
Temporary Protective Shoulder Implants for Revision Surgery with Bone Glenoid Grafting


Abstract
:1. Introduction
2. Materials and Methods
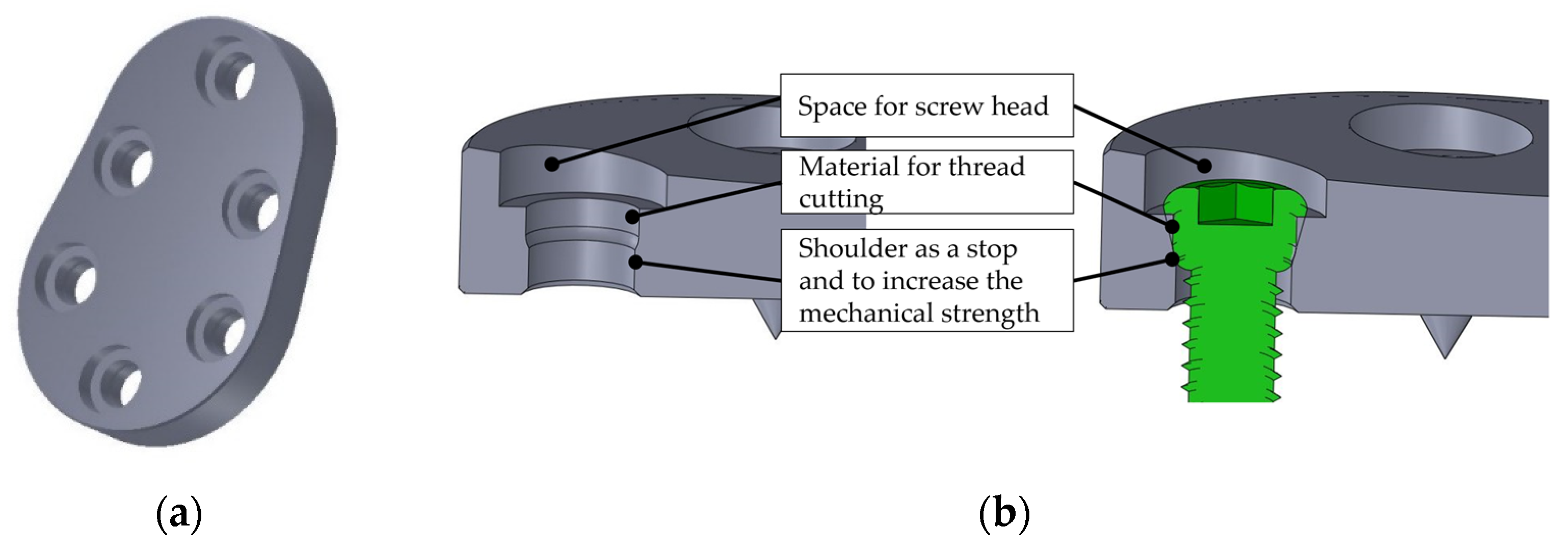
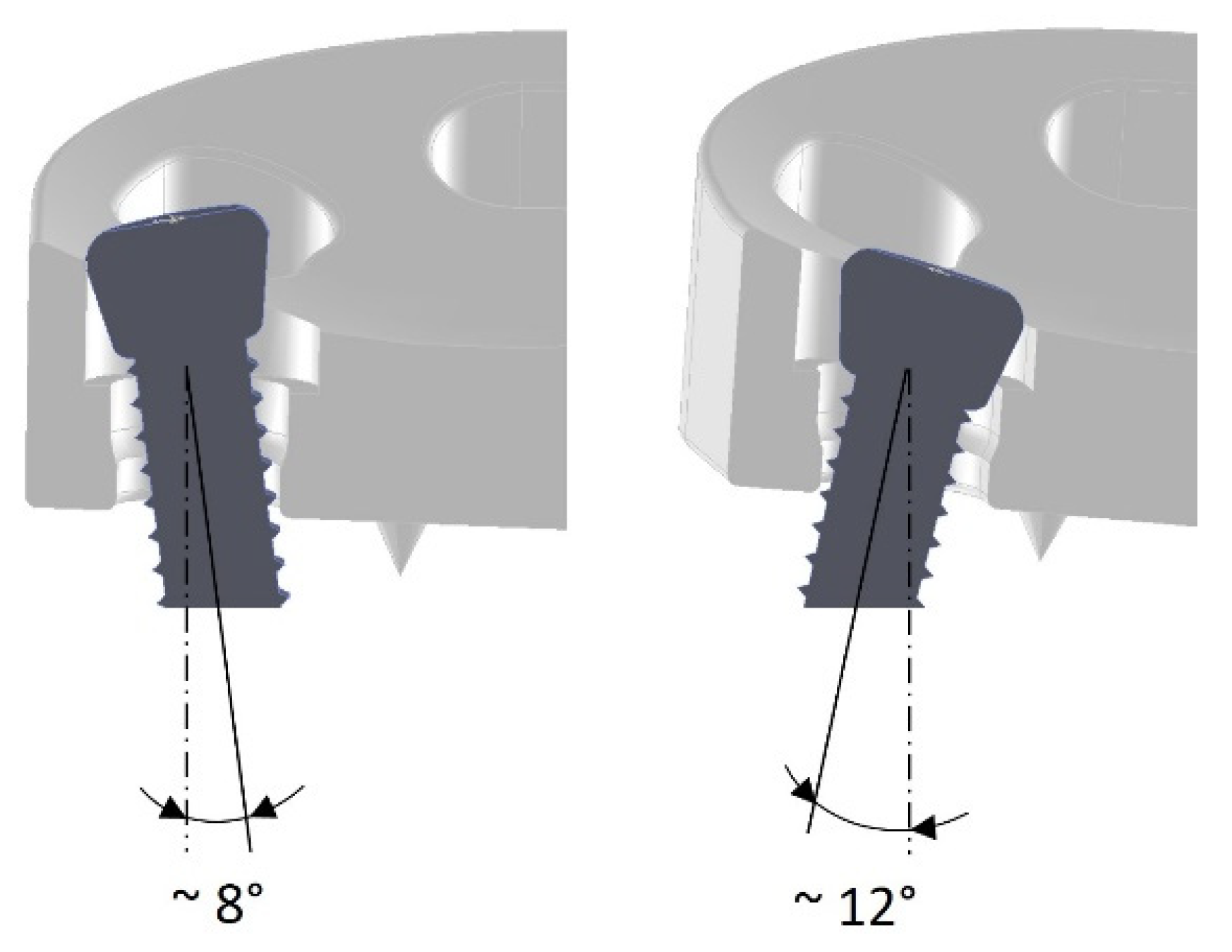
2.1. Variant 1: Multidirectional Angle-Stable Screw Connection (Rigid Fixation)
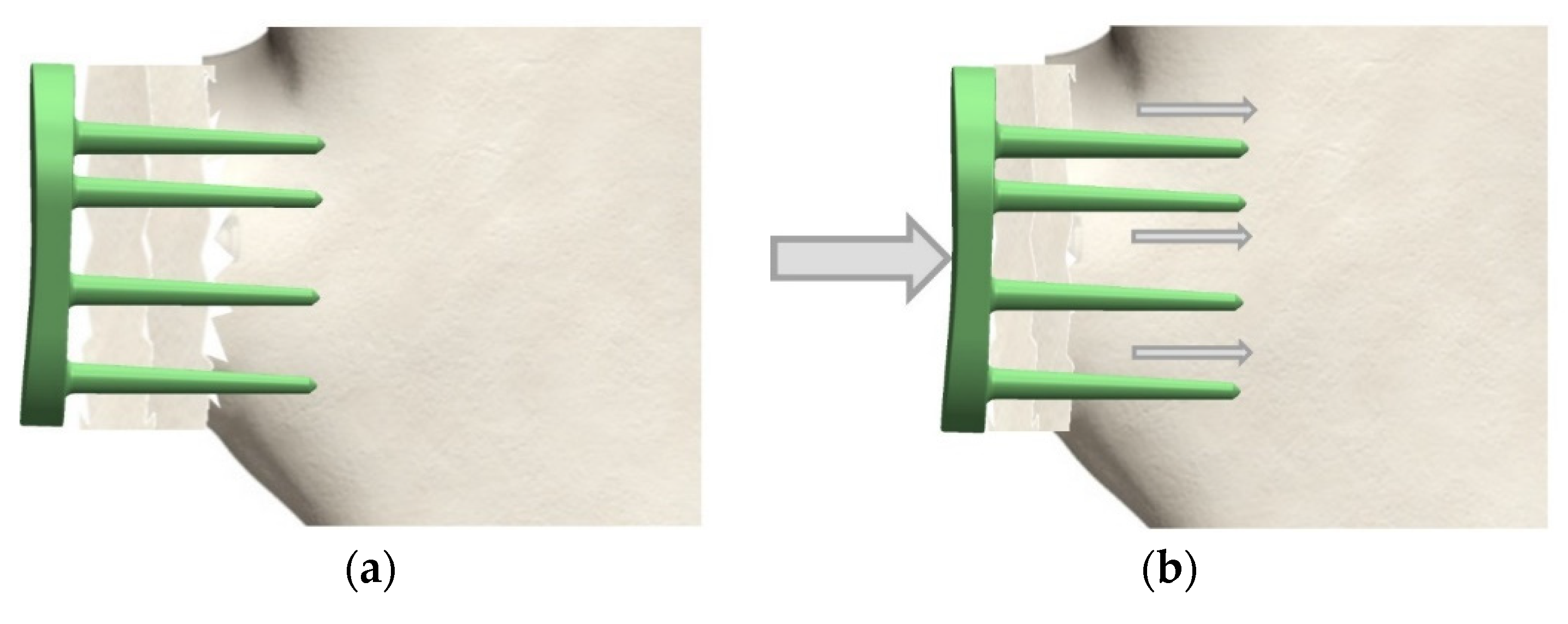
2.2. Variant 2: Dynamic Fixation (Angular Stable Pins)
3. Results
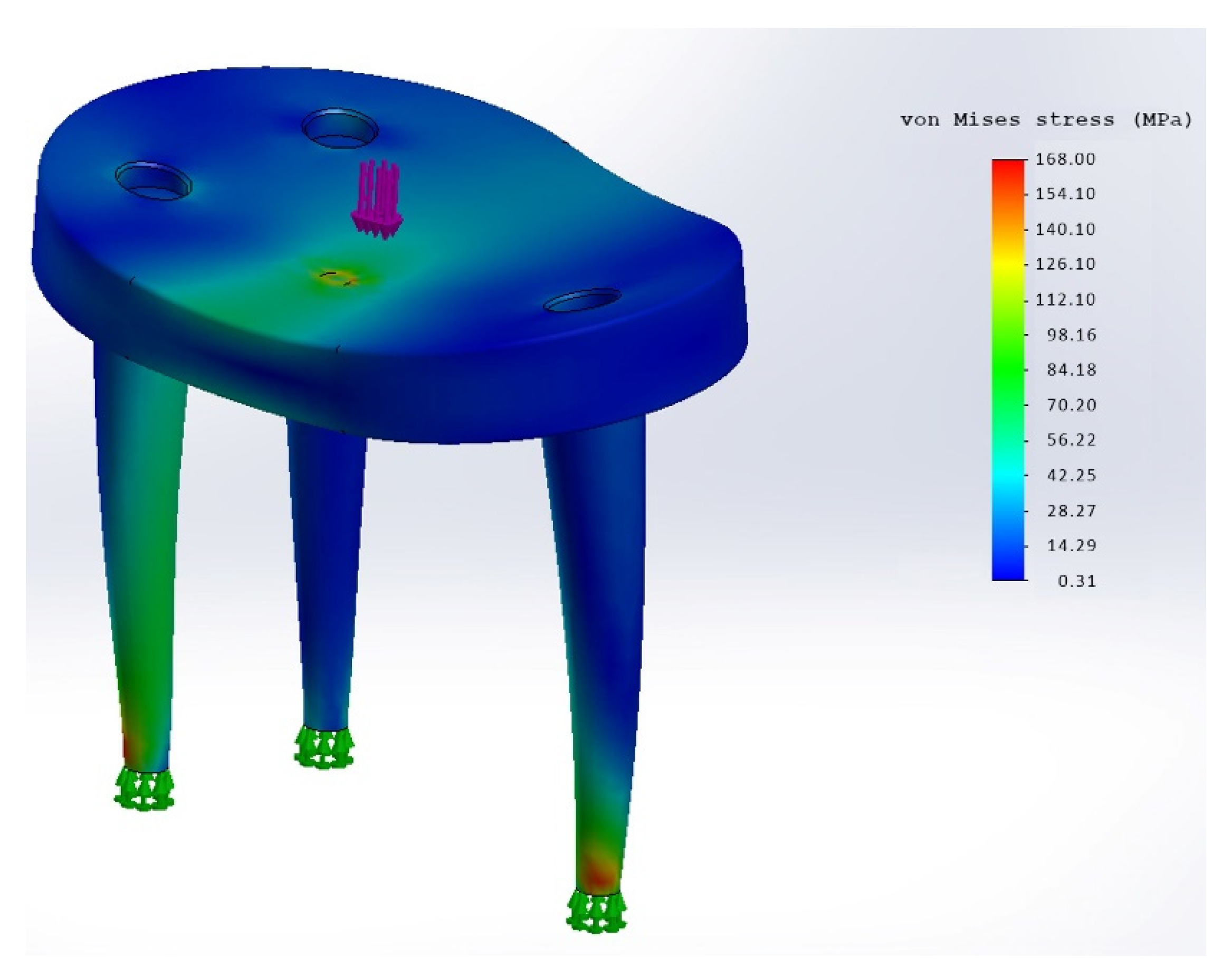
3.1. Simulation
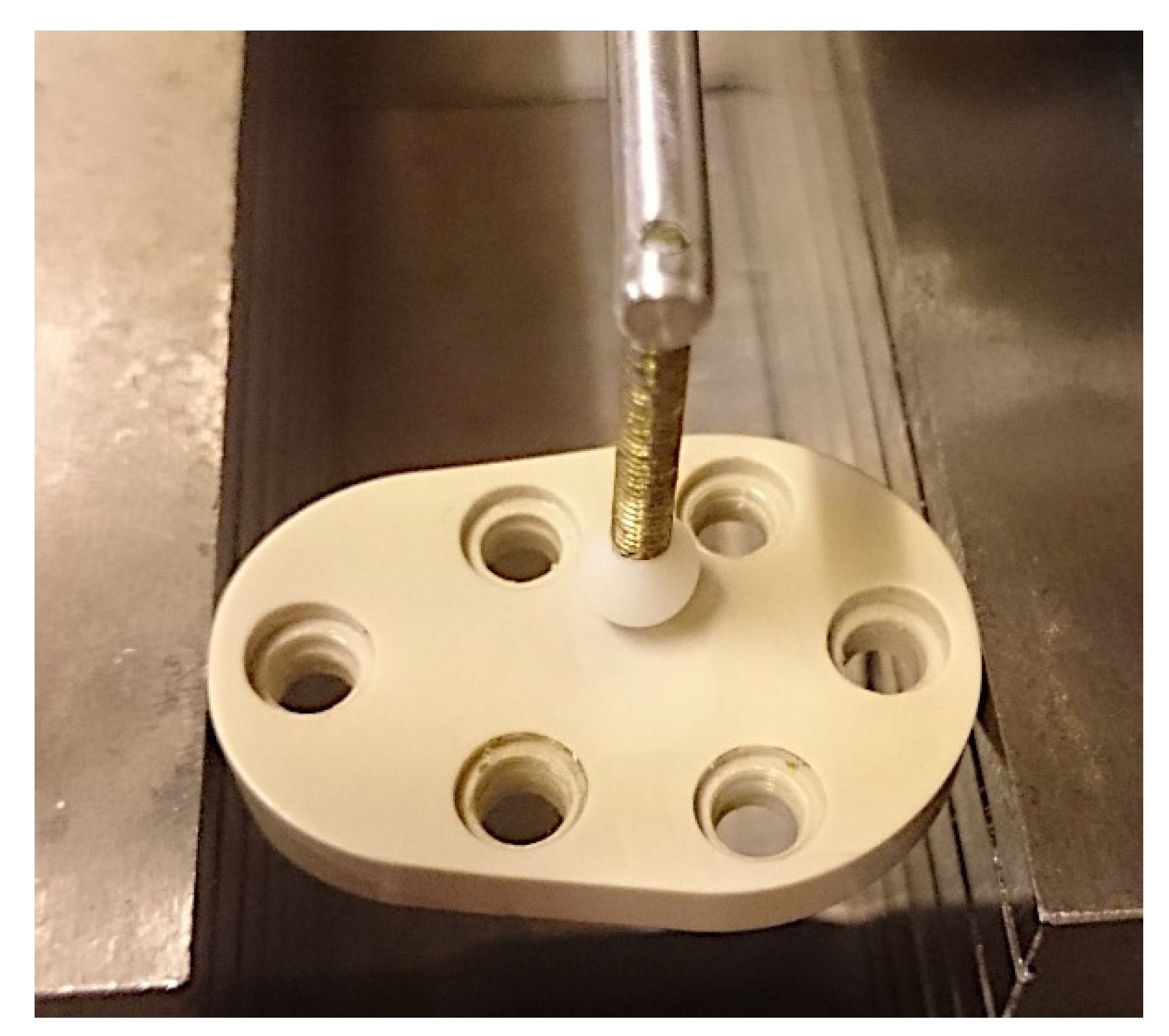
3.2. Mechanical Testing
3.2.1. Rigid Variant
3.2.2. Dynamic Variant
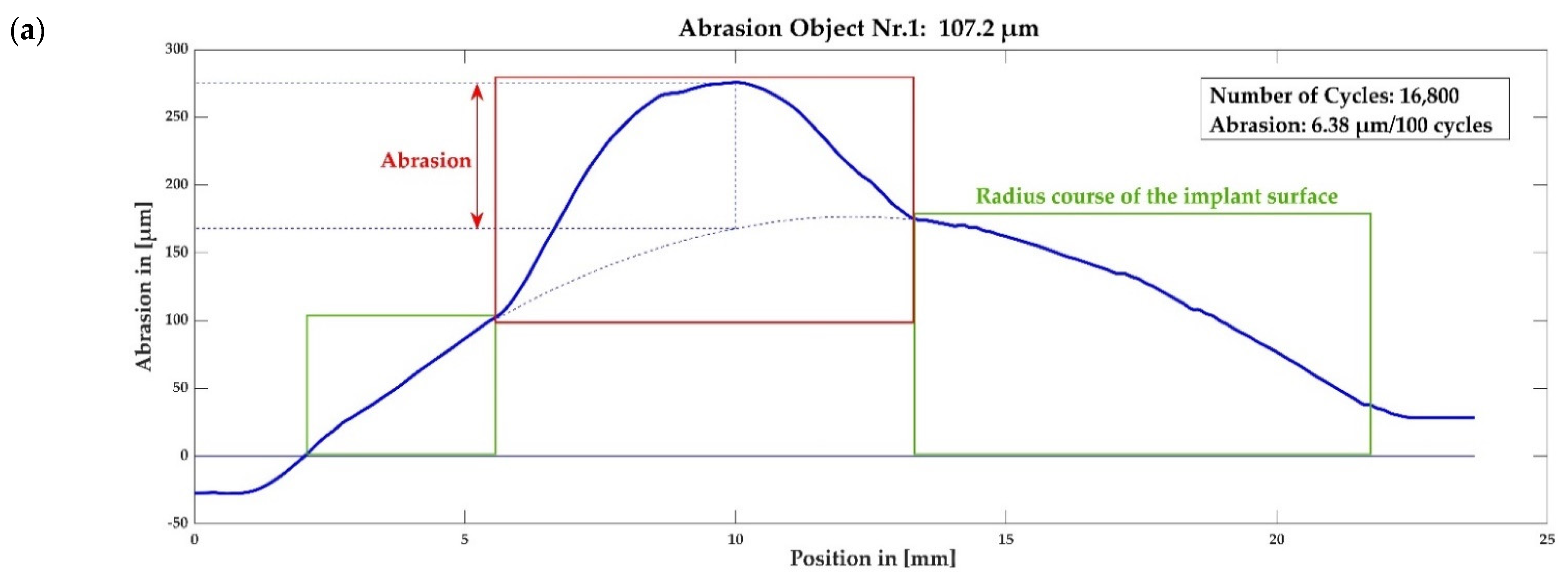
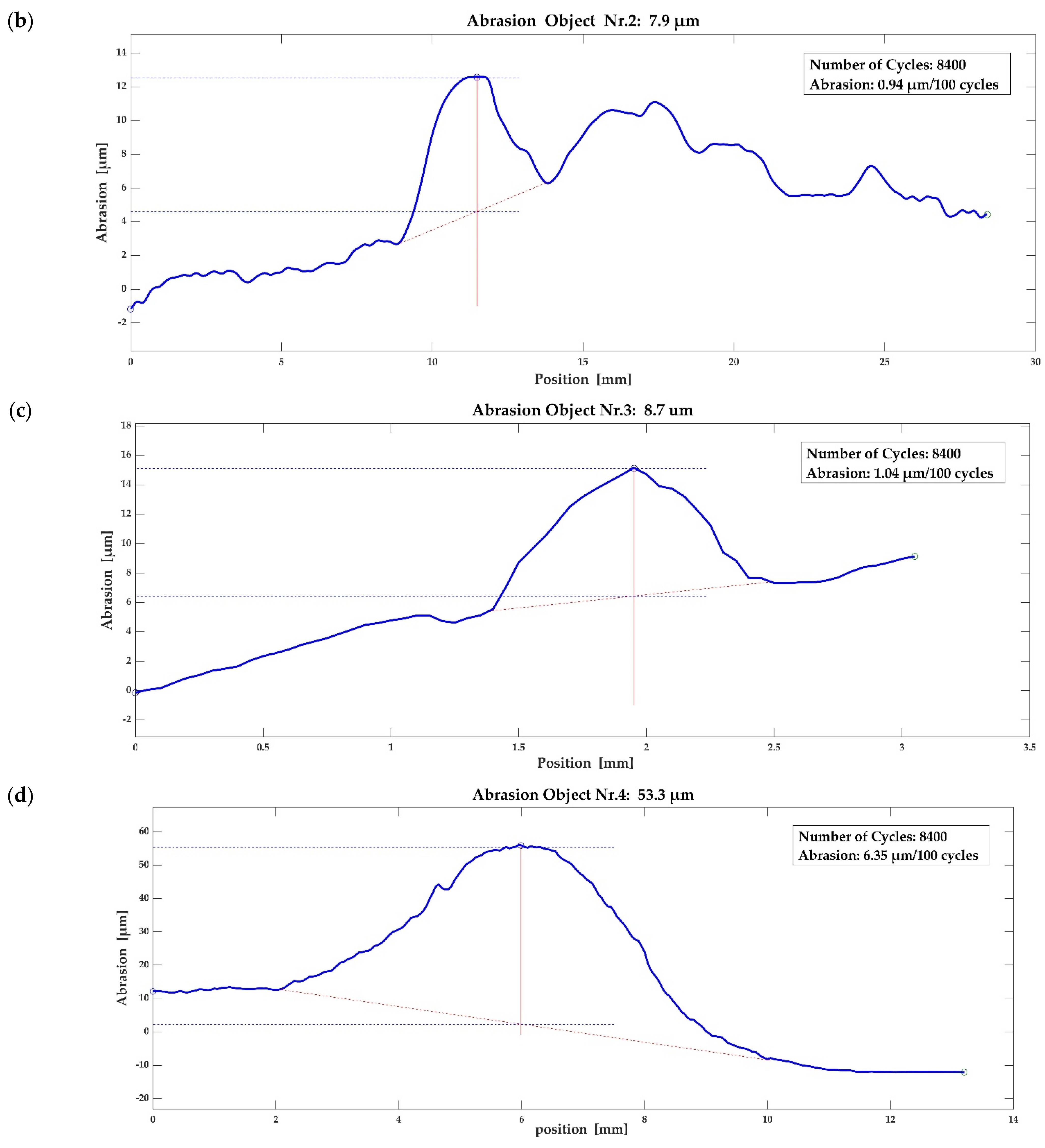
3.3. Abrasion Measurement
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
References
- Farley, K.X.; Wilson, J.M.; Kumar, A.; Gottschalk, M.B.; Daly, C.; Sanchez-Sotelo, J.; Wagner, E.R. Prevalence of Shoulder Arthroplasty in the United States and the Increasing Burden of Revision Shoulder Arthroplasty. JBJS Open Access 2021, 6, e20.00156. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Wise, B.L.; Zhang, Y.; Szabo, R.M. Increasing Incidence of Shoulder Arthroplasty in the United States. J. Bone Joint Surg. Am. 2011, 93, 2249–2254. [Google Scholar] [CrossRef] [PubMed]
- Wiater, J.M.; Fabing, M.H. Shoulder Arthroplasty: Prosthetic Options and Indications. J. Am. Acad. Orthop. Surg. 2009, 17, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Sotelo, J. Glenoid Bone Loss: Etiology, Evaluation, and Classification. Instr. Course Lect. 2019, 68, 65–78. [Google Scholar]
- Hill, J.M.; Norris, T.R. Long-Term Results of Total Shoulder Arthroplasty Following Bone-Grafting of the Glenoid. J. Bone Joint Surg. Am. 2001, 83, 877–883. [Google Scholar] [CrossRef]
