

Does Cytokine-Release Syndrome Induced by CAR T-Cell Treatment Have an Impact on the Pharmacokinetics of Meropenem and Piperacillin/Tazobactam in Patients with Hematological Malignancies? Findings from an Observational Case-Control Study
 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
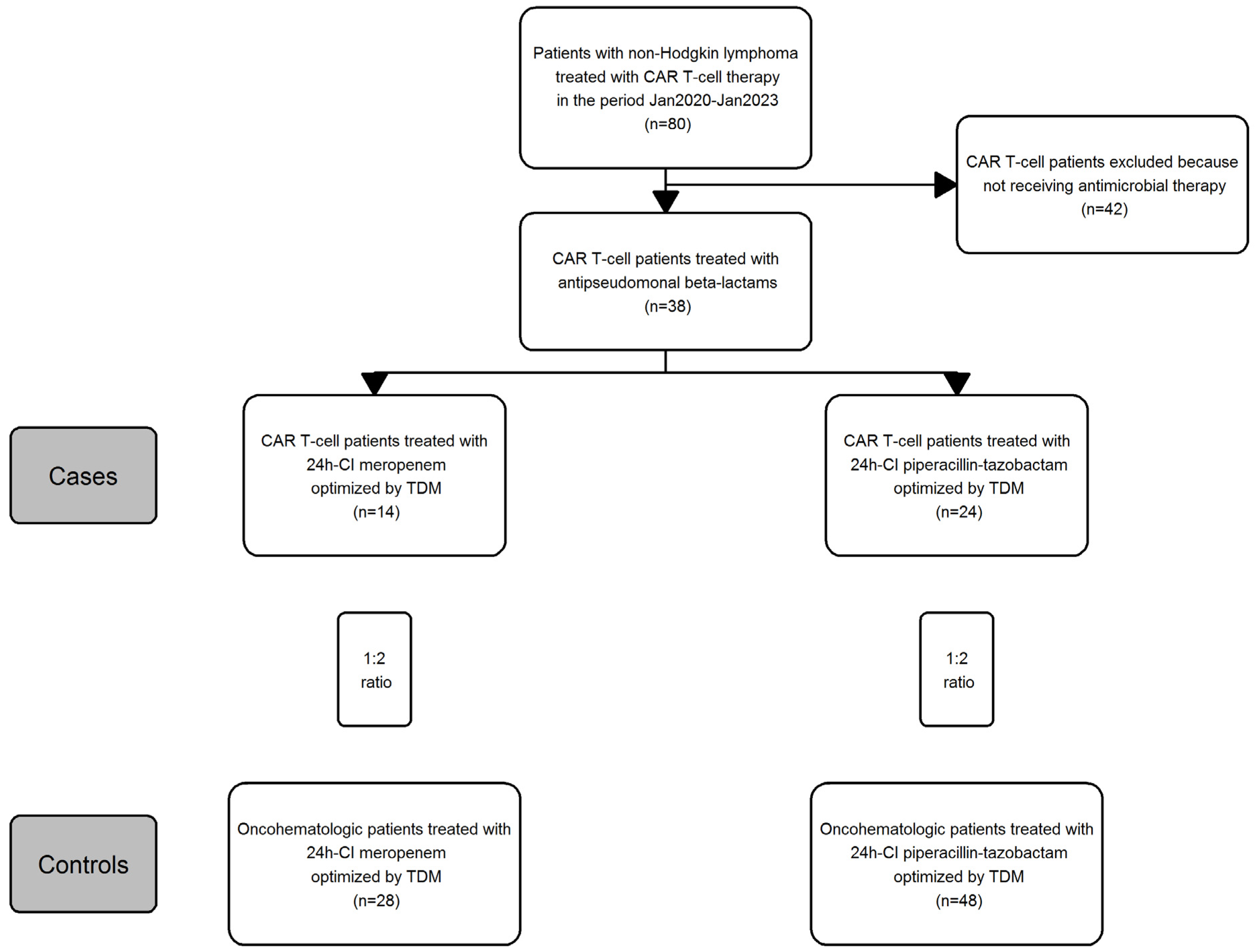
2.1. Study Design
2.2. Drug Analysis
2.2.1. Sample Pre-Treatment
2.2.2. Conditions of Liquid Chromatography and Mass Spectrometry
2.2.3. Calibration Curve and Quality Controls
2.2.4. Chemical and Reagents
2.2.5. Accuracy, Precision and Limit of Quantification
2.3. Patient Clinical Data and Pharmacokinetic Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hernandez-Lopez, A.; Tellez-Gonzalez, M.A.; Mondragon-Teran, P.; Meneses-Acosta, A. Chimeric Antigen Receptor-T Cells: A Pharmaceutical Scope. Front. Pharmacol. 2021, 12, 720692. [Google Scholar] [CrossRef]
- Roschewski, M.; Longo, D.L.; Wilson, W.H. CAR T-Cell Therapy for Large B-Cell Lymphoma—Who, When, and How? N. Engl. J. Med. 2022, 386, 692–696. [Google Scholar] [CrossRef]
- Teoh, P.J.; Chng, W.J. CAR T-cell therapy in multiple myeloma: More room for improvement. Blood Cancer J. 2021, 11, 84. [Google Scholar] [CrossRef] [PubMed]
- Hao, F.; Sholy, C.; Wang, C.; Cao, M.; Kang, X. The Role of T Cell Immunotherapy in Acute Myeloid Leukemia. Cells 2021, 10, 3376. [Google Scholar] [CrossRef] [PubMed]
- Fajgenbaum, D.C.; June, C.H. Cytokine Storm. N. Engl. J. Med. 2020, 383, 2255–2273. [Google Scholar] [CrossRef]
- Davila, M.L.; Riviere, I.; Wang, X.; Bartido, S.; Park, J.; Curran, K.; Chung, S.S.; Stefanski, J.; Borquez-Ojeda, O.; Olszewska, M.; et al. Efficacy and toxicity management of 19-28z CAR T cell therapy in B cell acute lymphoblastic leukemia. Sci. Transl. Med. 2014, 6, 224ra225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutgarts, V.; Jain, T.; Zheng, J.; Maloy, M.A.; Ruiz, J.D.; Pennisi, M.; Jaimes, E.A.; Perales, M.A.; Sathick, J. Acute Kidney Injury after CAR-T Cell Therapy: Low Incidence and Rapid Recovery. Biol. Blood Marrow Transplant. J. Am. Soc. Blood Marrow Transplant. 2020, 26, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Stewart, A.G.; Henden, A.S. Infectious complications of CAR T-cell therapy: A clinical update. Ther. Adv. Infect. Dis. 2021, 8, 20499361211036773. [Google Scholar] [CrossRef] [PubMed]
