Abstract
For many years, the use of probiotics in periodontitis treatment was reflected in their abilities to control the immune response of the host to the presence of pathogenic microorganisms and to upset periodontopathogens. Accordingly, the aim of the present study was to assess the use of probiotics as adjuvant therapy on clinical periodontal parameters throughout a systematic review and meta-analysis. The literature was screened, up to 4 June 2021, by two independent reviewers (L.H. and R.B.) in four electronic databases: PubMed (MedLine), ISI Web of Science, Scielo, and Scopus. Only clinical trials that report the effect of the use of probiotics as adjuvants in the treatment of periodontal disease were included. Comparisons were carried out using Review Manager Software version 5.3.5 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). A total of 21 studies were considered for the meta-analysis. For the index plaque, the use of probiotics did not improve this clinical parameter (p = 0.16). On the other hand, for the periodontal pocket depth, the clinical attachment loss, the bleeding on probing, and the use of probiotics as adjuvant therapy resulted in an improvement of these parameters, since the control group achieved statistically higher values of this parameter (p < 0.001; p < 0.001; and p = 0.005, respectively). This study suggests that the use of probiotics led to an improvement in periodontal pocket depth, clinical attachment loss, and bleeding on probing parameters. On the other hand, this protocol seems to not be beneficial for the index plaque parameter.
1. Introduction
The first trigger of periodontal disease is the accumulation of dental plaque due to poor oral hygiene [1]. According to this, it is defined as inflammatory conditions that affect tissues of the teeth, which leads to the formation of pockets, gingival recession, and therefore, there is attachment loss and bone loss [2]. The etiology of periodontal disease is associated with bacterial plaque and considers three important factors that will determine whether the disease develops; these factors are: a susceptible host, the presence of pathogenic species, and the reduction or absence of beneficial bacteria [3]. Additionally, the role of other microorganisms should be highlighted, such as fungal species, which may act as a cofactor inducing the production of pro-inflammatory cytokines and favoring the occurrence of periodontal attachment loss [4,5]. Epidemiological studies show that periodontal disease and gingivitis represent a serious public health problem that can lead to systemic diseases such as diabetes and cardiovascular diseases. Consequently, the prevention and treatment of periodontitis is crucial not only for dental maintenance and oral health but also for general health [6].
Scaling and root planning is a non-surgical treatment that removes the tartar from the crown and the root surfaces of the teeth and thus leads the reduction of the microorganisms load [7]. Scaling and root planning is the treatment considered as the gold standard, and this type of treatment has been shown to reduce the bacterial load and eliminate plaque and tartar. Supportive treatments for scaling and root planning include systemic and local antibiotics, local drug delivery, host modulation therapy, lasers, and other novel methods [8].
For many years, probiotics have been used in general medicine for the treatment of inflammatory bowel diseases and vaginal infections and for the prevention of allergies and respiratory infections [9]. In dentistry, the probiotics might prevent or treat oral diseases such as caries, gingivitis, or periodontitis [10]. Commonly used probiotics in dentistry are Bifidobacterium and Lactobacillus [11]. There is evidence that the use of a probiotic yogurt supplemented with Bifidobacterium animalis subsp. lactis (B. lactis) could have a positive effect on plaque buildup and gingival inflammation [1].
Probiotics are living microorganisms. When they are directed in correct amounts, they provide a benefit for the health of the host. Therefore, the probiotics strengthen the immune system and act against allergies, stress, and toxic substances [11]. It has been revealed that the use of probiotics (Lactobacillus reuteri) has diminished gingival bleeding and has also led to a decrease in gingivitis. On the other hand, oral administration of the probiotic Lactobacillus salivarius perfected the periodontal status of healthy volunteers, especially for smokers, except non-smoking volunteers (never/ex-smokers) [12].
Although the use of probiotics seems to be beneficial, the question of whether the use of this adjunct therapy could improve the periodontal disease remains. Hence, the objective of this study is to systematically review the literature to evaluate the use of probiotics as adjuvant therapy on clinical periodontal parameters. The null hypothesis to be tested is that the use of probiotics as adjuvant therapy will not have any influence on clinical periodontal parameters.
2. Materials and Methods
This systematic review and meta-analysis was performed in accordance with the PRISMA guidelines [13]. The following PICOS framework was used: population, periodontal disease; intervention, scaling, and root debridement plus the application of probiotics as adjuvant therapy; control, scaling, and root debridement only; outcome, clinical periodontal parameters; and study design, randomized clinical trials. The research question was: “Does the use of probiotics as adjuvant therapy for scaling and root debridement improve the clinical periodontal parameters?”.
2.1. Literature Search
The literature search was conducted by two independent reviewers up to June 04, 2021. No data limit was used for the search. Four electronic databases, PubMed (MedLine), ISI Web of Science, Scielo, and Scopus, were screened to identify manuscripts that could be included. The keywords and search strategy used in PubMed and adapted for other databases are listed in Table 1. The reviewers also performed a hand search of the reference lists of included articles for the identification of additional papers. Following the initial screening, all studies were imported into Mendeley Desktop 1.17.11 software (London, UK) to eliminate duplicates.

Table 1.
Keywords used in search strategy.
2.2. Study Selection
Two reviewers (L.H. and R.B.) individually assessed the titles and abstracts of all studies. Manuscripts for full-text review were selected according to the following eligibility criteria: (1) reported the effect of the use of probiotics as adjuvants in the treatment of periodontal disease; (2) included a control group where only scaling and root debridement was performed; (3) measured periodontal clinical parameters; (4) presented the data in mean and standard deviation; (5) published in the English, Spanish, or Portuguese language. Case reports, pilot studies, case series, and reviews were also excluded. Full copies of all of the potentially relevant studies were assessed. Papers that seemed to meet the inclusion criteria or had insufficient data in the title and abstract to produce a clear decision were designated for full analysis. The full-text manuscripts were considered independently in duplicate by two review authors. Any discrepancy concerning the eligibility of the included studies was decided and resolved through discussion and agreement by a third reviewer (C.E.C.-S.). Only papers that satisfied the eligibility criteria listed were included.
2.3. Data Extraction
The data of concern from the involved studies were extracted using Microsoft Office Excel 2019 (Microsoft Corporation, Redmond, WA, USA). These data comprised the year of publication, study design, characteristics of the included patients, periodontal disease diagnosis, type of probiotics used, clinical parameters measured, follow-up, and main outcomes. If any information was missing, the corresponding authors of the included studies were notified twice via an e-mail to retrieve the missing data. If the authors did not respond within 2 weeks of the first contact, the missing information was not included.
2.4. Quality Assessment
The risk of bias of the selected articles was evaluated and classified according to the Cochrane risk of bias tool for randomized clinical trials [14]. They were assessed by two reviewers (R.B. and L.H.) according to the following items: selection bias (sequence generation, allocation concealment), performance and detection bias (blinding of operators or participants and personnel), bias due to incomplete data, reporting bias (selective reporting, unclear withdrawals, missing outcomes), and other bias (protocol record in CONSORT). Each domain was classified as having a low risk, unclear risk, or high risk of bias.
