
A Volumetric Absorptive Microsampling UPLC-MS/MS Method for Simultaneous Quantification of Tacrolimus, Mycophenolic Acid and Creatinine in Whole Blood of Renal Transplant Recipients

 ,
,  ,
,
Abstract
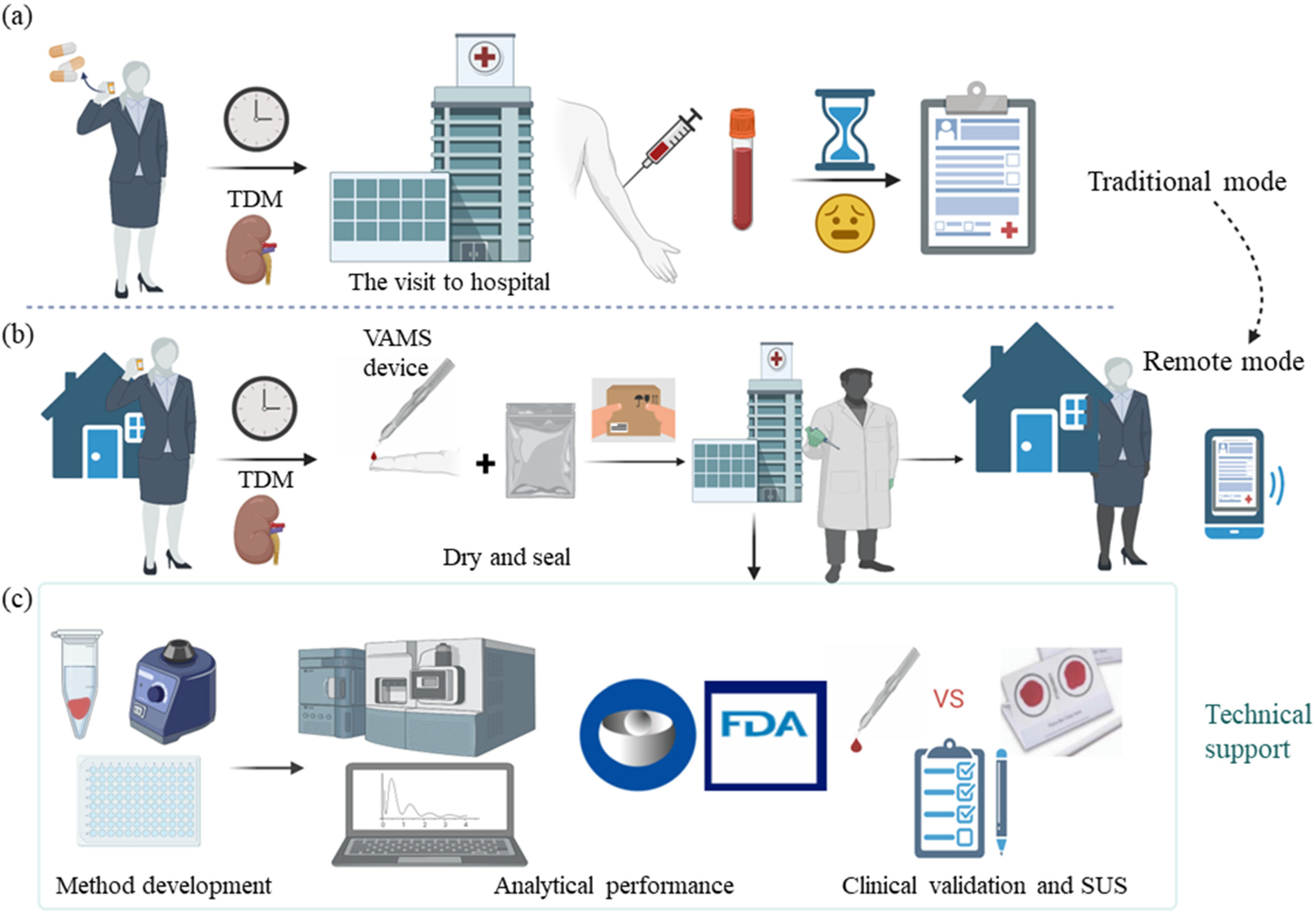
:1. Introduction
2. Materials and Methods
2.1. Reagents and Materials
2.2. Equipments and Conditions
2.3. Calibration Standards and Quality Control Samples
2.4. Shared Sample Extraction
2.5. Bioanalytical Validation
2.5.1. Standard Curve and Lower Limit of Quantitation
2.5.2. Selectivity and Carryover Effect
2.5.3. Accuracy and Precision
2.5.4. Matrix Effect, Extraction Recovery, and Process Efficiency
2.5.5. Dilution Integrity
2.5.6. Effects of Hematocrit and Anticoagulants
2.5.7. Stability
2.6. Clinical Validation
2.7. Statistical Analysis and Computing
3. Results
3.1. Equilibration Times
3.2. Bioanalytical Validation
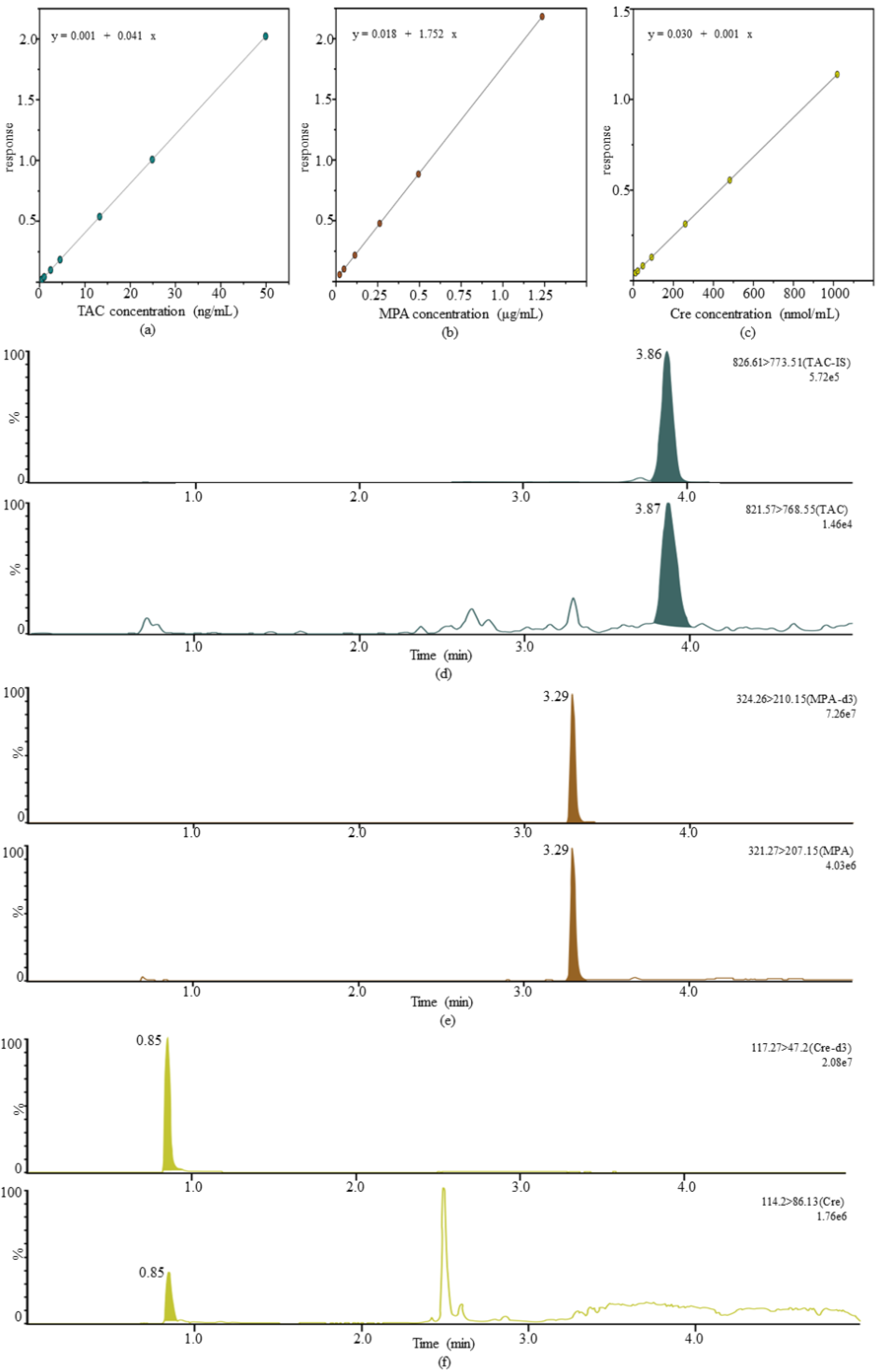
3.2.1. Standard Curve and Lower Limit of Quantitation
3.2.2. Selective and Carryover Effect
