Abstract
(1) Background: Globally there is a vast legacy of contaminated sites from past industrial, commercial and military activity, waste disposal, and mineral extraction. This review examined the extent to which the remediation of contaminated sites reduces health risks to new and existing populations. (2) Methods: Standard academic databases were searched for papers that reported on health-related outcomes in humans following remediation and redevelopment of contaminated sites. Title/abstract screening, followed by full-text screening identified sixteen papers that met the eligibility criteria. (3) Results: Most studies were set in the United States of America and reported changes in blood lead concentrations in children, following soil remediation and, in some cases, public health campaigns to reduce exposure. Two further studies examined the impacts of remediation on soil contaminated with chromium and sediments contaminated with polychlorinated biphenyls (PCBs). (4) Conclusions: Overall, the evidence suggests that remediation via removal, capping, and replacing soil, and planting vegetation is effective at reducing concentrations of lead and chromium in blood and urine in children. There is also evidence that sediment dredging can reduce PCB concentrations in umbilical cords in infants. Study designs are relatively weak and some recommendations are provided for those wishing to examine the health impacts of remediation.
1. Introduction
Land can be affected by contamination from current or previous land use, including on site or nearby land uses, such as from chemical, textile, timber, printing and coating industries, generation of energy, management of waste, mining and processing of metals, transport and engineering [1]. These industries may result in contamination of land through disposal of waste materials, accidental spillage or release of pollutants or deposits from air pollution [2,3]. Many countries have introduced regulations to reduce the risk of land becoming contaminated, but activities prior to regulation have left a global legacy of contaminated sites. The European Environment Agency (EEA) estimated that there were 2.8 million potentially contaminated sites across the EU-28 in 2018, and that only approximately 650,000 of these had been formally registered, representing an increase of 76,000 since 2014 [4]. Due to the vast health risks represented by contaminated sites, the World Health Organization (WHO) Regional Office for Europe has started work to assess the health risks of contaminated sites [5]. Based on the available evidence, waste and contaminated sites were established as one of the priority topics for the Sixth Ministerial Conference on Environment and Health (Ostrava, Czechia, June 2017), where member states committed to tackling the environment and health impacts of waste management and contaminated sites [6]. Following this commitment, the WHO Regional Office has developed a planning brief on protecting health through urban redevelopment of contaminated sites to support national and local governments in related efforts [7]. Furthermore, in November 2021, the European Commission adopted a new European Union (EU) soil strategy, aiming at concrete measures to protect and restore soils, and announced the establishment of a new Soil Health Law by 2023 [8].
To prevent environmental threats or health risks from contaminated sites, individual countries have developed legal definitions and risk assessment frameworks for the management of contaminated land [4,9]. Contaminated sites are defined here as: “areas having hosted or being affected by human activities which have produced environmental contamination of soil, sediment, surface or groundwater, air, or food-chain, resulting or being able to result in harm to human health, the environment or ecological systems” (adapted, based on Martuzzi, Pasetto and Martin-Olmedo [10]).
Contaminants include metals (e.g., cadmium, lead), metalloids (e.g., arsenic, antimony), organic substances (e.g., oils, polyaromatic hydrocarbons (PAHs), benzene, toluene, ethylbenzene and xylenes (BTEX), methyl tert-butyl ether (MTBE), polychlorinated biphenyls (PCBs), pesticides, chlorinated solvents, dioxins, volatile and semi-volatile organic compounds (VOCs; S-VOCs), and tars), acids and alkalis, asbestos, gases (e.g., methane), and radioactive substances. The health impacts of contaminants include decreased life expectancy, cognitive impairment and neurological damage, cancers, adverse impacts on respiratory, renal, reproductive and digestive systems, reduced foetal growth and miscarriages, and acute poisoning [1,2,11,12,13,14,15,16]. It is difficult to assess the impacts of contaminated land on human health, due to confounding by individual and area-level factors, such as other sources of pollution (e.g., air pollution), area deprivation, socioeconomic status and behaviours [17]. Furthermore, they usually affect whole local populations making it difficult to identify appropriate control groups.
Land affected by contamination is prioritised for remediation when it is adversely impacting, or is likely to adversely impact, a ‘receptor’. Receptors may include humans, water bodies, crops, property, and specific ecological systems. Contaminated sites do not necessarily pose a risk to receptors, for example, if they are not close by, or the contaminants are sufficiently immobile in the soil [13,16,18]. While contaminated land located in, or close to, urban centres may present a risk to people living nearby, the multiple sources of contamination in such areas often make it difficult to demonstrate an association between a source and a health impact, even if a risk assessment has identified that there is likely to be such an impact [17,19]. Closed sites are also often unattractive, derelict and a waste of land (i.e., brownfields), and their redevelopment can help prevent urban sprawl [20]. It is often due to redevelopment that contaminated sites are remediated [21]. For example, in England and Wales around 90% of sites remediated are through redevelopment [22]. A risk assessment will consider not only the risks presented by the site in its existing state, but also any risks that may occur through redevelopment (e.g., to site workers or new populations moving on to the site), and remediate taking into account newly introduced pathways and receptors. It is important to acknowledge that risk assessment of contaminated sites is often based on whether soil, water and/or indoor air concentrations are above reference values set to protect human or environmental health [9,13,18,19,23]. Where concentrations are found to be above these levels then a remediation strategy is developed [23], or further risk assessment takes place, that may involve additional site investigation, modelling or measurement of health-related outcomes (e.g., biomonitoring). A human health risk assessment (HHRA) often includes an exposure assessment to estimate the relative importance of different pathways to overall exposure [9].
Where a population is identified as being at risk, remediation may be combined with a public health campaign to reduce exposure (e.g., by reducing household dust exposure, or by cessation of vegetable growing) [15], or residents may be advised to relocate [24]. In extreme cases, such as Love Canal, United States of America (USA), the residents may be permanently evacuated, homes demolished and the contamination managed [11]. Remediation technologies can be described as physical (e.g., placing a barrier between a source and a receptor), chemical or biological methods (e.g., removing, degrading or immobilizing the contaminants), for example, using chemical additions to soil [1].
Remediation strategies normally include post-remediation monitoring to ensure that the objectives have been achieved [25], but these are usually focused on environmental media (e.g., soil, water or dust) and do not commonly include monitoring of human health outcomes. Given that most sites are remediated as part of the redevelopment process there is not a ‘before’ population on which to examine pre-remediation health outcomes, although neighbouring populations may be included in monitoring programmes.
Monitoring reports are often held by consultants and not in the public domain [26]. Indeed, several recent reviews have reported that the lack of full-scale remediation studies in the literature is hampering an evaluation of the outcomes of remediation [19,27,28]. Instead, these reviews focused on laboratory experiments or pilot demonstrations on site, which tend to dominate the literature due to the focus on development of new remediation technologies. Those publications that examine outcomes related to human health tend to cover the pre-remediation risk assessment and/or rely on data modelling exposure pathways or risk (e.g., [2,3,20,23]). However, there is a need to examine the evidence related to full-scale remediation and redevelopment of contaminated sites and their efficacy in terms of reducing harm to human health.
