
Exploring Musculoskeletal Complaints in a Needle Manufacturing Industry: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Sociodemographic Characteristics
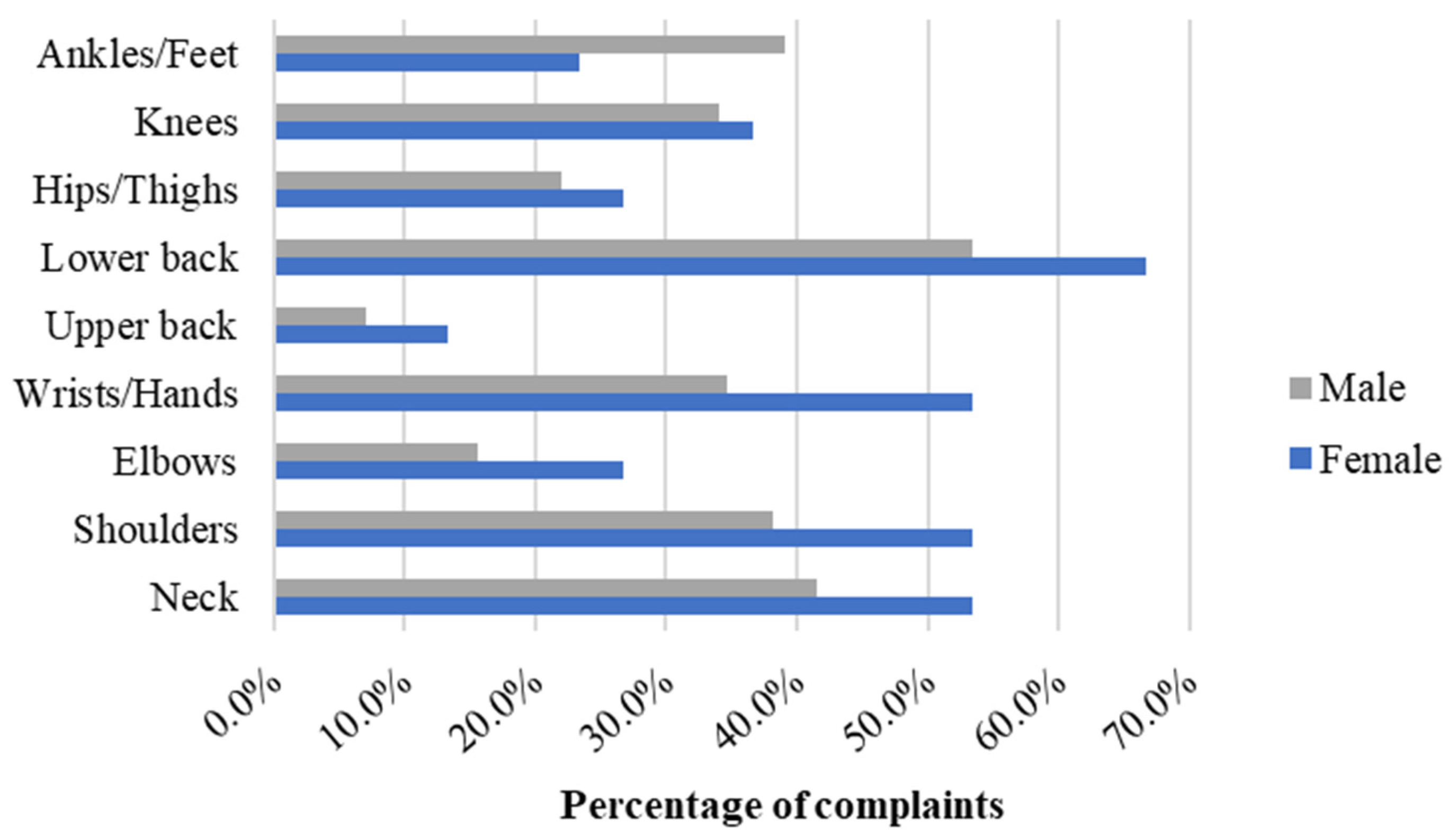
3.2. Gender-Related Complaints
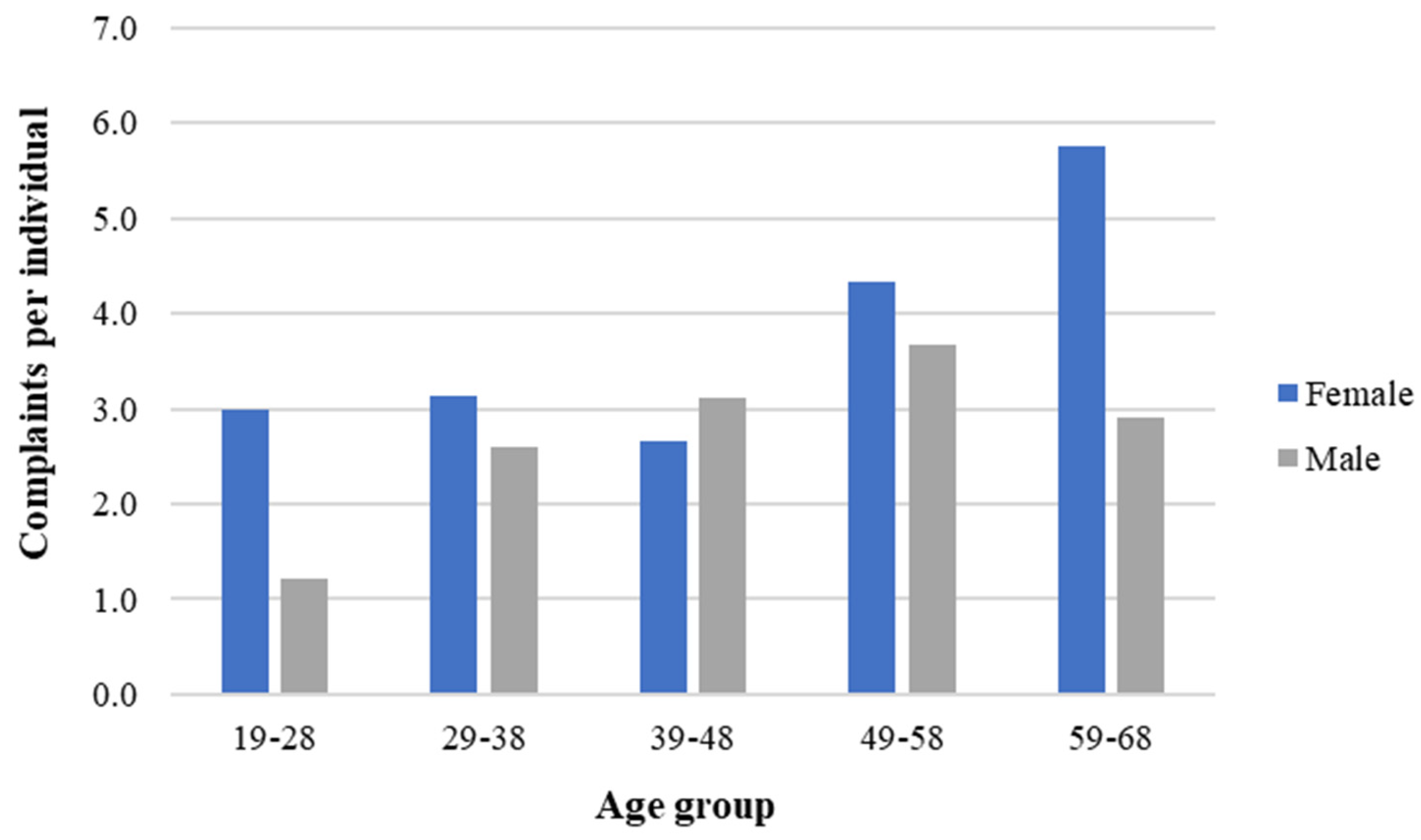
3.3. Age-Related Complaints
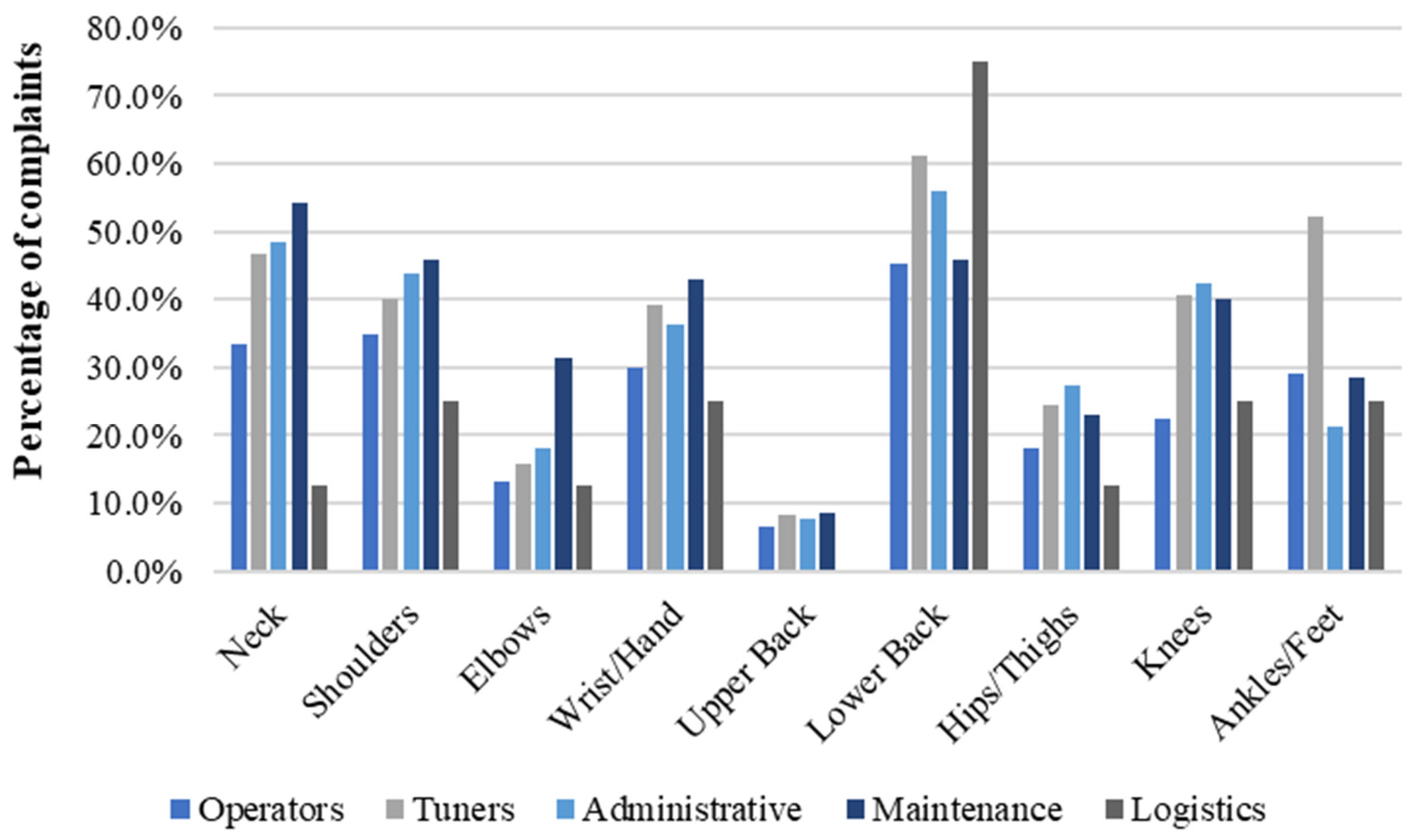
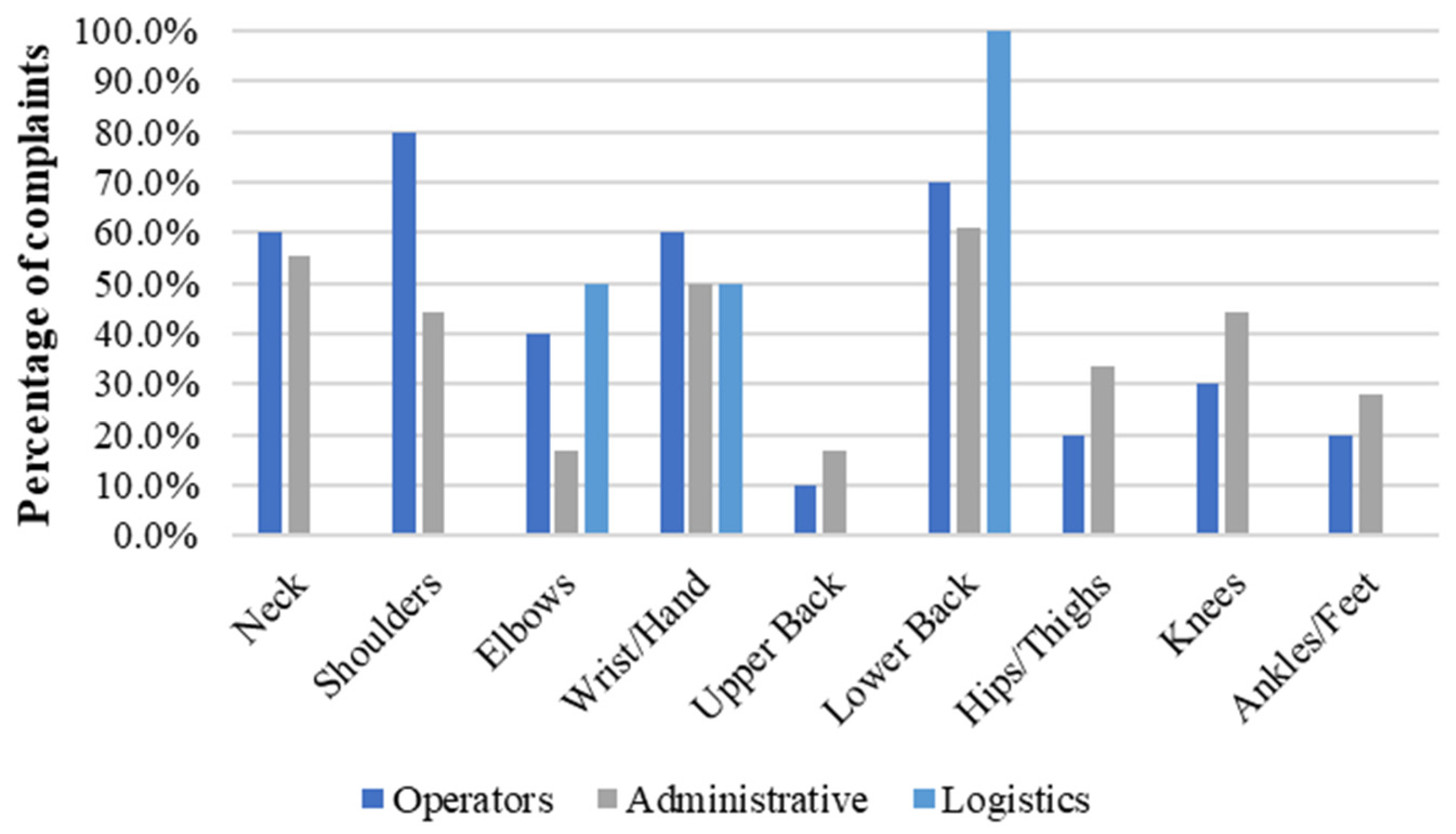
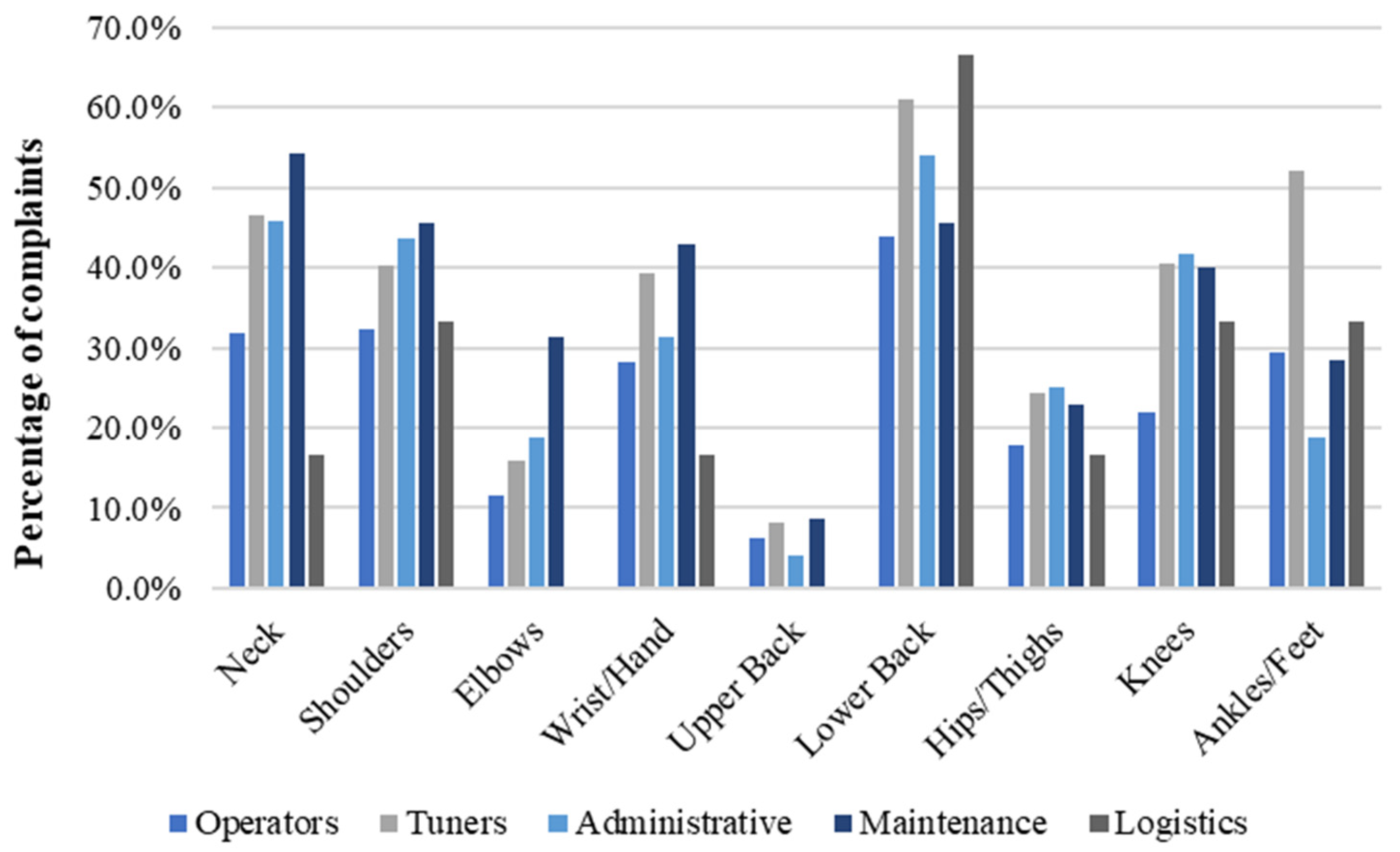
3.4. Occupation-Related Complaints
3.5. BMI
4. Discussion
4.1. National Representativeness
4.2. Associations between Gender, Age, Job, and Body Part Complaints
4.2.1. Gender vs Body Part Complaints
4.2.2. Age vs. Body Complaints
4.2.3. Occupation vs. Body Complaints
4.2.4. BMI vs. Body Complaints
4.3. Implications of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Woolf, A.D.; Vos, T.; March, L. How to Measure the Impact of Musculoskeletal Conditions. Best Pract. Res. Clin. Rheumatol. 2010, 24, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Linaker, C.H.; Walker-Bone, K. Shoulder Disorders and Occupation. Best Pract. Res. Clin. Rheumatol. 2015, 29, 405–423. [Google Scholar] [CrossRef]
- Crawford, J.O.; Berkovic, D.; Erwin, J.; Copsey, S.M.; Davis, A.; Giagloglou, E.; Yazdani, A.; Hartvigsen, J.; Graveling, R.; Woolf, A. Musculoskeletal Health in the Workplace. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101558. [Google Scholar] [CrossRef] [PubMed]
- Palmer, K.T.; Bovenzi, M. Rheumatic Effects of Vibration at Work. Best Pract. Res. Clin. Rheumatol. 2015, 29, 424–439. [Google Scholar] [CrossRef] [PubMed]
- Piedrah, H.; Punnett, L.; Shahnavaz, H. Musculoskeletal Symptoms in Cold Exposed and Non-Cold Exposed Workers. Int. J. Ind. Ergon. 2004, 34, 271–278. [Google Scholar] [CrossRef]
- Amiri, S.; Behnezhad, S. Is Job Strain a Risk Factor for Musculoskeletal Pain? A Systematic Review and Meta-Analysis of 21 Longitudinal Studies. Public Health 2020, 181, 158–167. [Google Scholar] [CrossRef]
