T.; Ratcliffe, S.J.; Pressler, S.J.; De Geest, S.; Potashnik, S.; Fleck, D.; Sha, D.; Sayers, S.L.; Weintraub, W.S.; et al. Excessive Daytime Sleepiness Is Associated with Poor Medication Adherence in Adults with Heart Failure. J. Card. Fail. 2011, 17, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Dickson, V.V.; Buck, H.; Riegel, B. A Qualitative Meta-Analysis of Heart Failure Self-Care Practices among Individuals with Multiple Comorbid Conditions. J. Card. Fail. 2011, 17, 413–419. [Google Scholar] [CrossRef]
- Jurgens, C.Y. Somatic Awareness, Uncertainty, and Delay in Care-Seeking in Acute Heart Failure. Res. Nurs. Health 2006, 29, 74–86. [Google Scholar] [CrossRef]
- Bidwell, J.T.; Vellone, E.; Lyons, K.S.; D’Agostino, F.; Riegel, B.; Paturzo, M.; Hiatt, S.O.; Alvaro, R.; Lee, C.S. Caregiver Determinants of Patient Clinical Event Risk in Heart Failure. Eur. J. Cardiovasc. Nurs. 2017, 16, 707–714. [Google Scholar] [CrossRef]
- Buck, H.G.; Harkness, K.; Wion, R.; Carroll, S.L.; Cosman, T.; Kaasalainen, S.; Kryworuchko, J.; McGillion, M.; O’Keefe-Mccarthy, S.; Sherifali, D.; et al. Caregivers’ Contributions to Heart Failure Self-Care: A Systematic Review. Eur. J. Cardiovasc. Nurs. 2015, 14, 79–89. [Google Scholar] [CrossRef]
- Nicholas Dionne-Odom, J.; Hooker, S.A.; Bekelman, D.; Ejem, D.; McGhan, G.; Kitko, L.; Strömberg, A.; Wells, R.; Astin, M.; Metin, Z.G.; et al. Family Caregiving for Persons with Heart Failure at the Intersection of Heart Failure and Palliative Care: A State-of-the-Science Review. Heart Fail. Rev. 2017, 22, 543–557. [Google Scholar] [CrossRef]
- Lyons, K.S.; Lee, C.S. The Theory of Dyadic Illness Management. J. Fam. Nurs. 2018, 24, 8–28. [Google Scholar] [CrossRef] [PubMed]
- Dunbar, S.B.; Clark, P.C.; Quinn, C.; Gary, R.A.; Kaslow, N.J. Family Influences on Heart Failure Self-Care and Outcomes. J. Cardiovasc. Nurs. 2008, 23, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Graven, L.J.; Grant, J.S. Social Support and Self-Care Behaviors in Individuals with Heart Failure: An Integrative Review. Int. J. Nurs. Stud. 2014, 51, 320–333. [Google Scholar] [CrossRef] [PubMed]
- Bidwell, J.T.; Higgins, M.K.; Reilly, C.M.; Clark, P.C.; Dunbar, S.B. Shared Heart Failure Knowledge and Self-Care Outcomes in Patient-Caregiver Dyads. Heart Lung J. Acute Crit. Care 2018, 47, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Buck, H.G.; Hupcey, J.; Mogle, J.; Rayens, M.K. Caregivers’ Heart Failure Knowledge Is Necessary but Not Sufficient to Ensure Engagement With Patients in Self-Care Maintenance. J. Hosp. Palliat. Nurs. 2017, 19, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Lyons, K.S.; Vellone, E.; Lee, C.S.; Cocchieri, A.; Bidwell, J.T.; D’Agostino, F.; Hiatt, S.O.; Alvaro, R.; Vela, R.J.; Riegel, B. A Dyadic Approach to Managing Heart Failure with Confidence. J. Cardiovasc. Nurs. 2015, 30, S64–S71. [Google Scholar] [CrossRef] [PubMed]
- Riegel, B.; Dickson, V.V. A Situation-Specific Theory of Heart Failure Self-Care. J. Cardiovasc. Nurs. 2008, 23, 190–196. [Google Scholar] [CrossRef]
- Riegel, B.; Dickson, V.V.; Faulkner, K.M. The Situation-Specific Theory of Heart Failure Self-Care Revised and Updated. J. Cardiovasc. Nurs. 2016, 31, 226–235. [Google Scholar] [CrossRef]