- Neyton, L.; Walch, G.; Nové-Josserand, L.; Edwards, T.B. Glenoid Corticocancellous Bone Grafting after Glenoid Component Removal in the Treatment of Glenoid Loosening. J. Shoulder Elb. Surg. 2006, 15, 173–179. [Google Scholar] [CrossRef]
- Steinmann, S.P.; Cofield, R.H. Bone Grafting for Glenoid Deficiency in Total Shoulder Replacement. J. Shoulder Elb. Surg. 2000, 9, 361–367. [Google Scholar] [CrossRef]
- Brown, M.; Eseonu, K.; Rudge, W.; Warren, S.; Majed, A.; Bayley, I.; Higgs, D.; Falworth, M. The Management of Infected Shoulder Arthroplasty by Two-Stage Revision. Shoulder Elb. 2020, 12, 70–80. [Google Scholar] [CrossRef]
- Zhang, B.; Niroopan, G.; Gohal, C.; Alolabi, B.; Leroux, T.; Khan, M. Glenoid Bone Grafting in Primary Anatomic Total Shoulder Arthroplasty: A Systematic Review. Shoulder Elb. 2021, 13, 509–517. [Google Scholar] [CrossRef]
- Sheth, U.; Lee, J.Y.J.; Nam, D.; Henry, P. Early Outcomes of Augmented Glenoid Components in Anatomic Total Shoulder Arthroplasty: A Systematic Review. Shoulder Elb. 2021, 14, 238–248. [Google Scholar] [CrossRef]
- Ghoraishian, M.; Abboud, J.A.; Romeo, A.A.; Williams, G.R.; Namdari, S. Augmented Glenoid Implants in Anatomic Total Shoulder Arthroplasty: Review of Available Implants and Current Literature. J. Shoulder Elb. Surg. 2019, 28, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Gohlke, F.; Werner, B. Humeral and glenoid bone loss in shoulder arthroplasty: Classification and treatment principles. Orthopade 2017, 46, 1008–1014. [Google Scholar] [CrossRef] [PubMed]
- Iannotti, J.P.; Frangiamore, S.J. Fate of Large Structural Allograft for Treatment of Severe Uncontained Glenoid Bone Deficiency. J. Shoulder Elb. Surg. 2012, 21, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Bohsali, K.I.; Wirth, M.A.; Rockwood, C.A.J. Complications of Total Shoulder Arthroplasty. J. Bone Joint Surg. Am. 2006, 88, 2279–2292. [Google Scholar] [CrossRef]
