Abstract
The aim of this systematic review was to evaluate the impact of a traumatic dental injury (TDI) of permanent teeth in children and adolescents on their oral health-related quality of life (OHRQoL) as well as on their families. A bibliographic search in the biomedical databases (PubMed, Cochrane Library, MEDLINE) was limited to studies published between January 2000 and February 2021. The study selection criteria were cross-sectional, case control, or prospective clinical studies, which analyzed TDI before and after the treatment of permanent teeth in healthy children and adolescent, assessed their OHRQoL, and were written in English. The search found 25 eligible articles that were included in the study. The quality assessment of the studies was performed using the quality assessment checklist for survey studies in psychology (Q-SSP). The results indicated that a TDI of permanent teeth strongly influences the OHRQoL of children and adolescents, and the timely-performed dental management of a TDI allows for preventing further biological and socio-psychological impacts. Sociodemographic status, economic status, parent’s education, gender, age group, and type of schooling were determinants of the TDI impact on OHRQoL.
1. Introduction
Quality of life is described as “an individual’s perception of their place in life concerning goals, aspirations, standards, and concerns in the sense of the culture and values in which they reside” [1]. The definition of oral health-related quality of life (OHRQoL) refers to how oral health or disease affects an individual’s everyday work, well-being, and, as a result, their overall quality of life [2]. The quality of life is highly affected by their state of health. Physical and psychological constraints in the field of dentistry can directly affect eating, speech, social interaction, and self-esteem [3]. A traumatic dental injury (TDI) is an irreversible disease that is attracting more consideration from health practitioners at the moment [4]. A TDI, especially in children, is considered a severe health issue. Maxillary anterior teeth are the most affected teeth that cause physical, aesthetic, and psychological problems for children and their parents [5,6]. The quality of life is a complex process, and each person’s self-perceptions are shaped by their experiences, future expectations, dreams, and lifestyle [7]. Besides that, people change their view of their OHRQoL over time [8]. The second-most prevalent TDI is a crown fracture involving enamel and dentin (CFED). It is associated with trouble feeding, avoidance of smiling, sensitivity and discomfort, and a higher prevalence of adverse effects on OHRQoL [9,10]. Traumatic dental injuries to permanent teeth are more frequent than in primary dentition [11,12]. Dental injuries primarily concern the maxillary anterior teeth. Falls, sporting events, road traffic accidents, and bicycling are the most common causes of these injuries. Dental trauma predisposing factors may be related to the anatomical characteristics of the individual, such as increased overjet, insufficient lip coverage of the upper anterior teeth, etc. [13,14]. Home and school are areas where dental accidents frequently occur. It was observed that the place of injury was gender-related, i.e., the school followed by the home was the most common place of injury for boys, whereas this finding is vice versa for girls [15,16,17].
In everyday dental practice, treating dental injuries is not an ordinary condition. The result of the procedure is closely linked to the dentist’s expertise and skills and the medical assistance at the injury site. Thus, the dentist, parents, teachers, and coaches must have basic knowledge of dental trauma emergency management. However, the rareness of a TDI and the uncertainty of treatment prognosis, an individual with a traumatized tooth becomes a concern for the dentist. It is not a routine operation for most dentists and requires accurate diagnosis, appropriate emergency management, and correct follow-up treatment.
In the case of dental trauma, all treatment methods are aimed to mitigate undesired complications that may contribute to the loss of the tooth and the loss of the alveolar bone and thereby hinder the realization of a potential treatment plan. It is important to remember that traumatic dental injury care is vital for young people. It is essential to realize that treatment of a traumatic dental injury in a young patient is often complicated, unpredictable, expensive, and can continue for the remainder of his/her life. Since most of traumatic injuries in permanent dentition are between the ages of 10–12 years, dental trauma may have a lifelong effect on the child’s quality of life [18]. Therefore, the objective of this systematic review aims to assess the impact of a traumatic dental injury of permanent teeth on oral health-related quality of life and to assess the study quality using the Q-SSP checklist.
2. Materials and Methods
The review protocol was registered at PROSPERO (international prospective register of systematic reviews), bearing registration number CRD42021230281.
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines [19].
2.1. Search Strategy
The following structured question was outlined based on PICO (Patient or problem in question; Intervention of interest; Comparison of intervention; Outcomes): “Does trauma and treatment of traumatic injuries influence the OHRQoL of children and adolescents with a TDI and also how it impacts their family members?”.
The electronic search strategy is described in Table 1. A comprehensive electronic search for relevant articles was performed in the following databases: PubMed, Cochrane Library, MEDLINE, and Google Scholar. For all these databases, Boolean operators (OR, AND) were used to combine and narrow down searches that included appropriate MeSH terms, keywords, and other terms following the syntax rules of each database. All references selected in the search were saved in Mendeley Desktop software to remove the duplicates.

Table 1.
Search strategy.
2.2. Study Selection
The literature search was limited to articles available in English and to those published between January 2000 and February 2021. Each article was assessed carefully and in detail.
Two independent reviewers (PD and LM) read abstracts and titles, and studies not pertaining to the research question were excluded. The remaining relevant studies’ full texts were read and analyzed independently. In this selection, if there was a disagreement of opinions, a third reviewer (DJ) was called to achieve a consensus.
The selection of studies was performed with no restrictions of place or year of publication. However, the restriction of language was applied, and only those articles written in English language were included. Titles and abstracts were analyzed to determine whether they fulfilled the inclusion criteria: (i) population: healthy children, adolescents, and family members; (ii) exposition: subjects experienced a TDI; (iii) outcome: impact on OHRQoL. The inclusion and exclusion criteria are depicted in Table 2.
Table 2.
Inclusion and exclusion criteria of selecting studies for systematic review.
Two reviewers (LM and SG) conducted the data extraction and collected the information independently. The relevant data of the included studies were extracted in detail, using Excel spreadsheet (Microsoft, Redmond, WA, USA, Version 2007). The extracted data included: title, journal name, year of publication, type of study, author, country, age group, instrument/application form, TDI index, sample size, tooth number, an association between TDI and OHRQoL, result, conclusion, publication, sample, country where the research was conducted, sample age, comparison, instrument applied, instrument purpose, TDI index, and type of treatment. Mean scores for the OHRQoL instruments (total scale and sub-scales) before and after treatment, p-value, and outcome were also identified.