3.2.3. Accuracy and Precision
3.2.4. Matrix Effect
3.2.5. Extraction Recovery and Process Efficiency
3.2.6. Dilution Integrity
3.2.7. Hematocrit Effect and Effects of Anticoagulants
3.2.8. Stability
3.3. Clinical Validation
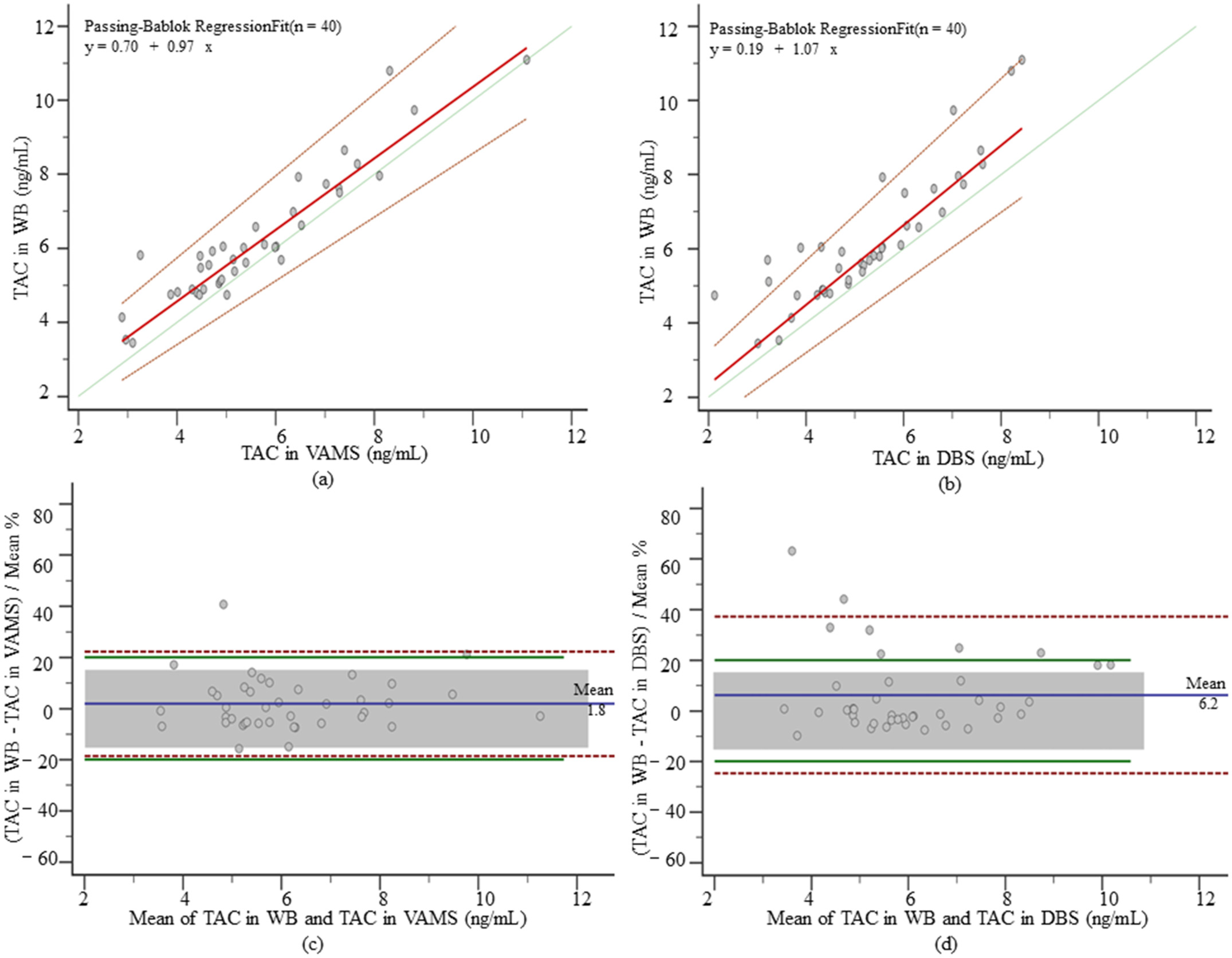
3.3.1. TAC in VAMS and DBS
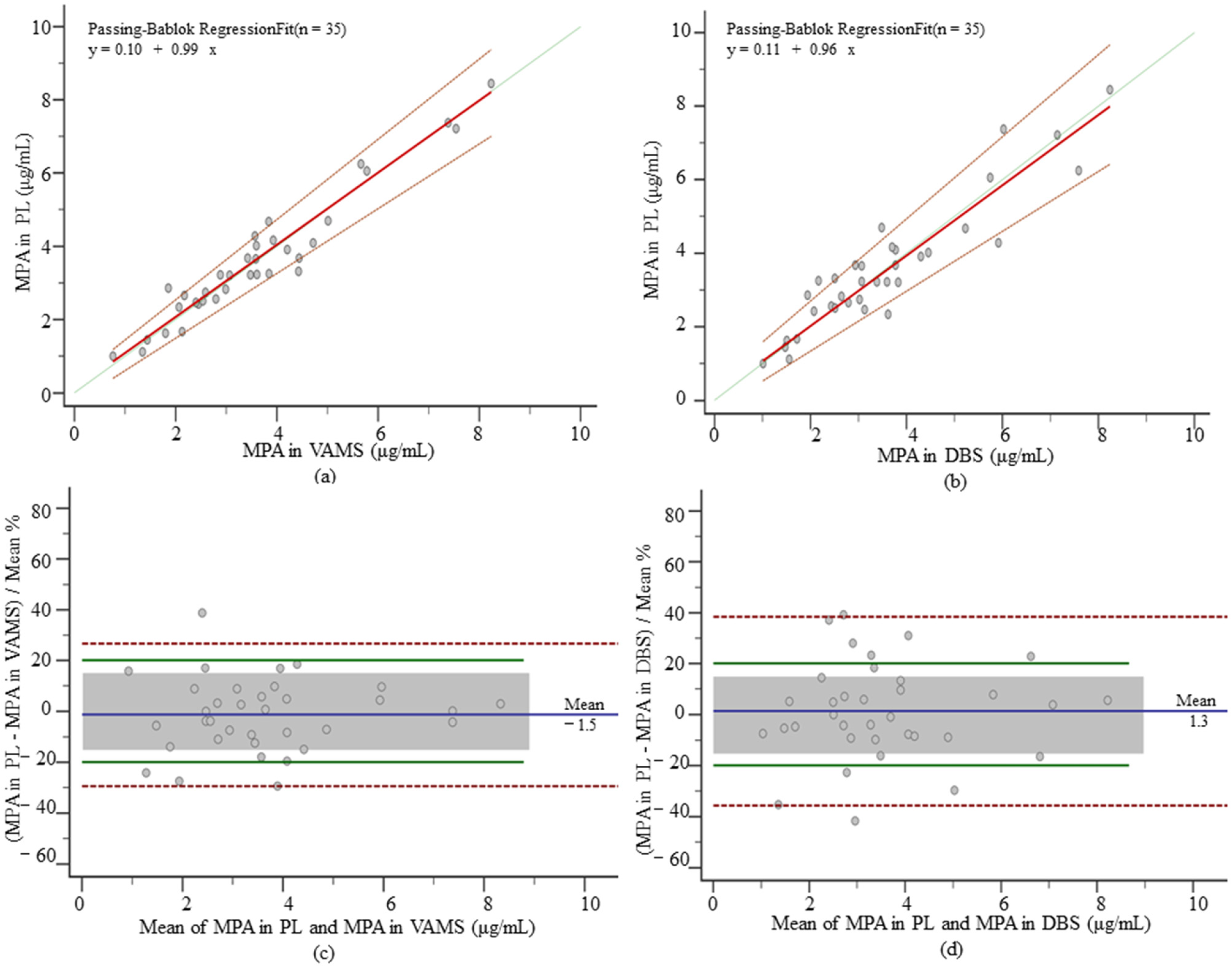
3.3.2. MPA in VAMS and DBS
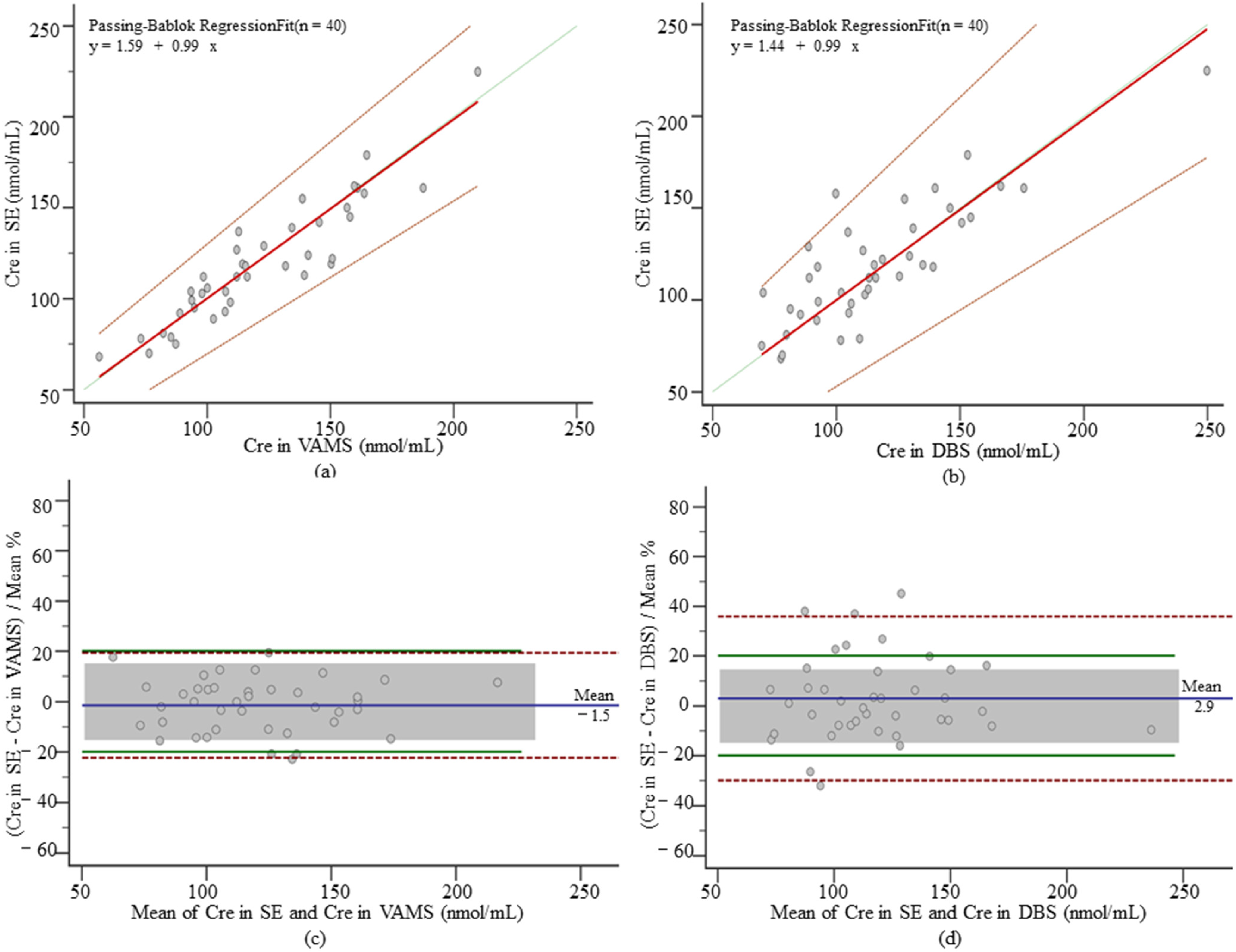
3.3.3. Cre in VAMS and DBS
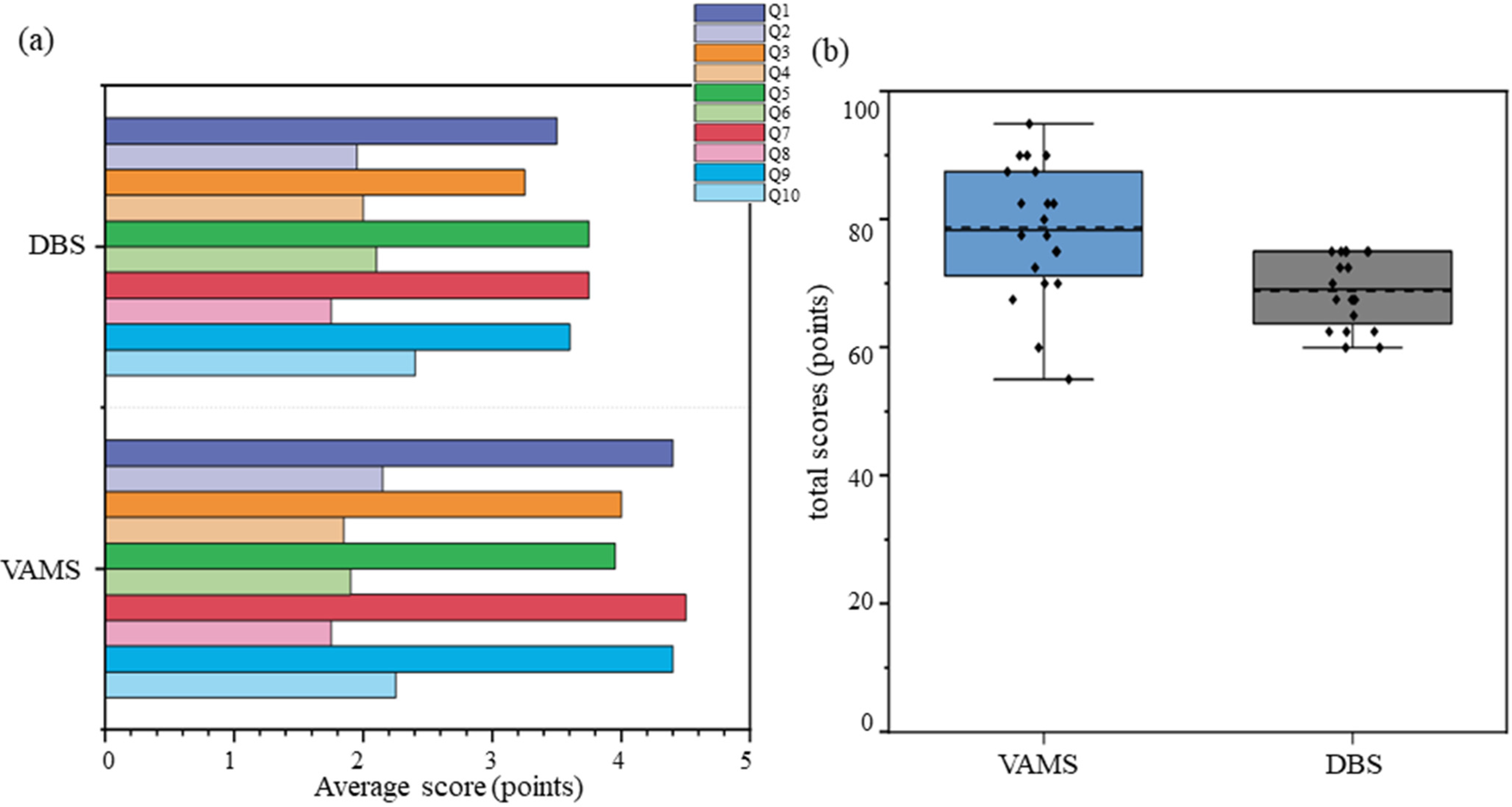
3.4. Questionnaires
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lim, M.A.; Kohli, J.; Bloom, R.D. Immunosuppression for kidney transplantation: Where are we now and where are we going? Transplant. Rev. 2017, 31, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Freudenberger, K.; Hilbig, U.; Gauglitz, G. Recent advances in therapeutic drug monitoring of immunosuppressive drugs. TrAC Trends Anal. Chem. 2016, 79, 257–268. [Google Scholar] [CrossRef]