- Chin, P.Y.K.; Sperling, J.W.; Cofield, R.H.; Schleck, C. Complications of Total Shoulder Arthroplasty: Are They Fewer or Different? J. Shoulder Elb. Surg. 2006, 15, 19–22. [Google Scholar] [CrossRef]
- Cofield, R.H.; Edgerton, B.C. Total Shoulder Arthroplasty: Complications and Revision Surgery. Instr. Course Lect. 1990, 39, 449–462. [Google Scholar]
- Hernandez, N.M.; Chalmers, B.P.; Wagner, E.R.; Sperling, J.W.; Cofield, R.H.; Sanchez-Sotelo, J. Revision to Reverse Total Shoulder Arthroplasty Restores Stability for Patients With Unstable Shoulder Prostheses. Clin. Orthop. Relat. Res. 2017, 475, 2716–2722. [Google Scholar] [CrossRef]
- Fox, T.J.; Cil, A.; Sperling, J.W.; Sanchez-Sotelo, J.; Schleck, C.D.; Cofield, R.H. Survival of the Glenoid Component in Shoulder Arthroplasty. J. Shoulder Elb. Surg. 2009, 18, 859–863. [Google Scholar] [CrossRef]
- Kasten, P.; Pape, G.; Raiss, P.; Bruckner, T.; Rickert, M.; Zeifang, F.; Loew, M. Mid-Term Survivorship Analysis of a Shoulder Replacement with a Keeled Glenoid and a Modern Cementing Technique. J. Bone Joint Surg. Br. 2010, 92, 387–392. [Google Scholar] [CrossRef]
- Walch, G.; Young, A.A.; Melis, B.; Gazielly, D.; Loew, M.; Boileau, P. Results of a Convex-Back Cemented Keeled Glenoid Component in Primary Osteoarthritis: Multicenter Study with a Follow-up Greater than 5 Years. J. Shoulder Elb. Surg. 2011, 20, 385–394. [Google Scholar] [CrossRef]
- McLendon, P.B.; Schoch, B.S.; Sperling, J.W.; Sánchez-Sotelo, J.; Schleck, C.D.; Cofield, R.H. Survival of the Pegged Glenoid Component in Shoulder Arthroplasty: Part II. J. Shoulder Elb. Surg. 2017, 26, 1469–1476. [Google Scholar] [CrossRef] [PubMed]