- Vellone, E.; Riegel, B.; Alvaro, R. A Situation-Specific Theory of Caregiver Contributions to Heart Failure Self-Care. J. Cardiovasc. Nurs. 2019, 34, 166–173. [Google Scholar] [CrossRef]
- Ciere, Y.; Cartwright, M.; Newman, S.P. A Systematic Review of the Mediating Role of Knowledge, Self-Efficacy and Self-Care Behaviour in Telehealth Patients with Heart Failure. J. Telemed. Telecare 2012, 18, 384–391. [Google Scholar] [CrossRef]
- Sousa, J.P.; Oliveira, C.; Pais-Vieira, M. Symptom Perception Management Education Improves Self-Care in Patients with Heart Failure. Work 2021, 69, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Karimi, M.; Clark, A.M. How Do Patients’ Values Influence Heart Failure Self-Care Decision-Making? A Mixed-Methods Systematic Review. Int. J. Nurs. Stud. 2016, 59, 89–104. [Google Scholar] [CrossRef]
- Spaling, M.A.; Currie, K.; Strachan, P.H.; Harkness, K.; Clark, A.M. Improving Support for Heart Failure Patients: A Systematic Review to Understand Patients’ Perspectives on Self-Care. J. Adv. Nurs. 2015, 71, 2478–2489. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.S.; Graven, L.J. Problems Experienced by Informal Caregivers of Individuals with Heart Failure: An Integrative Review. Int. J. Nurs. Stud. 2018, 80, 41–66. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.Y.; Oh, S.; Son, Y.J. Caring Experiences of Family Caregivers of Patients with Heart Failure: A Meta-Ethnographic Review of the Past 10 Years. Eur. J. Cardiovasc. Nurs. 2020, 19, 473–485. [Google Scholar] [CrossRef] [PubMed]
- Berg, C.A.; Upchurch, R. A Developmental-Contextual Model of Couples Coping with Chronic Illness across the Adult Life Span. Psychol. Bull. 2007, 133, 920–954. [Google Scholar] [CrossRef]
- Kitko, L.; McIlvennan, C.K.; Bidwell, J.T.; Dionne-Odom, J.N.; Dunlay, S.M.; Lewis, L.M.; Meadows, G.; Sattler, E.L.P.; Schulz, R.; Strömberg, A. Family Caregiving for Individuals with Heart Failure: A Scientific Statement from the American Heart Association. Circulation 2020, 141, e864–e878. [Google Scholar] [CrossRef]
- Lum, H.D.; Carey, E.P.; Fairclough, D.; Plomondon, M.E.; Hutt, E.; Rumsfeld, J.S.; Bekelman, D.B. Burdensome Physical and Depressive Symptoms Predict Heart Failure–Specific Health Status Over One Year. J. Pain Symptom Manag. 2016, 51, 963–970. [Google Scholar] [CrossRef]
- Strömberg, A.; Luttika, M.L. Burden of Caring: Risks and Consequences Imposed on Caregivers of Those Living and Dying with Advanced Heart Failure. Curr. Opin. Support. Palliat. Care 2015, 9, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Hwang, B.; Fleischmann, K.E.; Howie-Esquivel, J.; Stotts, N.A.; Dracup, K. Caregiving for Patients With Heart Failure: Impact on Patients’ Families. Am. J. Crit. Care 2011, 20, 431–442. [Google Scholar] [CrossRef]
- Bidwell, J.T.; Hostinar, C.E.; Higgins, M.K.; Abshire, M.A.; Cothran, F.; Butts, B.; Miller, A.H.; Corwin, E.; Dunbar, S.B. Caregiver Subjective and Physiological Markers of Stress and Patient Heart Failure Severity in Family Care Dyads. Psychoneuroendocrinology 2021, 133, 105399. [Google Scholar] [CrossRef]
- Schulz, R.; Beach, S.R.; Czaja, S.J.; Martire, L.M.; Monin, J.K. Family Caregiving for Older Adults. Annu. Rev. Psychol. 2020, 4, 635–659. [Google Scholar] [CrossRef]