2.5. Statistical Analysis
Meta-analyses were performed using Review Manager Software version 5.3.5 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). The analyses were carried out using the random-effects model, and pooled-effect estimates were obtained by comparing the standardized mean difference between the periodontal clinical parameters obtained from the control and experimental groups. Subgroups were built according to the follow-up time evaluated. A p-value <0.05 was considered statistically significant. Statistical heterogeneity of the treatment effect among studies was assessed using the Cochran Q test and the inconsistency I2 test.
3. Results
3.1. Literature Search
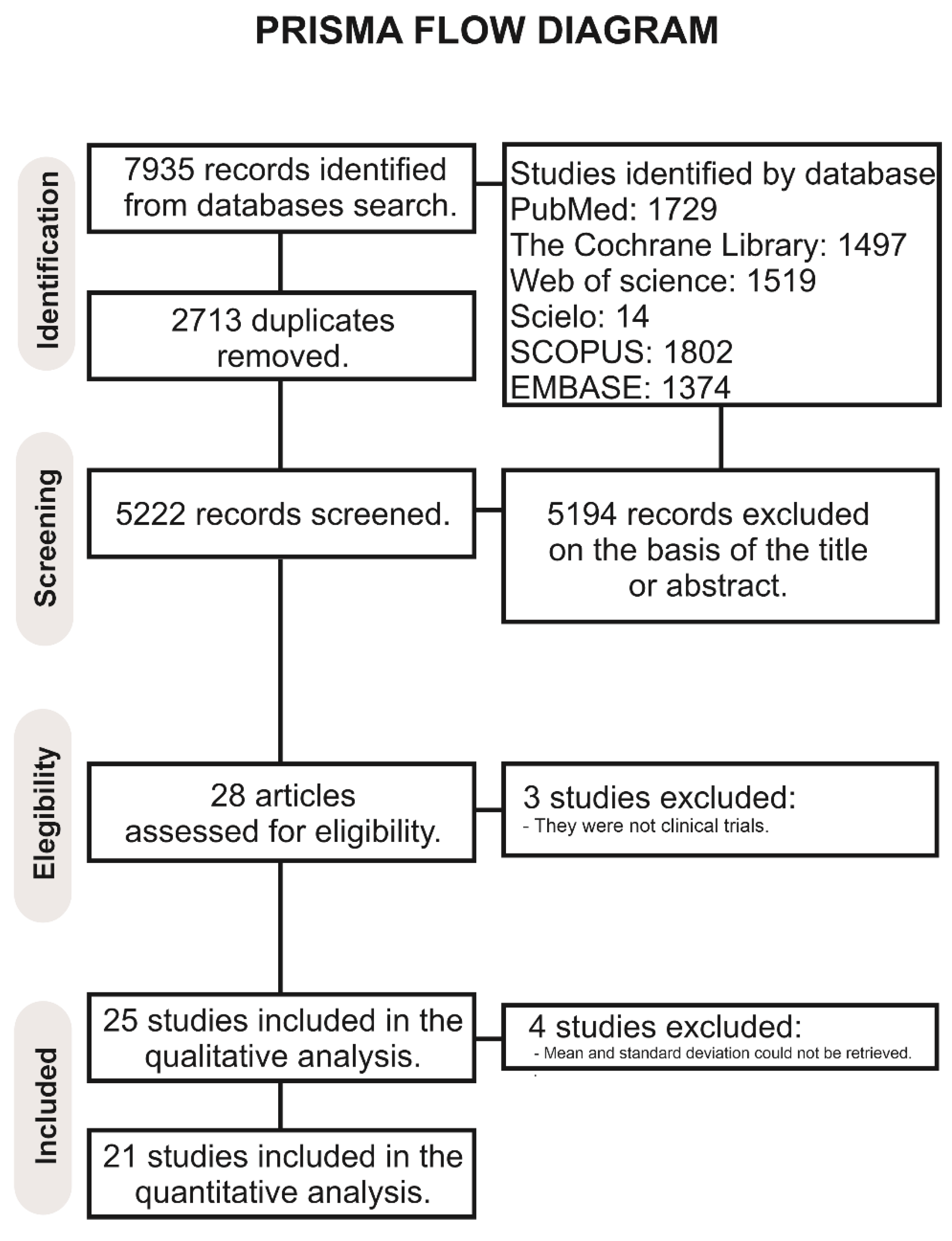
The search resulted in the retrieval of 7935 records (Figure 1). After removal of duplicates, 5222 articles were screened, and 5194 were excluded based on the eligibility criteria. A total of 28 full-text articles were assessed for eligibility. Of these, 3 were not considered for the qualitative analysis because they were not clinical trials, and 25 articles were included in the qualitative analysis [1,2,3,6,7,8,9,10,11,12,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29]. Of these, four studies [6,25,26,29] were excluded from the meta-analysis because the mean and standard deviation could not be retrieved. Finally, 21 studies were considered for the meta-analysis.
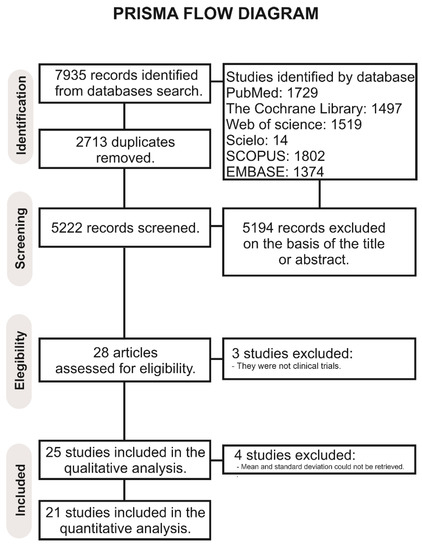
Figure 1.
PRISMA flowchart.
3.2. Qualitative/Descriptive Analysis
The characteristics of the studies included in the review are listed in Table 2. The studies included evaluated the performance of probiotics intake as adjuvant therapy from 4 weeks to a maximum follow-up time of 24 weeks. The probiotics tested included Lactobacillus brevis, Lactobacillus plantarum, Lactobacillus reuteri, Bifidobacterium animalis, Weissella cibaria, Lactobacillus salivarius, Lactobacillus rhamnosus, Lactobacillus rhamanosus, Lactobacillus brevis, Lactobacillus plantarum, Lactobacillus reuteri, and Bifidobacterium. Most of the included studies evaluated plaque index, bleeding on probing, probing pocket depth, and clinical attachment loss as clinical periodontal parameters.
Table 2.
Qualitative analysis of the included studies.
3.3. Risk of Bias of the Included Studies
When analyzing the risk of bias, most studies were not at a high risk of bias except for the parameter related to reporting bias and other bias (protocol recorded at CONSORT or ClinicalTrials). The selection, performance, and detection of bias due to incomplete data were those which presented a low risk of bias (Table 3).