- Franklin, J.L.; Barrett, W.P.; Jackins, S.E.; Matsen, F.A. 3rd Glenoid Loosening in Total Shoulder Arthroplasty. Association with Rotator Cuff Deficiency. J. Arthroplast. 1988, 3, 39–46. [Google Scholar] [CrossRef]
- Karelse, A.; Van Tongel, A.; Verstraeten, T.; Poncet, D.; De Wilde, L.F. Rocking-Horse Phenomenon of the Glenoid Component: The Importance of Inclination. J. Shoulder Elb. Surg. 2015, 24, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Grob, A.; Freislederer, F.; Marzel, A.; Audigé, L.; Schwyzer, H.K.; Scheibel, M. Glenoid Component Loosening in Anatomic Total Shoulder Arthroplasty: Association between Radiological Predictors and Clinical Parameters—An Observational Study. J. Clin. Med. 2021, 10, 234. [Google Scholar] [CrossRef]
- Scalise, J.J.; Iannotti, J.P. Bone Grafting Severe Glenoid Defects in Revision Shoulder Arthroplasty. Clin. Orthop. Relat. Res. 2008, 466, 139–145. [Google Scholar] [CrossRef]
- He, L.-H.; Zhang, Z.-Y.; Zhang, X.; Xiao, E.; Liu, M.; Zhang, Y. Osteoclasts May Contribute Bone Substitute Materials Remodeling and Bone Formation in Bone Augmentation. Med. Hypotheses 2020, 135, 109438. [Google Scholar] [CrossRef]
- Hussain, Z.; Ullah, I.; Liu, X.; Shen, W.; Ding, P.; Zhang, Y.; Gao, T.; Mansoorianfar, M.; Gao, T.; Pei, R. Tannin-Reinforced Iron Substituted Hydroxyapatite Nanorods Functionalized Collagen-Based Composite Nanofibrous Coating as a Cell-Instructive Bone-Implant Interface Scaffold. Chem. Eng. J. 2022, 438, 135611. [Google Scholar] [CrossRef]
- Ullah, I.; Hussain, Z.; Zhang, Y.; Liu, X.; Ullah, S.; Zhang, Y.; Zheng, P.; Gao, T.; Liu, Y.; Zhang, Z.; et al. Inorganic Nanomaterial-Reinforced Hydrogel Membrane as an Artificial Periosteum. Appl. Mater. Today 2022, 28, 101532. [Google Scholar] [CrossRef]
- Phipatanakul, W.P.; Norris, T.R. Treatment of Glenoid Loosening and Bone Loss Due to Osteolysis with Glenoid Bone Grafting. J. Shoulder Elb. Surg. 2006, 15, 84–87. [Google Scholar] [CrossRef]