- Timonet Andreu, E.M.; Morales Asencio, J.M.; Canca Sanchez, J.C.; Sepulveda Sanchez, J.; Mesa Rico, R.; Rivas Ruiz, F. Effects and Consequences of Caring for Persons with Heart Failure: (ECCUPENIC Study) a Nested Case-Control Study. J. Adv. Nurs. 2015, 71, 2987–2997. [Google Scholar] [CrossRef]
- Pressler, S.J.; Gradus-Pizlo, I.; Chubinski, S.D.; Smith, G.; Wheeler, S.; Sloan, R.; Jung, M. Family Caregivers of Patients with Heart Failure: A Longitudinal Study. J. Cardiovasc. Nurs. 2013, 28, 417–428. [Google Scholar] [CrossRef]
- Buck, H.G.; Hupcey, J.; Juárez-Vela, R.; Vellone, E.; Riegel, B. Heart Failure Care Dyadic Typology: Initial Conceptualization, Advances in Thinking, and Future Directions of a Clinically Relevant Classification System. J. Cardiovasc. Nurs. 2019, 34, 159–165. [Google Scholar] [CrossRef]
- Riegel, B.; Jaarsma, T.; Strömberg, A. A Middle-Range Theory of Self-Care of Chronic Illness. Adv. Nurs. Sci. 2012, 35, 194–204. [Google Scholar] [CrossRef]
- Rusbult, C.E.; Van Lange, P.A.M. Interdependence, Interaction, and Relationships. Annu. Rev. Psychol. 2003, 54, 351–375. [Google Scholar] [CrossRef]
- Campbell, L.; Kashy, D.A. Estimating Actor, Partner, and Interaction Effects for Dyadic Data Using PROC MIXED and HLM: A User-Friendly Guide. Pers. Relatsh. 2002, 9, 327–342. [Google Scholar] [CrossRef]
- Rayens, M.K.; Svavarsdottir, E.K. Focus on Research Methods: A New Methodological Approach in Nursing Research: An Actor, Partner, and Interaction Effect Model for Family Outcomes. Res. Nurs. Health 2003, 26, 409–419. [Google Scholar] [CrossRef]
- Ledermann, T.; Macho, S.; Kenny, D.A. Assessing Mediation in Dyadic Data Using the Actor-Partner Interdependence Model. Struct. Equ. Model. Multidiscip. J. 2011, 18, 595–612. [Google Scholar] [CrossRef]
- Lyons, K.S.; Sadowski, T.; Lee, C.S. The Role of Concealment and Relationship Quality on Patient Hospitalizations, Care Strain and Depressive Symptoms in Heart Failure Dyads. Eur. J. Cardiovasc. Nurs. 2020, 19, 118–124. [Google Scholar] [CrossRef]
- Thomson, P.; Howie, K.; Leslie, S.J.; Angus, N.J.; Andreis, F.; Thomson, R.; Mohan, A.R.M.; Mondoa, C.; Chung, M.L. Evaluating Emotional Distress and Healthrelated Quality of Life in Patients with Heart Failure and Their Family Caregivers: Testing Dyadic Dynamics Using the Actor-Partner Interdependence Model. PLoS ONE 2020, 15, e0227129. [Google Scholar] [CrossRef]
- Chung, M.L.; Moser, D.K.; Lennie, T.A.; Rayens, M.K. The Effects of Depressive Symptoms and Anxiety on Quality of Life in Patients with Heart Failure and Their Spouses: Testing Dyadic Dynamics Using Actor-Partner Interdependence Model. J. Psychosom. Res. 2009, 67, 29–35. [Google Scholar] [CrossRef]
- Al-Rawashdeh, S.Y.; Lennie, T.A.; Chung, M.L. The Association of Sleep Disturbances with Quality of Life in Heart Failure Patient-Caregiver Dyads. West. J. Nurs. Res. 2017, 39, 492–506. [Google Scholar] [CrossRef] [PubMed]
- Hooker, S.A.; Schmiege, S.J.; Trivedi, R.B.; Amoyal, N.R.; Bekelman, D.B. Mutuality and Heart Failure Self-Care in Patients and Their Informal Caregivers. Eur. J. Cardiovasc. Nurs. 2018, 17, 102–113. [Google Scholar] [CrossRef]
- Bidwell, J.T.; Vellone, E.; Lyons, K.S.; D’Agostino, F.; Riegel, B.; Juárez-Vela, R.; Hiatt, S.O.; Alvaro, R.; Lee, C.S. Determinants of Heart Failure Self-Care Maintenance and Management in Patients and Caregivers: A Dyadic Analysis. Res. Nurs. Health 2015, 38, 392–402. [Google Scholar] [CrossRef]