2.3. Study Quality Assessment
The quality of the individual studies was assessed by one reviewer (PD) and independently checked for agreement by a second reviewer (LM). In case of disagreement, a third review author (DJ) was consulted. The quality assessment of the included studies was conducted using the quality assessment checklist for survey studies in psychology (Q-SSP) (Figure 1) [20], published in the year 2020, which includes 20 checklist items. The Q-SSP checklist has been developed to standardize responses to uniform quality assessment across researchers [20]. The quality was judged for each domain and is expressed as a percentage by dividing YES (Y) scores by the total (T) number of APPLICABLE items and multiplying by 100. When (T) = 20, then a Y/T ≥ 75% score may be considered acceptable quality. When (T) = 19, then a Y/T ≥ 73% score may be considered acceptable quality. When (T) = 18, then a Y/T ≥ 72% score may be considered acceptable quality. When (T) = 17, then a Y/T ≥ 70% score may be considered acceptable quality. If the report fails to attain a Y score for five items, it may be classified as having questionable quality. The assessment was added to an Excel spreadsheet and then imported into ROBVIS (Risk of Bias Visualization web app software).
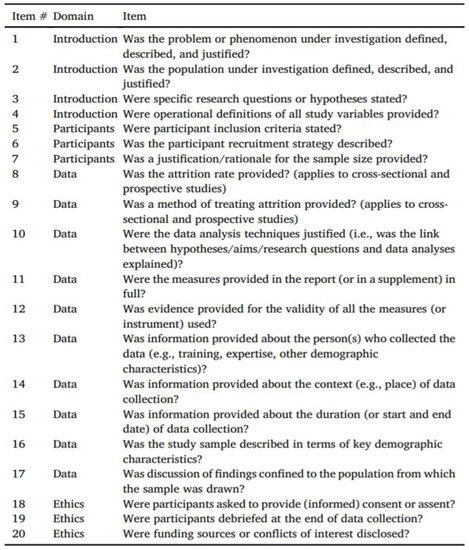
Figure 1.
Q-SSP checklist for assessing quality of included studies.
3. Results
3.1. Selection of Studies
Figure 2 presents a flowchart of the systematic review process. The search in the selected databases allowed for the identification of 2677 articles. After removing duplicates, 2350 searches remained. Of these, 2297 were excluded after reading the titles and abstracts. From 53 remaining articles, 25 articles were finally selected after reading the full texts. Table A1 in Appendix A presents a list of the studies excluded after reading the full texts and the justification.
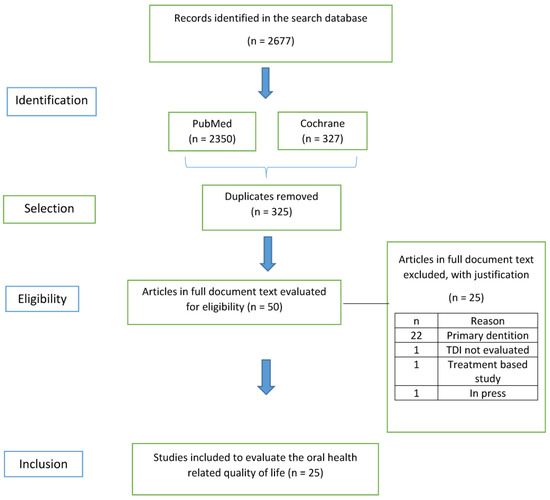
Figure 2.
PRISMA 2020 flow diagram for systematic review that includes searches of databases.
3.2. Characteristics of Studies
Most of the studies were cross-sectional [9,15,20,21,22,23,24,25,26,27,28,29,30], six studies were case control [31,32,33,34,35,36], and three studies were prospective clinical studies [37,38,39].
Nine studies [15,21,24,25,29,31,32,33,35] evaluated patients with TDI and no TDI, whereas eight studies [9,26,37,38,39,40,41,42] evaluated patients with TDI and after TDI treatment. One study [43] compared TDI and TDI with treatment needs. Another study [27] compared no TDI with TDI or without treatment needs. One study [22] evaluated TDI with no oral condition and TDI associated with dental caries, one study [23] evaluated mild/no TDI with severe TDI, one compared TDI with no treatment and TDI followed by treatment, two studies [28,30] evaluated patients with trauma, and one study [34] evaluated patients with TDI with unmet treatment needs and without TDI.
The included studies used different instruments to assess the OHRQoL (Table 3). From 25 included studies, the most widely used instrument for assessing OHRQoL of permanent teeth was the Child Perceptions Questionnaire (CPQ) (n = 15). The form of application most used was self-administered (n = 22). The Oral Impact on Daily Performances (OIDP) was used in five articles. The Family Impact Scale (FIS) was used in three articles, the Parental–Caregivers Perceptions Questionnaire (P-CPQ) in three articles, and the Oral Health Impact Profile (OHIP) in one study. One study used the National Research in Oral health (SBBrasil2010). Andreasen proposed the index for the TDI registry used by 15 articles. Seven articles used O’ Brien, one article used the Dental Trauma Index (DTI), and two articles used WHO 1997 for TDI registry. Regarding TDI association and impact on OHRQoL, 24 articles indicated an association, whereas one article indicated no association.
Table 3.
Data extraction of included studies.
3.3. Analysis of Quality of the Studies
Risk of bias in included studies is presented in Figure 3 and Figure 4. Out of the 25 included articles, 21 articles are of acceptable quality scoring 75%, whereas 4 articles are of questionable quality with a score of <75%.
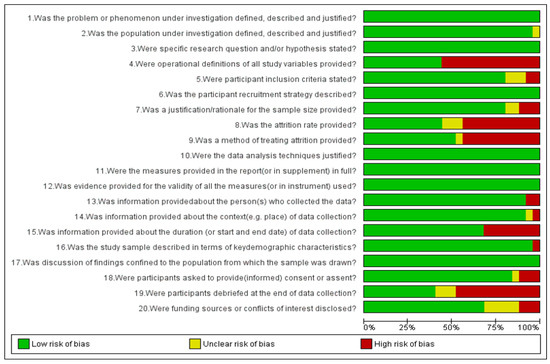
Figure 3.
Quality assessment of studies using a QSSP tool graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies.
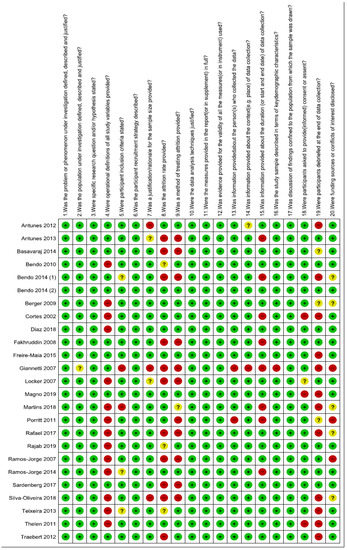
Figure 4.