- Golubovich, J.; Chang, C.H.; Eatough, E.M. Safety Climate, Hardiness, and Musculoskeletal Complaints: A Mediated Moderation Model. Appl. Ergon. 2014, 45, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Chen, S.G.; Tang, S.C.; Wang, S.; He, L.H.; Guo, Z.H.; Li, J.Y.; Yu, S.F.; Wang, Z.X. How Work Organization Affects the Prevalence of WMSDs: Biomed. Environ. Sci. 2015, 28, 627–633. [Google Scholar] [CrossRef]
- Govindu, N.K.; Babski-Reeves, K. Effects of Personal, Psychosocial and Occupational Factors on Low Back Pain Severity in Workers. Int. J. Ind. Ergon. 2014, 44, 335–341. [Google Scholar] [CrossRef]
- Schaafsma, F.G.; Anema, J.R.; Van Der Beek, A.J. Back Pain: Prevention and Management in the Workplace. Best Pract. Res. Clin. Rheumatol. 2015, 29, 483–494. [Google Scholar] [CrossRef]
- Maimaiti, N.; Wang, J.; Jin, X.; Wang, S.; Qin, D.; He, L.; Wang, F.; Zhang, Z.; Forsman, M.; Yang, L.; et al. Cervical Musculoskeletal Disorders and Their Relationships with Personal and Work-Related Factors among Electronic Assembly Workers. J. Safety Res. 2019, 71, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.; Williams, A.E.; Nester, C. Musculoskeletal Disorders, Foot Health and Footwear Choice in Occupations Involving Prolonged Standing. Int. J. Ind. Ergon. 2021, 81, 103079. [Google Scholar] [CrossRef]
- Harris, E.C.; Coggon, D. HIP Osteoarthritis and Work. Best Pract. Res. Clin. Rheumatol. 2015, 29, 462–482. [Google Scholar] [CrossRef] [PubMed]
- Dulay, G.S.; Cooper, C.; Dennison, E.M. Knee Pain, Knee Injury, Knee Osteoarthritis & Work. Best Pract. Res. Clin. Rheumatol. 2015, 29, 454–461. [Google Scholar] [CrossRef]
- Newington, L.; Harris, E.C.; Walker-Bone, K. Carpal Tunnel Syndrome and Work. Best Pract. Res. Clin. Rheumatol. 2015, 29, 440–453. [Google Scholar] [CrossRef] [PubMed]
- Widanarko, B.; Legg, S.; Stevenson, M.; Devereux, J.; Eng, A.; Cheng, S.; Douwes, J.; Ellison-loschmann, L.; Mclean, D.; Pearce, N. Prevalence of Musculoskeletal Symptoms in Relation to Gender, Age, and Occupational/Industrial Group. Int. J. Ind. Ergon. 2011, 41, 561–572. [Google Scholar] [CrossRef]