- Tumbarello, M.; Trecarichi, E.M.; Caira, M.; Candoni, A.; Pastore, D.; Cattaneo, C.; Fanci, R.; Nosari, A.; Spadea, A.; Busca, A.; et al. Derivation and validation of a scoring system to identify patients with bacteremia and hematological malignancies at higher risk for mortality. PLoS ONE 2012, 7, e51612. [Google Scholar] [CrossRef]
- Trecarichi, E.M.; Pagano, L.; Candoni, A.; Pastore, D.; Cattaneo, C.; Fanci, R.; Nosari, A.; Caira, M.; Spadea, A.; Busca, A.; et al. Current epidemiology and antimicrobial resistance data for bacterial bloodstream infections in patients with hematologic malignancies: An Italian multicentre prospective survey. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2015, 21, 337–343. [Google Scholar] [CrossRef] [Green Version]
- Heinz, W.J.; Buchheidt, D.; Christopeit, M.; von Lilienfeld-Toal, M.; Cornely, O.A.; Einsele, H.; Karthaus, M.; Link, H.; Mahlberg, R.; Neumann, S.; et al. Diagnosis and empirical treatment of fever of unknown origin (FUO) in adult neutropenic patients: Guidelines of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Medical Oncology (DGHO). Ann. Hematol. 2017, 96, 1775–1792. [Google Scholar] [CrossRef] [Green Version]
- Schmidt-Hieber, M.; Teschner, D.; Maschmeyer, G.; Schalk, E. Management of febrile neutropenia in the perspective of antimicrobial de-escalation and discontinuation. Expert Rev. Anti-Infect. Ther. 2019, 17, 983–995. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.A. Pharmacokinetic/pharmacodynamic parameters: Rationale for antibacterial dosing of mice and men. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 1998, 26, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Paul, S.K.; Akova, M.; Bassetti, M.; De Waele, J.J.; Dimopoulos, G.; Kaukonen, K.M.; Koulenti, D.; Martin, C.; Montravers, P.; et al. DALI: Defining antibiotic levels in intensive care unit patients: Are current beta-lactam antibiotic doses sufficient for critically ill patients? Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2014, 58, 1072–1083. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Pang, X.; Wu, X.; Shan, C.; Jiang, S. Clinical outcomes of prolonged infusion (extended infusion or continuous infusion) versus intermittent bolus of meropenem in severe infection: A meta-analysis. PLoS ONE 2018, 13, e0201667. [Google Scholar] [CrossRef] [PubMed]