Quality assessment of included studies summary: review authors’ judgements about each risk of bias item for each included study.
3.4. Synthesis of Results
Due to a high heterogeneity of the data, it was not possible to perform a meta-analysis for all the parameters used in the included studies; therefore, a qualitative assessment was performed. Table 4 shows the value of each domain and its impact on OHRQoL.
Table 4.
Data extraction of included studies—the value of each domain and its impact on OHRQoL.
4. Discussion
This review included 25 studies (Table 1) that assessed the impact of a traumatic dental injury of permanent teeth on the oral health-related quality of life (OHRQoL) in children and adolescent patients. The subjective evaluation of OHRQoL “reflects people’s comfort when eating, sleeping, and engaging in social interaction; their self-esteem; and their satisfaction concerning their oral health” [44]. With a growing emphasis on health promotion and illness prevention in health policy, OHRQoL has evolved to include positive and negative assessments of oral health and health outcomes [45]. As a result, oral health assessments might reveal both negative and positive effects on self-esteem and well-being.
We assessed the quality of the studies using the Q-SSP tool [20]. This tool helps researchers to perform a uniform quality assessment of survey studies in psychology across the globe. Using tools such as the Q-SSP checklist to evaluate study quality will raise the profile of reporting standards and drive greater precision in reporting the survey study methods. Researchers can use the tool to assess the quality of studies as an inclusion criterion in systematic reviews and meta-analyses. In addition, the tool may be used by professional clinicians, physicians, and practitioners wishing to evaluate the quality of psychological evidence that may inform their practice. It may also be helpful for educators to illustrate issues relating to study quality in research method courses.
Most of the studies used for evaluation of OHRQoL of patients with a TDI or a TDI with treatment needs were of acceptable quality, except for four studies [22,25,31,41], which had questionable quality (Figure 2). Therefore, the conclusion of these articles will be taken with caution. Seven tools were used in this systematic review. These were the P-CPQ tool, P-CPQ + CPQ(8–10), (11–14) + FIS, CPQ(8–10), CPQ(11–14)-16 short form and ten short forms, the Brazilian version of FIS, Oral Health Impact Profile (OHIP-14), Child-OIDP, and OIDP.
The most common tool used for the assessment of OHRQoL was CPQ(11–14) in 10 studies [15,25,26,27,29,31,33,41,42,43]. All questionnaire variations evaluated the impact of oral and orofacial conditions in children at symptomatic, functional, emotional, and social levels. To date, the CPQ has been translated, validated, and adapted to suit several languages and socio-cultural contexts, demonstrating its applicability and perfect psychometric properties on numerous clinical and epidemiological occasions [46].
The Child-OIDP was the second-most used tool for assessing the OHRQoL in children in five studies [9,28,34,35,36]. Child-OIDP and CPQ (11–14) differ in their aim and theoretical framework. The Child-OIDP has an advantage over the CPQ and other OHRQoL measures, as it specifies the different clinical causes of each oral impact [47,48]. The Child-OIDP has a greater sensitivity than CPQ in identifying the impact on the quality of life of schoolchildren with a TDI.
Due to much heterogeneity in the data, it was not possible to perform a meta-analysis for all the parameters used in studies; therefore, qualitative assessment was conducted. However, meta-analysis was possible for only two studies using the Child OIDP tool.
Most of the studies [24,25,29,31,32,33,35] that evaluated patients with TDI and no TDI revealed that patients with TDI have a negative impact on the OHRQoL, whereas in other studies [37,38,41] where TDI patients were compared based on whether they received treatment or not, they revealed that patients who received treatment had a positive impact on OHRQoL.
All the tools that analyzed the OHRQoL assessed the patient and their parents in various parameters, including sociodemographic status, economic status, parent’s education, gender, age group, and type of schooling. All these factors affected the OHRQoL of children, except for the type of schooling.
It was expected that a higher prevalence of TDI is in males compared to females [26], due to males being more engaged in sports and recreational activities involving physical contact. However, due to a change in social roles, adolescent females also pose an equal risk of TDI, as there is an increase in their participation in sports. Females are currently exposed to the same etiological factors. However, variations between genders may occur due to environmental, cultural, and behavioral factors, which are determinants of a stronger or weaker association between TDI and gender [49,50,51]. However, although four studies [25,26,28,31] out of eight [23,24,25,26,27,28,31,41] showed no association between gender and its impact on OHRQoL, another three studies [23,24,41] did imply that there is a strong association of TDI impact on OHRQoL among females compared to males. This outcome can be due to more significant aesthetic concerns of females than males, which negatively impacts their appearance [52,53,54].
All the studies expressed that the child perception of TDI impact on the OHRQoL does not change with age. Children between the age group of 8–10 years have criteria similar to those of children between 11–14 years regarding the self-perception of body image. To evaluate their appearance, children compare themselves to others of their age, and the judgment of peers exerts an influence on the development of self-esteem [55].
However, parents of the older children perceived a more significant reduction in their QoL than the parents of the 8–10-year-old group with TDI. This more remarkable impact on parents of the older children may be due to their children’s growing independence suddenly being reversed by the need for parental intervention and supervision [40].
Seven out of 10 studies evaluated another parameter that negatively impacts TDI associated OHRQoL: the family’s socioeconomic status of [9,21,24,27,29,30,34]. Due to their existing living conditions, which are usually less privileged and peripheries of urban areas, where facilities and quality healthcare are questionable, children are often exposed to unsafe environments. These underdeveloped areas increase accidents due to poorly-designed urban projects and neglected public spaces [56,57,58].
Even if parents wished to have the child’s condition treated, they cannot afford dental care at both private and public centers [59].
Parents’ education also impacts the OHRQoL of children with a TDI. Six studies [9,21,24,29,30,34] out of nine reported that fewer years of parents’ education level showed a negative impact on OHRQoL of children. The majority of parents in these studies had low education status. This reflects their lack of information, perception, and treatment needs associated with TDI and negatively influenced the child’s health behaviors.