- Vargas-Prada, S.; Coggon, D. Psychological and Psychosocial Determinants of Musculoskeletal Pain and Associated Disability. Best Pract. Res. Clin. Rheumatol. 2015, 29, 374–390. [Google Scholar] [CrossRef] [PubMed]
- Gomes, L.; Bispo, M.; Ferreira, C.; De, G.H.; Silva, O.; Lennick, N.; Albuquerque, B.D.; Magno, J. Risk Factors for Work-Related Musculoskeletal Disorders: A Study in the Inner Regions of Alagoas and Bahia. Saf. Sci. 2022, 153, 105804. [Google Scholar] [CrossRef]
- de Souza, D.S.F.; da Silva, J.M.N.; Santos, J.V.d.O.; Alcântara, M.S.B.; Torres, M.G.L. Influence of Risk Factors Associated with Musculoskeletal Disorders on an Inner Population of Northeastern Brazil. Int. J. Ind. Ergon. 2021, 86, 103198. [Google Scholar] [CrossRef]
- Wang, T.; Zhao, Y.L.; Hao, L.X.; Jia, J.G. Prevalence of Musculoskeletal Symptoms among Industrial Employees in a Modern Industrial Region in Beijing, China. Chin. Med. J. 2019, 132, 789–797. [Google Scholar] [CrossRef]
- Lu, J.; Twu, L.; Wang, M.J. Risk Assessments of Work-Related Musculoskeletal Disorders among the TFT-LCD Manufacturing Operators. Int. J. Ind. Ergon. 2016, 52, 40–51. [Google Scholar] [CrossRef]
- Chu, P.C.; Wang, T.G.; Guo, Y.L. Work-Related and Personal Factors in Shoulder Disorders among Electronics Workers: Findings from an Electronics Enterprise in Taiwan. BMC Public Health 2021, 21, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Di, N.; Guo, W.w.; bin Ding, W.; Jia, N.; Zhang, H.; Li, D.; Wang, D.; Wang, R.; Zhang, D.; et al. The Prevalence and Risk Factors of Work Related Musculoskeletal Disorders among Electronics Manufacturing Workers: A Cross-Sectional Analytical Study in China. BMC Public Health 2023, 23, 10. [Google Scholar] [CrossRef] [PubMed]