- Antuna, S.A.; Sperling, J.W.; Cofield, R.H.; Rowland, C.M. Glenoid Revision Surgery after Total Shoulder Arthroplasty. J. Shoulder Elb. Surg. 2001, 10, 217–224. [Google Scholar] [CrossRef]
- Elhassan, B.; Ozbaydar, M.; Higgins, L.D.; Warner, J.J.P. Glenoid Reconstruction in Revision Shoulder Arthroplasty. Clin. Orthop. Relat. Res. 2008, 466, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Bonnevialle, N.; Melis, B.; Neyton, L.; Favard, L.; Molé, D.; Walch, G.; Boileau, P. Aseptic Glenoid Loosening or Failure in Total Shoulder Arthroplasty: Revision with Glenoid Reimplantation. J. Shoulder Elb. Surg. 2013, 22, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Wolfson, M.; Curtin, P.; Curry, E.J.; Cerda, S.; Li, X. Giant Cell Tumor Formation Due to Metallosis after Open Latarjet and Partial Shoulder Resurfacing. Orthop. Rev. 2020, 12, 60–63. [Google Scholar] [CrossRef]
- Lederman, E.S.; Nugent, M.T.; Chhabra, A. Metallosis after Hemiarthroplasty as a Result of Glenoid Erosion Causing Contact with Retained Metallic Suture Anchors: A Case Series. J. Shoulder Elb. Surg. 2011, 20, e12–e15. [Google Scholar] [CrossRef] [PubMed]
- Sedrakyan, A. Metal-on-Metal Failures--in Science, Regulation, and Policy. Lancet 2012, 379, 1174–1176. [Google Scholar] [CrossRef]
- Smith, A.J.; Dieppe, P.; Vernon, K.; Porter, M.; Blom, A.W. Failure Rates of Stemmed Metal-on-Metal Hip Replacements: Analysis of Data from the National Joint Registry of England and Wales. Lancet 2012, 379, 1199–1204. [Google Scholar] [CrossRef]
- Seaman, S.; Kerezoudis, P.; Bydon, M.; Torner, J.C.; Hitchon, P.W. Titanium vs. Polyetheretherketone (PEEK) Interbody Fusion: Meta-Analysis and Review of the Literature. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Aust. 2017, 44, 23–29. [Google Scholar] [CrossRef]