Children with severe TDI also impacted the family regarding parental/family activity, parental emotions, family conflict, and financial burden [29,38,40]. Severe types of trauma more often affected the daily life of parents/caregivers. Parents/caregivers of adolescents with fractures involving the dentine or dentine/pulp reported more negative impact on parental/family activities than those with less severe TDI, such as enamel fracture [29]. A TDI is an unexpected event. More severe cases nearly always require urgent care and multiple searches for dental treatment, resulting in parents missing work and spending extra time taking care of their children. From these studies, it can be concluded that severe trauma not only affects the child in question, but it also affects the family.
Individual domains such as oral symptoms (OS), emotional well-being (EWB), social well-being (SWB), and functional limitations (FL) were mainly analyzed by different studies. These domains are individuals perception of TDI and their overall impact on OHRQoL. It was pretty evident that the most affected domains were EWB, OS, and FL. TDI was significantly affected by these three domains. The “emotional well-being” domain contains questions related to emotions such as sad, embarrassed, worried, upset, frustrated, angry, and concerned about what others think. Physical appearance and attractiveness play an essential role in social interactions and psychological well-being among adolescents between the ages of 11 and 14 [60]. Peer relationships are an important factor in an individual’s quality of life at this age [61]. Because the mouth is such a significant predictor of face attractiveness, any changes in dental features can have a detrimental or good impact on the quality of life [62]. The ‘oral symptoms’ domain contains questions about pain, wounds, mouth sores, bad breath, and food remains trapped in the mouth [38]. As this domain contains questionnaires related to lips, teeth, and jaws, the scores were high in this domain and thus affected the OHRQoL. The “functional limitations” domain contains questions related to difficulty with eating, biting, speaking, and sleeping. The overall cumulative effect of the individual domain significantly affected the TDI-associated OHRQoL.
Children with fractured teeth experienced more impacts on their daily living than children with no traumatic dental injury. Their actual daily basic performances such as ‘eating and enjoying food’, ‘cleaning teeth’, ‘smiling, laughing, and showing teeth without embarrassment’, ‘maintaining usual emotional state without being irritable’, and ‘enjoying contact with people’ significantly affected the OHRQoL when compared to children with no dental trauma experience [35].
It was observed that, after receiving the treatment of TDI, children were able to enjoy foods, smile, show one’s teeth without embarrassment, and socialize. Thus, dental treatment following a TDI is an important prevention strategy regarding biological and socio-psychological impacts [9]. Treatment of TDI improved the OHRQoL considerably.
5. Conclusions
Traumatic injuries to permanent dentition affect both a child and their caregivers or parents. These injuries affect both genders; however, adolescent girls tend to have a more negative impact on their OHRQoL than boys. A TDI and its severity significantly affect children and their families social and emotional well-being. Parents’ education and socioeconomic status play a significant role in providing care and treatment of TDIs in children. Treatment of TDIs improve the aesthetic and functional aspects of dentition and enhance the OHRQoL. Since the majority of studies used well-validated questionnaire tools and were of high quality, it can be concluded that the TDI impact on the OHRQoL is significant.
Author Contributions
Conceptualization, L.M. and P.D.; methodology, L.M.; software, B.L.; validation, L.M., D.J. and P.D.; formal analysis, L.M.; investigation, S.G.; resources, S.P.; data curation, P.D.; writing—original draft preparation, L.M.; writing—review and editing, B.L.; visualization, L.M.; supervision, B.L.; project administration, L.M.; funding acquisition, B.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We thank the Institute of Dental Sciences, Cochrane India Network for helping us with the resources required for the study.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| CFED | crown fracture involving enamel and dentin |
| COHQoL | Child Oral Health Quality of Life |
| CPQ | Child Perceptions Questionnaire |
| Child-OIDP | Child-Oral Impact on Daily Performances |
| FIS | Family Impact Scale in three articles |
| ISF | Impact Short Form |
| OIDP | Oral Impact on Daily Performances |
| OHIP | Oral Health Impact Profile |
| OHRQoL | Oral Health-Related Quality of Life |
| P-CPQ | Parental–Caregivers Perceptions Questionnaire |
| Q-SSP | Quality assessment checklist for survey studies in psychology |
| TDI | Traumatic Dental Inury |
Appendix A
Table A1 presents a list of the studies excluded from the review after reading their full texts.
Table A1.
List of excluded studies after reading the full text.
Table A1.
List of excluded studies after reading the full text.
| Author | Title | Reason for Exclusion |
|---|---|---|
| Flores et al. [63] | How Does Orofacial Trauma in Children Affect the Developing Dentition? Long-term Treatment and Associated Complications | The OHRQoL was not checked. It is a treatment-based study. |
| Gomes et al. [64] | Oral Problems and Self-Confidence in Preschool Children | This study was conducted in primary dentition. |
| Cengiz et al. [65] | Impact of seizure-related injuries on quality of life | TDI has not been evaluated. |
| Sakaryali et al. [66] | Evaluation of the Impact of Early Childhood Caries, Traumatic Dental Injury, and Malocclusion on Oral Health–Related Quality of Life for Turkish Preschool Children and Families | The study was conducted in primary dentition. |
| Soares et al. [10] | The impact of crown fracture in the permanent dentition on children’s quality of life | This article is not published in any journal and is in press. |
| Gonçalves et al. [67] | Impact of dental trauma and esthetic impairment on the quality of life of preschool children. | The study was conducted in primary dentition. |
| Braimah et al. [68] | Self-esteem following maxillofacial and orthopedic injuries: preliminary observations in sub-Saharan Africans | This study did not include permanent dentition. |
| Ramos-Jorge et al. [69] | Parents’ recognition of dental trauma in their children | This study was conducted in primary dentition. |