- Hembecker, P.K.; Reis, D.C.; Konrath, A.C.; Gontijo, L.A.; Eugenio, E.A. Investigation of Musculoskeletal Symptoms in a Manufacturing Company in Brazil: A Cross-Sectional Study. Braz. J. Phys. Ther. 2017, 21, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Mgbemena, C.E.; Tiwari, A.; Xu, Y.; Prabhu, V.; Hutabarat, W. Ergonomic Evaluation on the Manufacturing Shop Floor: A Review of Hardware and Software Technologies. CIRP J. Manuf. Sci. Technol. 2020, 30, 68–78. [Google Scholar] [CrossRef]
- Palmer, K.T.; Goodson, N. Ageing, Musculoskeletal Health and Work. Best Pract. Res. Clin. Rheumatol. 2015, 29, 391–404. [Google Scholar] [CrossRef]
- Zare, M.; Bodin, J.; Cercier, E.; Brunet, R.; Roquelaure, Y. Evaluation of Ergonomic Approach and Musculoskeletal Disorders in Two Different Organizations in a Truck Assembly Plant. Int. J. Ind. Ergon. 2015, 50, 34–42. [Google Scholar] [CrossRef]
- Bevan, S. Economic Impact of Musculoskeletal Disorders (MSDs) on Work in Europe. Best Pract. Res. Clin. Rheumatol. 2015, 29, 356–373. [Google Scholar] [CrossRef]
- De Kok, J.; Vroonhof, P.; Snijders, J.; Roullis, G.; Clarke, M.; Peereboom, K.; van Dorst, P.; Isusi, I. Work-Related Musculoskeletal Disorders: Prevalence, Costs and Demographics in the EU; European Agencyfor Safety and Healthat Work: Bilbao, Spain, 2019; ISBN 9789294791450. [Google Scholar]
- Bhattacharya, A. Costs of Occupational Musculoskeletal Disorders (MSDs) in the United States. Int. J. Ind. Ergon. 2014, 44, 448–454. [Google Scholar] [CrossRef]
- Vandekerckhove, S.; Lenaerts, K.; Szekér, L.; Desiere, S.; Lamberts, M.; Ramioul, M. Musculoskeletal Disorders and Psychosocial Risk Factors in The Workplace—Statistical Analysis of EU-Wide Survey Data; European Agencyfor Safety and Healthat Work: Bilbao, Spain, 2021; ISBN 9789294795953. [Google Scholar]
- Perista, H.; Carrilho, P. Portugal: Musculoskeletal Disorders Identified as Main Risk Factor in Companies. Available online: https://www.eurofound.europa.eu/en/resources/article/2018/portugal-musculoskeletal-disorders-identified-main-risk-factor-companies (accessed on 3 May 2024).