The aim of this systematic review is, therefore, to provide a robust assessment of the evidence for the effectiveness of remediation and redevelopment of contaminated sites in reducing environmental and health risks. It focuses on the redevelopment of contaminated sites to new residential neighbourhoods and public or recreational functions. Due to the small number of studies that evaluate post-redevelopment outcomes with specific reference to the remediation of contamination, the scope includes the remediation of contaminated sites to reduce or prevent health and environmental risks in existing urban areas in close proximity to the site. The review sought to answer the question: to what extent does remediation, and any subsequent redevelopment, of contaminated sites reduce environmental and health risks to new and existing populations and ecological systems, and are there any effects on equity in terms of the distribution of risks and outcomes?
2. Methods
This systematic review focuses on contaminated sites of any kind. The study followed a systematic search strategy, followed by title and abstract screening, full-text screening, data extraction and quality appraisal, following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines [29]. Since the review was carried out in a short space of time, it was not possible to develop and register a review protocol in advance, as suggested by guidelines for systematic reviews [30].
2.1. Search Strategy
The search strategy (Table 1) combined three sets of terms relating to the remediation and development of contaminated sites, based on De Sario et al. [31]. The first set of terms focussed on the contaminants (e.g., lead, polyaromatic hydrocarbons) and the land uses leading to contamination (e.g., mining, industrial). The second set of terms corresponded to remediation and redevelopment of these sites. The third described health-related outcomes (e.g., mortality, cancer). Title, abstract and keyword searches were carried out in Ovid (Embase, Medline, Global Health, PsycINFO, Cab Abstracts), Scopus, Open Grey, and ProQuest (theses database, ASSIA) on 4th June 2020. We used Scopus instead of Web of Science due to institutional subscription, because it is more international and interdisciplinary, both of which are important for our review, has better coverage of biomedical research [32] and includes health sciences [33]. We chose to include Open Grey as we expected that some evaluations relevant to our review might not have been published.

Table 1.
Terms in the search strategy.
2.2. Eligibility Criteria
A total of 6903 papers were selected for title and abstract screening based on the following inclusion criteria: the site was known to have soil contamination as a result of a land use or disposal of waste on or adjacent to the site, or deposition of pollution from nearby land uses AND remediation of some or all of the site (by any means) had taken place AND there was an evaluation of health-related outcomes for new or existing populations following remediation and/or redevelopment.
Studies. were excluded if: they reported on exposure from general sources (e.g., vehicular traffic) OR they only reported changes following laboratory or field experiments, rather than full scale remediation OR they reported on the outcomes of modelling and/or risk assessments where risk to humans was estimated either before or after remediation had taken place OR they focussed on post-development outcomes relating to regeneration (e.g., employment, inward investment, deprivation), rather than those associated with the remediation of contamination.
2.3. Data Extraction
Screening was carried out by DS, and a 15% sample was screened by a second reviewer (IB). Few papers met the inclusion criteria following title/abstract screening (n = 50; 14 included new development, 36 considered existing populations). Following title/abstract screening each paper was full-text screened by DS against the above criteria. Reference lists were also searched for additional studies (see flow diagram in Figure 1).
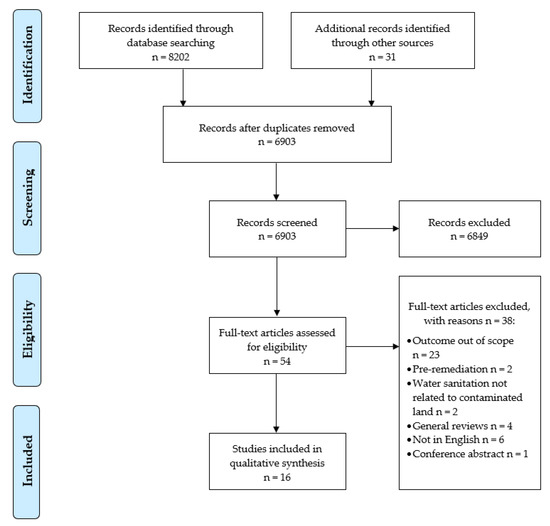
Figure 1.
PRISMA flow diagram [25].
Sixteen papers were included in the systematic review. Data were extracted from each paper using a standard proforma: Contaminant(s) of interest and source(s) of contamination; Remediation technique(s); Objective(s); Location; Study design and comparator; Sample size and population(s); Considerations of equity; Timing of sampling; Approach, methods, design; Outcome(s); Results (including confidence interval and p-values); Limitations/risks/bias. Data extraction was carried out independently by DS and IB and evidence synthesis was carried out by DS.
2.4. Quality Appraisal
Quality assessment was carried out using the Effective Public Healthcare Panacea Project’s Quality Assessment Tool for Quantitative Studies [34]). This tool assesses the quality of studies against a series of criteria, including study design, risk of bias, recruitment and withdrawal of participants (a detailed method can be found in the link above). Quality assessment was done independently by IB and DS and there was strong agreement between the assessments (94% for overall scores and 82% for individual components). Disagreement between scores related only to the representativeness of the sample study design (where not stated explicitly). All studies were judged as ‘weak’ using this tool (see Appendix A) and therefore studies were not excluded based on quality.
The studies fell into three categories, used to structure the results of the review:
Studies that examine health-related outcomes for new residents following remediation and redevelopment of contaminated land, all of which focussed on lead (n = 3) [35,36,37];
Studies that examine health-related outcomes for children in existing neighbourhoods resulting from exposure to lead (n = 8) [38,39,40,41,42,43,44,45] and chromium (n = 1) [46] following remediation and public health campaigns;
Studies that examine health-related outcomes in existing populations following remediation of contaminated land (n = 4) [47,48,49,50].
3. Results
3.1. Study Characteristics
Sixteen studies were included in the evidence synthesis (Table 2). The majority were based in the USA (n = 9). The remaining studies came from Australia (n = 1), Canada (n = 2), Nigeria (n = 1), Chile (n = 1), Italy (n = 1) and Finland (n = 1). Most of the studies (n = 12) reported on remediation of sites contaminated with lead originating from smelters in Finland [35], the USA [38,39,40,47], and Canada [41], from a lead reclamation plant in Canada [42], from informal gold mining in Nigeria [43], a copper mine in the USA [36], a lead mine in Australia [44] and from several sources in the USA [37,45]. Another study reported on the remediation of chromium waste sites [46] and another on the dredging of a harbour to reduce exposure to polychlorinated biphenyls (PCBs) [48], both in the USA. The remaining studies reported on sites contaminated with multiple metals. One reported on blood lead levels (BLLs) from a waste disposal site in Chile [49] and the other on cadmium, chromium, copper, manganese, lead and zinc from mining and industrial sources in Sardinia, Italy [50].