- Cojutti, P.G.; Candoni, A.; Lazzarotto, D.; Fili, C.; Zannier, M.; Fanin, R.; Pea, F. Population Pharmacokinetics of Continuous-Infusion Meropenem in Febrile Neutropenic Patients with Hematologic Malignancies: Dosing Strategies for Optimizing Empirical Treatment against Enterobacterales and P. aeruginosa. Pharmaceutics 2020, 12, 785. [Google Scholar] [CrossRef]
- Cojutti, P.G.; Morandin, E.; Baraldo, M.; Pea, F. Population pharmacokinetics of continuous infusion of piperacillin/tazobactam in very elderly hospitalized patients and considerations for target attainment against Enterobacterales and Pseudomonas aeruginosa. Int. J. Antimicrob. Agents 2021, 58, 106408. [Google Scholar] [CrossRef]
- Gatti, M.; Cojutti, P.G.; Bartoletti, M.; Tonetti, T.; Bianchini, A.; Ramirez, S.; Pizzilli, G.; Ambretti, S.; Giannella, M.; Mancini, R.; et al. Expert clinical pharmacological advice may make an antimicrobial TDM program for emerging candidates more clinically useful in tailoring therapy of critically ill patients. Crit. Care 2022, 26, 178. [Google Scholar] [CrossRef]
- Gatti, M.; Cojutti, P.G.; Pascale, R.; Tonetti, T.; Laici, C.; Dell’Olio, A.; Siniscalchi, A.; Giannella, M.; Viale, P.; Pea, F. Assessment of a PK/PD Target of Continuous Infusion Beta-Lactams Useful for Preventing Microbiological Failure and/or Resistance Development in Critically Ill Patients Affected by Documented Gram-Negative Infections. Antibiotics 2021, 10, 1311. [Google Scholar] [CrossRef]
- Cojutti, P.G.; Gatti, M.; Rinaldi, M.; Tonetti, T.; Laici, C.; Mega, C.; Siniscalchi, A.; Giannella, M.; Viale, P.; Pea, F. Impact of Maximizing Css/MIC Ratio on Efficacy of Continuous Infusion Meropenem Against Documented Gram-Negative Infections in Critically Ill Patients and Population Pharmacokinetic/Pharmacodynamic Analysis to Support Treatment Optimization. Front. Pharmacol. 2021, 12, 781892. [Google Scholar] [CrossRef] [PubMed]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 11.0. 2021. Available online: http://www.eucast.org (accessed on 24 February 2023).
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Santomasso, B.; Bachier, C.; Westin, J.; Rezvani, K.; Shpall, E.J. The Other Side of CAR T-Cell Therapy: Cytokine Release Syndrome, Neurologic Toxicity, and Financial Burden. Am. Soc. Clin. Oncol. Educ. Book. Am. Soc. Clin. Oncol. Annu. Meet. 2019, 39, 433–444. [Google Scholar] [CrossRef] [PubMed]