- White, C.A.; Siegal, D.; Akbari, A.; Knoll, G.A. Use of kidney function end points in kidney transplant trials: A systematic review. Am. J. Kidney Dis. 2010, 56, 1140–1157. [Google Scholar] [CrossRef] [PubMed]
- Guerra Valero, Y.C.; Wallis, S.C.; Lipman, J.; Stove, C.; Roberts, J.A.; Parker, S.L. Clinical application of microsampling versus conventional sampling techniques in the quantitative bioanalysis of antibiotics: A systematic review. Bioanalysis 2018, 10, 407–423. [Google Scholar] [CrossRef] [PubMed]
- Tey, H.Y.; See, H.H. A review of recent advances in microsampling techniques of biological fluids for therapeutic drug monitoring. J. Chromatogr. A 2021, 1635, 461731. [Google Scholar] [CrossRef]
- Patel, S.R.; Bryan, P.; Spooner, N.; Timmerman, P.; Wickremsinhe, E. Microsampling for quantitative bioanalysis, an industry update: Output from an AAPS/EBF survey. Bioanalysis 2019, 11, 619–628. [Google Scholar] [CrossRef]
- Scribel, L.; Zavascki, A.P.; Matos, D.; Silveira, F.; Peralta, T.; Goncalves Landgraf, N.; Lamb Wink, P.; Cezimbra da Silva, A.C.; Bordin Andriguetti, N.; Loss Lisboa, L.; et al. Vancomycin and creatinine determination in dried blood spots: Analytical validation and clinical assessment. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2020, 1137, 121897. [Google Scholar] [CrossRef]
- Dickerson, J.A.; Sinkey, M.; Jacot, K.; Stack, J.; Sadilkova, K.; Law, Y.M.; Jack, R.M. Tacrolimus and sirolimus in capillary dried blood spots allows for remote monitoring. Pediatr. Transplant. 2015, 19, 101–106. [Google Scholar] [CrossRef]
- Zwart, T.C.; Gokoel, S.R.M.; van der Boog, P.J.M.; de Fijter, J.W.; Kweekel, D.M.; Swen, J.J.; Guchelaar, H.J.; Moes, D. Therapeutic drug monitoring of tacrolimus and mycophenolic acid in outpatient renal transplant recipients using a volumetric dried blood spot sampling device. Br. J. Clin. Pharmacol. 2018, 84, 2889–2902. [Google Scholar] [CrossRef] [Green Version]
- Shokati, T.; Bodenberger, N.; Gadpaille, H.; Schniedewind, B.; Vinks, A.A.; Jiang, W.; Alloway, R.R.; Christians, U. Quantification of the Immunosuppressant Tacrolimus on Dried Blood Spots Using LC-MS/MS. J. Vis. Exp. 2015, 105, e52424. [Google Scholar] [CrossRef]