Table 2.
Studies meeting eligibility criteria included in the systematic review.
Most studies were cross-sectional (n = 8) [35,36,39,43,46,47,49,50]. Others included a randomised control trial (n = 1) [45], cohort study (n = 2) [37,48], pre-post-remediation (n = 1) [42], case-control (n = 1) [38] and interrupted time series (n = 3) [40,41,44].
The majority (n = 15) studied children living near sources of contamination, reflecting the vulnerability of this group to exposure from soils due to hand-to-mouth behaviours and the toxicity of contaminants such as lead [51]. One study examined BLLs in adults [50].
Most studies (n = 14) reported the results of human biomonitoring (HBM) of contaminants in blood [35,36,37,38,39,40,41,42,43,44,45,47,49,50]. Two studies reported concentrations in urine [46,49] and one in umbilical cord serum [48]. Concentrations were compared with a control group, post-remediation concentrations, or thresholds set to protect health (e.g., a BLL of 5 µg/dL) [35,37,38,39,40,41,42,43,44,45,46,47,49,50]. Some studies used the proportion of children exceeding these concentrations as a population-level outcome to assess the impact of remediation [36,37,39,40,42,47]. Remediation usually aimed to reduce soil concentrations to an acceptable level, but in one study this was reported as an additional outcome [43]. Household dust is an important exposure pathway from contaminated soil to humans, and two studies reported concentrations in household and/or day care centre dust as an outcome [35,47]. One study examined the impact of contaminant exposure and subsequent remediation on cognitive performance in children born pre- and post-remediation of a waste disposal site [49].
The evidence synthesis is based on the broad categories outlined above. The studies varied in the level of detail provided on the remediation and/or redevelopment of the sites and this information is included in the evidence tables where available.
3.2. Remediation Followed by Redevelopment
Three studies examined BLLs in children following remediation and redevelopment. The focus of these studies was the impact of the remediation, so the description of the redevelopment is less detailed (Table 3). All three studies report declining BLLs following remediation [35,36,37]. In adults, lead can damage several organs and is associated with hypertension, diabetes and heart disease, but it is the impact on children that is most commonly cause for concern-it is associated with reduced cognitive performance and increased behavioural problems [37].
Table 3.
Studies reporting health-related outcomes for people living near remediated sites following remediation and redevelopment.
Remediation generally involved the removal and replacement of surface soils although the criteria used to decide which soils should be remediated and the reasons for doing so varied between the studies. Although they all include redevelopment in some form, the focus of these studies is BLLs in existing populations.
The objectives of the studies also differ. The study in Finland examined the different exposure routes from remaining contaminated soils to ascertain whether children living in the area were at risk and to inform further remediation [35]. The study in New Orleans investigated persistent disparities in BLLs to identify areas where remediation was still required post-Katrina [37]. The study in Butte assessed changes in BLLs following a remediation programme [36].
The study in Finland [35] collected primary data on BLLs for the study. Conversely the two USA studies used data from existing population screening programmes [36,37].
Although these three studies report on changes in BLLs following redevelopment as well as remediation, their findings are primarily concerned with the impact on existing populations living on, or near to, contaminated land. They provide consistent evidence that soil remediation can lower BLLs of children living near contaminated sites. However, except for the study in Butte [36], the reporting of these studies makes it difficult to directly relate remediation to the changes in BLLs.
3.3. Existing Populations with Remediation and Public Health Intervention
There are nine studies that examine the impacts of remediation on existing populations without considering redevelopment of the site. In these situations, remediation is often carried out alongside a public health campaign with the aim of reducing exposure via household dust, which has a high proportion of soil, and reducing hand-to-mouth behaviours in young children.
These studies also tend to focus on lead contamination (Table 4). There is one study on chromium contamination in the USA [46], and five that consider lead exposure in the USA [45], Canada [41,42], Australia [44] and Nigeria [43]. The remaining three studies relate to lead contamination at the same site, Bunker Hill Superfund Site in Idaho, USA. These present the initial period of remediation [38], a detailed analysis of the impact of the different interventions [40], and a review of the remediation and its impact on BLLs [39].
Table 4.
Studies reporting health-related outcomes for people living near contaminated sites after remediation and public health campaigns.
In all nine studies the contamination came from a combination of waste disposal and industrial deposition. Again, the remediation methods mainly involved removal and capping of contaminated soil. The purpose of the studies was to evaluate the effectiveness of the remediation and public health campaigns, with some studies also assessing the impact of exposure pathways on levels of lead in blood, or chromium in urine, of local children [38,46].
Most of the studies presented here analysed BLLs collected as part of a screening programme. There are, however, two exceptions. The cross-sectional study in New Jersey measured chromium in household dusts and urine of 41 children from Lafayette Gardens (a public housing project surrounded on three sides by chromium disposal sites), and 23 children, matched by age and sex, from three comparator neighbourhoods, which included a public housing project and a more affluent neighbourhood [46]. The other exception was the study in Boston [45], which consisted of a randomised trial with three groups (groups 2 and 3 were later combined): those receiving soil remediation, home cleaning and interior loose-paint stabilisation (group 1; n = 54), those with only home cleaning and paint stabilisation (group 2; n = 51) and those receiving paint stabilisation (group 3; n = 47) [45].
Taken together, these studies provide consistent evidence that remediation of contaminated soils is effective at reducing both direct and indirect exposure to pollution in adjacent populations. The studies from Bunker Hill suggest that remediation of yards alone is not sufficient (the resuspension of soils from other locations leads to recontamination and inward migration means that new families moving into unremediated homes are at risk [39,40]). In addition, contaminated areas accessible by children lead to another direct exposure pathway [43,46]. One study in Bunker Hill [40] suggested that area-wide remediation was responsible for around three times more reduction in BLLs than individual yard remediation. These studies also demonstrate that, where populations are exposed to contamination and remediation programmes, public health campaigns are also effective at reducing exposure pathways. These campaigns provide information about the risks from contamination and the importance of cleaning dusts from homes, good personal hygiene, and discouraging hand-to-mouth behaviour and pica (eating dirt) in children [39,43]. Most of the studies do not report separately about the impact of public health campaigns, but the reduction in hand-to-mouth behaviour and pica [42], and the estimated effectiveness of the intervention [40], suggests that this can be an important strategy to reduce exposure while remediation is carried out.
3.4. Existing Population with Remediation Only
The remaining studies assessed the impact of remediation of contaminated soils on the health of existing populations. These studies reported on remediation only; there was no public health campaign reported, although this may have taken place (Table 5).
Table 5.
Studies reporting health-related outcomes for people living near contaminated sites after remediation.
These studies relate to sites contaminated by waste disposal [48,49], mining and deposition of industrial metal pollution [47,50] and consider a mixture of inorganic pollutants [47,49,50] and polychlorinated biphenyls (PCBs) [48].