- Honigmann, P.; Sharma, N.; Schumacher, R.; Rueegg, J.; Haefeli, M.; Thieringer, F. In-Hospital 3D Printed Scaphoid Prosthesis Using Medical-Grade Polyetheretherketone (PEEK) Biomaterial. Biomed Res. Int. 2021, 2021, 1301028. [Google Scholar] [CrossRef]
- de Ruiter, L.; Rankin, K.; Browne, M.; Briscoe, A.; Janssen, D.; Verdonschot, N. Decreased Stress Shielding with a PEEK Femoral Total Knee Prosthesis Measured in Validated Computational Models. J. Biomech. 2021, 118, 110270. [Google Scholar] [CrossRef]
- Morrison, C.; Macnair, R.; MacDonald, C.; Wykman, A.; Goldie, I.; Grant, M.H. In Vitro Biocompatibility Testing of Polymers for Orthopaedic Implants Using Cultured Fibroblasts and Osteoblasts. Biomaterials 1995, 16, 987–992. [Google Scholar] [CrossRef]
- Skirbutis, G.; Dzingutė, A.; Masiliūnaitė, V.; Šulcaitė, G.; Žilinskas, J. PEEK Polymer’s Properties and Its Use in Prosthodontics. A Review. Stomatologija 2018, 20, 54–58. [Google Scholar] [PubMed]
- Horák, Z.; Pokorný, D.; Fulín, P.; Šlouf, M.; Jahoda, D.; Sosna, A. Polyetheretherketon (PEEK)—I. Část: Perspektivní Materiál pro Ortopedickou a Traumatologickou Praxi. Acta Chir. Orthop. Traumatol. Cech. 2010, 77, 463–469. [Google Scholar] [PubMed]
- Pokorný, D.; Fulín, P.; Slouf, M.; Jahoda, D.; Landor, I.; Sosna, A. [Polyetheretherketone (PEEK). Part II: Application in Clinical Practice]. Acta Chir. Orthop. Traumatol. Cech. 2010, 77, 470–478. [Google Scholar]
- Williams, D. Polyetheretherketone for Long-Term Implantable Devices. Med. Device Technol. 2008, 19, 10–11. [Google Scholar]
- Abdullah, M.R.; Goharian, A.; Abdul Kadir, M.R.; Wahit, M.U. Biomechanical and Bioactivity Concepts of Polyetheretherketone Composites for Use in Orthopedic Implants-a Review. J. Biomed. Mater. Res. A 2015, 103, 3689–3702. [Google Scholar] [CrossRef]