- Neelapu, S.S.; Locke, F.L.; Bartlett, N.L.; Lekakis, L.J.; Miklos, D.B.; Jacobson, C.A.; Braunschweig, I.; Oluwole, O.O.; Siddiqi, T.; Lin, Y.; et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N. Engl. J. Med. 2017, 377, 2531–2544. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, M.C.; Lu, X.; Huang, Y.; Lin, X.; Mahmood, I.; Przepiorka, D.; Gavin, D.; Lee, S.; Liu, K.; George, B.; et al. FDA Approval Summary: Tisagenlecleucel for Treatment of Patients with Relapsed or Refractory B-cell Precursor Acute Lymphoblastic Leukemia. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2019, 25, 1142–1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, R.; Zhao, H.; Wang, Y.; Chen, Y.; Cai, H.; Hu, Y.; Wei, G.; Huang, H. Clinical characterization and risk factors associated with cytokine release syndrome induced by COVID-19 and chimeric antigen receptor T-cell therapy. Bone Marrow Transplant. 2021, 56, 570–580. [Google Scholar] [CrossRef]
- Kang, L.; Tang, X.; Zhang, J.; Li, M.; Xu, N.; Qi, W.; Tan, J.; Lou, X.; Yu, Z.; Sun, J.; et al. Interleukin-6-knockdown of chimeric antigen receptor-modified T cells significantly reduces IL-6 release from monocytes. Exp. Hematol. Oncol. 2020, 9, 11. [Google Scholar] [CrossRef] [PubMed]
- Cojutti, P.G.; Londero, A.; Della Siega, P.; Givone, F.; Fabris, M.; Biasizzo, J.; Tascini, C.; Pea, F. Comparative Population Pharmacokinetics of Darunavir in SARS-CoV-2 Patients vs. HIV Patients: The Role of Interleukin-6. Clin. Pharmacokinet. 2020, 59, 1251–1260. [Google Scholar] [CrossRef]
- Machavaram, K.K.; Almond, L.M.; Rostami-Hodjegan, A.; Gardner, I.; Jamei, M.; Tay, S.; Wong, S.; Joshi, A.; Kenny, J.R. A physiologically based pharmacokinetic modeling approach to predict disease-drug interactions: Suppression of CYP3A by IL-6. Clin. Pharmacol. Ther. 2013, 94, 260–268. [Google Scholar] [CrossRef]
- Kanduri, S.R.; Cheungpasitporn, W.; Thongprayoon, C.; Petnak, T.; Lin, Y.; Kovvuru, K.; Manohar, S.; Kashani, K.; Herrmann, S.M. Systematic Review of Risk factors and Incidence of Acute Kidney Injury Among Patients Treated with CAR-T Cell Therapies. Kidney Int. Rep. 2021, 6, 1416–1422. [Google Scholar] [CrossRef]
- Gupta, S.; Seethapathy, H.; Strohbehn, I.A.; Frigault, M.J.; O’Donnell, E.K.; Jacobson, C.A.; Motwani, S.S.; Parikh, S.M.; Curhan, G.C.; Reynolds, K.L.; et al. Acute Kidney Injury and Electrolyte Abnormalities After Chimeric Antigen Receptor T-Cell (CAR-T) Therapy for Diffuse Large B-Cell Lymphoma. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2020, 76, 63–71. [Google Scholar] [CrossRef]