| Ramos-Jorge et al. [70] | Effect of dark discolouration and enamel/dentine fracture on the oral health-related quality of life of pre-schoolers | This study was conducted in primary dentition. |
| Granville-Garcia et al. [71] | Parental influence on children’s answers to an oral-health-related quality of life questionnaire | This study was conducted in primary dentition. |
| Vieira-Andrade et al. [72] | Impact of traumatic dental injury on the quality of life of young children: a case–control study | This study was conducted in primary dentition. |
| Aldrigui et al. [73] | Impact of traumatic dental injuries and malocclusions on quality of life of young children | This study was conducted in primary dentition. |
| Firmino et al. [74] | Impact of oral health problems on the quality of life of preschool children: a case-control study | This study was conducted in primary dentition. |
| Barbosa Neves et al. [75] | Perception of parents and self-reports of children regarding the impact of traumatic dental injury on quality of life | This study was conducted in primary dentition. |
| Siqueira et al. [76] | Impact of Traumatic Dental Injury on the Quality of Life of Brazilian Preschool Children | This study was conducted in primary dentition. |
| Viegas et al. [77] | Influence of traumatic dental injury on quality of life of Brazilian preschool children and their families | This study was conducted in primary dentition. |
| Gomes et al. [78] | Impact of oral health conditions on the quality of life of preschool children and their families: a cross-sectional study | This study was conducted in primary dentition. |
| Abanto et al. [79] | Impact of traumatic dental injuries and malocclusions on quality of life of preschool children: a population-based study | This study was conducted in primary dentition. |
| Abanto et al. [80] | The impact of dental caries and trauma in children on family quality of life | This study was conducted in primary dentition. |
| Abanto et al. [81] | Impact of dental caries and trauma on quality of life among 5- to 6-year-old children: perceptions of parents and children | This study was conducted in primary dentition. |
| Feldens et al. [82] | Enamel fracture in the primary dentition has no impact on children’s quality of life: implications for clinicians and researchers | This study was conducted in primary dentition. |
| Scarpelli et al. [83] | Oral health-related quality of life among Brazilian preschool children | This study was conducted in primary dentition. |
| Viegas et al. [84] | Impact of Traumatic Dental Injury on Quality of Life Among Brazilian Preschool Children and Their Families | This study was conducted in primary dentition. |
| Kramer et al. [85] | Exploring the impact of oral diseases and disorders on quality of life of preschool children | This study was conducted in primary dentition. |
| Borges et al. [86] | Relationship between overweight/obesity in the first year of age and traumatic dental injuries in early childhood: Findings from a birth cohort study | This study was conducted in primary dentition. |
References
- Goursand, D.; Paiva, S.M.; Zarzar, P.M.; Pordeus, I.A.; Grochowski, R.; Allison, P.J. Measuring parental-caregiver perceptions of child oral health-related quality of life: Psychometric properties of the Brazilian version of the P-CPQ. Braz. Dent. J. 2009, 20, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Pahel, B.T.; Rozier, R.G.; Slade, G.D. Parental perceptions of children’s oral health: The Early Childhood Oral Health Impact Scale (ECOHIS. Health Qual. Life Outcomes 2007, 5, 6. [Google Scholar] [CrossRef] [PubMed]
- Sheiham, A.; Steele, J.G.; Marcenes, W.; Tsakos, G.; Finch, S.; Walls, A.W.G. Prevalence of impacts of dental and oral disorders and their effects on eating among older people; a national survey in Great Britain. Community Dent. Oral Epidemiol. 2001, 29, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Sgan-Cohen, H.D.; Megnagi, G.; Jacobi, Y. Dental trauma and its association with anatomic, behavioral, and social variables among fifth and sixth grade schoolchildren in Jerusalem. Community Dent. Oral Epidemiol. 2005, 33, 174–180. [Google Scholar] [CrossRef]
- Cardoso, M.; De Carvalho Rocha, M.J. Traumatized Primary Teeth in Children Assisted at the Federal University of Santa Catarina, Brazil. Dent. Traumatol. 2002, 18, 129–133. [Google Scholar] [CrossRef]
- Şaroğlu, I.; Sönmez, H. The prevalence of traumatic injuries treated in the pedodontic clinic of Ankara University, Turkey, during 18 months. Dent. Traumatol. 2002, 18, 299–303. [Google Scholar] [CrossRef]
- Eiser, C.; Morse, R. The measurement of quality of life in children: Past and future perspectives. J. Dev. Behav. Pediatr. JDBP 2001, 22, 248–256. [Google Scholar] [CrossRef]
- Allison, P.J.; Locker, D.; Feine, J.S. Quality of life: A dynamic construct. Soc. Sci. Med. 1982, 45, 221–230. [Google Scholar] [CrossRef]
- Ramos-Jorge, J.; Paiva, S.M.; Tataounoff, J.; Pordeus, I.A.; Marques, L.S.; Ramos-Jorge, M.L. Impact of treated/untreated traumatic dental injuries on quality of life among Brazilian schoolchildren. Dent. Traumatol. 2014, 30, 27–31. [Google Scholar] [CrossRef]
- Soares, J.P.; Barasuol, J.C.; Torres, F.M.; Giacomin, A.; Gonçalves, B.M.; Klein, D.; Borgatto, A.F.; Ramos-Jorge, M.L.; Cardoso, M.; Bolan, M. The impact of crown fracture in the permanent dentition on children’s quality of life. Dent. Traumatol. 2018, 34, 158–163. [Google Scholar] [CrossRef]
- Marcenes, W.; Beiruti, N.; Tayfour, D.; Issa, S. Epidemiology of traumatic injuries to the permanent incisors of 9-12-year-old schoolchildren in Damascus, Syria. Endod Dent. Traumatol. 1999, 15, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Granville-Garcia, A.F.; de Menezes, V.A.; de Lira, P.I.C. Dental trauma and associated factors in Brazilian preschoolers. Dent. Traumatol. 2006, 22, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Årtun, J.; Behbehani, F.; Al-Jame, B.; Kerosuo, H. Incisor trauma in an adolescent Arab population: Prevalence, severity, and occlusal risk factors. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Traebert, J.; Bittencourt, D.D.; Peres, K.G.; Peres, M.A.; de Lacerda, J.T.; Marcenes, W. Aetiology and rates of treatment of traumatic dental injuries among 12-year-old school children in a town in southern Brazil. Dent. Traumatol. 2006, 22, 173–178. [Google Scholar] [CrossRef]
- Bendo, C.B.; Paiva, S.M.; Torres, C.S.; Oliveira, A.C.; Goursand, D.; Pordeus, I.A. Association between treated/untreated traumatic dental injuries and impact on quality of life of Brazilian schoolchildren. Health Qual. Life Outcomes 2010, 8, 114. [Google Scholar] [CrossRef]
- Noori, A.J.; Al-Obaidi, W.A. Traumatic dental injuries among primary school children in Sulaimani city, Iraq. Dent. Traumatol. 2009, 25, 442–446. [Google Scholar] [CrossRef]