- Modjarrd, K.; Ebnesajjad, S. (Eds.) Handbook of Polymer Applications in Medicine and Medical Devices, 1st ed.; Elsevier Science: Oxford, UK, 2013; ISBN 9780323221696. [Google Scholar]
- Bola, M.; Simões, J.A.; Ramos, A. Finite Element Modelling and Experimental Validation of a Total Implanted Shoulder Joint. Comput. Methods Programs Biomed. 2021, 207, 106158. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, G.; Graichen, F.; Bender, A.; Rohlmann, A.; Halder, A.; Beier, A.; Westerhoff, P. In Vivo Gleno-Humeral Joint Loads during Forward Flexion and Abduction. J. Biomech. 2011, 44, 1543–1552. [Google Scholar] [CrossRef]
- Rafolt, D.; Gallasch, E. Surface myomechanical responses recorded on a scanner galvanometer. Med Biol Eng Comput. 2002, 40, 594–599. [Google Scholar] [CrossRef]
- Scholes, S.C.; Unsworth, A. Investigating the potential of implantable grade PEEK as a bearing material against various counterfaces. In Proceedings of the Europen Society for Biomaterials Conference, Nantes, France, 27 September–1 October 2006. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Property | Units | PEEK-OPTIMA |
|---|---|---|
| Tensile Strength (Yield) | MPa (ksi) | 115 |
| Tensile Elongation (Break) | % | 20 |
| Flexural Modulus | GPa | 4 |
| Flexural Strength | MPa | 170 |
| Izod Impact (Unnotched) | kJm−2 | Does not break |
| Izod Impact (Notched) | kJm−2 | 4.7 |
| Test Object No. | Material |
|---|---|
| Test object 1 | Test sample of a glenoid protective prosthesis made of technical PEEK: KETRON PEEK-1000 (not medical grade) |
| Test object 2 | Test plates made of medical grade PEEK No. 1 |
| Test object 3 | Test plates made of medical grade PEEK No. 2 |