- Nechemia-Arbely, Y.; Barkan, D.; Pizov, G.; Shriki, A.; Rose-John, S.; Galun, E.; Axelrod, J.H. IL-6/IL-6R axis plays a critical role in acute kidney injury. J. Am. Soc. Nephrol. JASN 2008, 19, 1106–1115. [Google Scholar] [CrossRef] [Green Version]
- Su, H.; Lei, C.T.; Zhang, C. Interleukin-6 Signaling Pathway and Its Role in Kidney Disease: An Update. Front. Immunol. 2017, 8, 405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimazui, T.; Nakada, T.A.; Tateishi, Y.; Oshima, T.; Aizimu, T.; Oda, S. Association between serum levels of interleukin-6 on ICU admission and subsequent outcomes in critically ill patients with acute kidney injury. BMC Nephrol. 2019, 20, 74. [Google Scholar] [CrossRef] [Green Version]
- Pai, M.P.; Cojutti, P.; Pea, F. Pharmacokinetics and pharmacodynamics of continuous infusion meropenem in overweight, obese, and morbidly obese patients with stable and unstable kidney function: A step toward dose optimization for the treatment of severe gram-negative bacterial infections. Clin. Pharmacokinet. 2015, 54, 933–941. [Google Scholar] [CrossRef]
- Kees, M.G.; Minichmayr, I.K.; Moritz, S.; Beck, S.; Wicha, S.G.; Kees, F.; Kloft, C.; Steinke, T. Population pharmacokinetics of meropenem during continuous infusion in surgical ICU patients. J. Clin. Pharmacol. 2016, 56, 307–315. [Google Scholar] [CrossRef]
- Usman, M.; Frey, O.R.; Hempel, G. Population pharmacokinetics of meropenem in elderly patients: Dosing simulations based on renal function. Eur. J. Clin. Pharmacol. 2017, 73, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Minichmayr, I.K.; Roberts, J.A.; Frey, O.R.; Roehr, A.C.; Kloft, C.; Brinkmann, A. Development of a dosing nomogram for continuous-infusion meropenem in critically ill patients based on a validated population pharmacokinetic model. J. Antimicrob. Chemother. 2018, 73, 1330–1339. [Google Scholar] [CrossRef] [PubMed]
- Dhaese, S.A.M.; Farkas, A.; Colin, P.; Lipman, J.; Stove, V.; Verstraete, A.G.; Roberts, J.A.; De Waele, J.J. Population pharmacokinetics and evaluation of the predictive performance of pharmacokinetic models in critically ill patients receiving continuous infusion meropenem: A comparison of eight pharmacokinetic models. J. Antimicrob. Chemother. 2019, 74, 432–441. [Google Scholar] [CrossRef]
- Li, C.; Kuti, J.L.; Nightingale, C.H.; Mansfield, D.L.; Dana, A.; Nicolau, D.P. Population pharmacokinetics and pharmacodynamics of piperacillin/tazobactam in patients with complicated intra-abdominal infection. J. Antimicrob. Chemother. 2005, 56, 388–395. [Google Scholar] [CrossRef]