Table 3.
Qualitative synthesis for clinical trials. (*: articles excluded from the meta-analysis).
3.4. Meta-Analysis
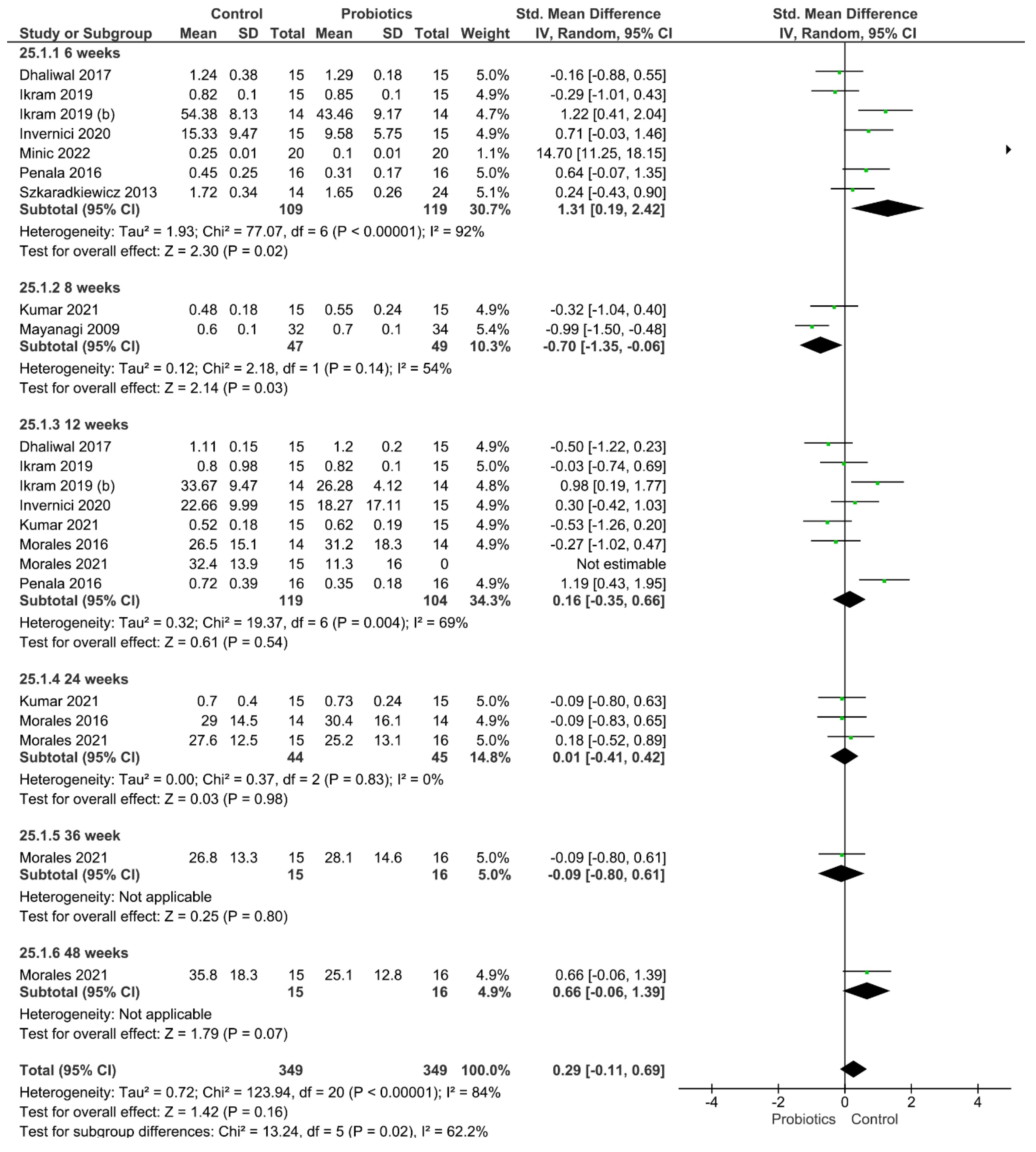
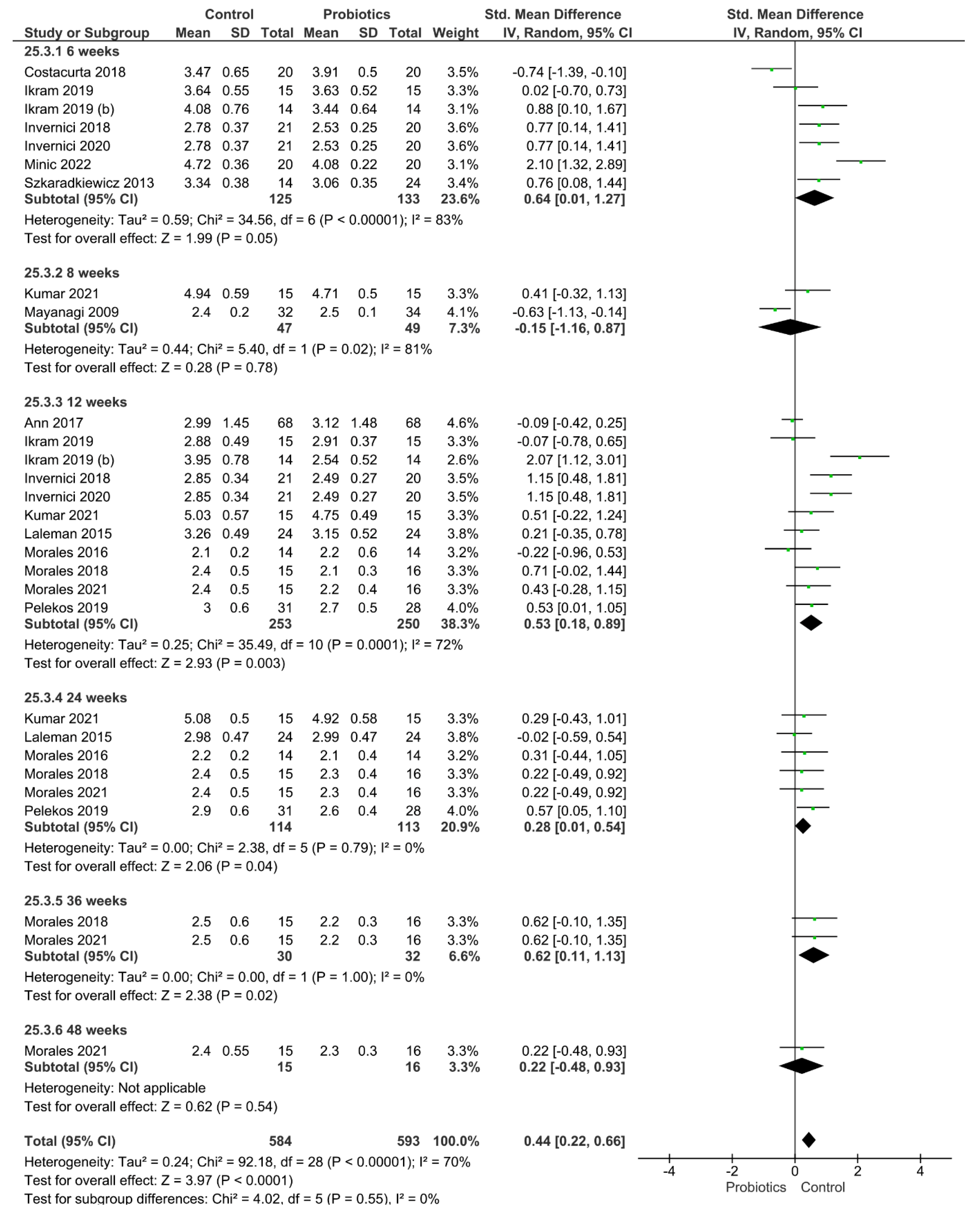
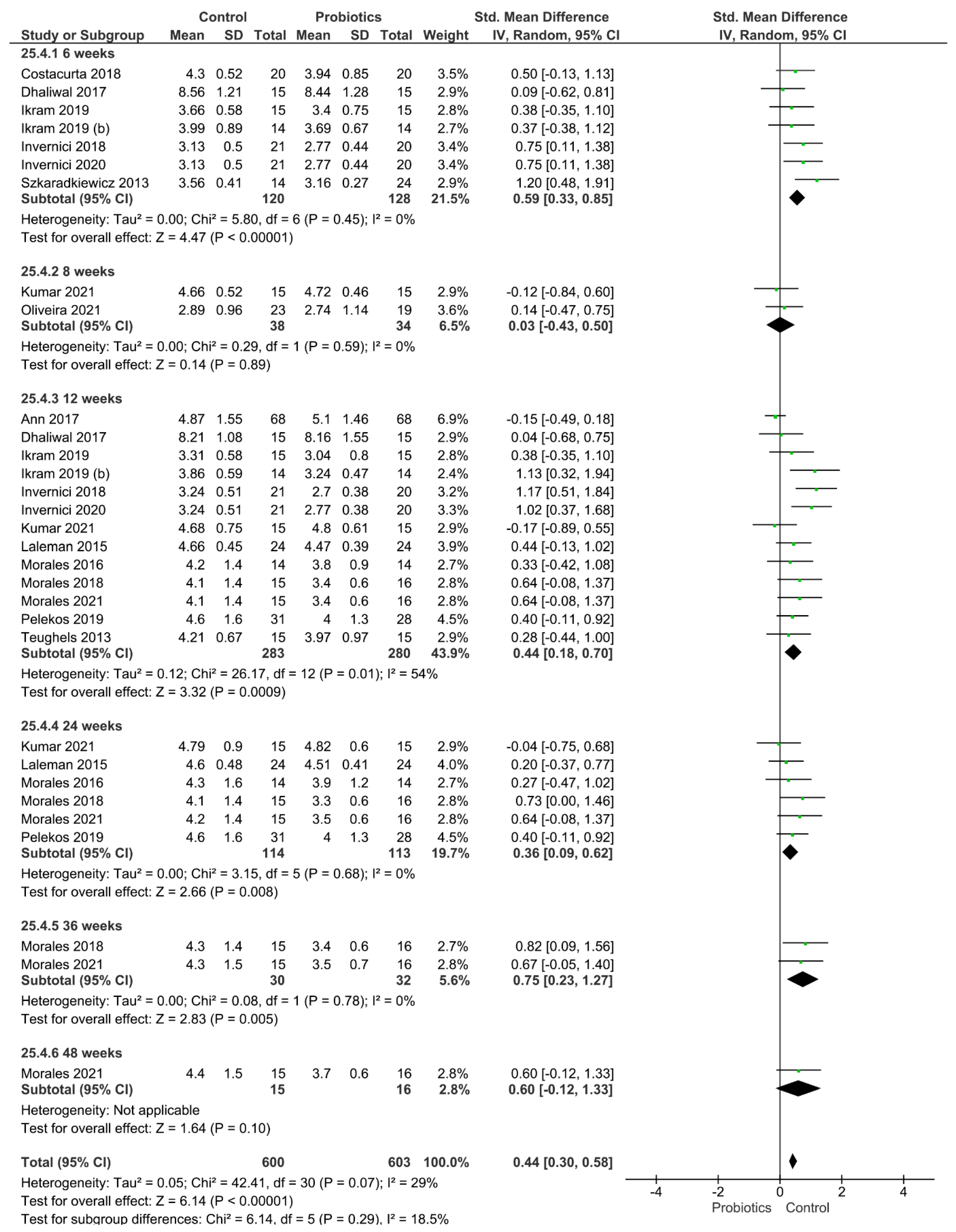
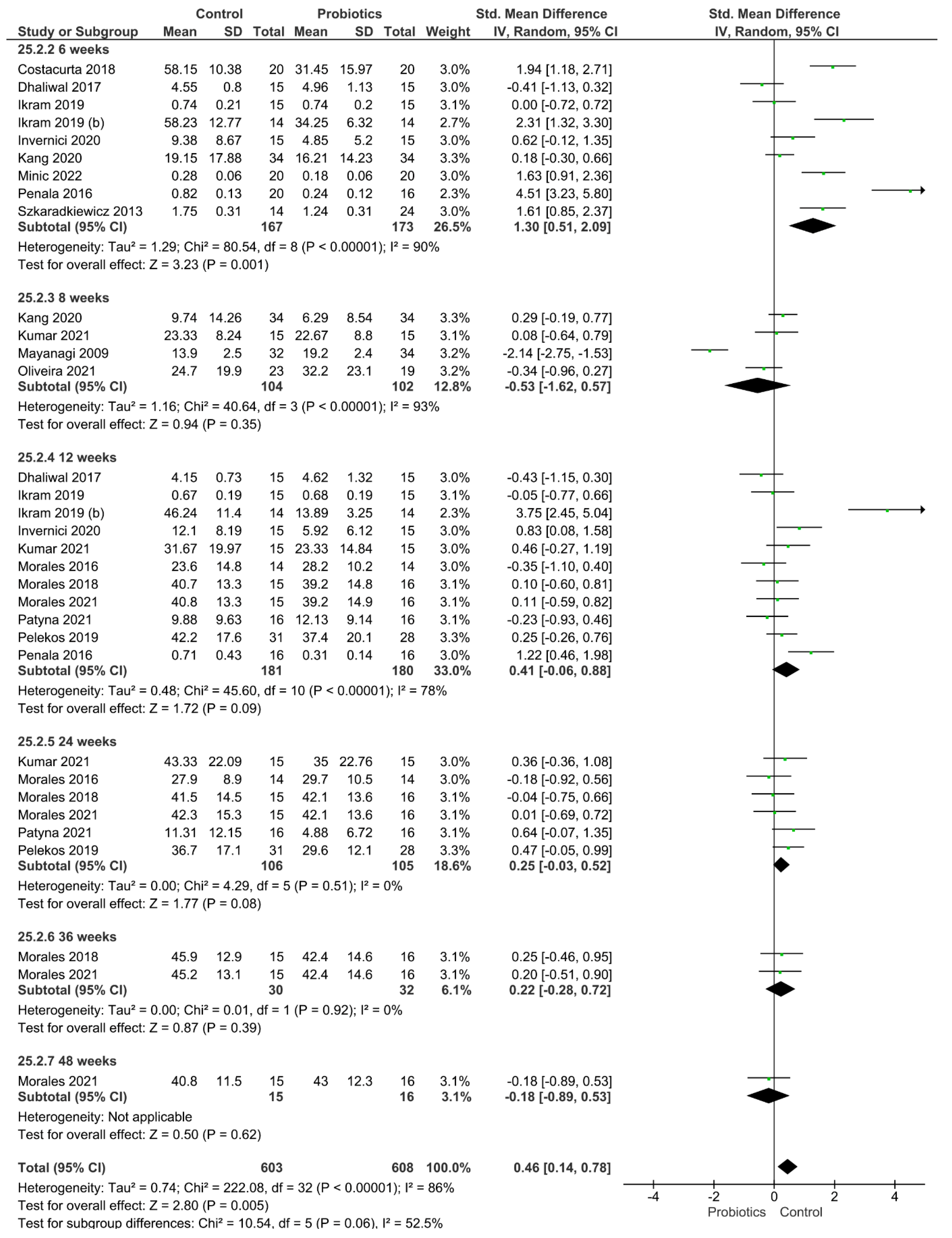
Four different clinical parameters were analyzed (Figure 2, Figure 3, Figure 4 and Figure 5). Figure 2 shows the results of the meta-analysis performed for the index plaque, where the use of probiotics did not improve this clinical parameter (p = 0.16). When evaluating the periodontal pocket depth, the use of probiotics as adjuvant therapy helped to improve this parameter, since the control group achieved statistically higher values of this parameter (p < 0.001; Figure 3). Figure 