The remediation technologies described in these studies were heterogeneous. The abandoned waste disposal site in Arica, Chile was active between 1984 and 1999. During remediation the wastes were removed, the site capped and fenced off and the roofs of homes in the vicinity were cleaned [49]. In Midvale, Utah mine tailings were capped, and a remediation programme removed soil from yards where lead concentrations exceeded 500 mg/kg, replacing it with clean soil [47]. The PCBs in New Bedford Harbour Superfund Site, MA, USA were caused by industrial waste disposal, including a capacitor, between the 1940s and 1977; the remediation of this site involved dredging and removing contaminated sediments between 1994 and 1995 [48]. The study in the Sulcis-Iglesiente area of Sardinia, Italy focuses on metals from an active industrial area, including three mines restored in the 1990 s, two lead/zinc mines and one coal mine [50]. There is no detail on the exact remediation measures employed at these sites.
These studies suggest that remediation of soil contamination alone can result in reduced exposure and contribute to improvements in health outcomes. The studies in Midvale and Arica give more information on the remediation methods employed and report consistent decreases in the BLLs or improved cognitive performance [47,49]. The study in New Bedford Harbour suggests that, although dredging of contaminated sediments can be successful in helping to reduce PCB exposure, the volatility of these contaminants means that there may be an increase in exposure during remediation, which should be considered in the planning of remediation strategies [48].
4. Discussion
This systematic review found consistent evidence that remediation of contaminated soils is effective at reducing direct and indirect exposure to pollution in local populations. The evidence for health outcomes is weighted towards studies of lead contamination, although some studies consider chromium and PCB contamination. The studies from Bunker Hill [39,40] suggest that soil cover alone is not sufficient (there needs to be excavation of contaminated surface soils to prevent upward migration) and that area-wide remediation is required to prevent recontamination. The experiences at Bunker Hill also suggest that this is particularly important where existing populations are present and mobile, as families may move into contaminated homes, and that ongoing monitoring is essential so that further requirements for remediation activities can be addressed during the programme [34,35]. The Bunker Hill studies also demonstrate the importance of considering the sustainability of remediation, especially with climate change, as remediated material was exposed following extreme weather events [39,40].
Although it appears that soil remediation is largely responsible for the decline in soil, dust and blood concentrations of contaminants, there is also good evidence that public health campaigns are effective at reducing exposure pathways for existing populations [39,40,42]. Several studies have highlighted the importance of multiple public agencies collaborating in site investigation and remediation, and the development of public health campaigns [33,42,52]. The importance of communication with residents was also highlighted in terms of gaining their trust and maximising participation [39,53]. Data collection, remediation and public health campaigns should be sensitive to their needs and experiences [18,52].
Due to the nature of research on remediation methods for contaminated sites, very few studies in the academic literature report on outcomes related to human health following full scale remediation. Searches of grey literature (i.e., OpenGrey and theses database) did not result in any additional studies. It does not follow that these technologies are unreliable, only that the monitoring and evaluation programmes to date have not often been reported on in the academic literature [26]. Our literature search found many studies reporting on laboratory, modelling or pilot studies, rather than full-scale remediation, and the lack of long-term evaluations following full-scale remediation is highlighted as a weakness in the literature in previous reviews focused on the efficacy of remediation for environmental outcomes [19,27,28]. In some countries, detailed remediation strategies, with well-defined success criteria and long-term monitoring programmes, require regulatory approval prior to the commencement of remediation, which is often not easily accessible.
4.1. Strengths and Limitations
Although the studies reported here generally find that HBM of contaminants decline following remediation, only one study reported on a clinical outcome [49]. HBM is an effective method to assess exposure, as it is relatively simple to measure concentrations of contaminants, (e.g., of metals in blood or urine), and it may be able to detect elevated concentrations before the development of clinical outcomes [54]. Frameworks and threshold concentrations for soil, water and blood concentrations vary by country, which hampers comparison between studies. In this review, most of the studies were based in the USA and focused on lead contamination.
The studies included are concerned, in the main, with lead pollution, often from a single source. There is a lack of heterogeneity, both in terms of the contaminants and the remediation employed. This could be because of the complexities associated with measuring organic contaminants in biological matrices, along with their prevalence in the environment from multiple sources. There is a notable gap in the evidence in relation to the mental health impacts of site remediation and redevelopment.
There is a lack of longer-term follow-ups from the remediation programmes reported in these studies. Given that recontamination of soils was reported after a relatively short time period [39] and previous studies have found an upward migration of metals 30 years after restoration [18], it is important for screening programmes to continue and report on longer term outcomes. Similarly, there is a lack of long-term trials on full-scale remediation in the published literature. Few studies examined health-related outcomes following both remediation and redevelopment. This is likely to be due to several factors; for example, the evaluation of full-scale remediation is not common, and the timescales involved between remediation and redevelopment and the different stakeholders involved make a long-term study extremely challenging. There are methodological challenges associated with health assessments; populations are often not present pre-remediation, or are also exposed to various contaminants in the urban environment reducing the ability to assess the impacts of a particular site, and finding an appropriate control group is challenging. This may explain the preponderance of studies in the USA and Australia where population densities are lower and urban areas are more likely to have grown around one industry (making the pathway between site and population simpler to study). Additionally, it is not generally desirable to remind a new population of the contamination history of their site [17], especially if remediation objectives have been met and there do not appear to be ongoing health impacts.
Few of the studies explicitly considered equity in their study design or outcomes. It is well documented in environmental justice literature that disadvantaged groups are more likely to live near contaminated sites [54]. Some studies did collect data on socioeconomic variables and include these as confounders in their analysis [36,38,45,47,48,49,50], others collected these variables but did not include them in the analysis [43] or simply discussed their findings in relation to socioeconomic status [37,39,40,46]. Only one study appeared to consider equity at the design stage, including control groups from neighbourhoods with both similar and more affluent socioeconomic profiles [46]. Often, the populations located near contaminated sites tend to be more disadvantaged. This is important because socioeconomic factors are likely to affect the exposure to soils either directly (e.g., length of residence, diet) or indirectly (e.g., income), or they may be related to the outcome (e.g., maternal education, income in the study examining cognitive performance).
All the studies examining health-related outcomes were scored as ‘weak’ in the quality assessment. For certain criteria, this was due to the nature of these studies. For example, few studies were blinded, but this is because it is difficult to blind participants to the existence of contaminated sites, which tends to be well-known in a neighbourhood. Similarly, the outcome assessor is likely to know whether participants live close to a contaminated site, especially if household dust samples or door to door surveys are being carried out. This could be avoided by asking participants to attend a test centre or clinic, although this may reduce participation. Such criteria are of less importance for the studies in this review as they tend to use objectively-measured outcomes (e.g., BLLs) that are unlikely to be affected by the participant being aware of the research questions or the assessor knowing the exposure status of the participant. Where blinding becomes more important is when data are collected on behaviours related to exposure such as outdoor play, hygiene and hand-to-mouth activity, or lifestyle factors (e.g., diet, smoking). For example, in the study of chromium concentrations in children’s urine, playing on the waste sites was not reported by the children, even though it had been observed by the researchers. The authors suggest this may be because the parents were present during the survey [46]. The earlier study at Bunker Hill reported possible problems with recall of activities over a 9-month period. Parents of children with higher BLLs may be more likely to remember behaviours related to higher levels of exposure [38].