- Dhaese, S.A.M.; Roberts, J.A.; Carlier, M.; Verstraete, A.G.; Stove, V.; De Waele, J.J. Population pharmacokinetics of continuous infusion of piperacillin in critically ill patients. Int. J. Antimicrob. Agents 2018, 51, 594–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, D.C.; Frey, O.; Rohr, A.; Roberts, J.A.; Koberer, A.; Fuchs, T.; Papadimas, N.; Heinzel-Gutenbrunner, M.; Brenner, T.; Lichtenstern, C.; et al. Therapeutic drug monitoring-guided continuous infusion of piperacillin/tazobactam significantly improves pharmacokinetic target attainment in critically ill patients: A retrospective analysis of four years of clinical experience. Infection 2019, 47, 1001–1011. [Google Scholar] [CrossRef] [Green Version]
- Trosi, C.; Cojutti, P.; Rinaldi, M.; Laici, C.; Siniscalchi, A.; Viale, P.; Pea, F. Measuring Creatinine Clearance Is the Most AccurateWay for Calculating the Proper Continuous Infusion Meropenem Dose for Empirical Treatment of Severe Gram-Negative Infections among Critically Ill Patients. Pharmaceutics 2023, 15, 551. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Liu, Y.; Li, L.; Ding, Y.; Qian, J.; Jiao, Z. Interactions Between Meropenem and Renal Drug Transporters. Curr. Drug Metab. 2022, 23, 423–431. [Google Scholar] [CrossRef]
- Daenen, S.; Erjavec, Z.; Uges, D.R.; De Vries-Hospers, H.G.; De Jonge, P.; Halie, M.R. Continuous infusion of ceftazidime in febrile neutropenic patients with acute myeloid leukemia. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 1995, 14, 188–192. [Google Scholar] [CrossRef]
- Cojutti, P.G.; Candoni, A.; Ramos-Martin, V.; Lazzarotto, D.; Zannier, M.E.; Fanin, R.; Hope, W.; Pea, F. Population pharmacokinetics and dosing considerations for the use of daptomycin in adult patients with haematological malignancies. J. Antimicrob. Chemother. 2017, 72, 2342–2350. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Aziz, M.H.; Alffenaar, J.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.A.; Pea, F.; Sjovall, F.; et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: A Position Paper. Intensive Care Med. 2020, 46, 1127–1153. [Google Scholar] [CrossRef] [PubMed]
- Hirai, K.; Ishii, H.; Shimoshikiryo, T.; Shimomura, T.; Tsuji, D.; Inoue, K.; Kadoiri, T.; Itoh, K. Augmented Renal Clearance in Patients With Febrile Neutropenia is Associated With Increased Risk for Subtherapeutic Concentrations of Vancomycin. Ther. Drug Monit. 2016, 38, 706–710. [Google Scholar] [CrossRef] [PubMed]