4 shows the result from the analysis of the clinical attachment loss parameter. Once again, the control group achieved statistically higher values of this parameter, meaning that the use of probiotics as adjuvant therapy resulted in an improvement (p < 0.001). Finally, bleeding on probing was also evaluated. The results favored the use of probiotics as adjuvant therapy, and the control group achieved statistically significant values for this clinical parameter (p = 0.005).
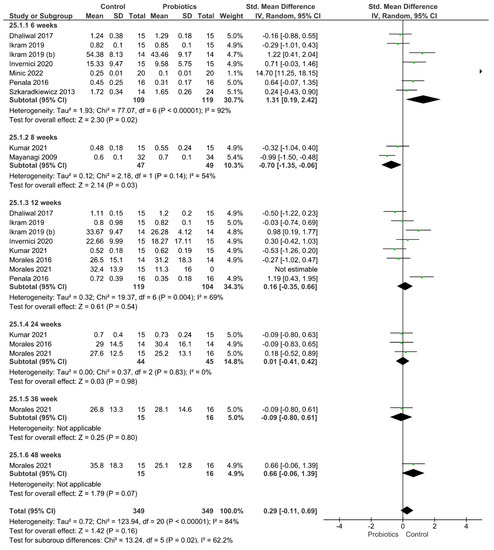
Figure 2.
Results from the meta-analysis for the index plaque clinical parameter.
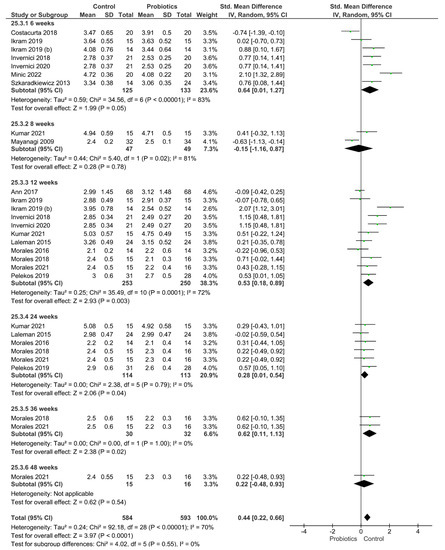
Figure 3.
Results from the meta-analysis for the periodontal pocket depth parameter.
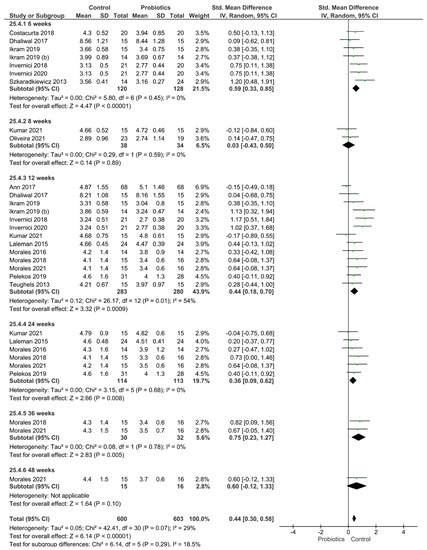