For other criteria, where papers scored poorly, this could have been avoided through better reporting of the study design. For example, it was usually not possible to tell how representative participants were of the target population, or the participation rate of those invited to take part. Studies that report analysis of data from population screening programmes (e.g., [37,40,43,48]) are more likely to be representative of the population but several studies did not report this information. Studies could also have provided more information about sample demographics; for example, the age range of the children in the study from New Orleans is not clear [37]. Participation in most of the studies was voluntary and several studies acknowledge selection bias as a limitation [38,39,40,45]. In Bunker Hill and Quebec, some parents did not want their children to be tested as they had low BLLs in previous years [39,42], meaning that the bias is likely to be towards those with higher BLLs [40]. One study from Bunker Hill highlights a practical and ethical consideration with many of these studies; the screening and remediation efforts target those most at risk of adverse health effects by design [40]. This bias in sampling is justified on ethical grounds [39], particularly where the need to treat a population overrides other considerations, as in the case of lead poisoning resulting from gold mining in Nigeria [43]. It was reported that if screening of BLLs at the Bunker Hill Superfund Site was characterised as an academic study, this had a negative effect on participation rates [40].
The number and reasons for participants dropping out of studies was not consistently reported. Another criterium where better reporting could have improved the quality ratings was related to the data collection methods, where it was not clear whether data collection methods were valid and/or reliable. Some studies, however, did report this information; for example, the precise methods of blood sampling and analysis with reference to standard protocols, or the use of standard tools (e.g., for cognitive performance).
Several studies collected data on confounders, but they did not always take them into account in the analysis or justify why some confounders were included in the analysis and others were not. Again, this could have improved the reporting of the study. In the case of behavioural factors this is particularly important, as it means that the effects of the public health programme cannot be separated out from those of the remediation. However, the later studies at Bunker Hill did assess the independent impact of remediation and public health campaigns [40].
Shortcomings in the design of studies of contaminated sites are difficult to address. There are not often resources available to provide a control group or randomised sample, and this would divert funds from assessing outcomes in at risk populations or taking remediation action [40]. Consequently, most of the studies considered here were cross-sectional. Some studies analysed outcomes before and after remediation [37,42,48], and were scored as ‘moderate’ on this criterium in the quality assessment. The analysis of the Bunker Hill Superfund site included a case-control study [38], and another study used samples from participants screened in multiple years to analyze an interrupted time series [40,41,44]. Most studies had relatively large sample sizes, but in a few cases the sample size affects the usefulness of the study [35,50]. Although the study in Boston was a randomised controlled trial [45], the analysis compared groups based on treatments received, rather than randomised groups (i.e., not ‘intention-to-treat’), thereby losing the benefits of randomisation.
Finally, the focus of several studies included in the review was on health-related outcomes, and therefore there was a lack of detailed information about remediation activities, thus restricting our ability to assess the effectiveness of specific remediation strategies.
4.2. Policy Implications and Future Research
Contaminated sites have raised considerable concern in many countries worldwide and affect local urban planning as well as global sustainability policies.
The large volume of industrial activities in such sites, associated with waste production, increased use of hazardous materials, as well as residual contamination in derelict military sites result in severe challenges for future use of potentially contaminated sites [55]. This is especially important for growing cities which have a continuous demand for land and cannot afford to leave abandoned sites (often referred to as brownfields) unused and undeveloped. Within the EU, land recycling and urban densification (such as converting industrial sites into urban functions and related infrastructure) accounted for only 13% of new developments and associated land take, identifying the increasing demand for land as a viable challenge for future sustainable development [56]. Therefore, redeveloping contaminated sites for urban functions is necessary for land recycling in many European countries. Reflecting this urgency, the remediation and redevelopment of contaminated sites has already been the focus of several activities and multilateral projects lead by the European Commission.
On a global scale, the problem of soil contamination is reflected in the Sustainable Development Agenda, which considers sustainable consumption and production patterns in the Sustainable Development Goal (SDG) 12. To feed the world sustainably, producers need to grow more food which requires healthy soils, unaffected by negative environmental impacts and degradation. The Agenda covers, among others, hazardous waste and chemicals, as well as extraction of natural resources [57]. Soil-related aspects are also covered (for example in relation to land degradation, ecosystem services or soil resources) in various other SDGs. Promoting sustainable production and management of resources including soil is also the objective of the circular economy concept, which aims to mitigate waste and pollution by keeping material resources in use and supporting natural material regeneration. Changing from a linear economy (take, make, dispose) to a circular economy (renew, remake, share) is therefore expected to support the attainment of SDG 12 [58]. The EU Green Deal, aiming to achieve a climate-neutral economy by 2050, thus includes the circular economy concept [59] and provides the policy context for the new EU soil strategy [8].
Interventions to redevelop contaminated sites therefore have both local and global policy relevance, and contribute directly and indirectly to social, environmental and health objectives. Research on the practical implementation, as well as the formulation, of adequate policy frameworks on the remediation and redevelopment of contaminated sites will be essential to support public authorities effectively tackle the local challenges that are posed by these sites.
This review highlights a real lack of long-term evaluations examining the impact of full-scale remediation in the academic literature. However, these studies do take place, often as a condition of remediation permits, and there is a need for the results to be published in the public domain, to enable a sharing of best practice. Where studies do exist, they tend to relate only to the impact of remediation on existing populations and/or do not include the redevelopment of the site. There are challenges in conducting this type of study, due to the timescales involved between remediation and redevelopment and the different actors involved at each stage in the process, as well as methodological challenges, including the lack of a pre-remediation ‘before’ population. However, if feasible, using administrative data (e.g., health and social outcomes, environmental data) could offer the opportunity to examine the impacts of contaminated site remediation and redevelopment, particularly where the impact of the site covers a large area, or where neighbourhood regeneration is concerned. Making use of secondary data, where available, may be more achievable than new studies. In addition, regeneration projects have previously been evaluated using natural experimental study designs (e.g., [60]) and this approach could also be taken to examine the impact of contaminated site redevelopment on health outcomes.