| Test object 4 | Comparison sample of a glenoid component of an anatomical shoulder prosthesis (Global Advantage Keeled Glenoid, DePuy) made of PE (1020 XLK UHMWPE) |
| Tensile Elongation | Rigid Variant | Dynamic Variant |
|---|---|---|
| max. Tensile Elongation PEEK-Optima | 20% | 20% |
| Analysis Sample Material | 24% | 24% |
| Result FEM (500 N) | 2.2% | - |
| Strain | Rigid Variant | Dynamic Variant |
| Tensile Strength PEEK-Optima | 100 MPa | 100 MPa |
| Analysis Sample Material | 117 MPa | 117 MPa |
| Max. Strain FEM (500 N) | 60 MPa | ~100 MPa (168 MPa peak) |
| Max. Strain FEM (1500 N) | 90 MPa | >100 MPa |
| Displacement | Rigid Variant | Dynamic Variant |
| Max. Displacement (deflection/sag) at 500 N FEM | 0.1 mm | 0.95 mm |
| CFR PEEK-OPTIMA/CFR PEEK-OPTIMA | CFR PEEK-OPTIMA/Alumina | CFR PEEK-OPTIMA/CoCrMo Steel | UHMWPE/CoCrMo Steel |
|---|---|---|---|
| 0.34 | 0.18 | 0.1 | 1.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schaffarzick, D.; Entacher, K.; Rafolt, D.; Schuller-Götzburg, P. Temporary Protective Shoulder Implants for Revision Surgery with Bone Glenoid Grafting. Materials 2022, 15, 6457. https://doi.org/10.3390/ma15186457
Schaffarzick D, Entacher K, Rafolt D, Schuller-Götzburg P. Temporary Protective Shoulder Implants for Revision Surgery with Bone Glenoid Grafting. Materials. 2022; 15(18):6457. https://doi.org/10.3390/ma15186457
Chicago/Turabian StyleSchaffarzick, Daniel, Karl Entacher, Dietmar Rafolt, and Peter Schuller-Götzburg. 2022. "Temporary Protective Shoulder Implants for Revision Surgery with Bone Glenoid Grafting" Materials 15, no. 18: 6457. https://doi.org/10.3390/ma15186457
APA StyleSchaffarzick, D., Entacher, K., Rafolt, D., & Schuller-Götzburg, P. (2022). Temporary Protective Shoulder Implants for Revision Surgery with Bone Glenoid Grafting. Materials, 15(18), 6457. https://doi.org/10.3390/ma15186457