- Fakhruddin, K.S.; Lawrence, H.P.; Kenny, D.J.; Locker, D. Etiology and environment of dental injuries in 12- to 14-year-old Ontario schoolchildren. Dent. Traumatol. 2008, 24, 305–308. [Google Scholar] [CrossRef]
- Zaleckiene, V.; Peciuliene, V.; Brukiene, V.; Drukteinis, S. Traumatic dental injuries: Etiology, prevalence and possible outcomes. Stomatologija 2014, 16, 7–14. [Google Scholar]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef]
- Protogerou, C.; Hagger, M.S. A checklist to assess the quality of survey studies in psychology. Methods Psychol. 2020, 3, 100031. [Google Scholar] [CrossRef]
- Díaz, S.; Vélez, M.P.; Martínez, L.M.; Ramos, K.; Boneckër, M.; Martins Paiva, S.; Abanto, J. Parental perceptions of impact of oral disorders on Colombian schoolchildren’s oral healthrelated quality of life. Acta. Odontol. Latinoam. 2018, 31, 82–90. [Google Scholar] [PubMed]
- Martins, M.T.; Sardenberg, F.; Bendo, C.B.; Vale, M.P.; Paiva, S.M.; Pordeus, I.A. Dental caries are more likely to impact on children’s quality of life than malocclusion or traumatic dental injuries. Eur. J. Paediatr. Dent. 2018, 19, 194–198. [Google Scholar] [PubMed]
- Freire-Maia, F.B.; Auad, S.M.; Abreu, M.H.N.G.D.; Sardenberg, F.; Martins, M.T.; Paiva, S.M.; Pordeus, I.A.; Vale, M.P. Oral Health-Related Quality of Life and Traumatic Dental Injuries in Young Permanent Incisors in Brazilian Schoolchildren: A Multilevel Approach. PLoS ONE 2015, 10, e0135369. [Google Scholar] [CrossRef] [PubMed]
- Sardenberg, F.; Cavalcante-Leão, B.L.; Todero, S.R.B.; Ferreira, F.M.; Rebellato, N.L.B.; Fraiz, F.C. A population-based study on the impact of orofacial dysfunction on oral health-related quality of life among Brazilian schoolchildren. Acta Odontol. Scand. 2017, 75, 173–178. [Google Scholar] [CrossRef]
- Silva-Oliveira, F.; Goursand, D.; Ferreira, R.C.; Paiva, P.C.P.; Paiva, H.N.; Ferreira, E.F.; Zarzar, P.M. Traumatic dental injuries in Brazilian children and oral health-related quality of life. Dent. Traumatol. 2018, 34, 28–35. [Google Scholar] [CrossRef]
- Rajab, L.D.; Abu Al Huda, D. Impact of treated and untreated traumatic dental injuries on oral health-related quality of life among 12-year-old schoolchildren in Amman. Dent. Traumatol. 2019, 35, 153–162. [Google Scholar] [CrossRef]
- Damé-Teixeira, N.; Alves, L.S.; Ardenghi, T.M.; Susin, C.; Maltz, M. Traumatic dental injury with treatment needs negatively affects the quality of life of Brazilian schoolchildren. Int. J. Paediatr. Dent. 2013, 23, 266–273. [Google Scholar] [CrossRef]
- Basavaraj, P.; Sunil, M.K.; Nagarajappa, R.; Ashish, S.; Ramesh, G. Correlation between oral health and Child-OIDP index in 12- and 15-year-old children from Modinagar, India. Asia Pac. J. Public Health 2014, 26, 390–400. [Google Scholar] [CrossRef]
- Bendo, C.B.; Paiva, S.M.; Abreu, M.H.; Figueiredo, L.D.; Vale, M.P. Impact of traumatic dental injuries among adolescents on family’s quality of life: A population-based study. Int. J. Paediatr. Dent. 2014, 24, 387–396. [Google Scholar] [CrossRef]
- Bomfim, R.A.; Herrera, D.R.; De-Carli, A.D. Oral health-related quality of life and risk factors associated with traumatic dental injuries in Brazilian children: A multilevel approach. Dent. Traumatol. 2017, 33, 358–368. [Google Scholar] [CrossRef]
- Bendo, C.B.; Paiva, S.M.; Varni, J.W.; Vale, M.P. Oral health-related quality of life and traumatic dental injuries in Brazilian adolescents. Community Dent. Oral Epidemiol. 2014, 42, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Antunes, L.S.; Debossan, P.F.; Bohrer, L.S.; Abreu, F.V.; Quintanilha, L.E.L.P.; Antunes, L.A.A. Impact of traumatic dental injury on the quality-of-life of children and adolescents: A case-control study. Acta Odontol. Scand. 2013, 71, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Fakhruddin, K.S.; Lawrence, H.P.; Kenny, D.J.; Locker, D. Impact of treated and untreated dental injuries on the quality of life of Ontario school children. Dent. Traumatol. 2008, 24, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Thelen, D.S.; Trovik, T.A.; Bårdsen, A. Impact of traumatic dental injuries with unmet treatment need on daily life among Albanian adolescents: A case-control study. Dent. Traumatol. 2011, 27, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Ilma de Souza Cortes, M.; Marcenes, W.; Sheiham, A. Impact of traumatic injuries to the permanent teeth on the oral health-related quality of life in 12-14-year-old children. Community Dent. Oral Epidemiol. 2002, 30, 193–198. [Google Scholar] [CrossRef]
- Ramos-Jorge, M.L.; Bosco, V.L.; Peres, M.A.; Nunes, A.C.G.P. The impact of treatment of dental trauma on the quality of life of adolescents ? A case-control study in southern Brazil. Dent. Traumatol. 2007, 23, 114–119. [Google Scholar] [CrossRef]
- Antunes, L.A.A.; Luiz, R.R.; Leão, A.T.T.; Maia, L.C. Initial assessment of responsiveness of the P-CPQ (Brazilian Version) to describe the changes in quality of life after treatment for traumatic dental injury. Dent. Traumatol. 2012, 28, 256–262. [Google Scholar] [CrossRef]
- Magno, M.B.; Jural, L.A.; Nogueira, A.D.V.; Lenzi, M.M.; Pithon, M.M.; Maia, L.C. Impact of crown fracture treatment on oral health-related quality of life of children, adolescents, and their families: A prospective clinical study. Int. J. Paediatr. Dent. 2019, 29, 86–93. [Google Scholar] [CrossRef]
- Giannetti, L.; Murri, A.; Vecci, F.; Gatto, R. Dental avulsion: Therapeutic protocols and oral health-related quality of life. Eur. J. Paediatr. Dent. 2007, 2, 69–75. [Google Scholar]
- Berger, T.D.; Kenny, D.J.; Casas, M.J.; Barrett, E.J.; Lawrence, H.P. Effects of severe dentoalveolar trauma on the quality-of-life of children and parents. Dent. Traumatol. 2009, 25, 462–469. [Google Scholar] [CrossRef]
- Porritt, J.M.; Rodd, H.D.; Ruth Baker, S. Quality of life impacts following childhood dento-alveolar trauma. Dent. Traumatol. 2011, 27, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Locker, D. Disparities in oral health-related quality of life in a population of Canadian children. Community Dent. Oral Epidemiol. 2007, 35, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Traebert, J.; de Lacerda, J.T.; Foster Page, L.A.; Thomson, W.M.; Bortoluzzi, M.C. Impact of traumatic dental injuries on the quality of life of schoolchildren. Dent. Traumatol. 2012, 28, 423–428. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General; U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health: Rockville, MD, USA, 2000. Available online: https://www.nidcr.nih.gov/sites/default/files/2017-10/hck1ocv.%40www.surgeon.fullrpt.pdf (accessed on 2 March 2022).