5. Conclusions
This systematic review examined the extent to which the remediation of contaminated land reduces health risks to new and existing populations. The papers included in the evidence synthesis suggest that there is good evidence that remediation via removal, capping, and replacing soil, and planting of bare soils, can reduce concentrations of lead and chromium in blood and urine in children. There is more limited evidence (from one study), that remediation of soils can improve cognitive performance in children living near waste dumps. There is also some evidence (also from one study), that sediment dredging can reduce PCB concentrations in umbilical cords in infants. However, the removal of soil is not a sustainable option for dealing with contaminated land and the preference now is to use technologies that reduce the environmental sequelae of remediation. Many other studies (not included in this review) examine the health outcomes associated with contaminated sites before remediation, and an opportunity exists to follow up some of these sites after remediation, with greatest priority being given to those that examine organic contaminants or inorganic contaminants other than lead. Similarly, results from long-term epidemiological or surveillance studies should be published whenever possible, to add to the existing evidence base.
Author Contributions
Conceptualization, D.S., I.B., G.B., M.B. and S.N.; methodology, D.S., I.B., G.B. and M.B.; investigation, D.S., and I.B.; resources, M.B. and S.N.; data curation, D.S. and I.B.; writing—original draft preparation, D.S., I.B. and M.B.; writing—review and editing, D.S., I.B., G.B., M.B. and S.N.; supervision, M.B.; project administration, D.S.; funding acquisition, M.B. and S.N. All authors have read and agreed to the published version of the manuscript.
Funding
For the project on redevelopment of contaminated sites, the WHO Regional Office for Europe acknowledges financial support by the German Federal Ministry for the Environment, Nature Conservation and Nuclear Safety.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Acknowledgments
We would like to thank Pauline Shaw for her assistance with the search strategy and the attendees of the expert workshop on the redevelopment of contaminated sites for their useful feedback. The findings of this review have contributed to a WHO technical report on the urban redevelopment of contaminated sites, published by the WHO Regional Office for Europe (2021).
Conflicts of Interest
The authors declare no conflict of interest. This review was funded by WHO Regional Office for Europe, M.B. and S.N. contributed to the design of the review, writing the manuscript, and decision to publish the results, but not to the collection, analyses or interpretation of the data. The authors affiliated with the World Health Organization (WHO) are alone responsible for the views expressed in this publication and they do not necessarily represent the decisions or policies of the WHO.
Appendix A
Table A1.
Results of the quality assessment.
Table A1.
Results of the quality assessment.
| Criteria | Scores | ||
|---|---|---|---|
| (A) SELECTION BIAS (Q1) Are the individuals selected to participate in the study likely to be representative of the target population? | Very likely = 11 Somewhat likely = 2 Can’t tell = 3 | ||
| (Q2) What percentage of selected individuals agreed to participate? | 80 to 100% = 4 60 to 79% = 3 Less than 60% = 3 Can’t tell = 6 | ||
| (B) STUDY DESIGN | Randomised control trial = 1 Cohort analytic = 2 Cohort (one group pre + post) = 1 Case control = 1 Interrupted time series = 3 Cross-sectional = 8 | ||
| (C) CONFOUNDERS (Q1) Were there important differences between groups prior to the intervention? | Yes = 10 No = 0 Can’t tell = 6 | ||
| (Q2) If yes, indicate the percentage of relevant confounders that were controlled (either in the design (e.g. stratification, matching) or analysis)? | 80 to 100% = 7 60 to 79% = 1 Less than 60% = 2 | ||
| (D) BLINDING (Q1) Was (were) the outcome assessor(s) aware of the intervention or exposure status of participants? | Yes = 4 No = 1 Can’t tell = 11 | ||
| (Q2) Were the study participants aware of the research question? | Yes = 3 No = 1 Can’t tell = 12 | ||
| (E) DATA COLLECTION METHODS (Q1) Were data collection tools shown to be valid? | Yes = 7 No = 1 Can’t tell = 8 | ||
| (Q2) Were data collection tools shown to be reliable? | Yes = 3 No = 1 Can’t tell = 12 | ||
| (F) WITHDRAWALS AND DROP-OUTS (Q1) Were withdrawals and drop-outs reported in terms of numbers and/or reasons per group? | Yes = 2 No = 2 N/A = 12 | ||
| (Q2) Indicate the percentage of participants completing the study. (If the percentage differs by groups, record the lowest). | 80 to 100% = 1 60 to 79% = 2 Less than 60% = 1 N/A = 12 | ||
| Strong | Moderate | Weak | |
| (A) SELECTION BIAS | 4 | 6 | 6 |
| (B) STUDY DESIGN | 1 | 7 | 8 |
| (C) CONFOUNDERS | 7 | 1 | 8 |
| (D) BLINDING | 1 | 0 | 15 |
| (E) DATA COLLECTION METHODS | 3 | 4 | 9 |
| (F) WITHDRAWALS AND DROP-OUTS (N/A = 12) | 1 | 1 | 2 |
| GLOBAL RATING | 0 | 0 | 16 |
References
- Souza, L.R.R.; Pomarolli, L.C.; da Veiga, M.A.M.S. From classic methodologies to application of nanomaterials for soil remediation: An integrated view of methods for decontamination of toxic metal(oid)s. Environ. Sci. Pollut. Res. 2020, 27, 10205–10227. [Google Scholar] [CrossRef] [PubMed]
- Coelho, P.C.D.S.; García-Lestón, J.; Silva, S.P.; da Costa, C.S.; da Costa, S.C.; Coelho, M.I.; Lage, B.L.; Mendez, E.P.; Teixeira, J.P. Geno- and immunotoxic effects on populations living near a mine: A case study of panasqueira mine in Portugal. J. Toxicol. Environ. Health Part A 2011, 74, 1076–1086. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Yan, X.; Zhong, L.; Tong, X. Benzene homologues contaminants in a former herbicide factory site: Distribution, attenuation, risk, and remediation implication. Environ. Geochem. Health 2020, 42, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Payá Pérez, A.; Rodriguez Eugenio, N. Status of local soil contamination in Europe. In Revision of the Indicator “Progress in the Management Contaminated Sites in Europe”, EUR 29124 EN; Publications Office of the European Union: Luxembourg, 2018. [Google Scholar]
- WHO Regional Office for Europe. Human Health in Areas with Industrial Contamination; WHO Regional Office for Europe: Copenhagen, Denmark, 2014. [Google Scholar]
- WHO Regional Office for Europe. Declaration of Sixth Ministerial Conference on Environmental and Health; WHO Regional Office for Europe: Copenhagen, Denmark, 2017; Available online: https://apps.who.int/iris/handle/10665/347444 (accessed on 26 November 2021).
- WHO Regional Office for Europe. Protecting Health through Urban Redevelopment of Contaminated Sites; A Planning Brief. WHO Regional Office for Europe: Copenhagen, Denmark, 2021; Available online: https://apps.who.int/iris/handle/10665/349922 (accessed on 26 November 2021).
- European Commission. EU Soil Policy; European Commission: Brussels, Belgium, 2021; Available online: https://ec.europa.eu/environment/soil/soil_policy_en.htm (accessed on 26 November 2021).