- Klak, A.; Pauwels, S.; Vermeersch, P. Preanalytical considerations in therapeutic drug monitoring of immunosuppressants with dried blood spots. Diagnosis 2019, 6, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Denniff, P.; Spooner, N. Volumetric absorptive microsampling: A dried sample collection technique for quantitative bioanalysis. Anal. Chem. 2014, 86, 8489–8495. [Google Scholar] [CrossRef] [PubMed]
- Protti, M.; Mandrioli, R.; Mercolini, L. Tutorial: Volumetric absorptive microsampling (VAMS). Anal. Chim. Acta 2019, 1046, 32–47. [Google Scholar] [CrossRef] [PubMed]
- Kok, M.G.M.; Fillet, M. Volumetric absorptive microsampling: Current advances and applications. J. Pharm. Biomed. Anal. 2018, 147, 288–296. [Google Scholar] [CrossRef]
- Kita, K.; Mano, Y. Application of volumetric absorptive microsampling device for quantification of tacrolimus in human blood as a model drug of high blood cell partition. J. Pharm. Biomed. Anal. 2017, 143, 168–175. [Google Scholar] [CrossRef]
- Marshall, D.J.; Kim, J.J.; Brand, S.; Bryne, C.; Keevil, B.G. Assessment of tacrolimus and creatinine concentration collected using Mitra microsampling devices. Ann. Clin. Biochem. 2020, 57, 389–396. [Google Scholar] [CrossRef]
- Paniagua-Gonzalez, L.; Lendoiro, E.; Otero-Anton, E.; Lopez-Rivadulla, M.; de-Castro-Rios, A.; Cruz, A. Comparison of conventional dried blood spots and volumetric absorptive microsampling for tacrolimus and mycophenolic acid determination. J. Pharm. Biomed. Anal. 2022, 208, 114443. [Google Scholar] [CrossRef]
- Bioanalytical Method Validation Guidance for Industry. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/bioanalytical-method-validation-guidance-industry (accessed on 10 September 2022).
- Bioanalytical Method Validation. Available online: https://www.ema.europa.eu/en/bioanalytical-method-validation (accessed on 10 September 2022).