- Gijsen, M.; Wilmer, A.; Meyfroidt, G.; Wauters, J.; Spriet, I. Can augmented renal clearance be detected using estimators of glomerular filtration rate? Crit. Care 2020, 24, 359. [Google Scholar] [CrossRef]
- Declercq, P.; Gijsen, M.; Meijers, B.; Schetz, M.; Nijs, S.; D’Hoore, A.; Wauters, J.; Spriet, I. Reliability of serum creatinine-based formulae estimating renal function in non-critically ill surgery patients: Focus on augmented renal clearance. J. Clin. Pharm. Ther. 2018, 43, 695–706. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Variable | CAR T-Cell Treated Patients | Oncohematological Patients | p-Value | |
|---|---|---|---|---|
| Number of patients (n) | 14 | 28 | - | |
| Age (year) | 61.5 (49–65) | 62.5 (55–69.5) | 0.371 | |
| Gender (male/female) | 9/5 | 21/7 | 0.491 | |
| Weight (kg) | 88.8 (71.0–97.0) | 73.4 (63.0–80.0) | 0.016 | |
| Height (m) | 1.75 (1.64–1.80) | 1.70 (1.64–1.75) | 0.926 | |
| Creatinine (mg/dL) | 1.08 (0.85–1.31) | 0.69 (0.49–0.94) | <0.001 | |
| eGFR (mL/min/1.73 m2) | 63.5 (54.0–90.5) | 94.5 (78.8–117.3) | 0.005 | |
| Reasons for meropenem | ||||
| FN (n, %) | 11 (78.7) | 21 (75.0) | 1.000 | |
| BSI (n, %) | 1 (7.1) | 5 (17.9) | 0.645 | |
| HAP(n,%) | 1 (7.1) | 2 (7.1) | 1.000 | |
| UTI (n, %) | 1 (7.1) | 0 (0) | 0.333 | |
| Meropenem treatment | ||||
| Drug daily dose (g) | 4.0 (4.0–4.0) | 4.0 (4.0–4.0) | 0.476 | |
| Treatment duration (day) | 9.0 (7.0–11.8) | 13.0 (8.0–17.0) | 0.101 | |
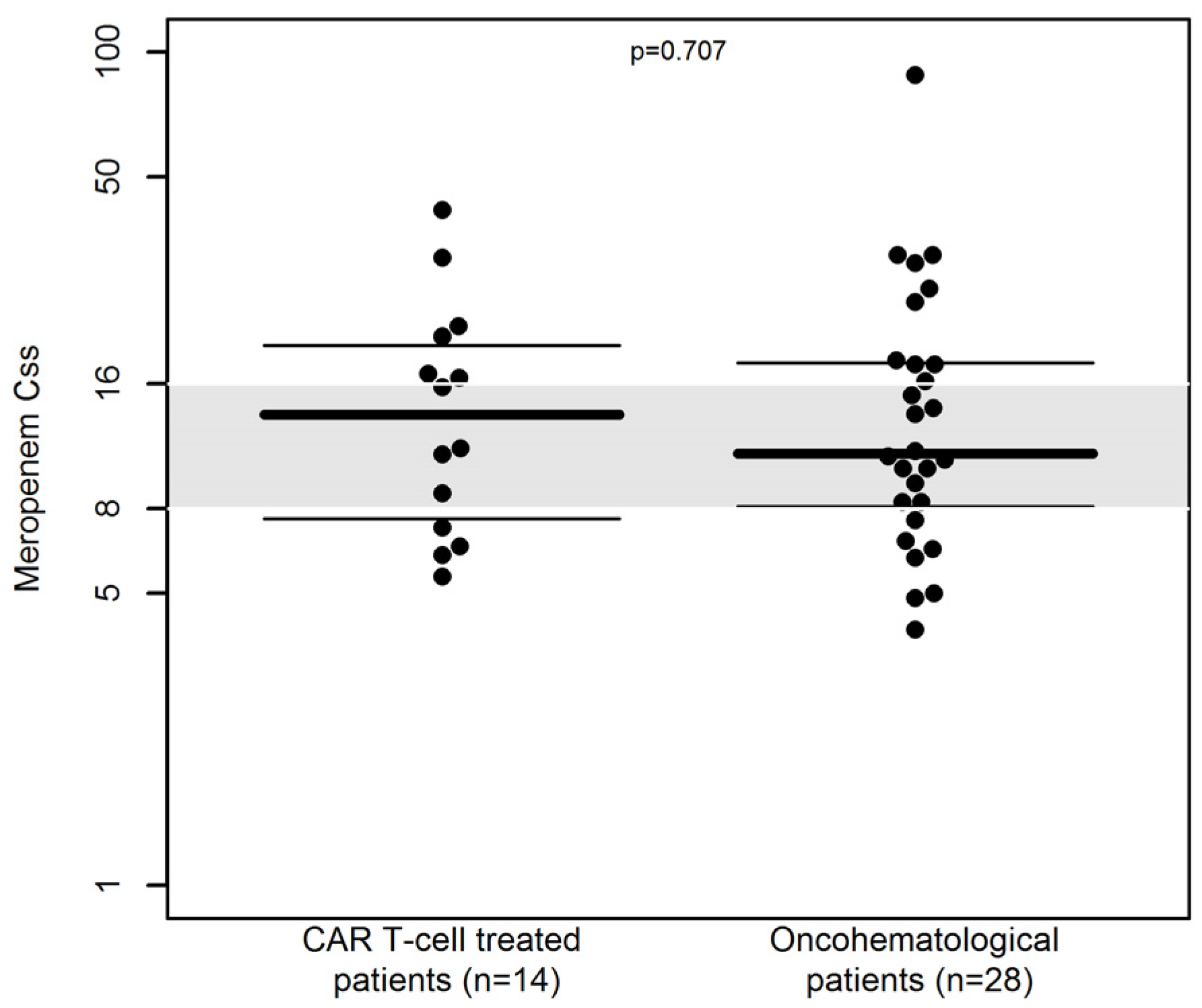
| Css (mg/L) | 11.0 (7.0–15.1) | 12.0 (6.7–17.5) | 0.852 | |
| CL (L/h) | 11.1 (7.9–21.2) | 11.7 (8.2–20.1) | 0.835 | |
| Variable | CAR T-Cell Treated Patients | Oncohematological Patients | p-Value | |
|---|---|---|---|---|
| Number of patients (n) | 24 | 48 | - | |
| Age (year) | 61 (52–64) | 64.5 (47–74) | 0.187 | |
| Gender (male/female) | 14/10 | 29/19 | 1.000 | |
| Weight (kg) | 70 (61.5–82.3) | 70.0 (60–80) | 0.236 | |
| Height (m) | 1.70 (1.63–1.76) | 1.70 (1.64–1.76) | 0.556 | |
| Creatinine (mg/dL) | 0.99 (0.81–1.18) | 0.81 (0.69–1.13) | 0.153 | |
| eGFR (mL/min/1.73 m2) | 76.5 (60.0–96.2) | 95.5 (59.8–105.3) | 0.186 | |
| Reasons for piperacillin/tazobactam | ||||
| FN (n, %) | 20 (83.3) | 35 (72.9) | 0.390 | |
| BSI (n, %) | 2 (8.3) | 10 (20.8) | 0.314 | |
| HAP (n,%) | 1 (4.2) | 2 (4.2) | 1.000 | |