- Hales, T.R.; Bernard, B.P. Epidemiology of Work-Related Musculoskeletal Disorders. Orthop. Clin. North Am. 1996, 27, 679–709. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. PLoS Med. 2007, 4, 1628–1654. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, C.C.; Ribeiro, J.C.; Moreira, P. Portuguese Version of the Standardized Nordic Musculoskeletal Questionnaire: Cross Cultural and Reliability. J. Public Heal. 2010, 18, 6. [Google Scholar] [CrossRef]
- Biadgo, G.H.; Tsegay, G.S.; Mohammednur, S.A.; Gebremeskel, B.F. Burden of Neck Pain and Associated Factors Among Sewing Machine Operators of Garment Factories in Mekelle City, Northern Part of Ethiopia, 2018, A Cross-Sectional Study. Saf. Health Work 2021, 12, 51–56. [Google Scholar] [CrossRef]
- Howell, D.C. Statistical Methods for Psychology. In Psychology; Wadsworth, Ed.; University of Vermont: Burlington, VT, USA; Belmont, CA, USA, 2013; p. 796. ISBN 9781111835484. [Google Scholar]
- Field, A. Discovery Statistics Using SPSS, 3rd ed.; Sage Publications Ltd.: London, UK, 2009; Volume 112, ISBN 9781847879066. [Google Scholar]
- IBM Cramér’s V. Available online: https://www.ibm.com/docs/en/cognos-analytics/11.1.0?topic=terms-cramrs-v (accessed on 26 May 2024).
- INE Total Jobs By Industry. Available online: https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_cnacionais2010b2016&perfil=392022253&INST=391941652&contexto=am (accessed on 3 May 2024).
- Israel, G.D. Determining Sample Size; University of Florida Cooperative Extension Service, Institute of Food and Agriculture Sciences, EDIS: Tampa, FL, USA, 1992; Volume 10, pp. 3–5. [Google Scholar]
- WHO BMI Classification. Available online: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations (accessed on 3 May 2024).
- PORDATA População Empregada: Total e Por Sexo. Available online: https://www.pordata.pt/municipios/populacao+empregada+total+e+por+sexo-812 (accessed on 13 May 2024).
- Pattani, R.; Marquez, C.; Dinyarian, C.; Sharma, M.; Bain, J.; Moore, J.E.; Straus, S.E. The Perceived Organizational Impact of the Gender Gap across a Canadian Department of Medicine and Proposed Strategies to Combat It: A Qualitative Study. BMC Med. 2018, 16, 48. [Google Scholar] [CrossRef] [PubMed]
- ILOSTAT Where Women Work: Female-Dominated Occupations and Sectors. Available online: https://ilostat.ilo.org/blog/where-women-work-female-dominated-occupations-and-sectors/#:~:text=Asidefromdominatingeconomicactivities,continuetobemale-dominated (accessed on 3 May 2024).
- Petrongolo, B.; Ronchi, M. Gender Gaps and the Structure of Local Labor Markets. Labour Econ. 2020, 64, 101819. [Google Scholar] [CrossRef]
- PORDATA População Empregada: Total e Por Grupo Etário. Available online: https://www.pordata.pt/db/municipios/ambiente+de+consulta/tabela (accessed on 13 May 2024).