- Martin-Olmedo, P.; Ranzi, A.; Santoro, M.; Dack, S.; de Hoogh, K.; Martuzzi, M.; Dogliotti, E.; Hoek, G.; Tomasova, J.; Dimovska, M.; et al. Methods and data needs to assess health impacts of chemicals in industrial contaminated sites. Epidemiol. Prev. 2019, 43, 223–237. [Google Scholar] [PubMed]
- Martuzzi, M.; Pasetto, R.; Martin-Olmedo, P. Industrially contaminated sites and health. J. Environ. Pub. Health 2014, 2014, 198574. [Google Scholar] [CrossRef] [PubMed]
- Engelhaupt, E. Happy birthday, Love Canal. Environ. Sci. Technol. 2008, 42, 8179–8186. [Google Scholar] [CrossRef] [PubMed]
- Green, D.; Sullivan, M.; Cooper, N.; Dean, A.; Marquez, C. A pilot study of children’s blood lead levels in Mount Isa, Queensland. Int. J. Environ. Res. Public Health 2017, 14, 1567. [Google Scholar] [CrossRef]
- Kalsi, A.; Celin, S.M.; Bhanot, P.; Sahai, S.; Sharma, J.G. Microbial remediation approaches for explosive contaminated soil: Critical assessment of available technologies, recent innovations and Future prospects. Environ. Technol. Innov. 2020, 18, 100721. [Google Scholar] [CrossRef]
- Kiaghadi, A.; Rifai, H.S.; Dawson, C.N. The presence of Superfund sites as a determinant of life expectancy in the United States. Nat. Commun. 2021, 12, 1947. [Google Scholar] [CrossRef]
- Prasad, L.R.; Nazareth, B. Contamination of allotment soil with lead: Managing potential risks to health. J. Public Health Med. 2020, 22, 525–530. [Google Scholar] [CrossRef][Green Version]
- Reisinger, H.J.; Burris, D.R.; Hering, J.G. Remediating subsurface arsenic contamination with monitored natural attenuation. Environ. Sci. Technol. 2005, 39, 458A–464A. [Google Scholar] [CrossRef] [PubMed]
- Farmer, J.G.; Jarvis, R. Strategies for improving human health in contaminated situations: A review of past, present and possible future approaches. Environ. Geochem. Health 2009, 31, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Ros, J.M.; Garcia, G.; Penas, J.M. Assessment of restoration success of former metal mining areas after 30 years in a highly polluted Mediterranean mining area: Cartagena-La union. Ecol. Eng. 2013, 57, 393–402. [Google Scholar] [CrossRef]
- Eckley, C.S.; Gilmour, C.C.; Janssen, S.; Luxton, T.P.; Randall, P.M.; Whalin, L.; Austin, C. The assessment and remediation of mercury contaminated sites: A review of current approaches. Sci. Total Environ. 2020, 707, 136031. [Google Scholar] [CrossRef]
- Wcisło, E.; Bronder, J.; Bubak, A.; Rodríguez-Valdés, E.; Gallego, J.L.R. Human health risk assessment in restoring safe and productive use of abandoned contaminated sites. Environ. Int. 2016, 94, 436–448. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, S.M.; Pereira, M.E.; da Silva, E.F.; Hursthouse, A.S.; Duarte, A.C. A review of regulatory decisions for environmental protection: Part I—Challenges in the implementation of national soil policies. Environ. Int. 2009, 35, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Environment Agency. Dealing with Contaminated Land in England and Wales; Environment Agency: Bristol, UK, 2009. [Google Scholar]
- Wcisło, E.; Ioven, D.; Kucharski, R.; Szdzuj, J. Human health risk assessment case study: An abandoned metal smelter site in Poland. Chemosphere 2002, 47, 507–515. [Google Scholar] [CrossRef]
- Yaffee, A.Q.; Scott, B.; Kaelin, C.; Cambron, J.; Sanderson, W.; Christian, W.J.; Moran, T.P.; Chamness, J. Collaborative response to arsenic-contaminated soil in an Appalachian Kentucky neighborhood. J. Toxicol. Environ. Health Part A 2019, 82, 697–701. [Google Scholar] [CrossRef]
- Gore, D.B.; Preston, N.J.; Fryirs, K.A. Post-rehabilitation environmental hazard of Cu, Zn, As and Pb at the derelict Conrad Mine, eastern Australia. Environ. Pollut 2007, 148, 491–500. [Google Scholar] [CrossRef]
- Jain, P.; Townsend, T.G.; Johnson, P. Case study of landfill reclamation at a Florida landfill site. Waste Manag. 2013, 33, 109–116. [Google Scholar] [CrossRef]
- Gong, Y.; Zhao, D.; Wang, W. An overview of field-scale studies on remediation of soil contaminated with heavy metals and metalloids: Technical progress over the last decade. Water Res. 2018, 147, 440–460. [Google Scholar] [CrossRef] [PubMed]
- Jing, R.; Fusi, S.; Kjellerup, B.V. Remediation of Polychlorinated Biphenyls (PCBs) in contaminated soils and sediment: State of knowledge and perspectives. Front. Environ. Sci. 2018, 6, 79. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 105906. [Google Scholar] [CrossRef]
- De Sario, M.; Pasetto, R.; Vecchi, S.; Zeka, A.; Hoek, G.; Michelozzi, P.; Iavarone, I.; Fletcher, T.; Bauleo, L.; Ancona, C. A scoping review of the epidemiological methods used to investigate the health effects of industrially contaminated sites. Epidemiol. Prev. 2018, 42, 59–68. [Google Scholar] [PubMed]
- Tabacaru, S. Web of Science versus Scopus: Journal Coverage Overlap Analysis. Texas A&M University Libraries. 2019. Available online: https//hdl.handle.net/1969.1/175137 (accessed on 21 April 2022).
- Falagas, M.E.; Pitsouni, E.I.; Malietzis, G.A.; Pappas, G. Comparison of PubMed, Scopus, Web of Science, and Google Scholar: Strengths and weaknesses. FASEB J. 2008, 22, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Effective Public Healthcare Panacea Project. Quality Assessment Tool for Quantitative Studies. 2022. Available online: https://www.ephpp.ca/quality-assessment-tool-for-quantitative-studies/ (accessed on 25 April 2022).