- Capiau, S.; Veenhof, H.; Koster, R.A.; Bergqvist, Y.; Boettcher, M.; Halmingh, O.; Keevil, B.G.; Koch, B.C.P.; Linden, R.; Pistos, C.; et al. Official International Association for Therapeutic Drug Monitoring and Clinical Toxicology Guideline: Development and Validation of Dried Blood Spot-Based Methods for Therapeutic Drug Monitoring. Ther. Drug Monit. 2019, 41, 409–430. [Google Scholar] [CrossRef]
- Mathew, B.S.; Mathew, S.K.; Aruldhas, B.W.; Prabha, R.; Gangadharan, N.; David, V.G.; Varughese, S.; John, G.T. Analytical and clinical validation of dried blood spot and volumetric absorptive microsampling for measurement of tacrolimus and creatinine after renal transplantation. Clin. Biochem. 2022, 105–106, 25–34. [Google Scholar] [CrossRef]
- Passing, H.; Bablok, W. A new biometrical procedure for testing the equality of measurements from two different analytical methods. Application of linear regression procedures for method comparison studies in clinical chemistry, Part I. J. Clin. Chem. Clin. Biochem. 1983, 21, 709–720. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Sheiner, L.B.; Beal, S.L. Some suggestions for measuring predictive performance. J. Pharmacokinet. Biopharm. 1981, 9, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Brooke, J. SUS: A quick and dirty usability scale. In Usability Evaluation in Industry, 1st ed.; Jordan, P.W., Thomas, B., Eds.; Taylor and Francis: London, UK, 1996; Volume 189. [Google Scholar]
- Undre, N.; Hussain, I.; Meijer, J.; Stanta, J.; Swan, G.; Dawson, I. Quantitation of Tacrolimus in Human Whole Blood Samples Using the MITRA Microsampling Device. Ther. Drug Monit. 2021, 43, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Koster, R.A.; Niemeijer, P.; Veenhof, H.; Hateren, K.V.; Alffenaar, J.C.; Touw, D.J. A volumetric absorptive microsampling LC-MS/MS method for five immunosuppressants and their hematocrit effects. Bioanalysis 2019, 11, 495–508. [Google Scholar] [CrossRef] [PubMed]
- Tron, C.; Ferrand-Sorre, M.J.; Querzerho-Raguideau, J.; Chemouny, J.M.; Houssel-Debry, P.; Verdier, M.C.; Bellissant, E.; Lemaitre, F. Volumetric absorptive microsampling for the quantification of tacrolimus in capillary blood by high performance liquid chromatography-tandem mass spectrometry. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2021, 1165, 122521. [Google Scholar] [CrossRef]
- Andriguetti, N.B.; Lisboa, L.L.; Hahn, S.R.; Pagnussat, L.R.; Antunes, M.V.; Linden, R. Simultaneous determination of vancomycin and creatinine in plasma applied to volumetric absorptive microsampling devices using liquid chromatography-tandem mass spectrometry. J. Pharm. Biomed. Anal. 2019, 165, 315–324. [Google Scholar] [CrossRef]
- Zwart, T.C.; Metscher, E.; van der Boog, P.J.M.; Swen, J.J.; de Fijter, J.W.; Guchelaar, H.J.; de Vries, A.P.J.; Moes, D. Volumetric microsampling for simultaneous remote immunosuppressant and kidney function monitoring in outpatient kidney transplant recipients. Br. J. Clin. Pharmacol. 2022, in press. [CrossRef]
- Koster, R.A.; Veenhof, H.; Botma, R.; Hoekstra, A.T.; Berger, S.P.; Bakker, S.J.; Alffenaar, J.C.; Touw, D.J. Dried blood spot validation of five immunosuppressants, without hematocrit correction, on two LC-MS/MS systems. Bioanalysis 2017, 9, 553–563. [Google Scholar] [CrossRef]
- Veenhof, H.; Koster, R.A.; Junier, L.A.T.; Berger, S.P.; Bakker, S.J.L.; Touw, D.J. Volumetric absorptive microsampling and dried blood spot microsampling vs. conventional venous sampling for tacrolimus trough concentration monitoring. Clin. Chem. Lab. Med. 2020, 58, 1687–1695. [Google Scholar] [CrossRef]
- Iboshi, H.; Yamaguchi, H.; Suzuki, H.; Kikuchi, M.; Tanaka, M.; Takasaki, S.; Takahashi, A.; Maekawa, M.; Shimada, M.; Matsuda, Y.; et al. Development of a Liquid Chromatography-Tandem Mass Spectrometric Method for Quantification of Mycophenolic Acid and Its Glucuronides in Dried Blood Spot Samples. Ther. Drug Monit. 2017, 39, 648–653. [Google Scholar] [CrossRef]
- Almardini, R.; Taybeh, E.O.; Alsous, M.M.; Hawwa, A.F.; McKeever, K.; Horne, R.; McElnay, J.C. A multiple methods approach to determine adherence with prescribed mycophenolate in children with kidney transplant. Br. J. Clin. Pharmacol. 2019, 85, 1434–1442. [Google Scholar] [CrossRef] [PubMed]