- Burgess, R.A.; Thompson, R.T.; Rollman, G.B. The Effect of Forearm Posture on Wrist Flexion in Computer Workers with Chronic Upper Extremity Musculoskeletal Disorders. BMC Musculoskelet. Disord. 2008, 9, 7. [Google Scholar] [CrossRef]
- Manchikanti, L.; Singh, V.; Datta, S.; Cohen, S.P.; Hirsch, J.A. Comprehensive Review of Epidemiology, Scope, and Impact of Spinal Pain. Pain Physician 2009, 12, 35–70. [Google Scholar] [CrossRef] [PubMed]
- Hogg-Johnson, S.; van der Velde, G.; Carroll, L.J.; Holm, L.W.; Cassidy, J.D.; Guzman, J.; Côté, P.; Haldeman, S.; Ammendolia, C.; Carragee, E.; et al. The Burden and Determinants of Neck Pain in the General Population. Spine 2008, 33, S39–S51. [Google Scholar] [CrossRef]
- Hoy, D.G.; Protani, M.; De, R.; Buchbinder, R. The Epidemiology of Neck Pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 783–792. [Google Scholar] [CrossRef]
- Leboeuf-Yde, C.; Nielsen, J.; Kyvik, K.O.; Fejer, R.; Hartvigsen, J. Pain in the Lumbar, Thoracic or Cervical Regions: Do Age and Gender Matter? A Population-Based Study of 34,902 Danish Twins 20–71 Years of Age. BMC Musculoskelet. Disord. 2009, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- Shiri, R.; Falah-Hassani, K.; Heliövaara, M.; Solovieva, S.; Amiri, S.; Lallukka, T.; Burdorf, A.; Husgafvel-Pursiainen, K.; Viikari-Juntura, E. Risk Factors for Low Back Pain: A Population-Based Longitudinal Study. Arthritis Care Res. 2019, 71, 290–299. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, M. Foot and Ankle Disorders. An. Orthop. Guid. Today’s GP 2017, 17, 101–121. [Google Scholar] [CrossRef]
- Miranda, H.; Punnett, L.; Viikari-Juntura, E.; Heliövaara, M.; Knekt, P. Physical Work and Chronic Shoulder Disorder. Results of a Prospective Population-Based Study. Ann. Rheum. Dis. 2008, 67, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Okabe, T.; Suzuki, M.; Goto, H.; Iso, N.; Cho, K.; Hirata, K.; Shimizu, J. Sex Differences in Age-Related Physical Changes among Community-Dwelling Adults. J. Clin. Med. 2021, 10, 4800. [Google Scholar] [CrossRef] [PubMed]
- Shur, N.F.; Creedon, L.; Skirrow, S.; Atherton, P.J.; MacDonald, I.A.; Lund, J.; Greenhaff, P.L. Age-Related Changes in Muscle Architecture and Metabolism in Humans: The Likely Contribution of Physical Inactivity to Age-Related Functional Decline. Ageing Res. Rev. 2021, 68, 101344. [Google Scholar] [CrossRef] [PubMed]
- Sansone, V.; Bonora, C.; Boria, P.; Meroni, R. Women Performing Repetitive Work: Is There a Difference in the Prevalence of Shoulder Pain and Pathology in Supermarket Cashiers Compared to the General Female Population? Int. J. Occup. Med. Environ. Health 2014, 27, 722–735. [Google Scholar] [CrossRef] [PubMed]
- Helliwell, P.S. The Elbow, Forearm, Wrist, and Hand. Ther. Exerc. Mov. Towar. Funct. 1999, 13, 687–730. [Google Scholar] [CrossRef] [PubMed]
- Dzakpasu, F.Q.S.; Carver, A.; Brakenridge, C.J.; Cicuttini, F.; Urquhart, D.M.; Owen, N.; Dunstan, D.W. Musculoskeletal Pain and Sedentary Behaviour in Occupational and Non-Occupational Settings: A Systematic Review with Meta-Analysis. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 56. [Google Scholar] [CrossRef]
- Carroll, L.J.; Hogg-Johnson, S.; van der Velde, G.; Haldeman, S.; Holm, L.W.; Carragee, E.J.; Hurwitz, E.L.; Côté, P.; Nordin, M.; Peloso, P.M.; et al. Course and Prognostic Factors for Neck Pain in the General Population. Spine 2008, 33, S75–S82. [Google Scholar] [CrossRef]
- Bontrup, C.; Taylor, W.R.; Fliesser, M.; Visscher, R.; Green, T.; Wippert, P.M.; Zemp, R. Low Back Pain and Its Relationship with Sitting Behaviour among Sedentary Office Workers. Appl. Ergon. 2019, 81, 102894. [Google Scholar] [CrossRef] [PubMed]
- Barone Gibbs, B.; Hergenroeder, A.L.; Perdomo, S.J.; Kowalsky, R.J.; Delitto, A.; Jakicic, J.M. Reducing Sedentary Behaviour to Decrease Chronic Low Back Pain: The Stand Back Randomised Trial. Occup. Environ. Med. 2018, 75, 321–327. [Google Scholar] [CrossRef]
- Mahdavi, S.B.; Riahi, R.; Vahdatpour, B.; Kelishadi, R. Association between Sedentary Behavior and Low Back Pain; A Systematic Review and Meta-Analysis. Heal. Promot. Perspect. 2021, 11, 393–410. [Google Scholar] [CrossRef] [PubMed]
- Leivas, E.G.; Corrêa, L.A.; Nogueira, L.A.C. The Relationship between Low Back Pain and the Basic Lumbar Posture at Work: A Retrospective Cross-Sectional Study. Int. Arch. Occup. Environ. Health 2022, 95, 25–33. [Google Scholar] [CrossRef]
- Nourollahi, M.; Afshari, D.; Dianat, I. Awkward Trunk Postures and Their Relationship with Low Back Pain in Hospital Nurses. Work 2018, 59, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Nieminen, L.K.; Pyysalo, L.M.; Kankaanpää, M.J. Prognostic Factors for Pain Chronicity in Low Back Pain: A Systematic Review. Pain Rep. 2021, 6, 17. [Google Scholar] [CrossRef]
- Heidari, B. Knee Osteoarthritis Prevalence, Risk Factors, Pathogenesis and Features: Part I. Casp. J. Intern. Med. 2011, 2, 205–212. [Google Scholar]
- Kraus, V.B.; Sprow, K.; Powell, K.E.; Buchner, D.; Bloodgood, B.; Piercy, K.; George, S.M.; Kraus, W.E. Effects of Physical Activity in Knee and Hip Osteoarthritis: A Systematic Umbrella Review. Med. Sci. Sports Exerc. 2019, 51, 1324–1339. [Google Scholar] [CrossRef]
- Reese, J.B.; Bober, S.L.; Daly, M.B.; Program, C.; Chase, F.; Sciences, B.; Care, P.; Chase, F.; Behavior, S.; Neoplasms, B. Sex Differences in Osteoarthritis of the Knee Dr. J. Am. Acad. Orthop. Surg. 2018, 20, 3. [Google Scholar]
- Rao, S.; Riskowski, J.L.; Hannan, M.T. Musculoskeletal Conditions of the Foot and Ankle: Assessments and Treatment Options. Best Pract. Res. Clin. Rheumatol. 2012, 26, 345–368. [Google Scholar] [CrossRef]
- Palmer, K.T.; Harris, E.C.; Coggon, D. Carpal Tunnel Syndrome and Its Relation to Occupation: A Systematic Literature Review. Occup. Med. 2007, 57, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, J.F.; Gerr, F.; Atroshi, I. Carpal Tunnel Syndrome and the Use of Computer Mouse and Keyboard: A Systematic Review. BMC Musculoskelet. Disord. 2008, 9, 9. [Google Scholar] [CrossRef] [PubMed]
- Mediouni, Z.; de Roquemaurel, A.; Dumontier, C.; Becour, B.; Garrabe, H.; Roquelaure, Y.; Descatha, A. Is Carpal Tunnel Syndrome Related to Computer Exposure at Work? A Review and Meta-Analysis. J. Occup. Environ. Med. 2014, 56, 204–208. [Google Scholar] [CrossRef]
- Feng, B.; Chen, K.; Zhu, X.; Ip, W.Y.; Andersen, L.L.; Page, P.; Wang, Y. Prevalence and Risk Factors of Self-Reported Wrist and Hand Symptoms and Clinically Confirmed Carpal Tunnel Syndrome among Office Workers in China: A Cross-Sectional Study. BMC Public Health 2021, 21, 10. [Google Scholar] [CrossRef] [PubMed]
- Beach, J.; Senthilselvan, A.; Cherry, N. Factors Affecting Work-Related Shoulder Pain. Occup. Med. 2012, 62, 451–454. [Google Scholar] [CrossRef] [PubMed]
- Andersen, J.H.; Haahr, J.P.; Frost, P. Risk Factors for More Severe Regional Musculoskeletal Symptoms: A Two-year Prospective Study of a General Working Population. Arthritis Rheum. 2007, 56, 1355–1364. [Google Scholar] [CrossRef] [PubMed]
- Harkness, E.F.; Macfarlane, G.J.; Nahit, E.S.; Silman, A.J.; McBeth, J. Mechanical and Psychosocial Factors Predict New Onset Shoulder Pain: A Prospective Cohort Study of Newly Employed Workers. Occup. Environ. Med. 2003, 60, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Leclerc, A.; Chastang, J.-F.; Niedhammer, I.; Landre, M.-F.; Roquelaure, Y. Repetitive S.G. on R.W. Incid of Shoulder Pain Repetitive Work. Occup. Environ. Med. 2004, 61, 39–44. [Google Scholar]
- Descatha, A.; Chastang, J.F.; Cyr, D.; Leclerc, A.; Roquelaure, Y.; Evanoff, B. Do Workers with Self-Reported Symptoms Have an Elevated Risk of Developing Upper Extremity Musculoskeletal Disorders Three Years Later? Occup. Environ. Med. 2008, 65, 205–207. [Google Scholar] [CrossRef]
- Social, S. Reforma. Available online: https://www.seg-social.pt/reforma (accessed on 3 May 2024).