Figure 4.
Results from the meta-analysis for the clinical attachment loss parameter.
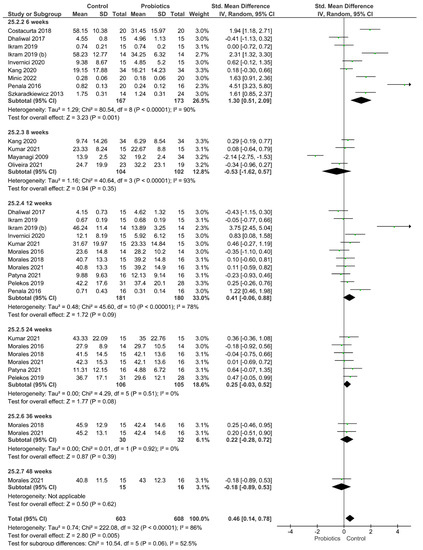
Figure 5.
Results from the meta-analysis for the bleeding on probing parameter.
4. Discussion
A systematic review and meta-analysis were conducted regarding the use of probiotics as adjuvant therapy on clinical periodontal parameters. Four different clinical parameters were analyzed. For index plaque, the use of probiotics did not improve this clinical parameter, while for the periodontal pocket depth, the clinical attachment loss, and the bleeding on probing, the use of probiotics as adjuvant therapy resulted in an improvement of these parameters. Accordingly, the null hypothesis tested in this study could be partially accepted.