- Buck, H.G.; Mogle, J.; Riegel, B.; McMillan, S.; Bakitas, M. Exploring the Relationship of Patient and Informal Caregiver Characteristics with Heart Failure Self-Care Using the Actor-Partner Interdependence Model: Implications for Outpatient Palliative Care. J. Palliat. Med. 2015, 18, 1026–1032. [Google Scholar] [CrossRef]
- Vellone, E.; Chung, M.L.; Cocchieri, A.; Rocco, G.; Alvaro, R.; Riegel, B. Effects of Self-Care on Quality of Life in Adults with Heart Failure and Their Spousal Caregivers: Testing Dyadic Dynamics Using the Actor-Partner Interdependence Model. J. Fam. Nurs. 2014, 20, 120–141. [Google Scholar] [CrossRef]
- Shamali, M.; Konradsen, H.; Stas, L.; Østergaard, B. Dyadic Effects of Perceived Social Support on Family Health and Family Functioning in Patients with Heart Failure and Their Nearest Relatives: Using the Actor–Partner Interdependence Mediation Model. PLoS ONE 2019, 14, e0217970. [Google Scholar] [CrossRef]
- Strömberg, A.; Liljeroos, M.; Ågren, S.; Årestedt, K.; Chung, M.L. Associations Among Perceived Control, Depressive Symptoms, and Well-Being in Patients With Heart Failure and Their Spouses: A Dyadic Approach. J. Cardiovasc. Nurs. 2021, 36, 198–205. [Google Scholar] [CrossRef]
- Lyons, K.S.; Hiatt, S.O.; Gelow, J.M.; Auld, J.; Mudd, J.O.; Chien, C.V.; Lee, C.S. Depressive Symptoms in Couples Living with Heart Failure: The Role of Congruent Engagement in Heart Failure Management. Aging Ment. Health 2018, 22, 1585–1591. [Google Scholar] [CrossRef]
- Vellone, E.; Chung, M.L.; Alvaro, R.; Paturzo, M.; Dellafiore, F. The Influence of Mutuality on Self-Care in Heart Failure Patients and Caregivers: A Dyadic Analysis. J. Fam. Nurs. 2018, 24, 563–584. [Google Scholar] [CrossRef]
- Dellafiore, F.; Chung, M.L.; Alvaro, R.; Durante, A.; Colaceci, S.; Vellone, E.; Pucciarelli, G. The Association between Mutuality, Anxiety, and Depression in Heart Failure Patient-Caregiver Dyads. J. Cardiovasc. Nurs. 2019, 34, 465–473. [Google Scholar] [CrossRef]
- Bugajski, A.; Buck, H.; Zeffiro, V.; Morgan, H.; Szalacha, L.; Alvaro, R.; Vellone, E. The Influence of Dyadic Congruence and Satisfaction with Dyadic Type on Patient Self-Care in Heart Failure. Eur. J. Cardiovasc. Nurs. 2020. [Google Scholar] [CrossRef]
- Kitko, L.A.; Hupcey, J.E.; Pinto, C.; Palese, M. Patient and Caregiver Incongruence in Advanced Heart Failure. Clin. Nurs. Res. 2015, 24, 388–400. [Google Scholar] [CrossRef]
- Bidwell, J.T.; Lyons, K.S.; Lee, C.S. Caregiver Well-Being and Patient Outcomes in Heart Failure a Meta-Analysis. J. Cardiovasc. Nurs. 2017, 32, 372–382. [Google Scholar] [CrossRef]
- Cameron, J.; Thompson, D.R.; Szer, D.; Greig, J.; Ski, C.F. Dyadic Incongruence in Chronic Heart Failure: Implications for Patient and Carer Psychological Health and Self-Care. J. Clin. Nurs. 2017, 26, 4804–4812. [Google Scholar] [CrossRef] [PubMed]
- Retrum, J.H.; Nowels, C.T.; Bekelman, D.B. Patient and Caregiver Congruence: The Importance of Dyads in Heart Failure Care. J. Cardiovasc. Nurs. 2013, 28, 129–136. [Google Scholar] [CrossRef]
- Lee, C.S.; Mudd, J.O.; Auld, J.; Gelow, J.M.; Hiatt, S.O.; Chien, C.V.; Bidwell, J.T.; Lyons, K.S. Patterns, Relevance and Predictors of Heart Failure Dyadic Symptom Appraisal. Eur. J. Cardiovasc. Nurs. 2017, 16, 595–604. [Google Scholar] [CrossRef]