- Louekari, K.; Mroueh, U.M.; Maidell-Münster, L.; Valkonen, S.; Tuomi, T.; Savolainen, K. Reducing the risks of children living near the site of a former lead smeltery. Sci. Total Environ. 2004, 319, 65–75. [Google Scholar] [CrossRef]
- Schoof, R.A.; Johnson, D.L.; Handziuk, E.R.; Landingham, C.V.; Feldpausch, A.M.; Gallagher, A.E.; Dell, L.D.; Kephart, A. Assessment of blood lead level declines in an area of historical mining with a holistic remediation and abatement program. Environ. Res. 2016, 150, 582–591. [Google Scholar] [CrossRef]
- Mielke, H.W.; Gonzales, C.R.; Powell, E.T.; Mielke, P.W. Environmental and health disparities in residential communities of New Orleans: The need for soil lead intervention to advance primary prevention. Environ. Int. 2013, 51, 73–81. [Google Scholar] [CrossRef]
- Maisonet, M.; Bove, F.J.; Kaye, W.E. A case-control study to determine risk factors for elevated blood lead levels in children, Idaho. Toxicol. Ind. Health 1997, 13, 67–72. [Google Scholar] [CrossRef]
- Sheldrake, S.; Stifelman, M. A case study of lead contamination cleanup effectiveness at Bunker Hill. Sci. Total Environ. 2003, 303, 105–123. [Google Scholar] [CrossRef]
- Von Lindern, I.; Spalinger, S.; Petroysan, V.; von Braun, M. Assessing remedial effectiveness through the blood lead:soil/dust lead relationship at the Bunker Hill Superfund Site in the Silver Valley of Idaho. Sci. Total Environ. 2003, 303, 139–170. [Google Scholar] [CrossRef]
- Hilts, S.R.; Bock, S.E.; Oke, T.L.; Yates, C.L.; Copes, R.A. Effect of interventions on children’s blood lead levels. Environ. Health Persp. 1998, 106, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Goulet, L.; Messier, A.; Gaudreau, J. Results of a lead decontamination program. Arch. Environ. Health 1996, 51, 68–72. [Google Scholar] [CrossRef]
- Tirima, S.; Bartrem, C.; von Lindern, I.; von Braun, M.; Lind, D.; Anka, S.M.; Abdullahi, A. Environmental remediation to address childhood lead poisoning epidemic due to artisanal gold mining in Zamfara, Nigeria. Environ. Health Persp. 2016, 124, 1471–1478. [Google Scholar] [CrossRef]
- Boreland, F.; Lesjak, M.S.; Lyle, D.M. Managing environmental lead in Broken Hill: A public health success. New South Wales Public Health Bull. 2008, 19, 174–179. [Google Scholar] [CrossRef]
- Aschengrau, A.; Beiser, A.; Bellinger, D.; Copenhafer, D.; Weitzman, M. Residential lead-based-paint hazard remediation and soil lead abatement: Their impact among children with mildly elevated blood lead levels. Am. J. Public Health 1997, 87, 1698–1702. [Google Scholar] [CrossRef]
- Freeman, N.C.G.; Wainman, T.; Lioy, P.J.; Stern, A.H.; Shupack, S.I. The effect of remediation of chromium waste sites on chromium levels in urine of children living in the surrounding neighborhood. J. Air Waste Manag. Assoc. 1995, 45, 604–614. [Google Scholar] [CrossRef]
- Lanphear, B.P.; Succop, P.; Roda, S.; Henningsen, G. The effect of soil abatement on blood lead levels in children living near a former smelting and milling operation. Public Health Rep. 2003, 118, 83–91. [Google Scholar] [CrossRef]
- Choi, A.L.; Levy, J.I.; Dockery, D.W.; Ryan, L.M.; Tolbert, P.E.; Altshul, L.M.; Korrick, S.A. Does living near a Superfund site contribute to higher polychlorinated biphenyl (PCB) exposure? Environ. Health Persp. 2006, 114, 1092–1098. [Google Scholar] [CrossRef]
- Burgos, S.; Tenorio, M.; Zapata, P.; Cáceres, D.D.; Klarian, J.; Alvarez, N.; Oviedo, R.; Toro-Campos, R.; Claudio, L.; Iglesias, V. Cognitive performance among cohorts of children exposed to a waste disposal site containing heavy metals in Chile. Int. J. Environ. Health Res. 2017, 27, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Madeddu, R.; Tolu, P.; Asara, Y.; Farace, C.; Forte, G.; Bocca, B. Blood biomonitoring of metals in subjects living near abandoned mining and active industrial areas. Environ. Monit. Assess. 2013, 185, 5837–5846. [Google Scholar] [CrossRef] [PubMed]
- Mielke, H.W.; Covington, T.P.; Mielke, P.W., Jr.; Wolman, F.J.; Powell, E.T.; Gonzales, C.R. Soil intervention as a strategy for lead exposure prevention: The New Orleans lead-safe childcare playground project. Environ. Pollut. 2011, 159, 2071–2077. [Google Scholar] [CrossRef] [PubMed]
- Greene, N.A.; White, J.D.; Morris, V.R.; Roberts, S.; Jones, K.L.; Warrick, C. Evidence for environmental contamination in residential neighborhoods surrounding the defense depot of Memphis, Tennessee. Int. J. Environ. Res. Public Health 2006, 3, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Pasetto, R.; Mattioli, B.; Marsili, D. Environmental justice in industrially contaminated sites. A review of scientific evidence in the WHO European Region. Int. J. Environ. Res. Public Health 2019, 16, 998. [Google Scholar] [CrossRef] [PubMed]
- Colles, A.; Ardeleanu, E.R.; Candeias, C.; Ranzi, A.; Demeter, Z.; Hofer, A.; Kowalska, M.; Makris, K.C.; Arrebola, J.P.; Schoeters, G.; et al. Human biomonitoring as a tool for exposure assessment in industrially contaminated sites (ICSs). Lessons learned within the ICS and Health European Network. Epidemiol. E Prev. 2019, 43, 249–259. [Google Scholar]
- Panagos, P.; Van Liedekerke, M.; Yigini, Y.; Montanarella, L. Contaminated sites in Europe: Review of the current situation based on data collected through a European network. J. Environ. Public Health 2013, 2013, 158764. [Google Scholar] [CrossRef]
- European Environment Agency. Land and Soil in Europe: Why We Need to Use These Vital and Finite Resources Sustainably; European Environment Agency: Copenhagen, Denmark, 2019; Available online: https://www.eea.europa.eu/signals/signals-2019-content-list/articles/land-and-soil-towards-the (accessed on 26 November 2021).
- United Nations. Sustainable Development Goals—Goal 12: Sustainable Consumption and Production Patterns; United Nations: New York, NY, USA, 2020; Available online: https://www.un.org/sustainabledevelopment/sustainable-consumption-production (accessed on 26 November 2021).
- WHO Regional Office for Europe. Circular Economy and Health: Opportunities and Risks; WHO Regional Office for Europe: Copenhagen, Denmark, 2018; Available online: https://apps.who.int/iris/handle/10665/342218 (accessed on 26 November 2021).
- European Commission. A European Green Deal. European Commission: Brussels, Belgium, 2020. Available online: europa.eu (accessed on 26 November 2021).
- Cummins, S.; Clark, C.; Lewis, D.; Smith, N.; Thompson, C.; Smuk, M.; Stansfeld, S.; Taylor, S.; Fahy, A.; Greenhalgh, T.; et al. The effects of the London 2012 Olympics and related urban regeneration on physical and mental health: The ORiEL mixed-methods evaluation of a natural experiment. Public Health Res. 2018, 6, 1–248. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).