According to the statistical analysis, the index plaque parameter was not improved by the use of probiotics. One should bear in mind that the first initiating mechanism in dental periodontal diseases is dental plaque accumulation. This could be the result of reduced oral hygiene [30]. Thus, maintaining the gingival health might prevent the rise of gingival crevicular fluid and, subsequently, the growth of proteins that act as a source of nutrients for periodontopathogens [1]. In fact, it has been determined that one favorable approach for the treatment and control of periodontal diseases is the modulating of the host inflammatory response, as it is distinct that certain principal pathogens are fascinated by inflammation. Consequently, controlling the inflammation is of supreme significance for dealing with the infection [31]. In this situation, a potential adjuvant therapy for preventing the gingival inflammation and the dental plaque accumulation could be achieved by using probiotics [32]. These live microorganisms might suppress harmful bacteria in oral health and lead to the reduction of plaque accumulation [33,34]. This conclusion did not match with the finding of this review, as probiotics did not play a role on the improvement of the index plaque parameter. This behavior may be due to the fact that dental plaque can be reduced only with proper oral hygiene, without the need for more specialized periodontal treatment [35].
For the periodontal pocket depth, the use of probiotics as adjuvant therapy improved this parameter. Ideally, when maintaining oral hygiene and using different probiotic strains, this resulted in lessening bacterial translocation through the pocket recuperation stage [8]. Additionally, the rationale behind the use of probiotics in periodontal therapy is converting the dysbiotic pocket microbiome to a symbiotic and beneficial microbiome [36,37]. Another explanation for the improvement in the periodontal pocket depth parameter could be found in the fact that probiotics have been probed to play a protective role in the gingival epithelial barrier by maintaining protein expression, thereby preventing mucous membrane apoptosis [38]. In addition to this, the improvement of this clinical parameter should take in account the supplementary role of the presence of the probiotics through various mechanisms such as the inhibition of the growth of pathogens, the inhibition of collagenases, and the reduction of inflammation associated molecules [3].
Regarding the clinical attachment loss parameter. Once again, the control group achieved statistically higher values of this parameter, meaning that the use of probiotics as adjuvant therapy resulted in an improvement of this parameter. The clinical attachment loss is a parameter used to assess the loss of periodontal tissue support in periodontitis [39]. In this sense, it is important to explain that pro-inflammatory cytokine response plays a significant role in the nonspecific response against bacterial and fungal pathogens, and this is considered a principal mediator of periodontal disease [40]. Some reports have explained that a decrease in the levels of TNF-a, IL-1b, and IL-17 in the periodontal pockets of patients with periodontitis is observed following the treatment with the probiotic strain of L Lactobacillus reuteri, which may carry clinical significance [41,42]. The decrease in the pro-inflammatory cytokine response in chronic periodontitis caused by the application of probiotics may explain the results obtained in this meta-analysis.
Finally, bleeding on probing was also evaluated, and the results also favored the use of probiotics as adjuvant therapy. Bleeding on probing is a primary parameter to set the threshold for gingivitis. The insertion of a probe to the bottom of the pocket elicits bleeding if the gingiva is inflamed and if the pocket epithelium is atrophic or ulcerated, which is believed to be mediated by subgingival pathogenic microorganisms [43]. Some studies [44,45] have demonstrated that the administration of probiotics is effective in the reduction of pathogens related to the periodontal disease, which can explain the results obtained in this review.
From this review, clinical evidence was assessed with regard to the use of probiotics as adjuvant therapy on clinical periodontal parameters. The outcomes should be considered with caution. Future research must be conducted, especially randomized controlled clinical trials, with the purpose of gaining a better understanding of the performance of probiotics in the improvement of the clinical and biochemical success of periodontal diseases. Moreover, a larger sample size with a longer follow-up should be employed in further studies. It needs to be mentioned that these findings should not be generalized, as probiotic agents were characterized by different concentrations and frequencies of application or other modes of administration. It is known that the selection of the “best” probiotic for oral health is still a controversial topic. Of interest, this study demonstrated that the use of probiotics seems to display beneficial outcomes when periodontal disease exists.
5. Conclusions
This study suggests that the use of probiotics leads to an improvement in some clinical parameters, including periodontal pocket depth, clinical attachment loss, and bleeding on probing. On the other hand, this protocol seems to be not beneficial for the index plaque parameter.
Author Contributions
Conceptualization, L.H., R.B. and C.E.C.-S.; methodology, L.H., R.B. and C.E.C.-S.; software, M.Z., L.H., R.B., M.N. and M.L.-S.; validation, L.H., R.B., P.M., C.E.C.-S., M.L.-S., F.L. and M.F.-R.; formal analysis, L.H., R.B., M.F.-R. and C.E.C.-S.; investigation, P.M., A.O.-C., M.N., L.H., R.B. and C.E.C.-S.; resources, A.O.-C., P.P.; M.F.-R., M.Z., N.J., R.B., L.H., P.M. and M.L.-S.; data curation, L.H., R.B. and C.E.C.-S.; writing—original draft preparation, L.H., R.B., C.E.C.-S., M.F.-R., A.O.-C. and M.L.-S.; writing—review and editing, F.L., L.H., C.E.C.-S. and M.L.-S.; visualization, N.J., M.N., P.P.; L.H., C.E.C.-S. and R.B.; supervision, L.H.; project administration, L.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Derived data supporting the findings of this study are available from the first author (L.H.) on request.