- Martial, L.C.; Hoogtanders, K.E.J.; Schreuder, M.F.; Cornelissen, E.A.; van der Heijden, J.; Joore, M.A.; Van Maarseveen, E.M.; Burger, D.M.; Croes, S.; Bruggemann, R.J.M.; et al. Dried Blood Spot Sampling for Tacrolimus and Mycophenolic Acid in Children: Analytical and Clinical Validation. Ther. Drug Monit. 2017, 39, 412–421. [Google Scholar] [CrossRef] [PubMed]
- Borrows, R.; Chusney, G.; Loucaidou, M.; James, A.; Lee, J.; Tromp, J.V.; Owen, J.; Cairns, T.; Griffith, M.; Hakim, N.; et al. Mycophenolic acid 12-h trough level monitoring in renal transplantation: Association with acute rejection and toxicity. Am. J. Transplant. 2006, 6, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Veenhof, H.; Koster, R.A.; Alffenaar, J.C.; Berger, S.P.; Bakker, S.J.L.; Touw, D.J. Clinical Validation of Simultaneous Analysis of Tacrolimus, Cyclosporine A, and Creatinine in Dried Blood Spots in Kidney Transplant Patients. Transplantation 2017, 101, 1727–1733. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Analyte | Precursor Ion (m/z) | Production (m/z) | Cone (V) | Collision (V) | Retention Time |
|---|---|---|---|---|---|
| TAC | 821.57 | 768.55 | 24 | 18 | 3.87 |
| TAC [13C,2H4] | 826.61 | 773.51 | 14 | 18 | 3.87 |
| MPA | 321.27 | 207.15 | 10 | 22 | 3.29 |
| MPA-d3 | 324.26 | 210.15 | 8 | 22 | 3.29 |
| Cre | 114.20 | 86.13 | 44 | 10 | 0.85 |
| Cre-d3 | 117.27 | 47.20 | 38 | 14 | 0.85 |
| Day 1 | Day 2 | Day 3 | Interbatch CV (%) | |||||
|---|---|---|---|---|---|---|---|---|
| Mean Deviation (%) | CV (%) | Mean Deviation (%) | CV (%) | Mean Deviation (%) | CV (%) | |||
| TAC | LLOQ (0.50) | −6.64 | 7.74 | 0.68 | 5.30 | −3.12 | 5.24 | 6.52 |
| (ng/mL) | LQC (1.50) | 1.79 | 5.18 | 0.94 | 4.39 | 2.71 | 2.77 | 3.98 |
| MQC (20.00) | 9.10 | 2.47 | 10.52 | 2.52 | 11.87 | 2.03 | 2.42 | |
| HQC (40.00) | 5.38 | 4.53 | 8.76 | 4.27 | 9.46 | 3.40 | 4.15 | |
| MPA | LLOQ (0.025) | −8.00 | 4.35 | −11.20 | 2.01 | −11.20 | 3.96 | 3.66 |
| (μg/mL) | LQC (0.075) | −0.64 | 3.18 | −4.33 | 4.19 | −5.52 | 1.82 | 3.72 |
| MQC (0.50) | −7.16 | 4.12 | −8.00 | 4.95 | −8.92 | 5.50 | 4.59 | |
| HQC (1.00) | −11.54 | 1.42 | −12.56 | 1.97 | −12.66 | 1.10 | 1.55 | |
| CRE | LLOQ (10.00) | 7.27 | 5.33 | 6.02 | 4.80 | 1.51 | 5.57 | 5.42 |
| (nmol/mL) | LQC (30.00) | 1.68 | 5.21 | 5.28 | 6.86 | −1.17 | 3.08 | 5.64 |
| MQC (400.00) | −0.54 | 5.30 | −1.46 | 4.59 | −2.15 | 4.53 | 4.52 | |
| HQC (800.00) | −3.26 | 2.82 | −6.07 | 3.19 | −7.02 | 3.03 | 3.29 | |
| Recovery Rate (%) | Process Efficiency (%) | |||||
|---|---|---|---|---|---|---|
| Analytes | LQC | MQC | HQC | LQC | MQC | HQC |
| TAC | 96.49 | 105.89 | 99.21 | 104.43 | 109.28 | 101.42 |
| MPA | 97.13 | 95.01 | 100.20 | 96.08 | 99.11 | 98.08 |
| CRE | 101.75 | 95.09 | 96.26 | 96.65 | 95.88 | 98.62 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Dai, X.; Wan, S.; Fan, Y.; Wu, L.; Xu, H.; Yan, L.; Gong, X.; Li, Y.; Luo, Y.; et al. A Volumetric Absorptive Microsampling UPLC-MS/MS Method for Simultaneous Quantification of Tacrolimus, Mycophenolic Acid and Creatinine in Whole Blood of Renal Transplant Recipients. Pharmaceutics 2022, 14, 2547. https://doi.org/10.3390/pharmaceutics14122547
Wang X, Dai X, Wan S, Fan Y, Wu L, Xu H, Yan L, Gong X, Li Y, Luo Y, et al. A Volumetric Absorptive Microsampling UPLC-MS/MS Method for Simultaneous Quantification of Tacrolimus, Mycophenolic Acid and Creatinine in Whole Blood of Renal Transplant Recipients. Pharmaceutics. 2022; 14(12):2547. https://doi.org/10.3390/pharmaceutics14122547
Chicago/Turabian StyleWang, Xueqiao, Xinhua Dai, Shiqi Wan, Yu Fan, Lijuan Wu, Huan Xu, Lin Yan, Xingxin Gong, Yamei Li, Yao Luo, and et al. 2022. "A Volumetric Absorptive Microsampling UPLC-MS/MS Method for Simultaneous Quantification of Tacrolimus, Mycophenolic Acid and Creatinine in Whole Blood of Renal Transplant Recipients" Pharmaceutics 14, no. 12: 2547. https://doi.org/10.3390/pharmaceutics14122547
APA StyleWang, X., Dai, X., Wan, S., Fan, Y., Wu, L., Xu, H., Yan, L., Gong, X., Li, Y., Luo, Y., Bai, Y., & Li, Y. (2022). A Volumetric Absorptive Microsampling UPLC-MS/MS Method for Simultaneous Quantification of Tacrolimus, Mycophenolic Acid and Creatinine in Whole Blood of Renal Transplant Recipients. Pharmaceutics, 14(12), 2547. https://doi.org/10.3390/pharmaceutics14122547