- Nordstrom, D.L.; Vierkant, R.A.; DeStefano, F.; Layde, P.M. Risk Factors for Carpal Tunnel Syndrome in a General Population. Occup. Environ. Med. 1997, 54, 734–740. [Google Scholar] [CrossRef]
- Luime, J.J.; Kuiper, J.I.; Koes, B.W.; Verhaar, J.A.; Miedema, H.S.; Burdorf, A. Work-Related Risk Factors for the Incidence and Recurrence of Shoulder and Neck Complaints among Nursing-Home and Elderly-Care Workers. Scand. J. Work. Environ. Health 2004, 30, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Anacleto Filho, P.C.; da Silva, L.; Mattos, D.; Pombeiro, A.; Castellucci, H.I.; Colim, A.; Carneiro, P.; Arezes, P. Establishing an Anthropometric Database: A Case for the Portuguese Working Population. Int. J. Ind. Ergon. 2023, 97, 103473. [Google Scholar] [CrossRef]
- Vieira, E.R.; Buckeridge Serra, M.V.G.; Brentini de Almeida, L.; Vieira Villela, W.; Domingos Scalon, J.; Veiga Quemelo, P.R. Symptoms and Risks for Musculoskeletal Disorders among Male and Female Footwear Industry Workers. Int. J. Ind. Ergon. 2015, 48, 110–116. [Google Scholar] [CrossRef]
- Moreira-Silva, I.; Azevedo, J.; Rodrigues, S.; Seixas, A.; Jorge, M. Predicting Musculoskeletal Symptoms in Workers of a Manufacturing Company. Int. J. Occup. Saf. Ergon. 2021, 27, 1136–1144. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Variables | Body Parts | Have You Had Trouble (Ache, Pain, Discomfort, Numbness) at Any Time During the Last 12 Months? * |
|---|---|---|
|
|
|
| Occupation | Male | Female | Total |
|---|---|---|---|
| Operators | 173 (32.9%) | 10 (1.9%) | 183 (34.8%) |
| Tuner | 234 (44.5%) | 0 (0.0%) | 234 (44.5%) |
| Administrative | 48 (9.1%) | 18 (3.4%) | 66 (12.5%) |
| Maintenance | 35 (6.7%) | 0 (0.0%) | 35 (6.7%) |
| Logistics | 6 (1.1%) | 2 (0.4%) | 8 (1.5%) |
| Total | 496 (94.3%) | 30 (5.7%) | 526 (100%) |
| Job Title | Task Description | Biomechanical Risk Factors |
|---|---|---|
| Operator |
|
|
| Tuner |
|
|
| Maintenance |
|
|
| Logistics |
|
|
| Administrative |
|
|
| Category | Underweight | Normal Weight | Pre-Obesity | Obesity Class I | Obesity Class II | Obesity Class III | Total |
|---|---|---|---|---|---|---|---|
| BMI Interval | (Below 18.5) | (18.5–24.9) | (25.0–29.9) | (30.0–34.9) | (35.0–39.9) | (Above 40) | |
| Female | 1 (4.2%) | 12 (50.0%) | 7 (29.2%) | 3 (12.5%) | 1 (4.2%) | 0 (0.0%) | 24 (5.4%) |
| Male | 1 (0.2%) | 161 (38.3%) | 208 (49.5%) | 38 (9.0%) | 10 (2.4%) | 2 (0.5%) | 420 (94.6%) |
| Total | 2 (0.5%) | 173 (39.0%) | 215 (48.4%) | 41 (9.2%) | 11 (2.5%) | 2 (0.5%) | 444 |
| Nutritional Status (BMI) | Age Groups (Years Old) | Total | ||||
|---|---|---|---|---|---|---|
| 19–28 | 29–38 | 39–48 | 49–58 | 59–68 | ||
| Underweight (Below 18.5) | 0 (0.0%) | 1 (0.8%) | 1 (0.8%) | 0 (0.0%) | 0 (0.0%) | 2 (0.5%) |
| Normal weight (18.5–24.9) | 31 (51.7%) | 57 (45.2%) | 38 (30.2%) | 40 (35.7%) | 5 (26.3%) | 171 (39.1%) |
| Pre-obesity (25.0–29.9) | 25 (41.7%) | 55 (43.7) | 62 (49.2%) | 56 (50.0%) | 12 (63.2%) | 210 (48.1%) |
| Obesity class I, II, and III (≥30.0) | 4 (6.7%) | 13 (10.3%) | 19 (15.8%) | 16 (14.3%) | 2 (10.5%) | 54 (12.4%) |
| Total | 60 (100%) | 126 (100%) | 120 (100%) | 112 (100%) | 19 (100%) | 437 |
| Body Parts | Statistics | Interpretation | Odds Ratio |
|---|---|---|---|
| Neck | [χ2 (1) = 1.615; p > 0.05] | A Chi-square test revealed a non-significant association between gender and developing trouble in the neck. | The odds of having neck trouble are 1.61 times greater for females than males. |
| Shoulders | [χ2 (1) = 2.758; p > 0.05] | A Chi-square test revealed a non-significant association between gender and developing shoulder trouble. | The odds of having shoulder trouble are 1.85 times greater for females than males. |
| Elbow | (p = 0.123) | Fisher’s exact test revealed a non-significant association between gender and developing elbow trouble. | The odds of having elbow trouble are 1.98 times greater for females than males. |
| Wrists/Hands * | [χ2 (1) = 4.287; p < 0.05] | A Chi-square test revealed a significant association between gender and developing trouble in wrists/hands. Although the result is statistically significant, the variables are only weakly associated. Cramer’s V effect size (0.090) indicates a weak association between the variables. | The odds of having wrist/hand trouble are 2.15 times greater for females than males. |
| Upper Back | (p = 0.267) | Fisher’s exact test revealed no significant association between gender and developing upper back trouble. | The odds of having upper back trouble are 2.02 times greater for females than males. |
| Lower Back | [χ2 (1) = 1.997; p > 0.05]. | A Chi-square test revealed a non-significant association between gender and developing trouble in the lower back. | The odds of having lower back trouble are 1.74 times greater for females than males. |
| Hips/Thighs | [χ2 (1) = 0.360; p > 0.05]. | A Chi-square test revealed a non-significant association between gender and developing trouble in the hip/thighs. | The odds of having hip/thigh trouble are 1.29 times greater for females than males. |
| Knees | [χ2 (1) = 0.085; p > 0.05]. | A Chi-square test revealed a non-significant association between gender and developing knee trouble. | The odds of having knee trouble are 1.12 times greater for females than males. |
| Ankles/Feet | [χ2 (1) = 2.983; p > 0.05]. | A Chi-square test revealed a non-significant association between gender and developing trouble in ankles/feet. | The odds of having ankles/feet trouble are 2.11 times greater for males than females. |
| Body Parts | Statistics | Interpretation | |
|---|---|---|---|