Acknowledgments
The authors Louis Hardan and Rim Bourgi would like to acknowledge the Saint- Joseph University of Beirut, Lebanon. The authors would also like to thank the University of Hidalgo State, Mexico, the University of Egas Moniz, Portugal, and the Medical University of Lodz, Poland, for supporting this research.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Invernici, M.M.; Furlaneto, F.A.; Salvador, S.L.; Ouwehand, A.C.; Salminen, S.; Mantziari, A.; Vinderola, G.; Ervolino, E.; Santana, S.I.; Silva, P.H.F.; et al. Bifidobacterium Animalis Subsp Lactis HN019 Presents Antimicrobial Potential against Periodontopathogens and Modulates the Immunological Response of Oral Mucosa in Periodontitis Patients. PLoS ONE 2020, 15, e0238425. [Google Scholar] [CrossRef]
- Ann, L.S.; Yin, G.C.; Fatimah, S.; En, N.S.; Dicksit, D.D.; Kalyan, C.; Muttalib, K.A. Effectiveness of Photodynamic Therapy and Probiotics as an Adjunct to Scaling and Root Debridement in the Treatment of Chronic Periodontitis. J. Pharm. Neg. Res. 2017, 8, 25. [Google Scholar]
- Dhaliwal, P.K.; Grover, V.; Malhotra, R.; Kapoor, A. Clinical and Microbiological Investigation of the Effects of Probiotics Combined with Scaling and Root Planing in the Management of Chronic Periodontitis: A Randomized, Controlled Study. J. Int. Acad. Periodontol. 2017, 19, 101–108. [Google Scholar]
- Andrade, J.C.; Kumar, S.; Kumar, A.; Černáková, L.; Rodrigues, C.F. Application of probiotics in candidiasis management. Crit. Rev. Food Sci. 2021, 22, 1–16. [Google Scholar] [CrossRef]
- Ribeiro, F.C.; Rossoni, R.D.; de Barros, P.P.; Santos, J.D.; Fugisaki, L.R.O.; Leão, M.P.V.; Junqueira, J.C. Action mechanisms of probiotics on Candida spp. and candidiasis prevention: An update. J. Appl. Microbiol. 2020, 129, 175–185. [Google Scholar] [CrossRef] [Green Version]
- Nędzi-Góra, M.; Wroblewska, M.; Gorska, R. The Effect of Lactobacillus Salivarius SGL03 on Clinical and Microbiological Parameters in Periodontal Patients. Pol. J. Microbiol. 2020, 69, 441. [Google Scholar] [CrossRef]
- Ikram, S.; Raffat, M.A.; Baig, S.; Ansari, S.A.; Borges, K.J.J.; Hassan, N. Clinical Efficacy of Probiotics as An Adjunct to Scaling and Root Planning in The Treatment Of Chronic Periodontitis. Ann. Abbasi Shaheed Hosp. Karachi Med. Dent. Coll. 2019, 24, 31–37. [Google Scholar]
- Kumar, V.; Singhal, R.; Rastogi, P.; Lal, N.; Pandey, S.; Mahdi, A.A. Localized Probiotic-Guided Pocket Recolonization in the Treatment of Chronic Periodontitis: A Randomized Controlled Clinical Trial. J. Periodontal Implant. Sci. 2021, 51, 199. [Google Scholar] [CrossRef]
- Minić, I.; Pejčić, A.; Bradić-Vasić, M. Effect of the Local Probiotics in the Therapy of Periodontitis A Randomized Prospective Study. Int. J. Dent. Hyg. 2022, 20, 401–407. [Google Scholar] [CrossRef]
- Kang, M.-S.; Lee, D.-S.; Lee, S.-A.; Kim, M.-S.; Nam, S.-H. Effects of Probiotic Bacterium Weissella Cibaria CMU on Periodontal Health and Microbiota: A Randomised, Double-Blind, Placebo-Controlled Trial. BMC Oral Health 2020, 20, 243. [Google Scholar] [CrossRef]
- Costacurta, M.; Sicuro, L.; Margiotta, S.; Ingrasciotta, I.; Docimo, R. Clinical Effects of Lactobacillus reuteri Probiotic in Treatment of Chronic Periodontitis. A Randomized, Controlled Trial. Oral Implantol. 2018, 11, 191–198. [Google Scholar]
- Mayanagi, G.; Kimura, M.; Nakaya, S.; Hirata, H.; Sakamoto, M.; Benno, Y.; Shimauchi, H. Probiotic Effects of Orally Administered Lactobacillus Salivarius WB21-containing Tablets on Periodontopathic Bacteria: A Double-blinded, Placebo-controlled, Randomized Clinical Trial. J. Clin. Periodontol. 2009, 36, 506–513. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Higgins, J.P.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Assessing Risk of Bias in a Randomized Trial. Cochrane Handb. Syst. Rev. Interv. 2019, 6, 205–228. [Google Scholar]
- Ikram, S.; Hassan, N.; Baig, S.; Borges, K.J.J.; Raffat, M.A.; Akram, Z. Effect of Local Probiotic (Lactobacillus reuteri) vs Systemic Antibiotic Therapy as an Adjunct to Non-surgical Periodontal Treatment in Chronic Periodontitis. J. Investig. Clin. Dent. 2019, 10, e12393. [Google Scholar] [CrossRef]
- Invernici, M.M.; Salvador, S.L.; Silva, P.H.; Soares, M.S.; Casarin, R.; Palioto, D.B.; Souza, S.L.S.; Taba, M., Jr.; Novaes, A.B., Jr.; Furlaneto, F.A.C.; et al. Effects of Bifidobacterium Probiotic on the Treatment of Chronic Periodontitis: A Randomized Clinical Trial. J. Clin. Periodontol. 2018, 45, 1198–1210. [Google Scholar] [CrossRef] [Green Version]
- Laleman, I.; Yilmaz, E.; Ozcelik, O.; Haytac, C.; Pauwels, M.; Herrero, E.R.; Slomka, V.; Quirynen, M.; Alkaya, B.; Teughels, W. The Effect of a Streptococci Containing Probiotic in Periodontal Therapy: A Randomized Controlled Trial. J. Clin. Periodontol. 2015, 42, 1032–1041. [Google Scholar] [CrossRef]
- Morales, A.; Gandolfo, A.; Bravo, J.; Carvajal, P.; Silva, N.; Godoy, C.; Garcia-Sesnich, J.; Hoare, A.; Diaz, P.; Gamonal, J. Microbiological and Clinical Effects of Probiotics and Antibiotics on Nonsurgical Treatment of Chronic Periodontitis: A Randomized Placebo-Controlled Trial with 9-Month Follow-Up. J. Appl. Oral Sci. 2018, 26, e20170075. [Google Scholar] [CrossRef]
- Morales, A.; Contador, R.; Bravo, J.; Carvajal, P.; Silva, N.; Strauss, F.-J.; Gamonal, J. Clinical Effects of Probiotic or Azithromycin as an Adjunct to Scaling and Root Planning in the Treatment of Stage III Periodontitis: A Pilot Randomized Controlled Clinical Trial. BMC Oral Health 2021, 21, 12. [Google Scholar] [CrossRef]
- Morales, A.; Galaz, C.; González, J.; Silva, N.; Hernández, M.; Godoy, C.; García-Sesnich, J.; Díaz, P.; Carvajal, P. Efecto Clínico Del Uso de Probiótico En El Tratamiento de La Periodontitis Crónica: Ensayo Clínico. Rev. Clínica Periodoncia Implantol. Rehabil. Oral. 2016, 9, 146–152. [Google Scholar] [CrossRef] [Green Version]