- Sischo, L.; Broder, H.L. Oral health-related quality of life: What, why, how, and future implications. J. Dent. Res. 2011, 90, 1264–1270. [Google Scholar] [CrossRef]
- Kavaliauskienė, A.; Šidlauskas, A.; Zaborskis, A. Modification and psychometric evaluation of the child perceptions questionnaire (CPQ11-14) in assessing oral health related quality of life among Lithuanian children. BMC Oral Health 2019, 19, 1. [Google Scholar] [CrossRef]
- Gherunpong, S.; Tsakos, G.; Sheiham, A. Developing and evaluating an oral health-related quality of life index for children; the CHILD-OIDP. Community Dent. Health 2004, 21, 161–169. [Google Scholar]
- Bernabé, E.; Oliveira, C.M.; Sheiham, A.; Tsakos, G. Comparison of the generic and condition-specific forms of the Oral Impacts on Daily Performances (OIDP) Index. J. Public Health Dent. 2009, 69, 176–181. [Google Scholar] [CrossRef]
- Soriano, E.P.; Caldas, A.D., Jr.; Carvalho, M.V.; Amorim Filho, H.D. Prevalence and risk factors related to traumatic dental injuries in Brazilian schoolchildren. Dent. Traumatol. 2007, 23, 232–240. [Google Scholar] [CrossRef]
- Glendor, U. Epidemiology of traumatic dental injuries—A 12 year review of the literature. Dent. Traumatol. 2008, 24, 603–611. [Google Scholar] [CrossRef]
- De Carvalho Rocha, M.J.; Cardoso, M. Traumatized permanent teeth in Brazilian children assisted at the Federal University of Santa Catarina, Brazil. Dent. Traumatol. 2001, 17, 245–249. [Google Scholar] [CrossRef]
- Leme, M.S.; de Souza Barbosa, T.; Gavião, M.B. Relationship among oral habits, orofacial function and oral health-related quality of life in children. Braz. Oral Res. 2013, 27, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Perez-Sayans, M.; Fernandez-Gonzalez, B.; Somoza-Martin, M.; Gándara-Rey, J.M.; García-García, A. Peri-Implant Bone Resorption around Implants Placed in Alveolar Bone Subjected to Distraction Osteogenesis. J. Oral Maxillofac. Surg. 2008, 66, 787–790. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, T.S.; Tureli, M.C.M.; Gavião, M.B.D. Validity and reliability of the Child Perceptions Questionnaires applied in Brazilian children. BMC Oral Health 2009, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Shaw, W.C. The influence of children’s dentofacial appearance on their social attractiveness as judged by peers and lay adults. Am. J. Orthod. 1981, 79, 399–415. [Google Scholar] [CrossRef]
- Marcenes, W.; Murray, S. Social deprivation and traumatic dental injuries among 14-year-old schoolchildren in Newham, London. Dent. Traumatol. 2001, 17, 17–21. [Google Scholar] [CrossRef]
- Cortes, M.I.S.; Marcenes, W.; Sheiham, A. Prevalence and correlates of traumatic injuries to the permanent teeth of school-children aged 9-14 years in Belo Horizonte, Brazil. Dent. Traumatol. 2001, 17, 22–26. [Google Scholar] [CrossRef]
- Damé-Teixeira, N.; Alves, L.S.; Susin, C.; Maltz, M. Traumatic dental injury among 12-year-old South Brazilian schoolchildren: Prevalence, severity, and risk indicators. Dent. Traumatol. 2013, 29, 52–58. [Google Scholar] [CrossRef]
- Bendo, C.B.; Paiva, S.M.; Oliveira, A.C.; Goursand, D.; Torres, C.S.; Pordeus, I.A. Prevalence and associated factors of traumatic dental injuries in Brazilian schoolchildren. J. Public Health Dent. 2010, 70, 313–318. [Google Scholar] [CrossRef]
- Marques, L.S.; Ramos-Jorge, M.L.; Paiva, S.M.; Pordeus, I.A. Malocclusion: Esthetic impact and quality of life among Brazilian schoolchildren. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 424–427. [Google Scholar] [CrossRef]
- Jokovic, A.; Locker, D.; Guyatt, G. What do children’s global ratings of oral health and well-being measure? Community Dent. Oral Epidemiol. 2005, 33, 205–211. [Google Scholar] [CrossRef]
- Ahrari, F.; Heravi, F.; Rashed, R.; Zarrabi, M.J.; Setayesh, Y. Which Factors Affect Dental Esthetics and Smile Attractiveness in Orthodontically Treated Patients? J. Dent. Tehran Iran 2015, 12, 491. [Google Scholar]
- Flores, M.T.; Onetto, J.E. How does orofacial trauma in children affect the developing dentition? Long-term treatment and associated complications. Dent. Traumatol. 2019, 35, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Gomes, M.C.; Perazzo, M.F.; Neves, É.T.; Martins, C.C.; Paiva, S.M.; Granville-Garcia, A.F. Oral problems and self-confidence in preschool children. Braz. Dent. J. 2017, 28, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Cengiz, O.; Atalar, A.Ç.; Tekin, B.; Bebek, N.; Baykan, B.; Gürses, C. Impact of seizure-related injuries on quality of life. Neurol. Sci. 2019, 40, 577–583. [Google Scholar] [CrossRef]
- Sakaryali, D.; Bani, M.; Cinar, C.; Alacam, A. Evaluation of the impact of early childhood caries, traumatic dental injury, and malocclusion on oral health-Related quality of life for Turkish preschool children and families. Niger. J. Clin. Pract. 2019, 22, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, B.M.; Dias, L.F.; Da Silva Pereira, C.; Filho, M.X.P.; Konrath, A.C.; Da Silva Bolan, M.; Cardoso, M. Impact of dental trauma and esthetic impairment on the quality of life of preschool children. Rev. Paul. Pediatr. 2017, 35, 448–455. [Google Scholar] [CrossRef][Green Version]