- Thompson, S.C.; Kyle, D.J. The Role of Perceived Control in Coping with the Losses Associated with Chronic Illness. In Loss and Trauma: General and Close Relationship Perspectives; Harvey, J.H., Miller, J.H., Eds.; Brunner-Routledge: Abingdon, UK, 2000; pp. 131–145. [Google Scholar]
- Olchowska-Kotala, A. Illness Representations in Individuals with Rheumatoid Arthritis and the Willingness to Undergo Acupuncture Treatment. Eur. J. Integr. Med. 2013, 5, 347–351. [Google Scholar] [CrossRef]
- Lowe, R.; Norman, P. Information Processing in Illness Representation: Implications from an Associative-Learning Framework. Health Psychol. 2017, 36, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, I.M. The Health Belief Model and Personal Health Behavior. Health Educ. Monogr. 1974, 2, 354–386. [Google Scholar] [CrossRef]
- Jones, C.L.; Jensen, J.D.; Scherr, C.L.; Brown, N.R.; Christy, K.; Weaver, J. The Health Belief Model as an Explanatory Framework in Communication Research: Exploring Parallel, Serial, and Moderated Mediation. Health Commun. 2015, 30, 566. [Google Scholar] [CrossRef] [PubMed]
- Hooker, S.A.; Grigsby, M.E.; Riegel, B.; Bekelman, D.B. The Impact of Relationship Quality on Health-Related Outcomes in Heart Failure Patients and Informal Family Caregivers: An Integrative Review. J. Cardiovasc. Nurs. 2015, 30, S52–S63. [Google Scholar] [CrossRef]
- Chung, M.L.; Lennie, T.A.; Mudd-Martin, G.; Dunbar, S.B.; Pressler, S.J.; Moser, D.K. Depressive Symptoms in Patients with Heart Failure Negatively Affect Family Caregiver Outcomes and Quality of Life. Eur. J. Cardiovasc. Nurs. 2016, 15, 30–38. [Google Scholar] [CrossRef]
- Timonet-Andreu, E.; Morales-Asencio, J.M.; Alcalá Gutierrez, P.; Cruzado Alvarez, C.; López-Moyano, G.; Mora Banderas, A.; López-Leiva, I.; Canca-Sanchez, J.C. Health-Related Quality of Life and Use of Hospital Services by Patients with Heart Failure and Their Family Caregivers: A Multicenter Case-Control Study. J. Nurs. Scholarsh. 2020, 52, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Jorge-Samitier, P.; Durante, A.; Gea-Caballero, V.; Antón-Solanas, I.; Fernández-Rodrigo, M.T.; Juárez-Vela, R. Sleep Quality in Patients with Heart Failure in the Spanish Population: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 7772. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Schlesinger, S.; Leitzmann, M.F.; Tonstad, S.; Norat, T.; Riboli, E.; Vatten, L.J. Physical Activity and the Risk of Heart Failure: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Eur. J. Epidemiol. 2021, 36, 367–381. [Google Scholar] [CrossRef]
- Lindgren, M.; Börjesson, M. The Importance of Physical Activity and Cardiorespiratory Fitness for Patients with Heart Failure. Diabetes Res. Clin. Pract. 2021, 176, 108833. [Google Scholar] [CrossRef]
- Pinchera, B.; Delloiacono, D.; Lawless, C.A. Best Practices for Patient Self-Management: Implications for Nurse Educators, Patient Educators, and Program Developers. J. Contin. Educ. Nurs. 2018, 49, 432–440. [Google Scholar] [CrossRef]
- Huntsinger, M.E.; Rabara, R.; Peralta, I.; Doshi, R.N. Current Technology to Maximize Cardiac Resynchronization Therapy Benefit for Patients With Symptomatic Heart Failure. AACN Adv. Crit. Care 2015, 26, 329–340. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).