- de Oliveira, A.M.; Lourenço, T.G.B.; Colombo, A.P.V. Impact of Systemic Probiotics as Adjuncts to Subgingival Instrumentation on the Oral-gut Microbiota Associated with Periodontitis: A Randomized Controlled Clinical Trial. J. Periodontol. 2021, 93, 31–44. [Google Scholar] [CrossRef]
- Patyna, M.; Ehlers, V.; Bahlmann, B.; Kasaj, A. Effects of Adjunctive Light-Activated Disinfection and Probiotics on Clinical and Microbiological Parameters in Periodontal Treatment: A Randomized, Controlled, Clinical Pilot Study. Clin. Oral. Investig. 2021, 25, 3967–3975. [Google Scholar] [CrossRef]
- Pelekos, G.; Ho, S.N.; Acharya, A.; Leung, W.K.; McGrath, C. A Double-blind, Paralleled-arm, Placebo-controlled and Randomized Clinical Trial of the Effectiveness of Probiotics as an Adjunct in Periodontal Care. J. Clin. Periodontol. 2019, 46, 1217–1227. [Google Scholar] [CrossRef]
- Penala, S.; Kalakonda, B.; Pathakota, K.R.; Jayakumar, A.; Koppolu, P.; Lakshmi, B.V.; Pandey, R.; Mishra, A. Efficacy of Local Use of Probiotics as an Adjunct to Scaling and Root Planing in Chronic Periodontitis and Halitosis: A Randomized Controlled Trial. J. Res. Pharm. Pract. 2016, 5, 86. [Google Scholar] [CrossRef]
- Petrushanko, T.; Loban, G.; Moshel, T.; Hancho, O. Therapeutic Potential of Lactobacilli-Based Drug in the Treatment of Generalized Periodontitis. Ukr. Med. Stomatol. Acad. 2020, 16, 121–125. [Google Scholar] [CrossRef]
- Shimauchi, H.; Mayanagi, G.; Nakaya, S.; Minamibuchi, M.; Ito, Y.; Yamaki, K.; Hirata, H. Improvement of Periodontal Condition by Probiotics with Lactobacillus Salivarius WB21: A Randomized, Double-blind, Placebo-controlled Study. J. Clin. Periodontol. 2008, 35, 897–905. [Google Scholar] [CrossRef]
- Szkaradkiewicz, A.K.; Stopa, J.; Karpiński, T.M. Effect of Oral Administration Involving a Probiotic Strain of Lactobacillus reuteri on Pro-Inflammatory Cytokine Response in Patients with Chronic Periodontitis. Arch. Immunol. Ther. Exp. 2014, 62, 495–500. [Google Scholar] [CrossRef] [Green Version]
- Teughels, W.; Durukan, A.; Ozcelik, O.; Pauwels, M.; Quirynen, M.; Haytac, M.C. Clinical and Microbiological Effects of Lactobacillus reuteri Probiotics in the Treatment of Chronic Periodontitis: A Randomized Placebo-controlled Study. J. Clin. Periodontol. 2013, 40, 1025–1035. [Google Scholar] [CrossRef] [Green Version]
- Vivekananda, M.; Vandana, K.; Bhat, K. Effect of the Probiotic Lactobacilli reuteri (Prodentis) in the Management of Periodontal Disease: A Preliminary Randomized Clinical Trial. J. Oral. Microbiol. 2010, 2, 5344. [Google Scholar] [CrossRef]
- Marsh, P.D. Are Dental Diseases Examples of Ecological Catastrophes? Microbiology 2003, 149, 279–294. [Google Scholar] [CrossRef]
- Bartold, P.M.; Van Dyke, T.E. Host Modulation: Controlling the Inflammation to Control the Infection. Periodontol. 2000 2017, 75, 317–329. [Google Scholar] [CrossRef]
- Ganguly, N.; Bhattacharya, S.; Sesikeran, B.; Nair, G.; Ramakrishna, B.; Sachdev, H.; Batish, V.; Kanagasabapathy, A.; Muthuswamy, V.; Kathuria, S. ICMR-DBT Guidelines for Evaluation of Probiotics in Food. Indian J. Med. Res. 2011, 134, 22–25. [Google Scholar]
- Krasse, P.; Carlsson, B.; Dahl, C.; Paulsson, A.; Nilsson, A.; Sinkiewicz, G. Decreased Gum Bleeding and Reduced Gingivitis by the Probiotic Lactobacillus reuteri. Swed. Dent. J. 2006, 30, 55–60. [Google Scholar]
- Riccia, D.D.; Bizzini, F.; Perilli, M.; Polimeni, A.; Trinchieri, V.; Amicosante, G.; Cifone, M.G. Anti-inflammatory Effects of Lactobacillus Brevis (CD2) on Periodontal Disease. Oral Dis. 2007, 13, 376–385. [Google Scholar] [CrossRef]
- Van der Weijden, G.; Hioe, K. A Systematic Review of the Effectiveness of Self-performed Mechanical Plaque Removal in Adults with Gingivitis Using a Manual Toothbrush. J. Clin. Periodontol. 2005, 32, 214–228. [Google Scholar] [CrossRef]
- Boesten, R.J.; de Vos, W.M. Interactomics in the Human Intestine: Lactobacilli: And: Bifidobacteria: Make a Difference. J. Clin. Gastroenterol. 2008, 42, S163–S167. [Google Scholar] [CrossRef]
- Papadimitriou, K.; Zoumpopoulou, G.; Foligné, B.; Alexandraki, V.; Kazou, M.; Pot, B.; Tsakalidou, E. Discovering Probiotic Microorganisms: In Vitro, in Vivo, Genetic and Omics Approaches. Front. Microbiol. 2015, 6, 58. [Google Scholar] [CrossRef] [Green Version]
- Mennigen, R.; Nolte, K.; Rijcken, E.; Utech, M.; Loeffler, B.; Senninger, N.; Bruewer, M. Probiotic Mixture VSL# 3 Protects the Epithelial Barrier by Maintaining Tight Junction Protein Expression and Preventing Apoptosis in a Murine Model of Colitis. Am. J. Physiol.-Gastrointest. Liver Physiol. 2009, 296, G1140–G1149. [Google Scholar]
- Farook, F.F.; Alodwene, H.; Alharbi, R.; Alyami, M.; Alshahrani, A.; Almohammadi, D.; Alnasyan, B.; Aboelmaaty, W. Reliability Assessment between Clinical Attachment Loss and Alveolar Bone Level in Dental Radiographs. Clin. Exp. Dent. Res. 2020, 6, 596–601. [Google Scholar] [CrossRef]
- Kowalski, J.; Gorska, R.; Dragan, M.; Kozak, I. Clinical State of the Patients with Periodontitis, IL-1 Polymorphism and Pathogens in Periodontal Pocket--Is There a Link?(An Introductory Report). Adv. Med. Sci. 2006, 51, 9–12. [Google Scholar]
- Servin, A.L. Antagonistic Activities of Lactobacilli and Bifidobacteria against Microbial Pathogens. FEMS Microbiol. Rev. 2004, 28, 405–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vissers, Y.M.; Snel, J.; Zuurendonk, P.F.; Kleerebezem, M.; Wichers, H.J.; Savelkoul, H.F. Lactobacillus Strains Differentially Modulate Cytokine Production by HPBMC from Pollen-Allergic Patients. FEMS Immunol. Med. Microbiol. 2011, 61, 28–40. [Google Scholar] [CrossRef]
- Lang, N.P.; Joss, A.; Orsanic, T.; Gusberti, F.A.; Siegrist, B.E. Bleeding on Probing. A Predictor for the Progression of Periodontal Disease? J. Clin. Periodontol. 1986, 13, 590–596. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2021, 9, 69. [Google Scholar] [CrossRef]
- Alok, A.; Singh, I.D.; Singh, S.; Kishore, M.; Jha, P.C.; Iqubal, M.A. Probiotics: A New Era of Biotherapy. Adv. Biomed. Res. 2017, 6, 31. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).