- Braimah, R.O.; Ukpong, D.I.; Ndukwe, K.C.; Akinyoola, L. Self-esteem following maxillofacial and orthopedic injuries: Preliminary observations in sub-Saharan Africans. Oral Maxillofac. Surg. 2019, 23, 71–76. [Google Scholar] [CrossRef]
- Ramos-Jorge, M.L.; Ramos-Jorge, J.; Mota-Veloso, I.; Oliva, K.J.; Zarzar, P.M.; Marques, L.S. Parents’ recognition of dental trauma in their children. Dent. Traumatol. 2013, 29, 266–271. [Google Scholar] [CrossRef]
- Ramos-Jorge, J.; Sá-Pinto, A.C.; Almeida Pordeus, I.; Martins Paiva, S.; Castro Martins, C.; Ramos-Jorge, M.L. Effect of dark discolouration and enamel/dentine fracture on the oral health-related quality of life of pre-schoolers. Eur. Arch. Paediatr. Dent. 2017, 18, 83–89. [Google Scholar] [CrossRef]
- Granville-Garcia, A.F.; Gomes, M.C.; Dantas, L.R.; Dantas, L.R.; da Silva, B.R.C.; Perazzo, M.D.F.; Siqueira, M.B.L.D. Parental influence on children’s answers to an oral-health-related quality of life questionnaire. Braz. Oral Res. 2016, 30, 1–8. [Google Scholar] [CrossRef]
- Vieira-Andrade, R.G.; Siqueira, M.B.L.; Gomes, G.B.; D’Avila, S.; Pordeus, I.A.; Paiva, S.M.; Granville-Garcia, A.F. Impact of traumatic dental injury on the quality of life of young children: A case-control study. Int. Dent. J. 2015, 65, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Aldrigui, J.M.; Abanto, J.; Carvalho, T.S.; Mendes, F.M.; Wanderley, M.T.; Bönecker, M.; Raggio, D.P. Impact of traumatic dental injuries and malocclusions on quality of life of young children. Health Qual. Life Outcomes 2011, 9, 78. [Google Scholar] [CrossRef] [PubMed]
- Firmino, R.T.; Gomes, M.C.; Clementino, M.A.; Martins, C.C.; Paiva, S.M.; Granville-Garcia, A.F. Impact of oral health problems on the quality of life of preschool children: A case–control study. Int. J. Paediatr. Dent. 2016, 26, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Barbosa Neves, É.T.; Perazzo, M.F.; Gomes, M.C.; Martins, C.C.; Paiva, S.M.; Granville-Garcia, A.F. Perception of parents and self-reports of children regarding the impact of traumatic dental injury on quality of life. Dent. Traumatol. 2017, 33, 444–450. [Google Scholar] [CrossRef]
- Siqueira, M.B.; Firmino, R.T.; Clementino, M.A.; Martins, C.C.; Granville-Garcia, A.F.; Paiva, S.M. Impact of traumatic dental injury on the quality of life of Brazilian preschool children. Int. J. Environ. Res. Public Health 2013, 10, 6422–6441. [Google Scholar] [CrossRef]
- Viegas, C.M.; Paiva, S.M.; Carvalho, A.C.; Scarpelli, A.C.; Ferreira, F.M.; Pordeus, I.A. Influence of traumatic dental injury on quality of life of Brazilian preschool children and their families. Dent. Traumatol. 2014, 30, 338–347. [Google Scholar] [CrossRef]
- Gomes, M.C.; Pinto-Sarmento, T.C.D.A.; Costa, E.M.M.D.B.; Martins, C.C.; Granville-Garcia, A.F.; Paiva, S.M. Impact of oral health conditions on the quality of life of preschool children and their families: A cross-sectional study. Health Qual. Life Outcomes 2014, 12, 55. [Google Scholar] [CrossRef]
- Abanto, J.; Tello, G.; Bonini, G.C.; Oliveira, L.B.; Murakami, C.; Bönecker, M. Impact of traumatic dental injuries and malocclusions on quality of life of preschool children: A population-based study. Int. J. Paediatr. Dent. 2015, 25, 18–28. [Google Scholar] [CrossRef]
- Abanto, J.; Paiva, S.M.; Raggio, D.P.; Celiberti, P.; Aldrigui, J.M.; Bönecker, M. The impact of dental caries and trauma in children on family quality of life. Community Dent. Oral Epidemiol. 2012, 40, 323–331. [Google Scholar] [CrossRef]
- Abanto, J.; Tsakos, G.; Paiva, S.M.; Carvalho, T.S.; Raggio, D.P.; Bönecker, M. Impact of dental caries and trauma on quality of life among 5- to 6-year-old children: Perceptions of parents and children. Community Dent. Oral Epidemiol. 2014, 42, 385–394. [Google Scholar] [CrossRef]
- Feldens, C.A.; Day, P.; Borges, T.S.; Feldens, E.G.; Kramer, P.F. Enamel fracture in the primary dentition has no impact on children’s quality of life: Implications for clinicians and researchers. Dent. Traumatol. 2016, 32, 103–109. [Google Scholar] [CrossRef]
- Scarpelli, A.C.; Paiva, S.M.; Viegas, C.M.; Carvalho, A.C.; Ferreira, F.M.; Pordeus, I.A. Oral health-related quality of life among Brazilian preschool children. Community Dent. Oral Epidemiol. 2013, 41, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Viegas, C.M.; Scarpelli, A.C.; Carvalho, A.C.; De Morais Ferreira, F.; Pordeus, I.A.; Paiva, S.M. Impact of traumatic dental injury on quality of life among brazilian preschool children and their families. Pediatr. Dent. 2012, 34, 300–306. [Google Scholar] [PubMed]
- Kramer, P.F.; Feldens, C.A.; Helena Ferreira, S.; Bervian, J.; Rodrigues, P.H.; Peres, M.A. Exploring the impact of oral diseases and disorders on quality of life of preschool children. Community Dent. Oral Epidemiol. 2013, 41, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Borges, T.S.; Chaffee, B.W.; Kramer, P.F.; Feldens, E.G.; Vítolo, M.R.; Feldens, C.A. Relationship between overweight/obesity in the first year of age and traumatic dental injuries in early childhood: Findings from a birth cohort study. Dent. Traumatol. 2017, 33, 465–471. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).