| UTI (n, %) | 1 (4.2) | 1 (2.1) | 1.000 | |
| Piperacillin/tazobactam treatment | ||||
| Drug daily dose (g) | 18.0 (13.5–18.0) | 18.0 (13.5–18.0) | 0.522 | |
| Treatment duration (day) | 6.0 (5.0–14.0) | 9.0 (7.0–12.0) | 0.394 | |
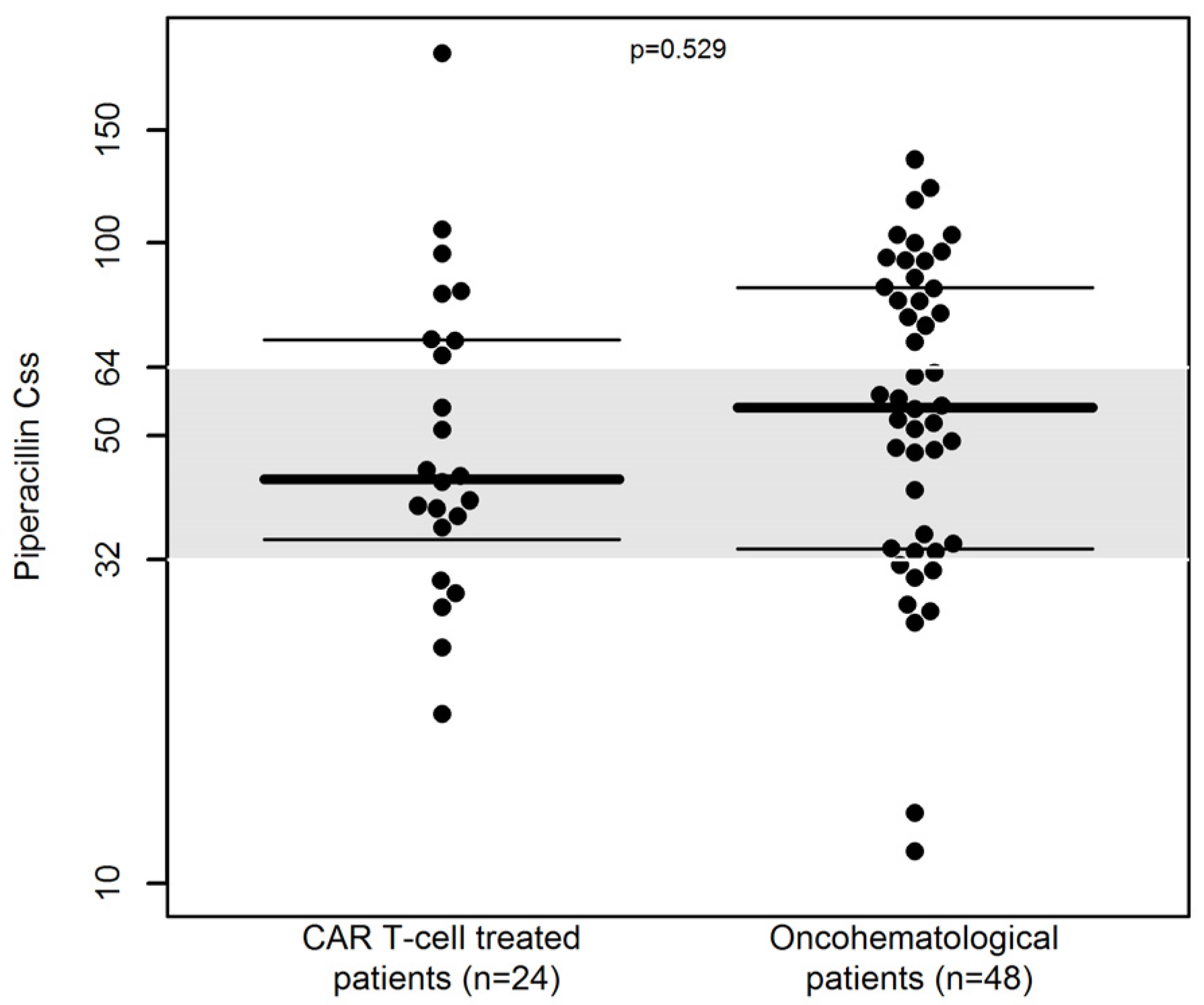
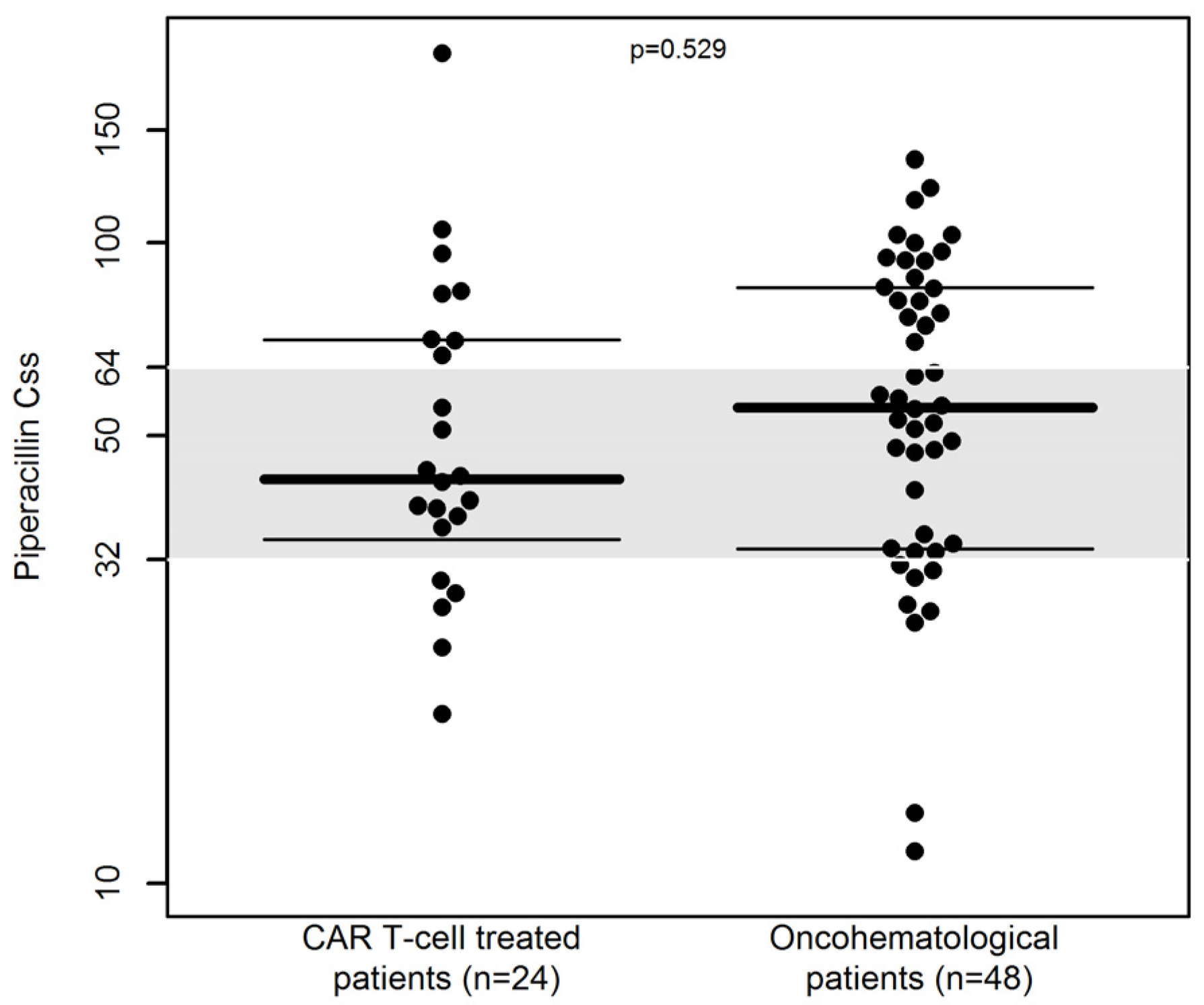
| Css (mg/L) | 43.7 (34.6–65.3) | 58.4 (34.8–90.1) | 0.058 | |
| CL (L/h) | 14.0 (9.0–19.3) | 10.40 (6.38–17.2) | 0.074 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, C.; Cojutti, P.G.; Giannella, M.; Roberto, M.; Casadei, B.; Cristiano, G.; Papayannidis, C.; Vianelli, N.; Zinzani, P.L.; Viale, P.; et al. Does Cytokine-Release Syndrome Induced by CAR T-Cell Treatment Have an Impact on the Pharmacokinetics of Meropenem and Piperacillin/Tazobactam in Patients with Hematological Malignancies? Findings from an Observational Case-Control Study. Pharmaceutics 2023, 15, 1022. https://doi.org/10.3390/pharmaceutics15031022
Liu C, Cojutti PG, Giannella M, Roberto M, Casadei B, Cristiano G, Papayannidis C, Vianelli N, Zinzani PL, Viale P, et al. Does Cytokine-Release Syndrome Induced by CAR T-Cell Treatment Have an Impact on the Pharmacokinetics of Meropenem and Piperacillin/Tazobactam in Patients with Hematological Malignancies? Findings from an Observational Case-Control Study. Pharmaceutics. 2023; 15(3):1022. https://doi.org/10.3390/pharmaceutics15031022
Chicago/Turabian StyleLiu, Chun, Pier Giorgio Cojutti, Maddalena Giannella, Marcello Roberto, Beatrice Casadei, Gianluca Cristiano, Cristina Papayannidis, Nicola Vianelli, Pier Luigi Zinzani, Pierluigi Viale, and et al. 2023. "Does Cytokine-Release Syndrome Induced by CAR T-Cell Treatment Have an Impact on the Pharmacokinetics of Meropenem and Piperacillin/Tazobactam in Patients with Hematological Malignancies? Findings from an Observational Case-Control Study" Pharmaceutics 15, no. 3: 1022. https://doi.org/10.3390/pharmaceutics15031022
APA StyleLiu, C., Cojutti, P. G., Giannella, M., Roberto, M., Casadei, B., Cristiano, G., Papayannidis, C., Vianelli, N., Zinzani, P. L., Viale, P., Bonifazi, F., & Pea, F. (2023). Does Cytokine-Release Syndrome Induced by CAR T-Cell Treatment Have an Impact on the Pharmacokinetics of Meropenem and Piperacillin/Tazobactam in Patients with Hematological Malignancies? Findings from an Observational Case-Control Study. Pharmaceutics, 15(3), 1022. https://doi.org/10.3390/pharmaceutics15031022