| Neck ** | [χ2 (4) = 15.306, p < 0.001]. | A Chi-square test revealed a significant association between age category and developing neck trouble. Cramer’s V effect size (0.172) indicates a weak association between the variables. | Workers aged 29–58 are more likely to have neck complaints than workers aged 19–28 and 59–68. |
| Shoulders ** | [χ2 (4) = 50.588, p < 0.001]. | A Chi-square test revealed a significant association between age category and developing shoulder trouble. Cramer’s V effect size (0.313) indicates a moderate association between the variables. | Workers aged 39–68 are more likely to have shoulder complaints than workers aged 19–38. |
| Elbow | Expected count less than 5 | ||
| Wrists/Hands ** | [χ2 (4) = 20.388, p < 0.001]. | A Chi-square test revealed a significant association between age category and developing trouble in writs/hands. Cramer’s V effect size (0.199) indicates a weak association between the variables. | Workers aged 39–68 are more likely to have wrists/hands complaints than workers aged 19–38. |
| Upper Back | Expected count less than 5 | ||
| Lower Back ** | [χ2 (4) = 18.566, p < 0.001] | A Chi-square test revealed a significant association between age category and developing trouble in the lower back. Cramer’s V effect size (0.190) indicates a weak association between the variables. | Workers aged 29–38 and 49–68 are more likely to have lower back complaints than workers aged 19–28 and 39–48. |
| Hips/Thighs ** | [χ2 (4) = 30.655, p < 0.001] | A Chi-square test revealed a significant association between age category and developing trouble in the hip/thighs. Cramer’s V effect size (0.244) indicates a moderate association between the variables. | Workers aged 49–68 are more likely to have hip/thigh complaints than workers aged 19–48. |
| Knees ** | [χ2 (4) = 23.202, p < 0.001] | A Chi-square test revealed a significant association between age category and developing knee trouble. Cramer’s V effect size (0.212) indicates a moderate association between the variables. | Workers aged 39–68 are more likely to have knee complaints than workers aged 19–38. |
| Ankles/Feet ** | [χ2 (4) = 20.819, p < 0.001] | A Chi-square test revealed a significant association between age category and developing trouble in ankles/feet. Cramer’s V effect size (0.201) indicates a moderate association between the variables. | Workers aged 39–68 are more likely to have ankle/foot complaints than workers aged 19–38. |
| Body Parts | Statistics | Interpretation | |
|---|---|---|---|
| Neck * | [χ2 (3) = 10.828; p < 0.05] | A Chi-square test revealed a significant association between job type and developing neck trouble. Cramer’s V effect size (0.145) indicates a weak association between the variables. | Tuners, Administrative, and Maintenance roles are more likely to have neck complaints than operators. |
| Shoulders | [χ2 (3) = 2.710; p > 0.05]. | A Chi-square test revealed a non-significant association between job type and developing shoulder trouble. | Tuners, Administrative, and Maintenance roles are more likely to have shoulder complaints than operators. |
| Elbow | [χ2 (3) = 7.473; p > 0.05]. | A Chi-square test revealed a non-significant association between job type and developing trouble in the elbow. | Administrative and Maintenance roles are more likely to have elbow complaints than Operators and Turners. |
| Wrists/Hands | [χ2 (3) = 4.646; p > 0.05]. | A Chi-square test revealed a non-significant association between job type and developing trouble in wrists/hands. | Tuners, Administrative and Maintenance roles are more likely to have wrist/hand complaints than Operators. |
| Upper Back | Expected count less than 5 | ||
| Lower Back ** | [χ2 (3) = 11.340; p < 0.001] | A Chi-square test revealed a significant association between job type and developing trouble in the lower back. Cramer’s V effect size (0.148) indicates a weak association between the variables. | Tuners and Administrative roles are more likely to have lower back complaints than Operators and Maintenance roles. |
| Hips/Thighs | [χ2 (3) = 3.431; p > 0.05] | A Chi-square test revealed a non-significant association between job type and developing trouble in the hip/thighs. | Tuners, Administrative and Maintenance people are more likely to have hips/thigh complaints than Operators. |
| Knees ** | [χ2 (3) = 18.031; p < 0.001] | A Chi-square test revealed a significant association between job type and developing knee trouble. Cramer’s V effect size (0.187) indicates a weak association between the variables. | Tuners, Administrative and Maintenance roles are more likely to have knee complaints than workers than Operators. |
| Ankles/Feet ** | [χ2 (3) = 35.225, p < 0.001]. | A Chi-square test revealed a significant association between job type and developing trouble in ankles/feet. Cramer’s V effect size (0.261) indicates a moderate association between the variables. | Tuners are more likely to have ankle/foot complaints than workers in Administrative, Maintenance and Operator roles. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anacleto Filho, P.C.; Braga, A.C.; Carneiro, P. Exploring Musculoskeletal Complaints in a Needle Manufacturing Industry: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2024, 21, 996. https://doi.org/10.3390/ijerph21080996
Anacleto Filho PC, Braga AC, Carneiro P. Exploring Musculoskeletal Complaints in a Needle Manufacturing Industry: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2024; 21(8):996. https://doi.org/10.3390/ijerph21080996
Chicago/Turabian StyleAnacleto Filho, Paulo C., Ana Cristina Braga, and Paula Carneiro. 2024. "Exploring Musculoskeletal Complaints in a Needle Manufacturing Industry: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 21, no. 8: 996. https://doi.org/10.3390/ijerph21080996